
Abstract
The fields of travel and international medicine are rapidly changing and growing. The role of occupational and travel health nurses is expanding and should be a focus for the future. At the American Association of Occupational Health Nurses Annual meeting on March 24, 2015, in Boston, five presentations were included in the session, An Update on Travel Vaccines and Issues in Travel and International Medicine. This article summarizes three of the presentations and includes a portion of the information generated by the Centers for Disease Control and Prevention (CDC) included in the fourth presentation. The first section focuses on the Essential Elements of Travel Medicine Programs including the pre-travel care assessment, trip research and risk identification, medication intervention review, non-pharmaceutical and prevention strategies, and post-travel care. The next section is an overview of key issues for business travelers. The growth in the number of international business travelers and unique aspects of business travel are emphasized in a comprehensive travel health program. This section also includes a discussion of expatriates and their special risks identified in recent literature (e.g., an assessment of the significant costs of health events and productivity losses by both business travelers and expatriates). The final section offers a specific example of a vaccine-preventable disease, namely, Japanese encephalitis (JE) virus, and needed changes in JE vaccine recommendations.
Keywords
The pre-travel consultation is a key element in assessing potential health risks and providing education on anticipated travel risks and the immunizations and prophylactic medications needed. The goal of the consultation is to empower travelers to manage their health during the trip including self-treatment if necessary.
Pre-travel care has several phases including assessment, trip research and risk identification, pharmacological interventions, and non-pharmacological and prevention strategies (Rosselot, 2004). Phase 1, the pre-travel assessment, begins with a full understanding of the trip. Each destination and any stopovers must be considered as well as the dates and duration of each portion of the trip. A comprehensive travel health history is essential and should include demographic information, health history including allergies, immune status, medications, immunizations and vaccinations, any special conditions (e.g., pregnancy, breast feeding, disability), and prior travel experience (CDC, 2008).
Phase 2, trip research and risk identification, begins with a full review of the planned modes of travel. The timing of a potential trip is important because the season of the year (e.g., rainy or dry season) at each site will impact risk. In addition, some areas may be prone to natural disasters. The accommodations should be reviewed for any specific safety or security issues and the availability of heating, ventilation, and air conditioning. The activities during planned trips including events and leisure time should be examined for potential risks. The type of activities anticipated are an important part of trip details and how the traveler will prepare for these activities, particularly outdoor activities. Any disabilities or special needs (e.g., food) and family members or other members of the travel group should be considered. Specific cultural issues, laws, and what to expect in remote and urban areas should be addressed (Druckman, Harber, Liu, & Quigley, 2014).
After a full understanding of the trip itinerary, Phase 3 includes an evaluation of vaccines and medications. Routine, required and recommended vaccines, and prior vaccination history are essential as are risk factors, contraindications, precautions, and level of immunocompetence. Indicated travel vaccines should be identified using updated materials from government agencies (e.g., Centers for Disease Control and Prevention [CDC], WHO) and expert databases (e.g., Travax/Shoreland). The timing of vaccinations must insure adequate time for the full course of vaccination or a plan for vaccines to be administered simultaneously at the same visit (Chen, 2014). All employees must be monitored for adverse reactions. Routine vaccinations include hepatitis B, human papillomavirus (HPV), influenza, measles, mumps, rubella, meningococcal, pneumococcal, polio, tetanus, diphtheria, pertussis, varicella, and herpes zoster. Common travel vaccines include hepatitis A, yellow fever, typhoid, meningococcal, Japanese encephalitis (JE), rabies, tick-borne encephalitis, and cholera. However, tick-borne encephalitis and cholera vaccines are not available in the United States (Chen).
The occupational health nurse should also determine the need for antimalarials, antimotility agents, antibiotics, motion sickness agents, antivirals, and allergy medications. Both dosage for prophylaxis and treatment should be ascertained (CDC, 2008).
In Phase 4, the non-pharmacological and prevention strategies are addressed. Health education must be customized and includes appropriate presentation of risks, risk management, psychological impact of travel, and vaccines and chemoprophylaxis recommendations. Employees must carry medical records (e.g., electrocardiogram) including all immunizations (e.g., yellow fever).
