
Abstract
Business cases are arguments developed to secure management commitment and approval for investment in an intervention. This systematic review evaluated 12 experimental and quasi-experimental studies on occupational health and safety interventions (OHSI) in various settings. The search engines used in this systematic review include PubMed, CINAHL, and Scopus. A cost and benefit analysis of OHSI was completed at the organizational level in these studies. The focus of this analysis included sample, design, theoretical framework, interventional strategies, and threats to validity and outcomes. Positive returns on investment of OHSI outcomes were shown in 10 of the studies. The other two studies concluded that their chosen OHSI were not cost-effective.
Keywords
According to the U.S. Bureau of Labor Statistics (BLS), nearly 3 million nonfatal workplace injuries and illnesses were reported by private industry employers in 2014. This number of injuries and illnesses reflects a rate of 3.2 cases per 100 full-time workers. Also, the U.S. BLS (2015) has preliminarily reported a total of 4,679 fatal work injuries in 2014. Liberty Mutual’s Workplace Safety Index of 2016 concluded that disabling and nonfatal workplace injuries resulted in nearly US$62 billion of workers’ compensation costs. These costs translate into more than US$1 billion a week spent by businesses on workplace injuries (Liberty Mutual Workplace Safety Index, 2016). On the contrary, a study by Goldman Sachs JBWere Investment Research (2007) revealed that companies adequately managing workplace safety and health performed better financially than those that did not.
A previous systematic review showed a direct positive correlation between investments in safety, health, and environmental performance and subsequent returns on investments (ROIs) from multiple industries and countries, including metal in Finland, aviation in the Netherlands, wood processing in the United States, pet food production in the United Kingdom, automotive industries in Canada, and electronics in Malaysia (Verbeek, Pulliainen, & Kankaanpaa, 2009).
Promoting an effective occupational health and safety intervention (OHSI) system can significantly reduce injuries and illnesses and lower associated costs, including workers’ compensation payments, health care expenses, and lost productivity (Goldman Sachs JBWere Investment Research, 2007; Noben et al., 2015). Existing systematic reviews have examined the effectiveness of OHSI (Verbeek et al., 2009); however, this review critiques the study designs and examines threats to validity of each study. The purpose of this systematic review was to (a) analyze and critique the experimental and quasi-experimental studies using OHSI and (b) examine the efficacy of OHSI. Findings from this review may provide business cases which could be used to secure management commitment and approval of investments in OHSI.
Method
For this integrated review, search engines included PubMed, CINAHL, and Scopus. Search terms include economics, occupational health and safety, business case, cost–benefit analysis (CBA), ROI, and productivity. Inclusion criteria included studies of employed and actively working populations, intervention outcomes based on measurement of costs and benefits in monetary terms, intervention study design (experimental or quasi-experimental studies), and published in English between 2011 and 2016. Exclusion criteria included populations below 18 years of age and OHSI studies that only demonstrated intervention outcomes, not economic outcomes. The search yielded 269 references in PubMed, 99 in CINAHL, and 321 in Scopus. After removal of duplicate references, 328 articles remained. Studies were then screened by title and abstract, and another 282 references were excluded. Finally, after applying inclusion criteria, 12 articles were retained (Figure 1).
