
Abstract
In response to startling statistics in the increasing number of workplace violence (WPV) incidents against health care workers, California employers across the continuum of care are preparing their organizations to comply with California Occupational Safety and Health Administration (CAL/OSHA) regulation SB 1299. This groundbreaking legislation requires hospitals and other health care settings to implement written strategic prevention plans and broaden the identification and reporting of incidents related to WPV. Also included in the law is a minimum staff education requirement and formal risk identification and mitigation plans. The occupational health nurse will play a critical role in preparing health care organizations and staff in this endeavor.
Keywords
In 2015, the Occupational Safety and Health Administration (OSHA) reported that health care workers are injured as a result of violence at an alarming rate, with approximately 24,000 assaults reported in health care settings between 2010 and 2013. California OSHA’s (CAL/OSHA) new regulations, effective April 1, 2017, require hospitals to implement written strategic prevention plans to protect all employees from violent and aggressive behavior in the workplace. All health care facilities with patients admitted for 24-hour stays or longer (e.g., hospitals, home health agencies [including hospice at home], emergency medical services, medical transport companies, and correctional and detention settings) must comply with the regulations (CAL/OSHA, 2017).
The approach to the implementation cascades over the next 12 months. Beginning in April of 2017, hospitals must establish and maintain a log devoid of personal identifying information that captures all incidents of workplace violence (WPV)—whether an injury occurred or not—and include postincident responses and the investigation of any WPV injuries over the last year (CAL/OSHA, 2017). These agencies are also tasked with establishing documentation of workplace hazard identification, evaluating risks and correcting any findings, and tracking all training records of employees. One of the larger components of the legislation is the mandatory reporting of any incident where physical force was used against an employee, whether or not the employee was injured in the attack. Any incident involving a firearm or other dangerous weapon, whether or not directed toward an employee, must also be reported (CAL/OSHA, 2017).
By April 1, 2018, health care facilities identified in the legislation also must develop formal written WPV Prevention Plans, to be reviewed annually, as part of each employer’s Injury and Illness Prevention Program (IIPP). In addition, employers are also to provide effective training on WPV prevention for all employees and to provide all necessary protective equipment and tools required by CAL/OSHA (2017).
Background
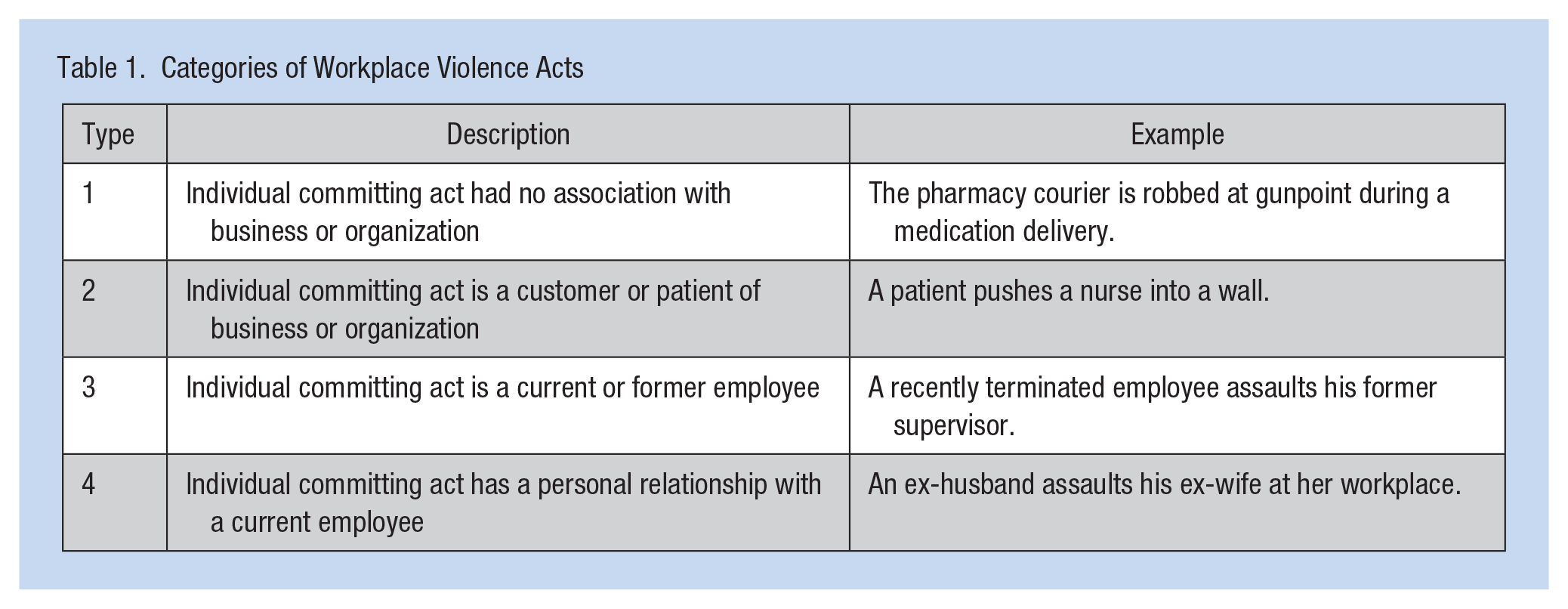
SB 1299 defines WPV as “any act of violence or threat of violence that occurs at the worksite” (Workplace Violence Prevention Plans: Hospitals, 2017, p. 3); any act of violence or threat of violence toward an employee that causes physical or psychological harm or have a high potential to harm as well as any incident involving the use of a firearm or other weapon. The distinction between act or threat of violence is important; no actual physical contact need take place for the report and response to be required according to the legislation—the threat of violence is sufficient. Categories of WPV incidents are listed with examples in Table 1 (Howard, 1996; Peek-Asa, Howard, Vargas, & Kraus, 1997; Workplace Violence Prevention Plans: Hospitals, 2017).