Safety and security issues (i.e., vehicular safety, road animals, and poor signage with unfamiliar language) should also be discussed. Air travel risks include jet lag, travel-related venous thrombosis, airborne illness, and aerotitis. Disruption of circadian rhythm from poor sleep or fatigue is also an area for education.
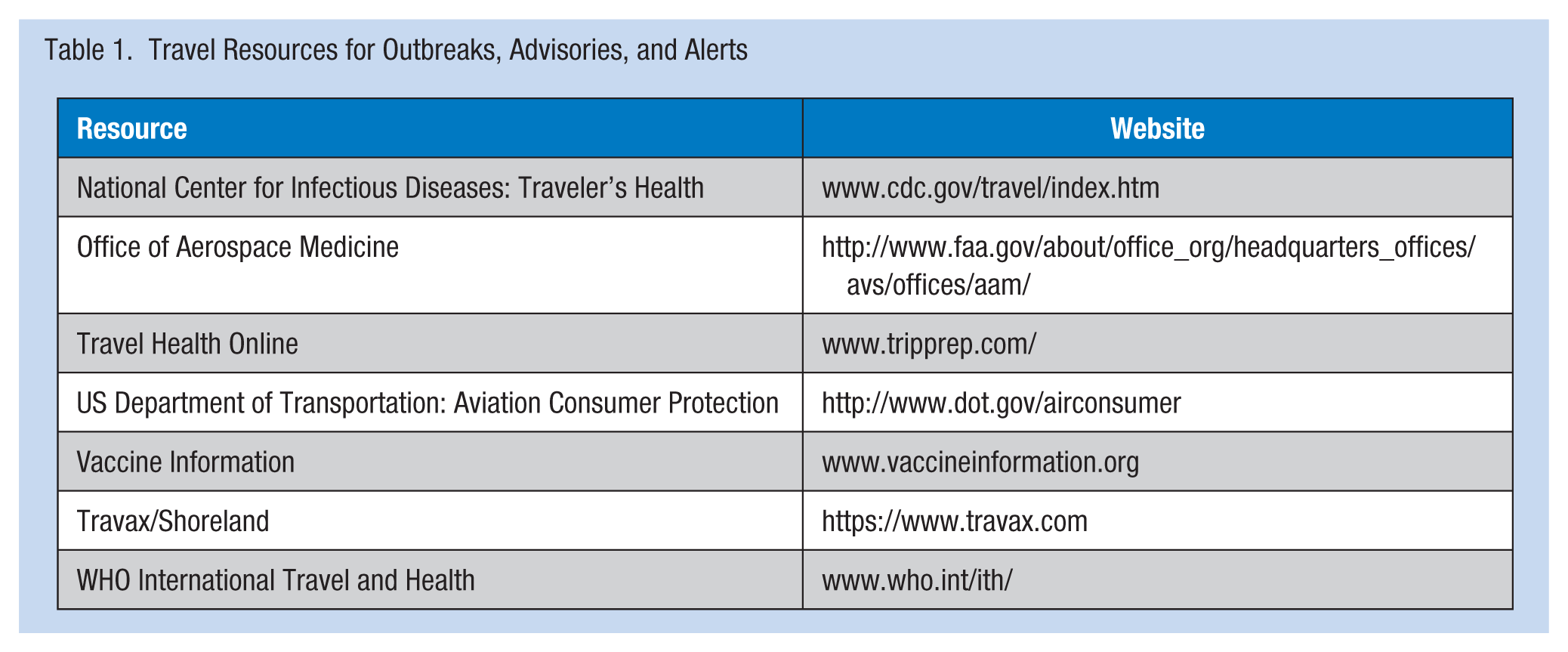
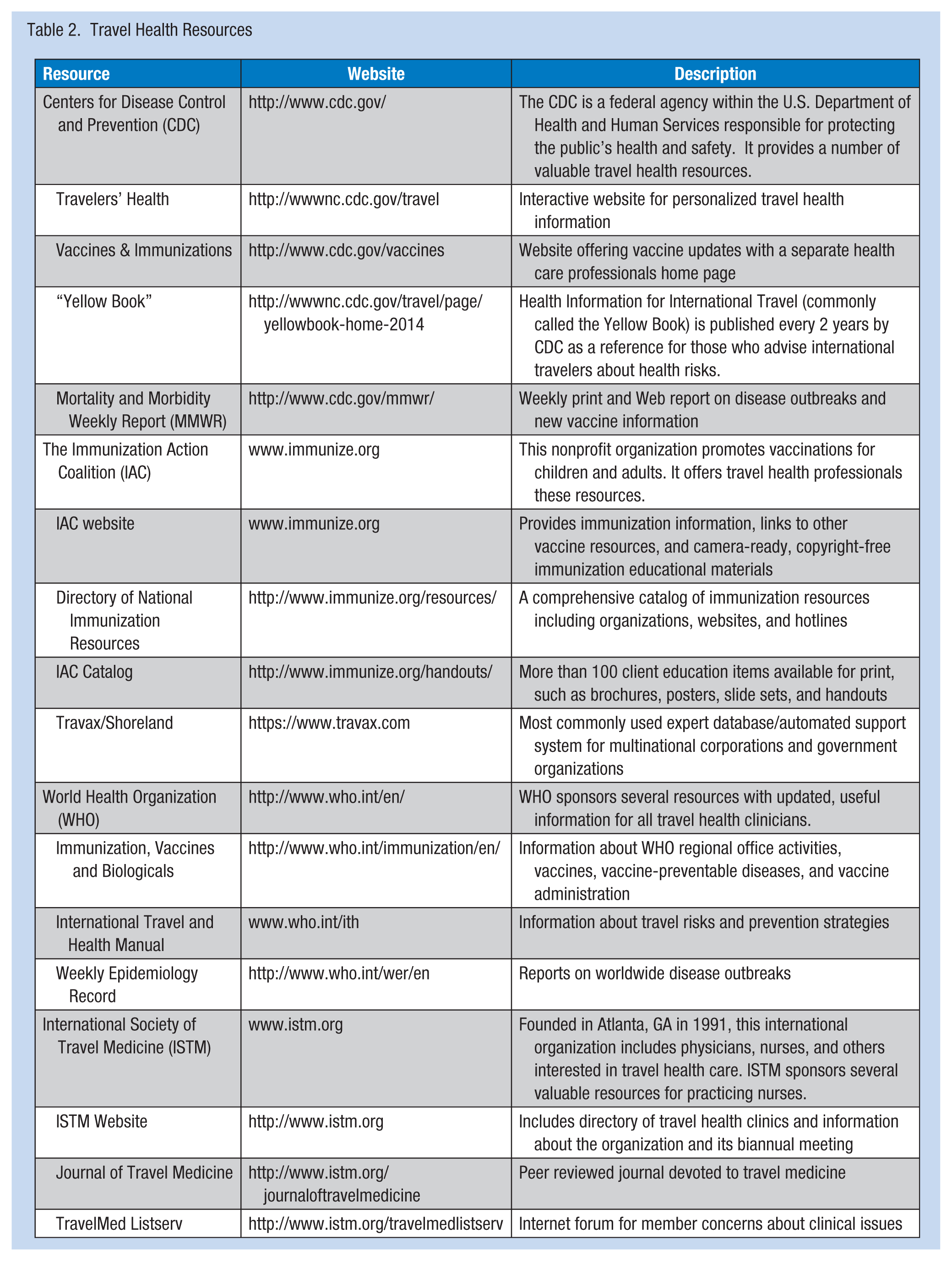
Specific infectious diseases (e.g., food- and water-borne illnesses and those caused by blood-borne pathogens and insects) at each destination and their prevention as well as environmental factors (e.g., heat and cold, sunburn, air and water pollution, recreational hazards, altitude, and animals) should be discussed. Self-management of minor illnesses and injuries, and exercise options are often provided in concise handouts. Travel medicine kits with first aid supplies and specific medications can be provided (Kogelman, Barnett, Chen, & Quinn, 2014). A number of resources can be used to find travel advisories, outbreaks or alerts, and travel health resources (see Tables 1 and 2).
Travel Resources for Outbreaks, Advisories, and Alerts.
Travel Health Resources.