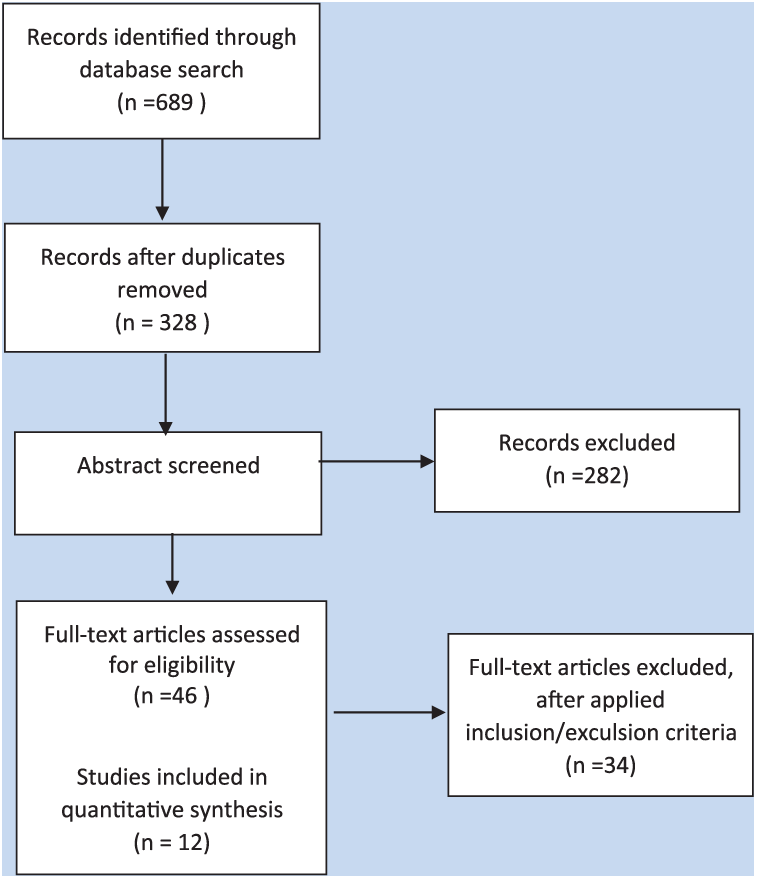
Search flow diagram.
Results
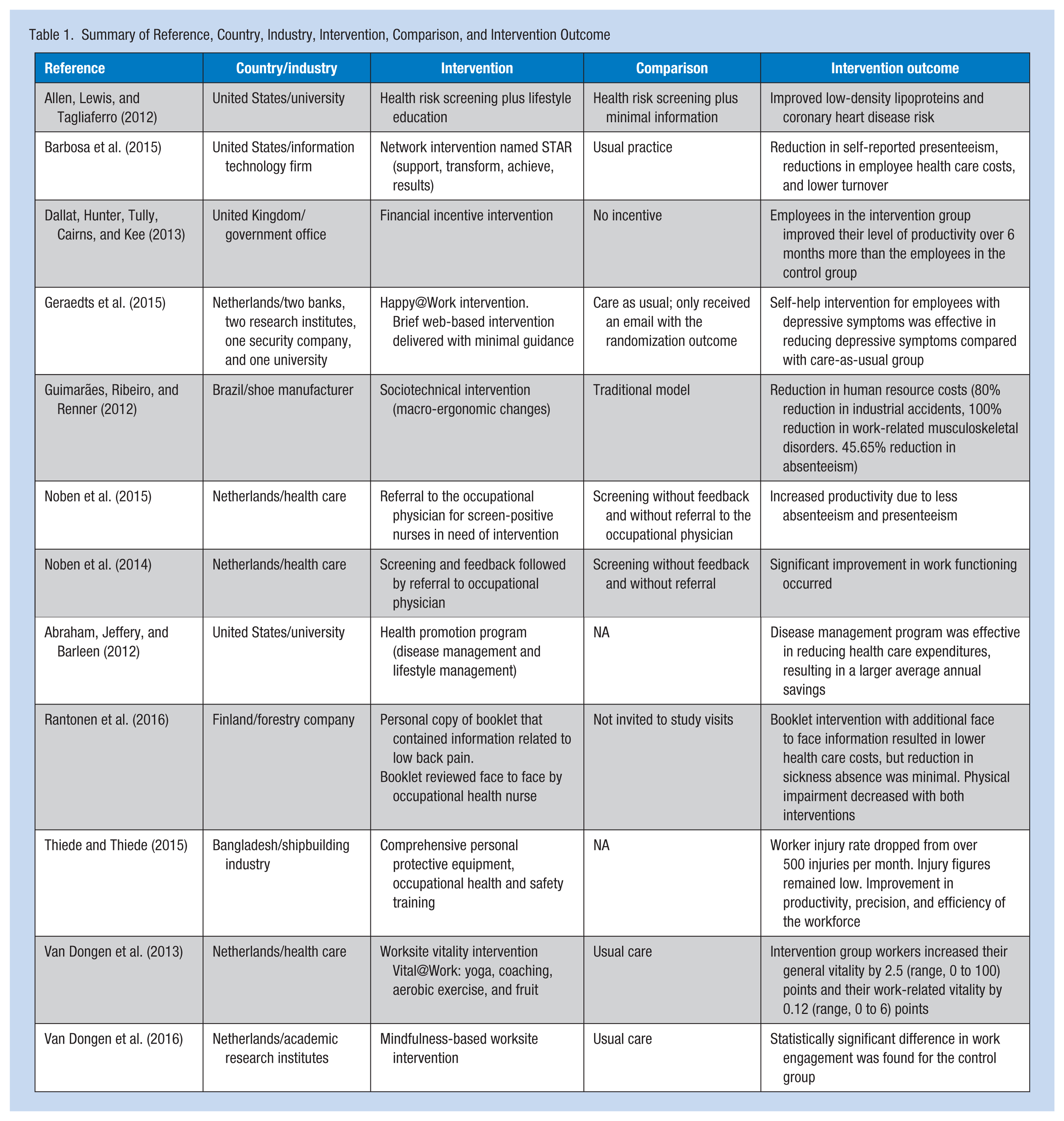
Samples from all studies included employed and actively working individuals. Study samples were selected from various business settings, including a bank, research institutes, government organizations, medical centers, shipbuilding, forestry, universities, information technology firms, and shoe manufacturers (Table 1). Samples were included from six countries (i.e., the United States, the United Kingdom, the Netherlands, Brazil, Finland, and Bangladesh; Table 1). Sample sizes varied among the studies, ranging from 55 (Allen, Lewis, & Tagliaferro, 2012) to 7,936 (Nyman, Abraham, Jeffery, & Barleen, 2012) and are described in Table 3. Only one study (Rantonen et al., 2016) reported power calculations: 85% power using two-tailed tests with the alpha of 0.05 for a sample of 73 employees in each group. Characteristics of the samples were well described among the studies, but only two studies (Barbosa et al., 2015; Rantonen et al., 2016) reported clear diagrams of sample formation and inclusion and exclusion criteria. Noben et al.’s (2014) study provided simple narrative inclusion and exclusion criteria. Van Dongen et al. (2016) only described exclusion criteria, and Van Dongen et al. (2013) study only provided inclusion criteria.
Summary of Reference, Country, Industry, Intervention, Comparison, and Intervention Outcome
Designs
