
Abstract
The objective of this study was to evaluate the effectiveness of a brief, office-based educational intervention to increase parent or patient recognition of the early warning signs and symptoms of diabetic ketoacidosis (DKA). Forty-two patients aged > 13 years and 34 parents of children aged ≤ 13 years were given a pretest questionnaire about their knowledge of signs and symptoms of DKA and sick day management practices. They received a brief refresher course on sick day management specific to their treatment modality (pump vs. injection) and were given a take-home flow sheet of guidelines for diabetes sick day management. Subjects were retested with the same knowledge questionnaire after 6 to 12 months. Patients or parents scored higher on the posttest than the pretest and called the emergency line for assistance more frequently (p = .032) following the intervention. Emergency department visits were significantly reduced in adolescents (p = .024). A short educational intervention and printed management tool is effective in improving sick day and DKA knowledge and appears to be effective in reducing emergency department visits by increasing utilization of a diabetes emergency line for early outpatient intervention.
Keywords
Introduction
Diabetic ketoacidosis (DKA) is a leading cause of morbidity and mortality in young people with type 1 diabetes (T1D; Miller et al., 2015), being responsible for approximately 50% of the deaths in people with diabetes under 24 years old (Bismuth & Laffel, 2007; Laffel, 2000), and over 75% of deaths in women with diabetes under age 30 years (Ellis et al., 2008; Realsen, Goettle, & Chase, 2012). In addition, the financial burden of DKA on the health-care system is quite substantial; treatment of a single episode of DKA costs about US$11,000 and the total cost of all episodes of DKA in the United States in 2004 was more than US$1.8 billion (Bismuth & Laffel, 2007; Realsen et al., 2012). While the incidence of DKA in patients with undiagnosed diabetes is relatively difficult to impact, the majority of patients with DKA have known diabetes. It is estimated that up to 50% of these cases of DKA may be preventable with appropriate education to facilitate early identification and treatment (Bismuth & Laffel, 2007). Such a reduction in emergency department (ED) visits and hospital admissions for DKA would have enormous public health implications (Centers for Disease Control and Prevention, 2014).
There are several examples of successful DKA prevention programs that have been implemented in the experimental setting, including an extensive primary prevention program in schools in Parma, Italy (Vanelli et al., 1999). This and other similar DKA prevention programs focused on patient education about sick day guidelines, as well as 24 hour or 7 days per week availability of on-call physicians (Kaufman & Halvorson, 1999), multisystemic family psychotherapy (Ellis et al., 2008), or creation of Care Ambassadors to help guide families through the challenges of T1D care (Laffel, Brackett, Ho, & Anderson, 1998). While these interventions were successful in reducing incidence of DKA or frequency of hospitalizations, they required multilevel changes in practice and extra funding for additional staff members to carry out the programs. These are among the reasons why the results of clinical trials of DKA prevention programs have been difficult to translate into clinical practice. Thus, there remains a need for new educational programs for reducing the incidence of DKA that can be implemented quickly in a busy practice setting without necessitating increased funding or allocations of time.
The objective of our study was to evaluate the effectiveness of a brief educational intervention and printed teaching tool to increase patient or parent knowledge regarding the recognition and management of the early signs and symptoms of ketosis. We hypothesized that patients or parents would retain the information covered in the intervention’s educational module and use the home guide for illness management. Moreover, early recognition and treatment might, in turn, lead to earlier and more effective management of ketosis and reduce ED visits.
Methods
Study Design
This was a pre–post intervention study, whose primary aim was to assess the efficacy of an in-office educational module on diabetes sick day management which aimed to improve knowledge about DKA and how it should be treated in pediatric patients with T1D aged 2 to 22 years. Important secondary outcomes included changes in the number of ED visits, the number of calls to the emergency line, and HbA1c levels. Inclusion criteria included having a diagnosis of T1D and being treated by one of the pediatric providers at the clinic. Exclusion criteria included patients who did not comprehend written and spoken English. There were no inclusion or exclusion criteria related to duration of diabetes, as the goal was to apply the program throughout the entire clinic population.
Subject Recruitment
Subjects were approached while waiting for their regularly scheduled diabetes management visits, either in the waiting room or in the exam room. The study was explained, and they were given the opportunity to participate; no compensation was offered for participation in the study.
Initial Knowledge Assessment
Subjects who agreed to participate in the study were given a preintervention questionnaire comprised of multiple choice questions about DKA and sick day diabetes management (Supplementary Material). The questions were divided into “skills” and “understanding” subsets to reflect skills in managing diabetes during sick days and knowledge of the proximal causes of DKA. Two different versions of the questionnaire were administered, one reflecting multiple daily injection regimens and one reflecting insulin pump regimens. The surveys required approximately 5 to 10 minutes to complete and were completed by the patient if they were over the age of 13 years or by the parent if the child was 13 years of age or younger.