Categories of Workplace Violence Acts
In 2016, OSHA reported approximately 24,000 health care employee assaults between 2010 and 2013, with physical injuries ranging from minor to major, psychological harm, and both temporary and permanent disabilities. The Joint Commission (TJC) examined 74 rapes, 38 assaults, and 33 homicides for which the victims were nurses, physicians, security officers, and other health care workers. All these incidents were classified as sentinel events, and all resulted in employee death, severe temporary harm or permanent disability (TJC, 2016).
Hospitals in the United States have reported increasing violent crime, up from two events per 100 beds in 2012 to 2.8 events per 100 beds in 2015. A significant number of these violent events were categorized as aggravated assaults (44%); 46% of aggravated assaults occurred in emergency departments compared with all other areas of the hospital (TJC, 2016). Nurses are among the health care workers most exposed to WPV, and the results can be devastating (International Council of Nurses, 2009; Roche, Diers, Duffield, & Catling-Paull, 2010). The negative effects on victims and their colleagues can lead to emotional distress, diminished well-being, low self-esteem, depression, fear, feelings of powerlessness, lower job satisfaction, and even suicidal ideation (Applebaum, Semerjian, & Mohan 2012; Aytac & Dursun, 2012; Embree & White, 2010; Waschgler, Ruiz-Hernandez, Llor-Esteban, & Garcia-Izquierdo, 2013).
Although violence typically affects all categories of workers regardless of race, religion, education, and other demographics, women are still targets more often than men, and 95% of nurses around the world are women (International Council of Nurses, 2009). The International Council of Nurses (2009) reports that some of the more startling statistics about nurses and WPV include the following:
Health care workers are more likely to be assaulted at work than prison guards or police officers
Female nurses are the most vulnerable category of health care worker for WPV
General inpatient units are now the second most frequent area for assaults, with the emergency department being first and psychiatric wards moving into third place
Assaults are most frequently perpetrated by patients
In the United Kingdom, 97% of respondents to a survey indicated that they knew a nurse assaulted during the last year
In the United States, 72% of nurses responding to a survey do not feel safe from WPV
Underreporting of assaults to administration or law enforcement also leads to misconceptions regarding the scope of the problem. Regrettably, for many health care workers, violence is perceived as “part of the job,” which may contribute to underreporting WPV (Centers for Disease Control, 2014; OSHA, 2015). Copeland and Henry (2017) described the two most prevalent reasons for not reporting assaults: “no one was hurt” and “it is an expected part of the job;“ if no one was hurt, the situation might not register as a WPV incident. In 2008, the Emergency Nurses Association conducted a member survey and the most frequently cited barrier to reporting WPV events was fear of retaliation (45%). Nurses report that strong leadership support increases their perception of safety (Copeland & Henry, 2017).