The OHSI studies for this systematic review used either an experimental or quasi-experimental design (Table 2). Seven studies used a randomized control trial design. Barbosa et al. (2015) used adaptive randomization to ensure balance on job function, leadership, and size of the study group. The next three studies clearly described randomization and allocation methods. Van Dongen et al. (2013) used random allocation software, and the operator for this randomization had no information about the samples to ensure concealment of treatment allocation. Noben et al. (2014) employed cluster randomization at the hospital ward level to prevent contamination between participants working in the same ward. Noben et al.’s study also used a prerandomization procedure with an “incomplete-double-consent” design, in which participants were only informed about their own group to further minimize the risk of contamination. Rantonen et al.’s (2016) study chose a randomization scheme for a trial that was prepared by an independent biostatistician before the study began. Rantonen et al.’s study used a computer-generated randomization table with a block size of eight.
Summary of Study Population, Study Design, Economic Evaluation Method, and Economic Outcome
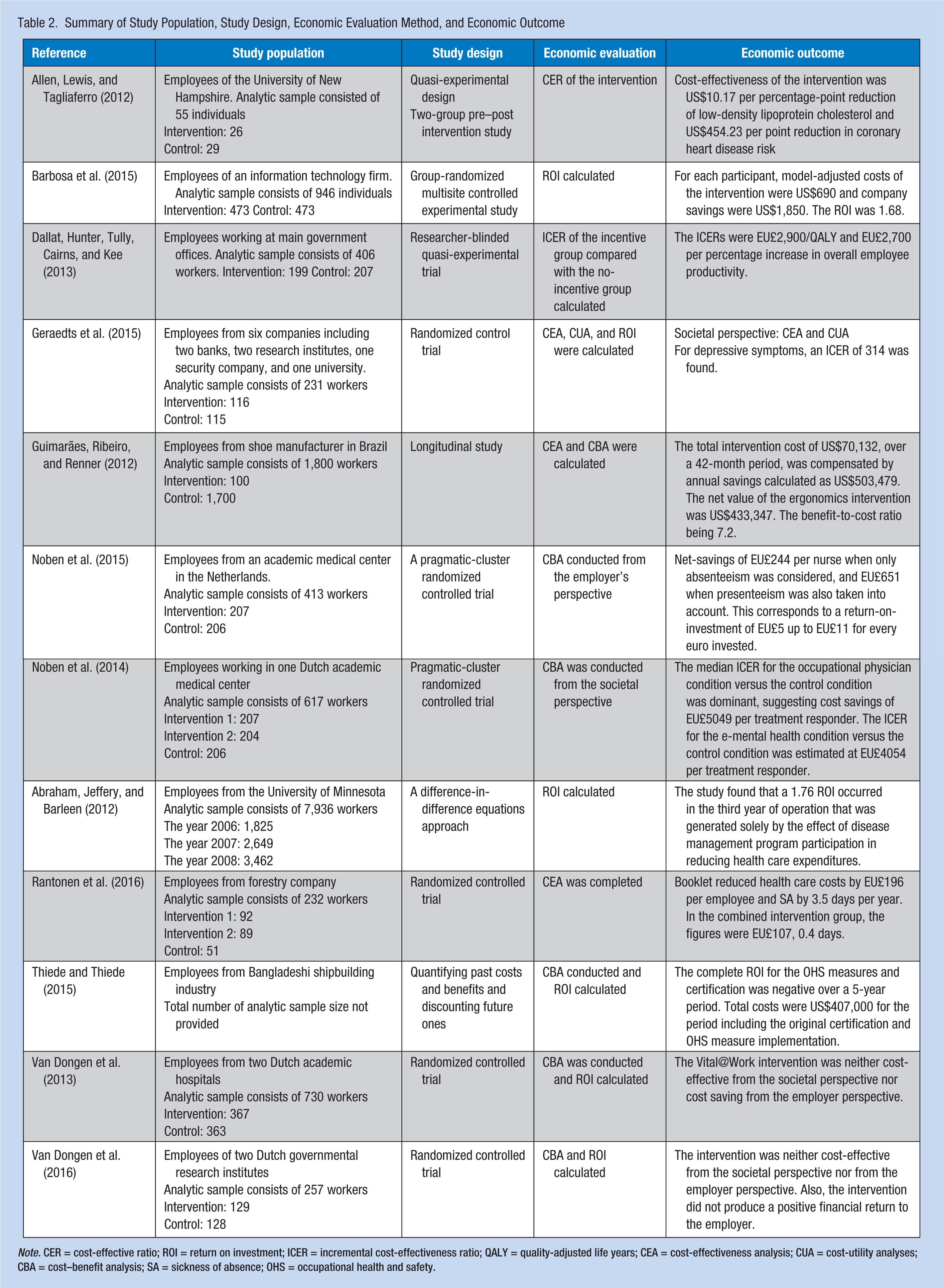
Note. CER = cost-effective ratio; ROI = return on investment; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life years; CEA = cost-effectiveness analysis; CUA = cost-utility analyses; CBA = cost–benefit analysis; SA = sickness of absence; OHS = occupational health and safety.