Education Intervention
During the clinic visit, diabetes clinicians (physicians, advanced practice nurses, or certified diabetes educators) reviewed sick day diabetes management guidelines with the patients or parents, and families were sent home with a printed algorithm of sick day management instructions with magnetic backing that could be placed in a convenient location, such as a refrigerator door (Figure 1(a) and (b)). The review of sick day guidelines required another 10 minutes to complete.
(a) Algorithm for patients managed with (a) an insulin pump and (b) injections. BG = blood glucose. NPH = Neutral Protamine Hagedorn.
Clinical Data
Additional information on the use of the diabetes emergency line and the number of ED visits during the year prior to the intervention were collected by self-report from the patient and family. Frequency of emergency line calls was assessed by self-report as ≤ 1 per year, monthly, or > 1 per month. Gender, age, duration of diabetes, age at diagnosis of diabetes, and current hemoglobin A1c (HbA1c) levels were recorded from the medical record. ZIP codes were collected from the medical record as well, and the median income of that ZIP code was recorded as a proxy for socioeconomic status.
Effectiveness Evaluation
All but 3 of the 79 subjects who completed the initial questionnaire also agreed to complete the postintervention evaluation, which was administered 6 to 12 months later. The postintervention questionnaire consisted of the same knowledge and skills questions as the initial knowledge assessment. In addition, subjects were queried about the use of the emergency call line and ED visits during the postintervention period. HbA1c levels were recorded from the medical record. If the subject had turned 13 in the period between the two visits, the parent (who had filled out the initial questionnaire) filled out the follow-up questionnaire.
Data Analyses
Descriptive statistics, univariate analyses, and pre–post comparisons were performed using SAS (version 9.4, SAS Inc. Cary, NC). Paired t tests and Wilcoxon signed-rank tests were performed for the parametric and nonparametric values, respectively, to see whether there was any significant difference before and after the intervention. The emergency call line use data were analyzed using a χ2 test for trend. The results were dichotomized into those patients who were greater than 13 years of age (who had completed the questionnaires themselves) and those patients who were 13 years of age or younger (whose parents had completed the questionnaires). Additional exploratory analyses were conducted to inform potential next steps in this research, despite potential limitations in sample size.
Results
Preintervention Baseline Data in Youth Who Participated in the Study.

Note. HbA1c = hemoglobin A1c.
Change in Questionnaire Scores and ED Visits After Intervention.
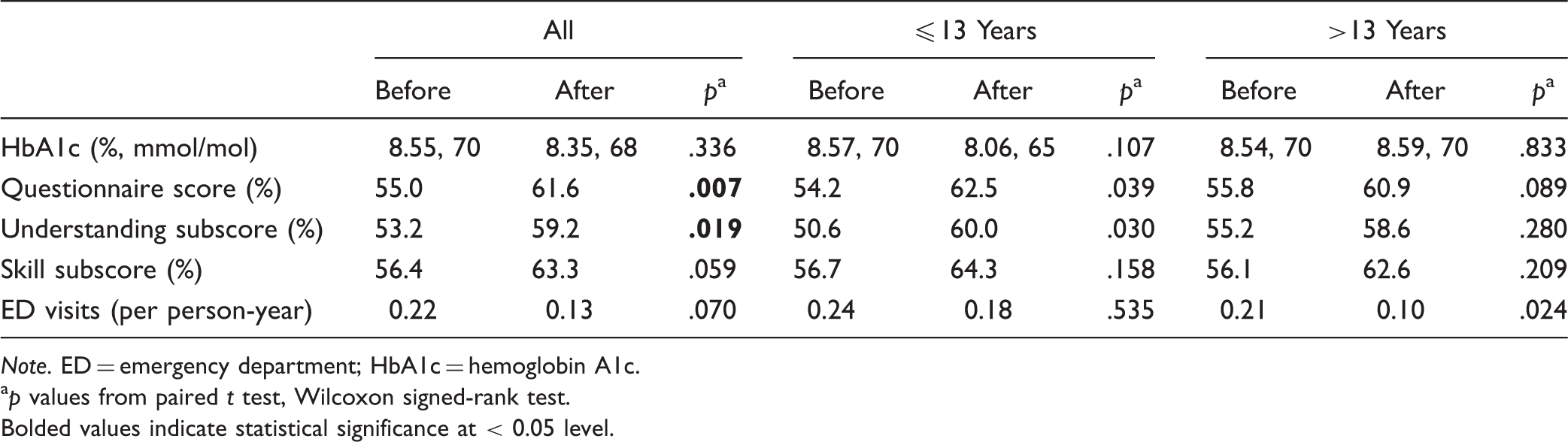
Note. ED = emergency department; HbA1c = hemoglobin A1c.
ap values from paired t test, Wilcoxon signed-rank test. Bolded values indicate statistical significance at < 0.05 level.