Risk Identification in the Health Care Setting
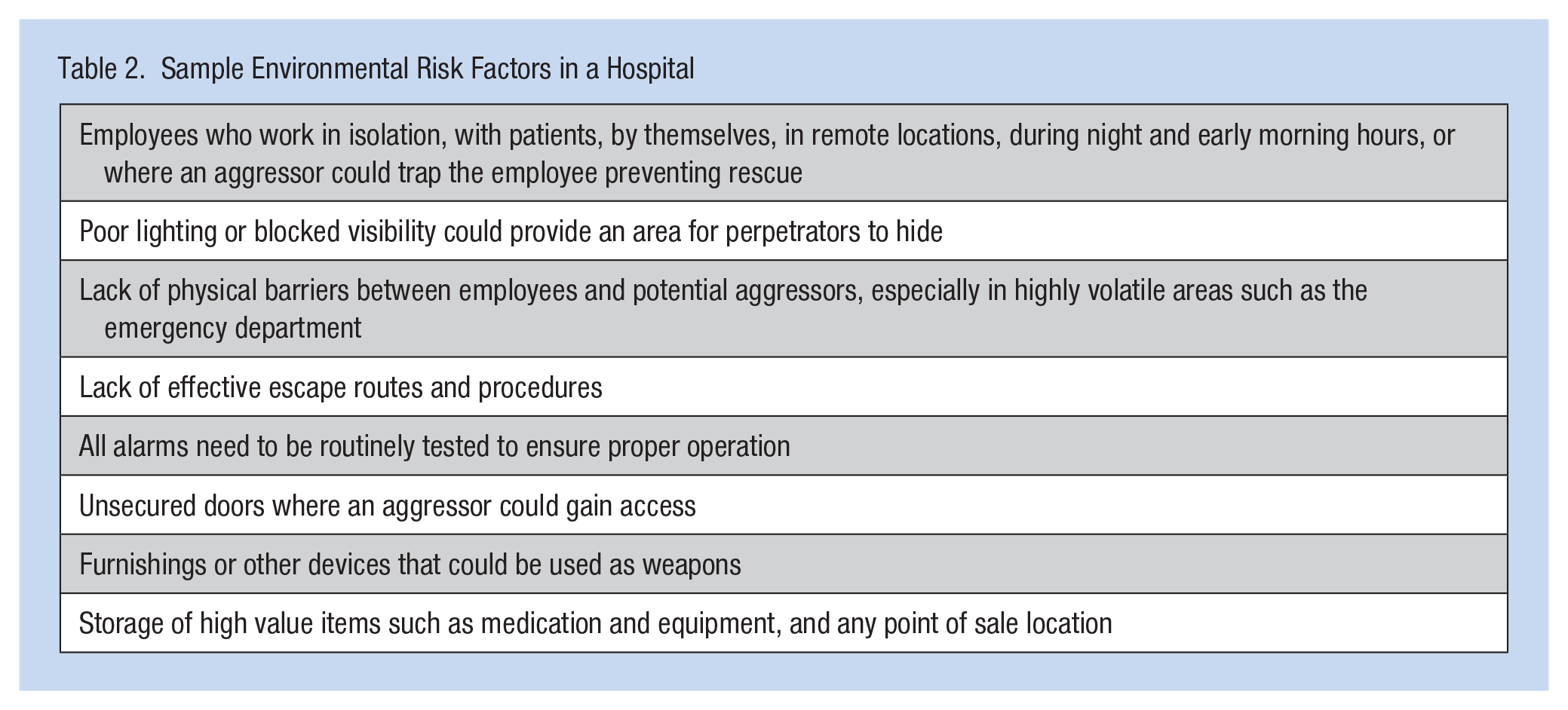
The legislation also calls for assessment procedures to identify risk factors in the workplace environment and the community, including a review of all WPV injuries during the previous year, whether or not they resulted in injuries (Workplace Violence Prevention Plans: Hospitals, 2017). An environmental risk assessment refers to identifying any factors or conditions in a health care facility that may contribute to the severity of a WPV event. Environmental risk factors can also be associated with specific tasks, such as collecting money or transporting medications (Workplace Violence Prevention Plans: Hospitals, 2017).
Specific risk assessments in fixed workplaces (e.g., acute care hospital) evaluate the potential for violence on each unit and in every area inside the facility as well as areas surrounding facilities (e.g., parking lots, common walkways, and driveways). Leaders must develop assessment tools, checklists, and other strategies to identify locations and situations where WPV is more apt to occur; the WPV prevention plan must be reviewed annually. Table 2 shows a list of potential environmental risk factors to consider (Workplace Violence Prevention Plans: Hospitals, 2017).
