
Abstract
Evidence suggests that diabetes education can be delivered at the worksite to better support employees’ diabetes self-management and improve productivity and health care costs. This study was conducted to address the feasibility of a diabetes worksite education program for employees at a large urban academic health care institution. The diabetes education program was delivered in the diabetes center at the institution, a resource that was previously underutilized by employees. Through collaboration with groups in the institution, 20 employees of diverse ethnicity participated in the worksite diabetes education program with positive outcomes: improved glycemic control measured (HbA1c), attainment of self-management goals, and satisfaction with the program. Work absences trended downward, but numbers of hospitalizations and emergency department visits were unchanged in the 3 months following education. Recommendations include replication of the study with more employee participation and program evaluation over a longer period of time to continue assessment of employees’ educational needs.
Keywords
Diabetes presents one of the most serious challenges to human health and the delivery of health care. More than 29 million individuals, or 9.3% of the U.S. population, have diabetes (Centers for Disease Control and Prevention, 2014). In 2012, 1.7 million individuals aged 20 years and older were newly diagnosed with diabetes (Centers for Disease Control and Prevention, 2014). Diabetes is the leading cause of blindness, non-traumatic lower extremity amputation, and renal failure. Individuals with diabetes are 2 to 3 times as likely as those without diabetes to have coronary and cerebral vascular disease.
Diabetes complications have obvious human costs to quality of life and early death, but the disease and its related complications also represent a significant economic burden (American Diabetes Association [ADA], 2010). In 2012, the estimated direct and indirect costs associated with diabetes totaled US$245 billion (ADA, 2013). Indirect costs include absenteeism, reduced productivity, and disability. Diabetes accounts for an annual 15 million workdays lost, 120 million workdays with less productivity due to illness (presenteeism), and 107 million workdays lost to disability from diabetic complications (Boles, Pelletier, & Lynch, 2004; Centers for Disease Control Diabetes, 2014). The absenteeism rate for individuals with diabetes is 0.8% higher than for those without diabetes.
Sylvia et al. (2012) examined the relationship between work limitations and morbidity burden (severity of illness) for employees with diabetes. Work limitations were defined as functional limitations that restrict an individual’s ability to perform work responsibilities. The authors reported that the higher the morbidity burden, the more prevalent work ability impairment. According to the Medical Expenditure Panel Survey (MEPS), diabetes is one of the three leading chronic conditions causing work loss (Druss et al., 2001). Boles et al. (2004) concur noting that of all chronic diseases, diabetes had the largest proportion of lost productivity, specifically absenteeism and presenteeism.
The ADA’s 2010 position statement holds that any individuals with diabetes should be eligible for qualified employment. However, the high morbidity burden associated with this disease is a potential barrier to attaining and sustaining employment. Sylvia et al. (2012) recommended that worksite nurses not only assess and educate employees with diabetes but also provide resources for supervisors, coworkers, and administrative staff who support these employees. Nurse-led diabetes self-management education (DSME) programs have demonstrated significant positive impact on cardiovascular risk factors and HbA1c, a blood test that provides information about the average level of glucose over a 90-day period (Tshiananga et al., 2012).
According to the U.S. Community Preventive Services Task Force (2013), DSME programs in community settings, such as the worksite, need further evaluation. Previous literature examined the negative impact of diabetes on productivity and associated expenditures. However, few studies concern worksite diabetes education initiatives that aim to decrease absenteeism, hospitalizations, and HbA1c levels. No studies were found that measured reductions in hospitalizations or the attainment of the American Association of Diabetes Educators’ seven (AADE-7™) self-management goals (see sidebar).