Five studies were quasi-experimental designs. Dallat, Hunter, Tully, Cairns, and Kee’s (2013) study was a researcher-blinded quasi-experimental trial. Both the intervention group and control group could use electrical cards to self-monitor their physical activity levels at work. However, the intervention group received points that could be redeemed for rewards.
Theoretical Frameworks
The theoretical frameworks used for each study were not described in any of the articles included in this systematic review. Three main keywords were used throughout the included articles reviewed, “cost-effectiveness,” “costs and benefits,” and “return on investment.” Because the purpose of the business case is an economic evaluation of OHSI, a positive monetary return is a key research driver. The word “cost-effectiveness” is used in the title of eight included studies.
Economic Evaluation
Four different methods were used for calculating the economic effectiveness of OHSI. A cost-effective ratio (CER) was used in two studies. The CER was calculated by dividing the cost of the intervention by unit of effectiveness. Cost–benefit analysis was used in six studies. The CBA is a systematic process for calculating and comparing benefits and cost of a decision (Table 2). Cost-effectiveness analysis (CEA) was calculated in three studies. The CEA compares the relative costs and outcomes (effects) of different courses of action. Return on investment was calculated in four studies. Return on investment is used to evaluate the efficiency of an investment. A higher ROI means the investment gains compare favorably to investment costs. Seven studies used only one economic evaluation method; the other studies used more than two of the previously listed methods.