While there was a trend for a reduction in the frequency of ED visits after the intervention in the group as a whole (Table 2, p = .07), the difference was significant in the > 13-year-old group (p = .024) but not in the parents of younger subjects (p = .535). The use of the emergency call line was also greater after the intervention, especially in the older subjects (p = .04). HbA1c levels did not change significantly after the intervention in the whole cohort or in the two age groups (Table 2).
Discussion
Due to the all too frequent occurrence of potentially preventable episodes of DKA in patients with established T1D, clinicians in our Pediatric T1D Clinic program developed a relatively brief DKA recognition and sick day management intervention that was readily integrated into regularly scheduled clinic visits of our patients and their parents. This study was designed to determine whether the intervention was successful in improving knowledge of the early warning signs and symptoms of DKA (the primary outcome of the study), as well as encouraging the more frequent use of the emergency on-call telephone line to seek assistance in management. We anticipated that both of these factors might reduce the number of visits to the ED for treatment of DKA.
It is particularly encouraging that the results of the study were as good or better than expected: The intervention successfully increased knowledge and understanding of how DKA develops and should be treated, utilization of the emergency line increased (Figure 2), and the frequency of ED visits tended to be reduced, especially in adolescents. These results indicate that subjects retained the information that they learned and applied it in recognizing their own diabetes sick days and calling the emergency line first rather than going directly to the ED. It is particularly gratifying that the results of our study were similar to several previous DKA prevention studies, even though our intervention was integrated into regular clinic visits and did not require special Care Ambassadors (Laffel et al., 1998) or extra personnel to deliver multisystemic psychotherapy to patients and families (Ellis et al., 2008).
Frequency of calls to the emergency line before and after the intervention.
We observed that the increase in the use of the emergency on-call line and the decrease in the ED visits were greatest in the > 13-year-old group. Directing the intervention at the teenagers rather than just their parents appears to have made these adolescents more aware of the available resources. The parents of younger patients were already frequently utilizing resources like the emergency call line prior to the intervention.
There are some limitations inherent to the design of this study. All of the subjects were drawn from a single practice, which may not be generalizable to all practice settings. While the intervention is appropriate for implementation among the general clinic populations, there are individuals with recurrent DKA admissions who may require more intensive interventions against DKA (Ellis et al., 2008). In view of relatively small sample sizes, the failure to observe significant differences in some of the pre- versus postintervention outcomes within each of the two age groups should be interpreted with caution. In addition, the validity of self-reported ED visit data may be questioned given potential limitations of self-report. Previous studies, however, have shown that self-report is up to 93% concordant with physician records at determining health-care utilization for rare, memorable events such as inpatient hospitalizations and ED visits (Bhandari & Wagner, 2006; Cengiz et al., 2013; Roberts, Bergstralh, Schmidt, & Jacobsen, 1996). Despite these limitations, our finding indicate that a short educational intervention and printed management tool is effective in improving sick day and DKA knowledge and appears to be effective in reducing ED visits by increasing utilization of diabetes emergency line for early outpatient intervention. More widespread implementation of such a program, delivered in person with written or even web-based or mobile phone compatible content, offers the potential for improving the outpatient management of sick days and prevention of DKA in youth with type 1 diabetes.
Supplemental Material
sj-pdf-1-son-10.1177_2377960818804742 - Supplemental material for An Effective Diabetic Ketoacidosis Prevention Intervention in Children With Type 1 Diabetes
Supplemental material, sj-pdf-1-son-10.1177_2377960818804742 for An Effective Diabetic Ketoacidosis Prevention Intervention in Children With Type 1 Diabetes by Rebecca J. Vitale, Casey E. Card, Judith H. Lichtman, Kate Weyman, Camille Michaud, Kristin Sikes, William V. Tamborlane and Stuart A. Weinzimer in SAGE Open Nursing
Footnotes
Authors' Note
Casey E. Card is now affiliated with Our Lady's Children's Hospital, Dublin, Ireland.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.A.W. is a consultant for Sanofi and Zealand Pharmaceuticals, a speaker for Insulet and Medtronic, and has received grant support (to his institution) from Medtronic. W.V.T. is a consultant for Novo Nordisk, Sanofi, Eli Lilly, and Medtronic Diabetes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received support from National Institutes of Health Clinical Center (Award ID: T32DK007058).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.