
Abstract
Few studies have assessed the effectiveness of competitive incentivized worksite weight loss programs. Scale Back Alabama (SBA) is a free, state-supported program designed to promote weight loss among overweight and obese citizens. The purpose of this manuscript is to describe the design and preliminary findings of SBA as a worksite intervention among employees at a collegiate institution and university hospital. In teams of 4 employees, SBA participants volunteered to engage in a 10-week competitive weight loss contest; both teams and individuals who lost significant weight were eligible for randomly drawn cash incentives. Trained staff objectively measured participants’ weight before and at the conclusion of the contest. Preliminary analyses suggest that SBA as a worksite program can promote weight loss among employees, but future analyses are warranted to understand the context of these findings and determine if current results are confounded by unmeasured factors.
Keywords
Obesity remains a public health challenge for the United States. Recent estimates suggest that approximately 33% of U.S. adults are obese (Ogden, Carroll, Kit, & Flegal, 2014). It has been well-documented that weight loss can reduce the incidence of cardiovascular disease, diabetes, hyperlipidemia, and mortality (Whitlock et al., 2009). The southern region of the United States has historically been challenged by the obesity epidemic (Wang & Beydoun, 2007).
In a statewide effort to mitigate obesity prevalence, the Alabama Department of Public Health (ADPH) in collaboration with organizations, including hospitals around the state and supported by Blue Cross and Blue Shield of Alabama, hosted the Scale Back Alabama (SBA) worksite weight loss contest, a social marketing and public awareness campaign. In 2014, SBA was in its seventh year of existence, had won awards for its success in motivating weight loss among program participants, and enrolled a total of 25,352 participants in a statewide contest, of which 5,908 participants lost at least 10 pounds. SBA’s 2014 successes resulted in an estimated total of 114,511 pounds lost statewide among participants (Blackmon, 2014).
The results from SBA suggest that human interactions are an important factor in promoting significant weight loss (Forbus & Synder, 2013). However, existing wellness programs require evaluation using sound scientific methodology (Goetzel & Ozminkowski, 2008). In this study, the authors evaluated the effectiveness of SBA, a competitive weight loss contest, at a large university and affiliated hospital worksite. Prior to this study, the impact of SBA had not been evaluated.
Planning
SBA is a 10-week social marketing and public awareness healthy weight campaign hosted during the spring of every year in Alabama. The aim of the contest is to motivate adults to exercise and have fun losing weight. Each participating organization’s designated staff measures participants’ weekly weights in pounds. Team and individual cash prizes are awarded to various participants. To be eligible for the statewide random drawing for an individual prize, participants must lose at least 1 pound (five $50 prizes) or at least 10 pounds (one hundred $100 prizes) by the end of 10 weeks. To be eligible for the statewide three-team prize random drawings, each member of a four-member team must lose 10 pounds in 10 weeks (the first team drawing $1,000 per team member, the second team drawing $500 per team member, and the third team drawing $250 per team member). Team prize winners are not eligible for individual prizes.
ADPH provided the university’s office of employee wellness staff with program rules and the scheduled dates to measure weights. Employee wellness staff recruited volunteer coordinators from the worksite via the ADPH website. These employees volunteered to be weighed on scheduled dates at various sites across the worksite campus. Staff promoted SBA using website and print (e.g., institution’s weekly newsletter, campus electronic billboards) advertising. Staff secured calibrated scales and taught designated volunteers standard confidential weigh-in and tracking procedures to assure measurement accuracy. Volunteer coordinators were responsible for managing weigh-in sites and tracking participants’ weights. They manually recorded participants’ weights on a form and then transferred participant data to an excel spreadsheet and entered the data into the ADPH SBA database after weigh-in or weigh-out sessions. Weigh-in and weigh-out were defined as measuring participants’ weight at SBA’s inception (or weekly) and at the end of the program, respectively.
Method
Staff conducted a retrospective cohort study using data from a convenience sample of employees who participated in this worksite weight loss contest. Each year, employees, family members and community members 19 years and older are invited to form teams of four members to compete in the weight loss social marketing public awareness contest. Motivated teams competed for cash prizes to lose the most weight over 10 weeks. Between 2011 and 2013, about 3,007 visits for weigh-ins were recorded. To be considered for the study, participants were required to be (a) adults 19 years or older and (b) screened at the university or its affiliated hospital for weigh-in and weigh-out.