Sample Environmental Risk Factors in a Hospital
Other facets of the legislation are in the process of being implemented in hospitals across California including establishing procedures to identify and evaluate patient-specific risk factors and the daunting task of assessing visitors and other individuals in the facility who are not employees or patients (Workplace Violence Prevention Plans: Hospitals, 2017). Some of this work must be collaborative with community law enforcement and emergency medical service partners. Hospital safety officers must also develop strategies to address and mitigate any of the risks identified in the environmental risk assessment and, where a permanent fix is not available, implement and document interim measures.
Besides creating and maintaining a log of all WPV instances, leaders must develop an effective response plan for actual or potential WPV events, again collaborating with community law enforcement and emergency medical agencies. This log should include responding to mass casualty threats (e.g., active shooter) with evacuation and sheltering plans, a procedure for alerting staff and a process for evaluating the effectiveness of the plan (Workplace Violence Prevention Plans: Hospitals, 2017).
Identification and Discussion of Legal Risks
Penalties associated with CAL/OSHA regulation noncompliance have not been published nor has weighting been assigned to any of the categories to prioritize actions at the organizational level. For example, for the stipulation that a potential risk in the environment is no barrier between staff and patients is difficult to enforce and still provide care. If it is not logically feasible, what is the potential facility penalty? Legal counsel should be engaged to determine likely scenarios in health care organizations based on individual environmental risk assessments.
A prominent area of focus is staff training. All employees of the hospital must have training about specific threats they may encounter in their work settings. Over the last several months, leaders in organizations across the state have been working with in-house security colleagues to develop web-based and interactive training for all employees, with additional training for emergency department and behavioral health workers, and some are also offering the optional active shooter course for employees in all settings because of the prominence of these events in the news. Training must occur on hire and annually, with all training records retained for a period of 1 year and disclosed to CAL/OSHA upon request.
Discussion of New Reporting Expectations
Although every organization typically has emergency operation plans, WPV has not always been a prominent focus, and only reports to OSHA when an injury occurs. A significant paradigm shift for both employees and leaders should occur so hospitals will comply with regulations regarding the reporting of all WPV, whether or not injuries occur. To incorporate definitions of required reported situations, organizations must support staff members in interpreting and defining situations based on context (Copeland & Henry, 2017). As an example, if a nurse is injured because a patient with delirium strikes the employee, that Type 2 event could be interpreted by the nurse differently than if it were a patient’s daughter who attempts to strike a nurse because she is upset with the quality of her mother’s care. However, no preclusion exists for patients with dementia to be exempt from reporting; nurses must know this, discuss it, and be able to apply logic to these situations.
Implications for Occupational Health Nurses
SB 1299 indicates that organizations must operationalize procedures that support postincident investigation and reporting, including a plan to provide first aid to employees who were injured in an incident, ensuring all employees involved in the incident are identified, and providing trauma counseling to all employees impacted by the incident (Workplace Violence Prevention Plans: Hospitals, 2017). One of the greatest challenges occupational health nurses face is an awareness of incidents that are not reported. Collaboration with hospital safety officers, security, and other key leaders is necessary to integrate the occupational health team into the WPV Prevention Plan and increase staff awareness of the issues.
Prevention, planning, response, and recovery are four key areas that occupational health nurses must use to prepare responses to WPV in their organizations (Brown & Burns, 2013). Key strategies for the occupational health nurse include (Ford, 2012) the following:
Collaborate on policies with the interdisciplinary team that focus on the prevention and response to WPV incidents
Participate in worksite analyses to identify risks and opportunities for improvement
Coordinate with safety leaders to provide the required education for all staff members
Establish workflows that include availability of trauma counseling postincident for all employees affected
Assist in the development of workflows that promote the reporting of WPV incidents that do not result in injury
Conclusion
Implementing the requirements of California SB 1299 is more difficult because of the long-standing expectation by frontline staff that they will be exposed to violence and the current perception that if there is no injury, no violence took place (Copeland & Henry, 2017). Leaders must provide an emotionally safe environment where frontline staff is supported by realistic and effective mechanisms to respond to WPV. A risk assessment and corrective action plan that build the WPV Prevention Plan can mitigate potential WPV staff exposures. An effective and interactive training program that is specific to defining WPV and educating employees on realistic safety procedures can provide guidance and support to staff during challenging times. The role of the occupational health nurse is central to the interdisciplinary team responsible for the prevention, response, and reporting of WPV incidents.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Patricia (Pidge) Gooch has more than 28 years of acute care experience, and for the last 15 years, worked in emergency services, disaster preparedness, and executive hospital operations. She holds her master’s degree in nursing administration (MSN) from Florida Atlantic University and is currently completing her doctor of nursing practice (DNP) degree at the University of San Francisco.