To examine the literature about worksite diabetes education the Cochrane Library, OVID Medline biomedical journal database, CINAHL database index of nursing and research journals, and the website for the Agency for Healthcare Quality and Research were searched. Key words included employee education, diabetes, employee diabetes education, absenteeism, HbA1c, and hospitalization. To identify literature on behavioral outcomes of worksite employee education, the key word AADE-7™, for the AADE seven self-care behaviors framework, was also used. Inclusion criteria for the articles identified included publication dates from 2000 to 2014, written in English, and adult worksite interventions. Forty-three articles and one report were identified. Twenty-five articles were excluded because they referred to pediatric interventions, school education programs, or a hospital-based patient education program for inpatient or post discharge education. Thus, a total of 18 articles and one report were included in the study; these articles reported relationships among diabetes, cost and productivity, as well as worksite education initiatives to decrease absenteeism, hospital visits and HgA1c levels. Of the 18 articles, 4 described worksite education interventions for employees with diabetes. Using the Johns Hopkins Nursing Evidence-Based Practice criteria, 3 articles reported on Level II quasi-experimental studies (Burton & Connerty, 2002; Carloti, Lavigne, Stone, Tortoretti, & Chiverton, 2001; Thomas & Miceli, 2006), and 1 article was a Level III study (Dearholt & Dang, 2012; Wolf et al., 2009).
Syntheses of the evidence identified several key interventions: flexible scheduling for appointments for 1:1 or group educational sessions; provider expertise, including certified diabetic educators (CDEs), advance practice nurses (APN), or registered dieticians (RD); structured curricula; behavioral goal setting; and longitudinal monitoring that informed the development of this feasibility study. Collectively, these evidence-based interventions readily translated to this study’s population and organizational structure.
A paucity of worksite interventions included diverse populations. Most participants in the aforementioned studies were White and male. A significant gap was found in the worksite diabetes literature addressing outcomes, reducing hospitalizations and emergency department (ED) visits and attaining AADE-7™ self-management goals.
Purpose
The purpose of this study was to test the feasibility of a worksite diabetes education program in a large urban health care institution. Testing of recruitment strategies, assessing demand for the program among employees, and the outcomes of HbA1c, attainment of one AADE-7™ self-management goal, work absences, hospitalizations/ED visits, and employee satisfaction with the program were integral aspects of the program
Method
Research Design
This feasibility study was designed to test the viability and effectiveness of a targeted employee worksite diabetes education program led by CDEs at the institution. The study was approved by the University’s Institutional Review Board via expedited review. The researchers used a quasi-experimental, pretest–posttest design. Outcomes of interest included acceptability of the program to employees, demand or interest in the program, and traditional measures of HbA1c, number of days absent from work, number of hospitalizations or ED visits, participants’ self-management goal attainment, and satisfaction with the program. Participant recruitment, consent, and diabetes education program sessions occurred over a 10-week period from September 23 until November 25, 2013. Data were collected at baseline and 3 months after the intervention.
Setting
The site of the program was a large academic urban health care institution with an accredited diabetes center. The diabetes center, centrally located in the outpatient center, evaluates, educates, and manages patients with diabetes and includes a staff of five endocrinologists and fellows and four CDEs (i.e., three nurse practitioners and one registered dietitian).
The study’s educational program was based on the Center’s existing ADA diabetes curriculum and no changes were made to the curriculum for this project. The curriculum focused on nutrition, physical activity, self-monitoring of blood glucose, medication use and adherence, prevention of complications, and stress reduction and coping strategies.
Participants self-selected to participate in an individual 1-hour appointment with the CDE or one 3-hour group visit, similar to other patients at the Diabetes Center. Based on appointment availability, the participants were assigned to one of the four CDEs (i.e., nurse practitioner or dietitian). Group visits had two to three participants. The curriculum was the same regardless of visit type. Three months after the initial education, participants returned for an additional assessment and further education.
Participants
Employees were eligible to participate if they were adults currently employed by the institution, had a diagnosis of either type 1 or type 2 diabetes for at least 3 months, and spoke English or a language with available interpreter services. Employees were excluded from participation if they were pregnant, had secondary diabetes, or were deemed medically unstable by the nurse practitioner (e.g., severe hyper or hypoglycemia, dizziness).