Implementation
Staff registered with the ADPH and volunteered to be a SBA weigh-in site. Each year, weigh-in was implemented as planned and each team was given a schedule of SBA-designated dates and several convenient locations for weigh-in and weigh-out. The Wellness Director coordinated and supervised the program. Program kick-off was held the first week in January and weigh-out was scheduled for the second week in April.
Staff used the SBA weigh-in site coordinator tool kit, which included fact sheets, promotional emails, suggested activities, and team registration forms. All information collected was confidential.
Data Analysis
The authors received the de-identified weights (pounds) collected by the Wellness Program director and staff for years 2011 to 2013. Sequential numbers were applied in a spreadsheet by the wellness center staff to track participants’ weights at baseline and at the end of 10 weeks for 3 years. After institutional review board (IRB) approval, de-identified weights and year of visit were analyzed using SAS.
During the 3 years, 3,007 weigh-in visits were recorded. However, only individuals with valid, non-missing weight measurements at both time points (baseline and post weight loss) were included in the analyses. Implausible weight values were not included in the analyses. The authors anticipated implausible values and hypothesized these values might be due to data entry errors (n = 7). Therefore, the final sample size was 2,432 visits: 958 visits in 2011, 623 visits in 2012, and 851 visits in 2013. Descriptive statistics such as means, standard deviations, frequencies, and proportions were calculated. The distribution of weight change was determined to be non-normal based on stem-and-leaf plots, normal probability plots, and the Kolmogorov–Smirnov test. Comparisons of participants’ weight change were calculated by year using the exact Wilcoxon signed-rank test. Statistical tests were two-sided and applied a significance level of p < .05.
The researchers analyzed the data for each year separately. Longitudinal analyses across the 3 years were not attempted because study data were only collected for 10 weeks each year; no further contact with the participants after the 10-week study period was attempted; specific individuals who participated in the study varied widely for each of the 3 years; and some individual participants each year did not have valid, non-missing weight measurements at both time points. In addition, the researchers were not able to use any adjusted analyses because the participant demographic variables and clinical variables were not observed or measured as part of the study protocol.
Results
The average weight loss by participants was 3.57 pounds (SD = 5.83) in 2011, 8.27 pounds (SD = 6.94) in 2012, and 3.16 pounds (SD = 5.54) in 2013. The mean weights at weigh-in and weigh-out for each year are displayed in Figure 1. A significant difference in weight loss for all 3 years was calculated (2011, p < .001; 2012, p < .001, and 2013, p < .001). The authors compared weight change by year and categorized the weights into three categories to describe the weight lost. The distribution of weight loss during the 10 weeks of the weight loss contest for 1 pound and less than 5 pounds was 13.36% (128), 20.71% (129), and 10.81% (92) for the years 2011, 2012, and 2013, respectively. A similar pattern of weight loss was found for the 5 pounds and less than 10 pounds category: 13.05% (125), 29.37% (183), and 12.34% (105) for the years of 2011, 2012, and 2013, respectively. The largest proportion of weight loss was observed in the 10 pounds or greater category: 18.27% (175), 38.84% (242), and 15.75% (134) for the years 2011, 2012, and 2013, respectively. The percentages of participants who lost 1 pound or less each year between 2011 and 2013 at this worksite location was 59.19%, 12.84%, and 63.10%, respectively. Many participants lost at least 1 pound or more over the 10-week period: 44.68% (438) in 2011; 88.92% (554) in 2012; and 38.9% (331) in 2013. Of note, many participants did not weigh out in 2012 because the prizes were awarded that year to only those participants who lost 10 pounds or more. In 2013, the competition was changed and prize drawings were offered to those participants who lost at least 1 pound and weighed out. For example, in 2012, if participants did not lose at least 10 pounds, they had little motivation to weigh out, even if they lost 7 or 8 pounds.