Economic Outcome
Monetary economic outcomes are described in Table 2. Van Dongen et al.’s (2013; Van Dongen et al., 2016) two studies concluded their interventions were neither cost-effective nor cost saving. The other studies showed their interventions resulted in positive monetary savings or return. Thiede and Thiede (2015) study’s unique conclusion showed that complete ROI for the OHSI was negative over a 5-year period.
Interventions
Comparison of interventions is described in Table 1. Occupational health and safety interventions in this review study are either health promotion or injury prevention strategies. Interventions for eight studies were health promotion or injury prevention education and training, including lifestyle change training, online-supported cognitive therapy, a disease management program, yoga, exercise, or an educational booklet. Thiede and Thiede (2015) described the scale of an organizational intervention. The study was implemented in the Bangladeshi shipbuilding industry, and the study intervention included comprehensive personal protective equipment, occupational health and safety training, and the establishment of a primary health care center. The level of intervention and size of settings varied in this systematic study.
Intervention Outcome
Although Van Dongen et al.’s (2013; Van Dongen et al., 2016) two studies concluded no monetary savings or ROI resulted from the studied intervention, a positive intervention outcome was identified from both of their studies and the other studies that were evaluated. Measuring effectiveness of their intervention methods varied depending on the intervention. Intervention outcomes (i.e., lowering heart disease risk, depressive symptoms, turnover rate, weight, injury rates, health care costs, and self-reported presenteeism or improving productivity and vitality) are described in Table 1.
Discussion
Threats to Validity
Table 3 describes threats to validity. Mortality was the most frequent threat to internal validity. Nine studies reported “dropout” as a study limitation. Because the purpose of the studies was to examine the efficacy of the OHSI, 6 months to 12 months of monitoring was required to examine economic outcomes. Retaining all participants until the end of the study period was extremely challenging. Researchers could have contacted the participants more frequently than was reported to encourage participants to stay in the study until the end. Asking open-ended questions of participants regarding factors that would motivate them to participate in the study for longer periods of time may have been an effective approach. Selection bias was the second most frequently found internal validity threat. Eight study authors reported selection bias as a limitation of their studies. The convenience sampling method could have resulted in overselecting participants who volunteered, or high-achieving employees. Random sampling could decrease this threat.
Threats to Validity
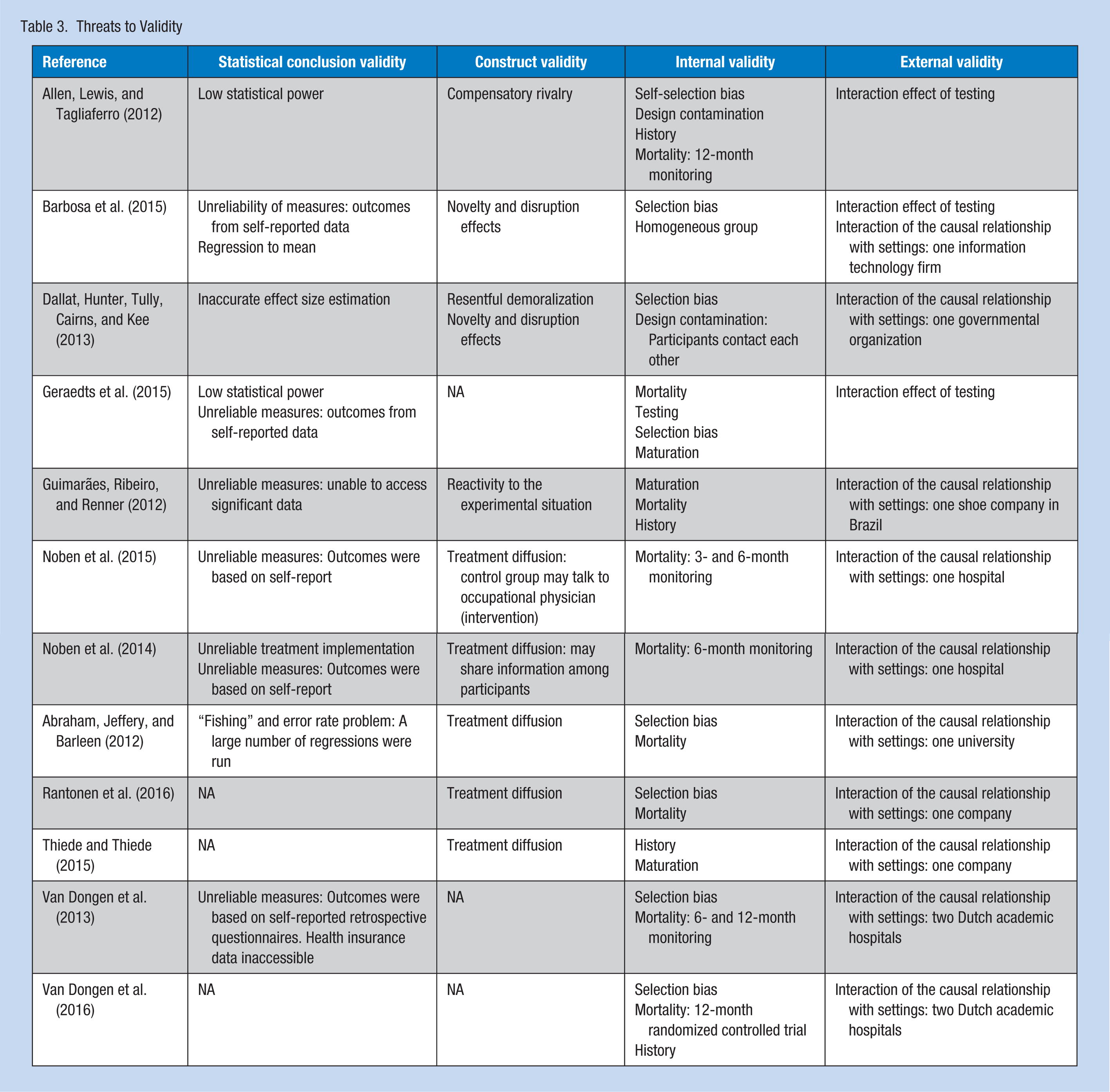
Interaction of the causal relationship with settings was noted in 10 studies as a threat to external validity. Most of the studies collected data from one or two settings, the result of both financial and situational factors. Results from the studies may be transferable to similar settings but not every business setting. Selecting multiple settings would increase the generalizability of study findings.