In 2012, only 3% (n = 7 / 226) of the patients attending the diabetes education program were current employees of the institution. In a targeted effort to recruit employees, the study team contacted the institutions’ occupational health center, employee wellness group, and employee insurance plan’s case management team. Recruitment of participants occurred through these groups as well as the diabetes center, internal medicine clinic, and flyers placed throughout the institution (see Figure 1).
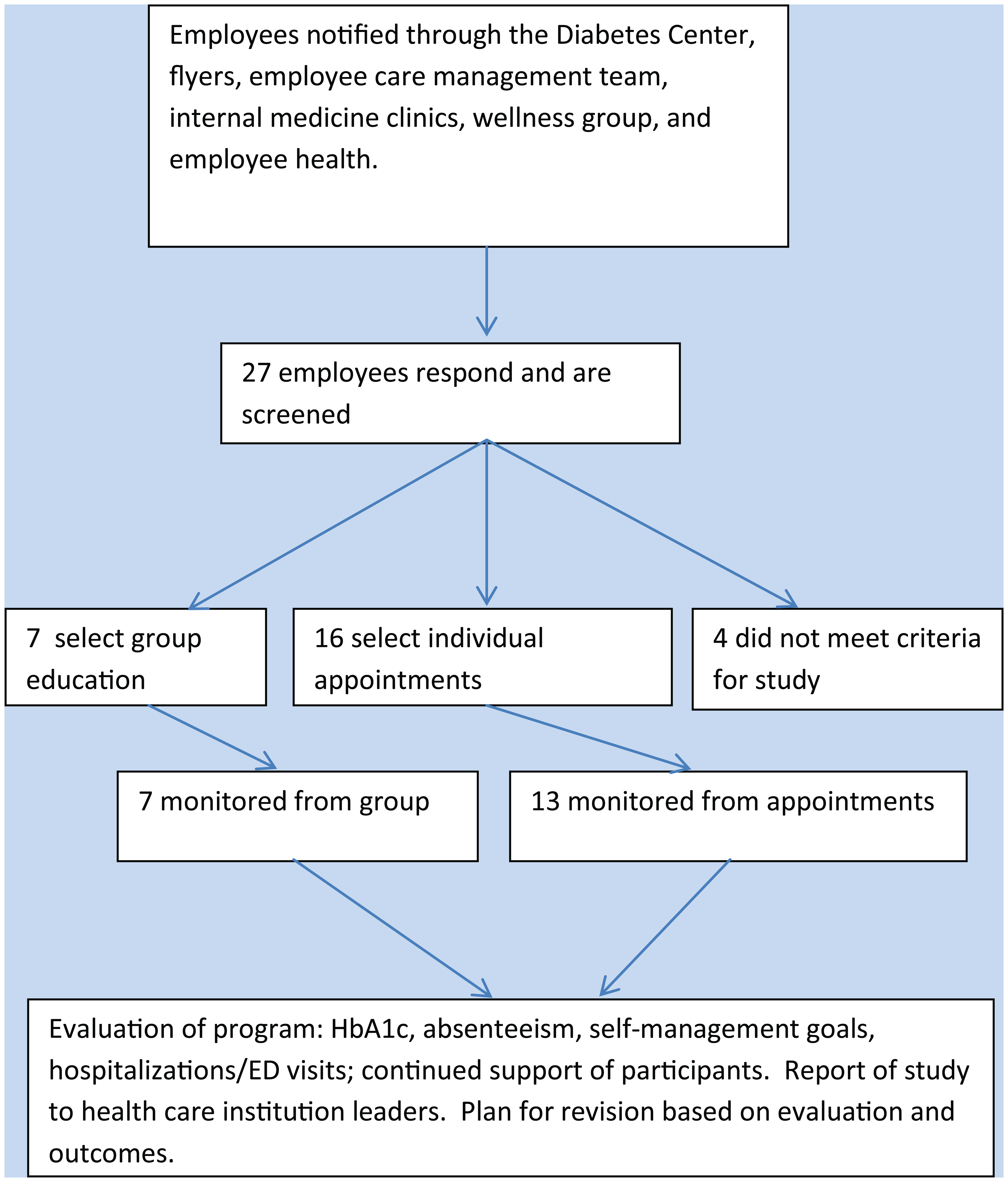
Flow of participants through education program.