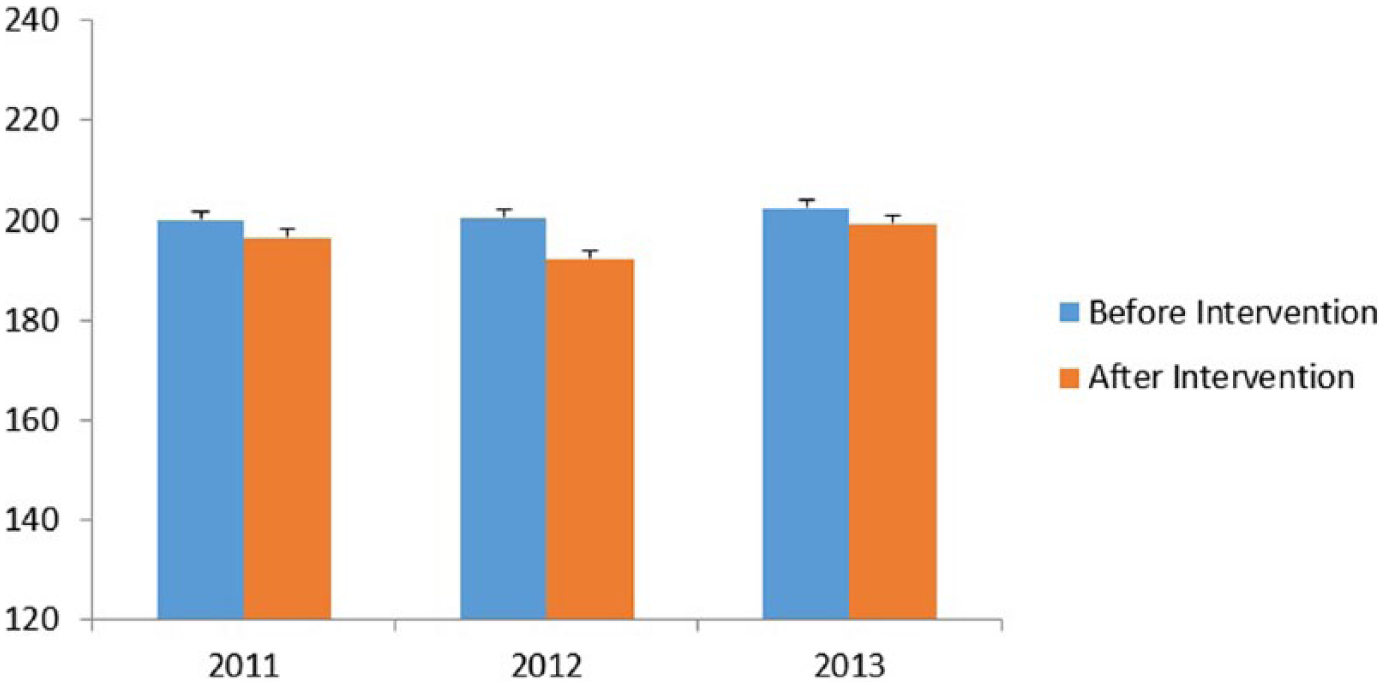
Weight of participants before and after intervention.
Discussion
The purpose of SBA is to encourage weight loss among citizens of Alabama at risk for obesity, and do so in a way that they perceived to be fun. Preliminary evidence suggests that SBA was effective in promoting weight loss among residents in a region of the United States that historically has a high prevalence of obesity. Findings from this pre- or postintervention analyses using objectively measured weight indicated that at least 16% of participants lost 10 pounds or more each year in total body weight. These findings are consistent with similar statewide weight loss campaigns (Leahey, Kumar, Weinberg, & Wing, 2012). This study’s findings suggest that SBA as a worksite incentive program may be more effective than other worksite weight management programs because these other programs often produce only modest weight loss (Roberts & Krebs, 2012).
A recently published literature review suggested that standard worksite weight loss programs often use only physical activity, diet, and education interventions (Ausburn, LaCoursiere, Crouter, & McKay, 2014). The social influences of a team-based weight loss intervention and provisions of incentives are two components of SBA’s intervention that distinguishes it from standard weight loss programs. Previous findings provide evidence that individuals’ social networks can encourage health-protective behaviors related to weight loss (Gabriele, Walker, Gill, Harber, & Fisher, 2005; Leahey, Gokee LaRose, Fava, & Wing, 2011; Leahey et al., 2012). Although not directly assessed in this analysis, it is a distinguishing component of SBA.