Treatment diffusion was found to be a construct validity threat in five studies. When data are collected in only one or two settings, participants may share information about interventions or treatments. Compensatory rivalry and demoralization might have also been noted in Allen et al.’s (2012) and Dallat et al.’s (2013) studies. Selecting study populations from a variety of units and settings and using blind or double-blind study designs may reduce this threat.
Limited measurement reliability was noted in six studies, raising questions concerning statistical conclusions and validity. Certain outcomes, and participant’s perspectives on the efficacy of the interventions, were measured based on self-report. Based on the results, it is difficult to conclude that participant reports were accurate and outcome measures were reliable. Use of tools that measure objective outcomes may reduce this threat.
Strengths
The strength of this literature review is that business cases were searched systematically using Internet search engines. This literature review emphasized CBA to secure decision makers’ commitment and approval to implement OHSI. As shown above, all but two studies resulted in improved employee health and monetary benefits to employers. The cases provide meaningful information on how OHSI can create a positive balance between cost and benefit.
Limitations
The outcome of the interventions was either total dollars saved annually or ROI. Most studies were longitudinal and the assumption that the benefits would continue at the same level as the first year could be false. It is possible that this review missed case studies reported in the gray literature (Google or Yahoo general search engines). Business cases that demonstrated unfavorable results are less likely to be published. Consequently, published studies included in this review may bias interpretation of the evidence regarding OHSI results.
Implications for Practice and Research
The following are areas for improvement. Intangible benefits such as reputation damage and risk of disobeying regulations should be assessed. Reliable and valid guidelines for reporting business cases are needed. The value of the cases can be underestimated when structures and consensus among business administrators are missing. None of the studies from this review were conducted based on a theoretical framework or model. Theory-based studies provide stronger evidence of a positive correlation between OHSI and economic effectiveness. Selecting study populations from a variety of geographic regions and business settings, with worker racial and socioeconomic diversity, could result in a more representative sample.
Conclusion
This integrative review suggests the economic benefits of OHSI. Administrators will use OHSI based on data, evaluation of health and economic impact, and their assessment of OHSI importance to the company. The foundation of policies and regulations related to occupational safety and health must be economically and ethically sound. However, because economic value is a critical factor that drives administrator decision making, conducting well-designed business case studies should be expanded.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Geunjae Lee is a PhD student, College of Nursing, University of Cincinnati.