Measures
Assessment form
All participants completed a standardized assessment form (i.e., preceding 3-month history of hospitalizations or ED visits, days absent from work, and recent HbA1c level either verified by laboratory report or ordered at the time of the first appointment). These data were collected again at 3 months post education.
Self-management goal
Participants were asked to choose one self-management goal to focus on over the next 3 months. Goals were based on AADE-7™ behaviors: healthy eating, being active, taking medication, monitoring blood glucose, risk reduction, problem-solving, and healthy coping/stress-management skills (AADE, 2013). After 3 months, the participant and the CDE jointly evaluated goal progress based on a percentage scale as follows: 1 = no progress (0%), 2 = making changes with minor setback(s) (25%), 3 = changes becoming habits (50%), 4 = perceived health improvement (75%), 5 = lab results indicate improvement (100%; AADE, 2013).
Evaluation
Employee satisfaction with the program was evaluated using an eight-item Likert-type scale developed by the CDEs in the diabetes center. The evaluation was optional and anonymous. On a scale of 1 to 5 where 5 indicated highest level of agreement, participants rated the following:
This course lived up to my expectations.
The content is relevant to my diabetes goals.
The course activities stimulated my learning.
The pace of this course is appropriate.
The training facility was comfortable.
The staff was professional and courteous.
The information presented on diabetes management increased my awareness of how to live a healthier life.
I would highly recommend this class to a friend.
The CDE’s teaching was effective.
Two open-ended questions asked the participants to list program improvements they would recommend and the most and least valuable part of the education program.
Statistical Analyses
Analyses were conducted using the Statistical Package for the Social Sciences, Version 21.0. Data were entered into a de-identified database. Descriptive statistics of mean, median, standard deviation, frequency, and percentage were calculated as applicable. Dependent t tests were used to compare pre- and post-education HbA1c levels, days absent from work, and number of hospitalizations and ED visits. All t tests were two-tailed, and significance was set at p < .05.