Finally, post-travel care is essential. Studies show that upon return, 22% to 64% of travelers will have a health-related problem that was not resolved by the conclusion of the trip (Fairley, 2014). Particularly for business and occupational travelers, occupational health professionals will be asked to address these illnesses and injuries. The post-travel visit will consider the severity of the illness, travel itinerary, duration, timing, and place of illness onset. The most common illnesses are diarrhea, upper respiratory infections and dermatologic conditions, or febrile illnesses. In addition to risk factors during the trip, a past health history, any current medications or medications taken during the trip, and a full review of vaccinations and compliance with chemoprophylaxis (e.g., antimalarials) should be conducted. Accommodations, insect precautions, drinking water sources, types of food consumed (e.g., raw meat, seafood, unpasteurized dairy products, food from street vendors), fresh water exposure (swimming, rafting), scratches, insect or animal bites, body fluid exposures (tattoos), sexual activity, and health care sought during the trip (e.g., injections or transfusions) should be evaluated. Careful case management of each traveler and appropriate referral such as infectious disease diagnosis and treatment should be conducted.
Business and Occupational Travelers Assignees Vaccine Prevention and Productivity Issues
The number of international travelers reached 1,138,000,000 in 2014 with 1,600,000,000 expected by 2020. Business travelers now constitute approximately half of all international travelers. Travel patterns are changing with increased business travel to Asia and developing countries (World Tourism Organization, 2014). Business travelers travel for their occupation or work (e.g., education, research, or volunteer work) and have also been termed occupational travelers. The number of international assignees or expatriates is also rapidly increasing with a 50% increase expected by 2020.
Business travel and international assignments have been growing with the globalization of large corporations. Multinational corporations (MNCs) have expanded outside their home countries not only to produce goods at lower costs for home consumption but also to expand overseas markets. For many MNCs, international revenues have already exceeded domestic revenues (Newman, 2011). The number of countries with expatriates or assignees also continues to increase. Currently, MNCs place international expatriates or assignees in more than 20 countries on average, and the number of countries continues to grow (Druckman, Harber, Liu & Quigley, 2012). For MNCs, 95% of their consumers live outside the United States, and the growth in revenues from developing countries will drive continued globalization and the need for business travel and overseas assignments (Druckman et al., 2012, 2014).
Several categories of overseas assignments require regular business travel. The international business frequent traveler undertakes a number of trips per year to different locations focusing on management, marketing, or training. A second category of travelers is the business commuter who returns to an international facility on a weekly or monthly basis.
Many international assignees also travel regularly. Expatriates are employees with long-term assignments; employees and their families move to host countries for specified time periods (e.g., 2-5 years). Some expatriates relocate but their families remain in their home countries with frequent visitation. A group that is increasing is the short-term assignee (e.g., 4-12 months) who travels internationally for specific time to achieve limited objectives (e.g., finance managers, auditors, specialists in specified jobs). The assignee does not relocate to the site but has temporary housing, returns home on a scheduled basis, and is focused on a specific task. Studies have shown that short-term assignees are less prepared and at higher risk of adverse health events than expatriates.
Business travelers’ health and safety risks have historically been considered “low.” However, studies have shown that these risks are similar to the risks of other international travelers. In fact, in a recent study of travelers to Asia, more than 60% of high risk travelers listed a business reason for their trips (Deshpande, Rao, Jentes, Hills, & Fischer, 2014). Studies have also shown more hospitalizations and evacuations for “low risk” travelers, although the country risk level was also a predictor (Druckman et al., 2014). A study of World Bank employees showed that the overall costs to their health plan were 72% higher compared with their non-traveling counterparts. In the study, risks were increased for almost every physical disease category and mental health diagnoses; most risks were correlated with the frequency of travel (Liese, Mundt, Dell, Nagy, & Demure, 1997).
For international business trips (e.g., 10 days, 2 weeks), approximately one third of travelers develop infectious illnesses (e.g., diarrhea, respiratory) or suffer injuries. Moreover, a significant increase in the risk of high or very high mental stress was reported among business travelers. Sleep disorders and substance abuse are common. Also, non-communicable diseases showed increases similar to infectious diseases. Thus, health care costs increase for international travelers because the risks increase for accidents and injuries; the risk of death from traffic accidents increases fivefold (Bunn, 2001).