Another important aspect of SBA is the incentives. The literature suggests that weight loss incentives are effective in achieving weight loss goals (Finkelstein, Linnan, Tate, & Birken, 2007; John et al., 2011; Volpp et al., 2008). Relevant to SBA, team incentives are suggested to be more effective at producing weight loss among participants compared with individual incentives (Kullgren et al., 2013). Future studies should randomize team assignments among a subpopulation of participants and provide varied cash incentives at differing intervention sites to determine the true magnitude that social influence and incentives have on SBA results.
Limitations
This study had two primary limitations. First, no control group was established, and various covariates (e.g., socioeconomic status, sex, race, etc.) were not included in the analysis. As such, the researchers cannot report with confidence that study results are free of confounding. The authors believe that the low attrition rate was not only due to SBA’s offered incentives, but also because not soliciting various covariates in this survey increased participants’ anonymity and odds that they would remain in the program at weight out. Given the program’s findings, future evaluation of SBA should include key covariates with sampling procedures to account for participants who may be lost at follow-up and participants who may wish to avoid survey questions addressing important covariates (e.g., socioeconomic status). Second, due to the cross-sectional nature of the research design, it was not possible to determine whether participants maintained weight loss over the 3 years of the study. However, knowing that study findings suggest that SBA might be effective at producing weight loss, future analyses should address these limitations to better understand the context of the findings.
Study limitations were balanced by several strengths. First, the outcome (i.e., weight) at both pre- and postintervention was objectively measured and not self-reported. Second, data analysis will be used for SBA quality control purposes so that future program modifications are based on sound scientific rationale.
Evaluation
This worksite weight loss incentive program intervention of weigh-in and weigh-out was relatively easy to manage without being wellness staff intensive. SBA was a creative way to engage employees in significant weight loss each year for three consecutive years. Measuring the outcome of weight loss among groups competing for prizes, regardless of method used to lose weight, motivated many employees to lose at least 10 pounds within 10 weeks.
In Summary
As a cost-effective population-level weight loss intervention, preliminary results suggest that SBA has promise.
SBA’s effectiveness in motivating participants to lose a significant amount of weight (10 pounds) in 10 weeks and for 3 consecutive years warrants further investigation.
To gain a deeper understanding of SBA’s results, program interventions should be tailored for various settings in the future.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (Grant UL1 TR000165). Dr. Oster reports grants from the National Center for Advancing Translational Sciences/NIH (Grant UL1 TR000165), National Institute of Diabetes and Digestive and Kidney Diseases (P30DK056336), National Heart, Lung, and Blood Institute (T32HL007457), during the conduct of the study. Dr. Lewis Jr. reports grant support from the National Institute of Diabetes and Digestive and Kidney Diseases (P30DK056336) and grant support from the National Heart, Lung, and Blood Institute (T32HL007457), during the conduct of the study. Dr. Breaux-Shropshire reports grant support from the National Heart, Lung, and Blood Institute (T32HL007457) and Veterans Administration Quality Scholars, during the conduct of the study.
Author Biographies
Tonya L. Breaux-Shropshire is a Veterans Administration Quality Scholar Fellow, and Adjunct Faculty, University of Alabama at Birmingham School of Nursing Community Health, Family, and Outcomes. Her research interests are resistant hypertension, medication adherence, obesity, hypertension self management, health disparities, quality and safety metrics and measurement.
Lauren Whitt is the Wellness Coordinator, University of Alabama at Birmingham Wellness Center, Birmingham Alabama.
Robert A. Oster is an associate professor in the Department of Medicine, Division of Preventive Medicine, and is Co-Director of the UAB Center for Clinical and Translational Science Biostatistics, Epidemiology, and Research Design Program. His area of expertise is biostatistics.
Dwight Lewis Jr. is a postdoctoral fellow at The University of Alabama at Birmingham.
Toneyell S. Shropshire is a doctoral physical therapy student at Louisiana State University Physical Therapy program in New Orleans Louisiana.
David A. Calhoun is Professor of Medicine at the University of Alabama at Birmingham, Vascular Biology and Hypertension Program. He has published over 150 papers and book chapters related to hypertension. His research interest has been primarily to identify mechanisms of resistant and refractory hypertension.