Results
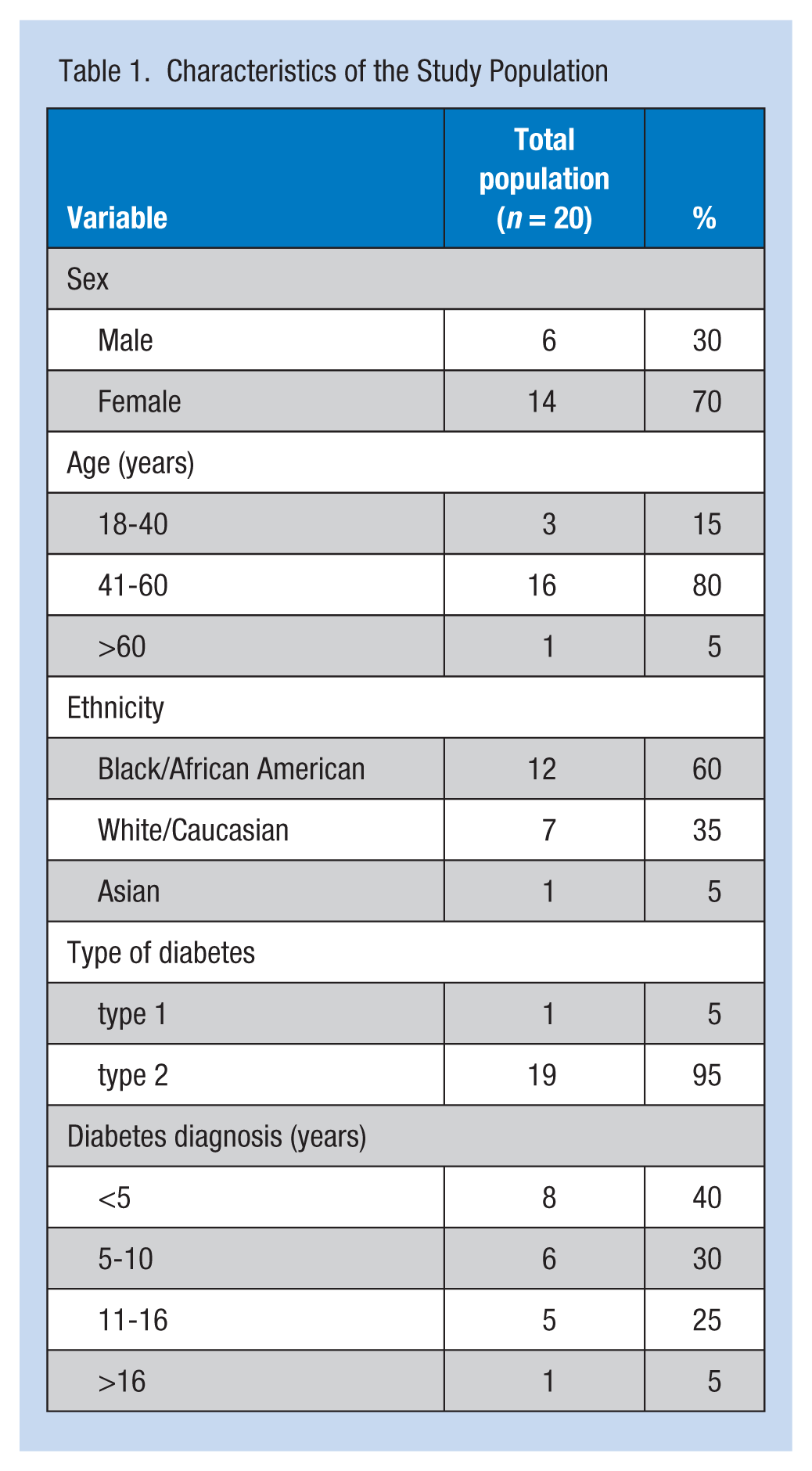
Twenty employees completed this worksite education over a 10-week recruitment period. Thirteen employees attended individual sessions and 7 attended group classes. Fourteen were female. The majority were African American (n = 12), followed by Caucasian (n = 7) and Asian (n = 1). The average age was 54 years. One participant had type 1 diabetes, and 19 participants had type 2 diabetes. The average number of years since diagnosis was 7.7 years (range = 1 to 23 years; see Table 1).
Characteristics of the Study Population
HbA1c
Seventy-five percent of participants (n = 15) reduced their HbA1c after the education. Mean HbA1c prior to the worksite education program, was 8.5 (SD = 1.8). Mean HbA1c post intervention was significantly lower at 7.5 (SD = 1.3; p = .009).
Days absent
The average number of days absent in the 3-month period preceding the education was 1.25 days (SD = 3.43 days). Three months after the education, the average number of days absent was 0.65 (SD = 1.42 days); although lower, the difference was not statically significant (p = .437).
Number of hospitalizations/ED visits
The average number of hospitalizations or ED visits during the 3 months prior to education was 0.25 (SD = 0.44). Three months after education, the average reported hospitalizations or ED visits was not significantly different at 0.20 visits (SD = 0.41; p = .716).
Attainment of a self-management goal
Participants chose one self-management goal and were evaluated on progress toward that goal 3 months after education. Evaluation was based on the perceptions of the participant and the CDE. Eight participants chose risk reduction goals, five healthy eating, three being active, three monitoring, and one taking medications. Eighty-five percent of the participants achieved at least 50% of their goal. Eight participants reached 100% of their goal, five reached 75% of their goal, four reached 50% of their goal, two reached 25% of their goal, and one made no progress during the 3 months following the education intervention (see Figure 2).