Health risks for business travelers and assignees differ from the health risks in their home countries. Infectious diseases vary widely from country to country and region to region. The diseases encountered may change rapidly and information may be outdated. Infectious diseases, not encountered in developed countries, may be significant risks (e.g., malaria, typhoid, cholera, rabies, encephalitis). In addition, increased risks of other illnesses and injuries may be related to exposures to air and water pollution, allergens, and physical (cold, heat) and chemical hazards. Accommodations for disabilities are not required in many countries (e.g., elevators, ramps), nor are protective devices (e.g., seat belts, air bags), which increase the risk of accidents and resulting injuries.
The risk of developing illnesses and being injured is compounded by the quality of health care available, particularly emergency and acute care. Emergency transportation (e.g., ambulances) may not be available. Access to health care is also challenging because many facilities are funded through a public health system; private care may be limited and have special payment requirements. Therefore, even treatment for a minor illness may not be easily available or may require significant periods away from work to seek appropriate care. For serious illnesses, quality local care may not be available, and evacuation to regional health care centers or to home countries may be necessary.
Risk reduction programs for international travelers, expatriates, and assignees have been recommended by many expert groups. Measures include screenings, health education, vaccination and prophylaxis, computerized databases with updated travel and destination health risk information, travel kits, information on best care facilities, and access information for evacuation. However, these programs are not available to most business travelers, expatriates, and assignees (Bunn, 2001).
Recent Articles on Business Travelers
Two recent articles (Bunn, 2014; Druckman et al., 2014) addressed specific issues for business travelers. The Druckman article included a review of more than 800,000 business trips and almost 1,200 cases. The article focused on hospitalizations, evacuations, and risk factors. Aggregate trips to “low risk” countries resulted in a greater number of hospitalizations and evacuations than trips to “high risk” countries. The country risk categorization was predictive for adverse events; however, the article suggested a significant risk for employees even when traveling to “low risk” countries.
The editorial by Bunn discussed the Druckman article and a 2014 article by Kogelman (Kogelman et al., 2014). The Kogelman article demonstrated that providers of travel health care often have limited knowledge of vaccines and vaccine-preventable diseases. The study showed that for rare diseases, the knowledge gap was significantly greater than for more common diseases, particularly among primary care physicians (PCPs) and offices that offer travel health care. The study also showed travel and occupational health nurses provided pre-travel consultation in 41% of travel medicine clinics; PCPs provided this service in 27% of clinics. The study compared providers’ knowledge of hepatitis A, yellow fever, and JE. Although the providers were very familiar with hepatitis (78.9%), only 18.9% of the providers were familiar with yellow fever and 9.8% with JE. Japanese encephalitis is rare, but 20% to 30% of cases are fatal and 50% of survivors have permanent neurologic sequelae. Despite a safe effective vaccine, studies have shown only 1% to 11% of at-risk groups are vaccinated and that even in GlobalEpiNet, a sophisticated consortium of travel clinics, only 28% of clients were vaccinated according to Advisory Committee on Immunization Practices (ACIP)/CDC recommendations. The most common reason for failure to vaccinate has been the failure to consider or recognize the need for vaccination despite ACIP guidelines.
These recent articles demonstrate the need to carefully review vaccine requirements prior to business travel. The responsibility for appropriate vaccination and education is not solely with a travel clinic. The referring occupational health clinic must assure appropriate vaccine prophylaxis and education is provided.
Productivity Among Business Travelers, Expatriates, and Assignees
The cost per year of an employee on overseas assignment is US$300,000 to US$400,000 on average. The cost of a failed expatriate assignment is approximately US$1,000,000; the loss of a recurrent or frequent business traveler is also high. To evacuate an employee can easily exceed US$100,000. The rate of expatriate and assignee failure is estimated to be 6% to 12%. Therefore, the direct costs of repatriation and assignment failure are high, and preventive measures can produce significant returns on investment in terms of care and repatriation costs alone (Bunn, 2001).
Effective travel programs for health, safety, and security are an expectation, and when programs are either of poor quality or absent, a loss of confidence by employees and their families can affect the entire company. Corporations, businesses, and universities are liable for tort suits due to negligence and workers’ compensation claims. Businesses also may suffer damaged public relations and corporate trust. These issues impact not only the health of the traveler but also the productivity of co-workers and the profitability of the company (Bunn, 2014).
Despite the large and growing number of international business travelers, continued globalization, increased employee health risks, limited access to quality care, and the high costs of assignment failure and evacuations, little analysis of the direct costs of clinical care or evaluation of health and productivity of these workers has been undertaken. Approximations of costs in a previous article (Bunn, 2001) suggest a significant potential return on investment, but a full analysis of direct costs is needed. The indirect costs of absenteeism, disability, workers’ compensation claims, and notably presenteeism have not been assessed. These costs will be difficult to accurately quantify. Many international health care expenditures are not included in health plans and limited data are available on wage replacement for business travelers, expatriates, or assignees.
Summary
To summarize, occupational health nurses and nurses in travel clinics provide pre-travel consultations. International business travelers are one of the largest at-risk worker groups. The health and safety risks for this group are significant and are higher for almost all categories of illness and injury, not just infections. In fact, the health risks for business travelers may exceed the risks of other travel groups (Deshpande et al., 2014).
Risk reduction programs are complex and comprehensive and must respond to changes in risk. Business travelers pose special legal risks for corporations, businesses, and universities. Studies show current programs for vaccination of business travelers are not adequate and government/ACIP recommendations are commonly not followed (Bunn, 2014). Travel vaccines and prevention programs must be aggressively offered to business travelers and their employers. Effective business travel programs will not only protect workers and their companies but also be cost-effective, particularly when lost productivity is included in the calculation.
The JE Virus: An Under-Appreciated Risk to the Business Traveler
Japanese encephalitis is a flavivirus transmitted by Culex mosquitoes, which breed on farms and in rice paddies; they bite dusk-to-dawn. This infection is common in Asia, the tropical areas year round and the temperate areas during the months of May through October. Recent evidence, however, has documented cases of JE in temperate areas of Asia outside the usual transmission months. Japanese encephalitis is endemic in a large area of Asia, and a careful review of planned itineraries or potential itineraries is necessary to accurately advise travelers about this disease (Halstead, Jacobson, & Dubischar-Kastner, 2013).
The risk of infection has been calculated at 1 in 5,000 travelers per month of stay. Risk is correlated with rural exposure in endemic areas. In addition to visiting rural and semi-rural areas, outdoor exposure between dusk and dawn, length of stay, and seasonal variation (i.e., mosquitoes becoming more active in the rainy season) are all risk factors (Hills, Griggs, & Fischer, 2010).
The effect of climate change is unclear, but areas at risk of JE appear to be increasing. A study of JE cases in Taiwan between 1991 and 2005 showed that JE cases correlated with rainfall and temperature in the previous 1 to 2 months. The peak JE transmission season had shifted from June to October to May to August. New irrigation projects and increased rice production may have increased JE transmission in some areas by increasing vector habitats.
After the bite of a Culex mosquito carrying the JE virus and an incubation period of 5 to 15 days, those individuals who develop symptoms display fever, headache, vomiting, and mental status changes leading to neurologic deficits including movement disorders. Of JE cases, 15% to 30% die and 30% to 50% of survivors have significant neurologic sequelae. The risk is highest among long-term travelers and those traveling in rural areas with extensive outdoor exposure. Specifically, individuals who travel to agricultural areas where pigs are raised are at particular risk.
The introduction of pig farming to some parts of Asia may have led to epidemics of JE. In other areas, centralization and segregation of pig farms away from population centers may have reduced human risk. For example, in Singapore, all pig farms were moved off the island and JE transmission decreased. Infections with JE by Culex quinquefasciatus, pipiens, and Aedes albopictus (all urban mosquitoes) have been observed, and there is speculation regarding their role as vectors for JE. Interestingly, the flight radius of the Culex tritaeniorhynchus is about 5 km, but they can be blown by the wind up to 500 km (Hsu, Yen, & Chen, 2008).
Economic and agricultural changes are blurring the boundaries of rural areas. Increased migration to cities has led to urbanization of rural areas, where the natural enzootic cycle exists. For example, one of the concerns with travel to Beijing for the Olympics was that many of the Olympic athletes were housed in quarters outside the city, where the risk of JE was high. Likewise, industrial corporations are building plants in areas such as Hanoi when, in fact, the plants are 45 to 60 minutes outside city limits. Climate changes and horticultural and agricultural practices have expanded urban areas and new data on JE vectors suggest that JE is an unpredictable threat.