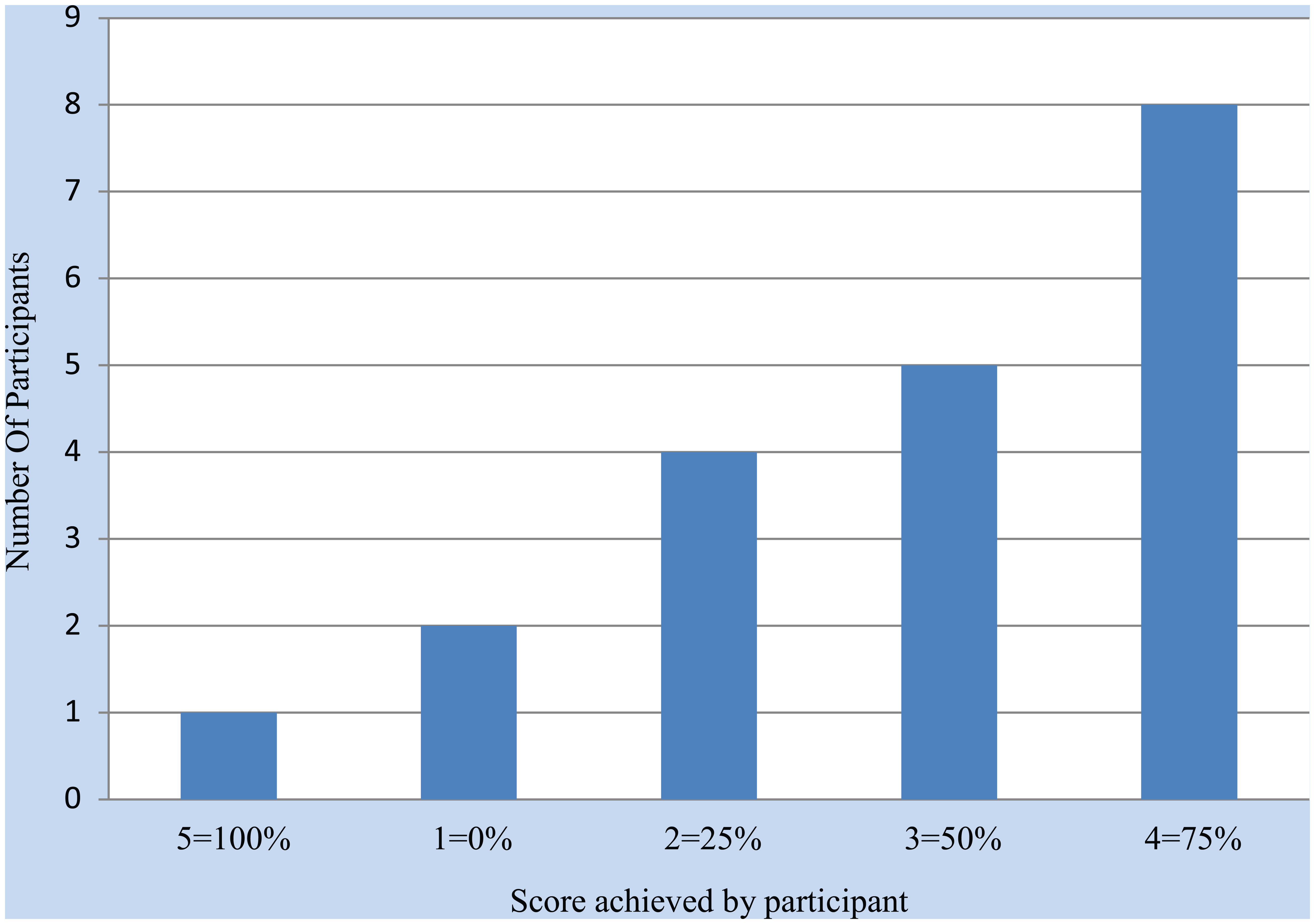
Attainment of self-management goal at 3 months.
Education evaluation
Seventeen participants submitted anonymous evaluations of the education. All rated the education at the highest score on the 7-point Likert-type scale indicating the highest level of agreement. Comments to the open-ended questions included “The class should be longer,” “Provide snacks,” “Make all diabetic employees do this,” and “All information is helpful.”