Personal risk factors may increase the risk associated with the JE. Older age is a significant risk factor for clinical illness with the risk of neuro-invasive illness five to tenfold higher in adults age 50 and older compared with older children and young adults. Young age is also a risk factor for symptomatic illness and is associated with a higher frequency of neurologic sequelae. In a review of travelers from non-endemic countries (Hills et al., 2010), 55 cases were reviewed from 17 countries with an age range of 1 to 91, median 34 years. Eighteen percent died and 44% had mild to severe sequelae.
Personal protective measures are the first line of defense, but bed netting, screens, and insect repellants are only partially effective. Human vaccination is the best means of protection. The inactivated mouse brain-derived vaccine is no longer produced, and inactivated cell culture-derived vaccine is recommended with two doses at day zero and 28 for individuals ages 2 months to 16 years and through adulthood.
In a study of travel clinics with a database of 8,289 U.S. travelers above the age of 17, researchers collected data about travelers’ itineraries, vaccinations, and other parameters. The researchers found that only 26.8% of higher risk travelers received the JE vaccine. Despite the fact that in some cases travelers had insufficient time to receive both doses of the vaccine, the vaccine was not available, or the individual had contraindications for receiving the vaccine, the majority of high risk travelers, clinicians did not vaccinate because they deemed the JE vaccine was “not indicated” (Deshpande et al., 2014). The low vaccination rate indicates the current recommendations are not being implemented. Recently, an accelerated dosing Phase 3 blinded randomized multicenter study of 661 adults was conducted. The study showed 99% seroconversion at day 15 (7 days after the second injection) and seroconversion rates remained high after 1 year. Adverse events were similar in the accelerated and conventional dosing groups (Jelinek, 2015). Short course dosing should significantly reduce the number of travelers who do not have time to receive a second dose.
In summary, JE is an unpredictable threat for travelers. Cases show that travelers visiting for a short time, even with little or no rural exposure and outside the established transmission season, have contracted JE. Human vaccination is the best protection, and all travelers should be assessed for their risk of contracting JE.
Current ACIP guidelines for JE vaccines are narrowly focused and have not significantly changed since 1993. The guidelines recommend JE vaccine should be given to travelers who plan to spend a month or longer in endemic areas during the transmission season. The guidelines also include a “consideration” for short-term travelers with “at-risk” activities: camping, hiking, trekking, biking, fishing, hunting, or farming. The recommendations do not address business travelers or the evolving risks of JE. The 1 month criterion is arbitrary, and travel patterns and “at-risk” areas are changing. Updated recommendations are needed and should reflect current risks, be clear and concise, and always encourage health care provider–employee discussions.
A Japanese Encephalitis Vaccine Recommendations Working Group met in New Orleans in conjunction with the American Society of Tropical Medicine Hygiene (ASTMH) in November 2014. Revised recommendations were agreed upon by consensus at this meeting and included (a) a discussion of JE and availability of a safe and effective vaccine with all travelers to endemic areas of Asia; (b) travelers to rural or peri-urban areas in endemic countries, irrespective of duration of travel or itinerary, should be offered the vaccine; (c) all expatriates living in endemic countries or frequent travelers who may visit rural or peri-urban areas in endemic countries should be offered the vaccine; (d) travelers with uncertain itineraries or itineraries that may change should be offered the vaccine; and (e) the vaccine is not generally recommended if travel is restricted exclusively to urban areas.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Bonnie Rogers is associate professor and director of the Occupational Health Nursing Program in the School of Public Health at the University of North Carolina and is director of the North Carolina Occupational Safety and Health Education Research Center. She has published 200 papers and authored two books. She chairs the National Institute on Occupational and Heath Board of Scientific Counselors and the National Occupational Research Agenda Liaison Committee.
William B. Bunn is recently retired vice president of Health Safety Security and Productivity at Navistar. He now serves as a consultant/advisor and is an adjunct professor at the Medical University of South Carolina and Northwestern University. He has over 150 publications and is author/editor of five books.
Bradley A. Connor is the founder and medical director of the New York Center for Travel and Tropical Medicine. He is clinical associate professor at the Weill Medical College of Cornell University and a coauthor of the textbook, Travel Medicine, and past president of the International Society of Travel Medicine.