Discussion
A paucity of literature concerning worksite diabetes education initiatives that target diverse populations and aim to decrease absenteeism, hospitalizations and ED visits, and HbA1c levels was found. No previous studies of worksite diabetes education were found that addressed the outcomes of fewer hospitalizations and ED visits or attainment of AADE-7™ self-management goals. Studies identifying employees with diabetes (Gulley, Boggs, Mullins, & Brock, 2014) or work limitations related to diabetes (Sylvia et al., 2012) recommended employee education.
Employers have a compelling interest in maximizing employee wellness, particularly for employees with chronic diseases. Diabetes represents the chronic disease with the highest incidence of morbidity burden (Druss et al., 2001). Of all chronic diseases, diabetes is most likely to affect productivity, specifically absenteeism and presenteeism (Boles et al., 2004).
It is therefore striking that a large academic medical center with an existing diabetes center provided education to only 7 employees in 2012. With little effort and 10 weeks of targeted recruitment, 20 employees participated in the Diabetes Center’s education program. This finding suggests both interest on the part of the employees and that recruitment strategies that engage multiple stakeholders are successful. Next steps will focus on formalizing and sustaining these recruitment strategies through the institution’s occupational health center, employee wellness group, employee insurance plan case management team, diabetes center, and flyers placed throughout the institution.
Employees who attended the worksite diabetes education program demonstrated improvements in HbA1c and their ability to attain diabetes self-management goals. Seventy-five percent of the participants improved their HbA1c, and 85% reached at least 50% of a chosen self-management goal over 3 months. The HbA1c reduction was similar or better than many other interventions to control HbA1c (Sherifali, Nerenberg, Pullenayegum, Cheng, & Gerstein, 2010). Although previous worksite diabetes education studies have shown improvement in HbA1c (Agency for Healthcare Research and Quality [AHRQ], 2009; Burton & Connerty, 2002; Thomas & Miceli, 2006; Wolf et al., 2009), to the authors’ knowledge, this is the first study to report on employee attainment of self-management goals. Affecting self-management goals is consistent with the AADE recommendation that the best way to affect behavior change in diabetes patients is through the use of behavioral goals (AADE, 2013).
Participants in this feasibility study were representative of an ethnically diverse employee community. This sampling differed from previous worksite-based studies where the majority of participants were Caucasian (AHRQ, 2009; Burton & Connerty, 2002; Carloti et al., 2001; Thomas & Miceli, 2006; Wolf et al., 2009). Employees expressed a high rate of satisfaction with their education. Thus, this study suggests the ability of the CDEs at the diabetes center to demonstrate culturally competent diabetes education and adds to employee health knowledge of worksite diabetes education for minority employees.
Employees with diabetes have higher health care costs, lower productivity, and more absenteeism (ADA, 2012; Centers for Disease Control and Prevention, 2014). The study design, duration, and lack of statistical power limit the interpretation of outcomes that measure absenteeism and hospitalizations/ED visits; however, preliminary results suggest that the numbers of days absent trended downward. The study would be strengthened by a study design that addressed effect size and randomization and included additional measures of presenteeism and the effects of the worksite program on this outcome.
The relationship between absenteeism, presenteeism, and need for hospitalization is complex. As an example, one employee participant required a total knee replacement secondary to severe arthritis, but was unable to schedule surgery due to poor glucose control (HbA1c of 8.7%). After the diabetes worksite education, the employees’ HbA1c was controlled at 7% and she was able to schedule surgery. Her surgery resulted in absenteeism and a hospitalization. However, the surgery may also result in long-term improvement, including less presenteeism in the workplace.
Notable study limitations included the following:
The one-group quasi-experimental pre- and posttest design limits the generalizability of the results.
The lack of statistical power due to the small number of participants limits the researcher’s ability to detect significant differences.
The short period of 10 weeks from education intervention to evaluation does speak to short-term changes but not whether these changes were sustained over time.
Lack of online education or social media and education sessions were limited to one visit. Nonetheless, this feasibility study found promising results for this group of employees with diabetes.
Implications for Practice
Preliminary results suggest that a worksite diabetes intervention, based on the ADA standards and delivered by CDEs, shows promise. The number of employees who have diabetes is continuing to increase. An on-site, readily accessible, employee-centered diabetes educational program provided by CDE’s brings evidence-based diabetes care directly to employees at the worksite. Other forms of education delivered by CDEs such as web-based, other online, or social media should be further investigated.
In any workplace with employees who have diabetes, an assessment of available diabetes education and support resources is crucial. Also, the occupational health nurse should assess employee awareness and use of workplace resources. In a health care institution, diabetes education may be available for the employees, but underutilized as it was at this site. In non-health care settings, employees without direct access to diabetes education may be directed to existing community resources in close proximity, or programs could be developed by collaborating with employee health services. As was found in this study, existing organizational structures and communication channels within organizations are effective and easily accessible methods to promote worksite education initiatives. Relationships with these organizational structures (i.e., occupational health, employee wellness groups, and insurance case management teams) are highly effective and should be fostered and maintained.
This feasibility study describes the outcomes of a worksite diabetes education program at a large urban health care institution. An underutilized resource was promoted to employees, and participants were successful in improving diabetes self-management. The program served employees of varying ethnicities and was representative of the population with the greatest risk for diabetes and its complications. In a large institution with a diverse employee population, worksite diabetes education must be flexible and adaptive to meet the needs of culturally diverse participants.
HbA1c levels were reduced in the participants at levels similar to other evidence-based interventions. In addition, participants were successful in attaining self-management goals in just 3 months. With any employee education initiative, evaluation is crucial to direct improvements, maximize benefits, measure effectiveness, and demonstrate flexibility to changing needs. Diabetes outcomes of HbA1c and self-management goal attainment could reflect program efficacy in improving employees’ diabetes control and should be measured within a few months of the initial education. Because diabetes results in decreased productivity and absenteeism, outcomes such as days absent, presenteeism, and hospitalization should be measured longitudinally, beyond the 12-week period described in this study
Furthermore, because this diabetes center serves a heterogeneous population, development and evaluation of education specific to cultural needs is an important next step. Finally, future studies should include refinement of outcome measures, a larger sample size, evaluation of outcomes beyond 3 months, and testing at additional worksites. Characteristics of employees who choose or do not choose to attend worksite diabetes education, how those at the highest risk can be engaged in worksite education programs, and other methods of education and support also warrant further study.
Employee-based worksite diabetes education represents a win-win for employees, employers, and insurers. Although this feasibility study was based on a quasi-experimental design and not statistically powered, preliminary results suggest a clear demand for employee worksite-based diabetes education that provides opportunities to affect and improve employee health outcomes.
Applying Research to Practice
The AADE-7™ self-management goals are described in patient-centered behavioral terms:
Healthy eating,
Being active,
Taking medication,
Monitoring blood glucose,
Risk reduction,
Problem-solving, and
Healthy coping/stress-management skills (AADE, 2013).
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Susan Renda, DNP, ANP-BC, CDE, has a joint appointment at Johns Hopkins University with the School of Medicine as a nurse practitioner and ADA program coordinator for the Johns Hopkins Diabetes Center, and as faculty with the School of Nursing. Her clinical and research interests include improving care and management of diabetes and increasing access to diabetes education.
Marianne Baernholdt, RN, MPH, PhD, FAAN, is the Director of the Langston Center for Quality, Safety, and Innovation and Nursing Alumni Endowed Distinguished Professor, School of Nursing at Virginia Commonwealth University. Her research focuses on how quality of care is defined and factors affecting quality of care in rural areas.
Kathleen Becker, DNP, ANP-BC, is an assistant professor at the Johns Hopkins School of Nursing. She coordinates the Adult Geriatric Nurse Practitioner Program. Her clinical and research interests include provision of primary care services to complex community dwelling under-served populations and development of interprofessional practice.