
Abstract
The purpose of this study was to investigate the relationship among Turkish primary health care workers’ socio-demographic characteristics, working conditions, and anxiety. A cross-sectional study was conducted with 88 of 103 (85.4%) eligible health care workers from the city of Mugla participating. The participants’ average age was 31 years, 85.2% were university graduates, 30.7% were nurses, and 64.8% had been working between 11 and 20 years at the time of the study; 93.6% worked 8 hours each day or less. State anxiety scores for males (p = .016), health care workers age 31 or older (p = .035), nurse participants (p = .043), and individuals who had worked 11 or more years (p = .044) were significantly higher than the rest of the sample; however, trait anxiety scores for participants who did not work overtime and were not scheduled for shift work were significantly higher (p = .033 and p = .004, respectively) than the rest of the sample. According to the logistic regression analysis, risk factors for anxiety included being male and older than 31 years.
Factors causing anxiety among workers are increasing, and psychosocial causes are the most common (Bennett, Williams, Page, Hood, & Woollard, 2004; Edimansyah et al., 2008; World Health Organization [WHO], 1990). Stress, defined as the response to any non-specific request of the body, is encountered frequently in work environments (Foxall, Zimmerman, Standley, & Captain, 1990). From the perspective of work life, stress is the worker’s perception of requests in the work environment, “a negative compulsion,” “a threat to the peace and health,” or “a fear of failure” (Kaufmann, Pornschlegel, & Udris, 1982). According to an International Labour Organization (ILO) publication, stress in the workplace is the biological and psychological response of workers to their environments (Levi, 1998). Encountering stressful incidents can result in anxiety (Mahan et al., 2010; Stein & Hollander, 2002). Anxiety may be a short-term response to work-related stress (Petersen, 1999).
The word anxiety is derived from the Latin “angere,” meaning “occlusion, suffocation” (Berksun, 2003). Anxiety warns individuals of impending danger and motivates individuals to take precautions (Tukel, 2000). Freud (1894) described anxiety as a motivational condition resulting in defensive behavior. However, anxiety also plays a role in many psychiatric disorders (Nutt, Feeney, & Argyroppolous, 2002).
Anxiety may also contribute to occupational injuries and illnesses, particularly affecting physical, intellectual, and social health (Beck, Rowlins, & Williams, 1988). Symptoms of anxiety include restlessness, dyspnea, and a general state of excitement. In addition, chronic anxiety is related to burnout syndrome (Ersoy, Yıldırım, & Edirne, 2001; Turnipseed, 1998). Anxiety may result in job dissatisfaction; a nursing study showed a negative association between their work satisfaction and anxiety (Durmuş & Günay, 2007). Individuals frequently encounter both anxiety and fear. Although these two emotions are distinct, they are often related (Yuksel, 2006). Anxiety may increase fear and lead to violence (Noyes & Saric, 1998).
Anxiety may contribute to occupational accidents and resulting injuries (Galazzi, Rancati, & Milos, 2014; Walter, Bourgois, Margarita Loinaz, & Schillinger, 2002). A study of 60 adults working in the fabricated metal products sector found that 37 workers had experienced work-related accidents and 64.8% of those workers had been diagnosed with psychiatric disorders; anxiety was one of the most common psychiatric disorders identified (Spor, Akbulut, Turkbikmaz, & Akayoglu, 1988). In another study of ship builders, workers who had experienced occupational accidents were found to have higher anxiety scores compared with workers who had not reported work-related injuries (L. Onen, Issever, & Sabuncu, 1998).
Negative working conditions are associated with anxiety; 82% of employees on the night shift working in Turkey’s iron and steel industry were found to suffer from anxiety (L. Onen, 1990). The literature documents many examples of traumatic workplace events that could cause anxiety (Taino, Pezzuto, Pucci, & Imbriani, 2014; Wicker et al., 2014), or anxiety may have contributed to these work-related injuries (Galazzi et al., 2014; Walter et al., 2002).
Several studies have reported that health care workers are likely to suffer from anxiety (Bennett, Lowe, Matthews, Dourali, & Tattersall, 2001; Canbaz et al., 2008; Ding, Qu, Yu, & Wang, 2014; Donmez, Aktekin, Erengin, Dinc, & Karaman, 1996; Fiabane, Giorgi, Sguazzin, & Argentero, 2013; Gorak & Yildiz, 1992; Hayran, Cali, & Harmanci, 1994; Laranjeira, 2011; Lim, Bogossian, & Ahern, 2010; Lindsay, Hanson, Taylor, & McBurney, 2008; McEwan & Goldenberg, 1999; R. Onen, Kaptanoglu, & Aksaray, 1993; Weinberg & Creed, 2000). Health care workers practice in high stress environments. Risk factors for anxiety among health care workers should be identified.
This study examined the relationship among socio-demographic status and working conditions of Turkish primary health care workers in the city of Mugla and their state-trait anxiety levels.
Method
The governor of Mugla, Mugla S.K. University, and Mugla Provincial Directorate of Health approved this study, and primary health care workers consented verbally before the interview.
Study Population
This study was conducted in Mugla, a city of 838,324 residents located in southwestern Turkey. The city is a center for energy production and tourism (Turkey Statistical Information Services, 2014). One hundred three primary health care workers were practicing in the Mugla city center at the time of this study and comprised the study’s population (Public Health Directorate, 2014). The researchers chose to include all primary health care centers and health care workers (i.e., physicians, nurses, midwives, and laboratory assistants) working in the city center at the time of the study. Eighty-eight (85.5%) of the 103 primary health care workers agreed to participate, 6 refused to participate, and 9 could not be reached due to military service, parental leave, or annual leave. To gather data, a questionnaire was used during face-to-face 15- to 20-minute interviews with the health care workers at their offices. Data were collected between January 11, 2009, and February 15, 2009.
Instruments
Socio-demographic characteristics and working conditions
The independent variables for this study included gender, age, education, marital status, number of children, income other than salary, professional status, total (annual) work time, daily work hours, overtime in the last 12 months, and shift worked in the last 12 months.
State-Trait Anxiety Inventory (STAI)
Developed by Spielberger, Gorsuch, Lushene, Vagg, and Jacobs (1983), this inventory consists of two 20-item scales to differentiate state and trait anxiety. The state portion of the instrument (SAI) assesses individuals’ “present” feelings; the trait portion of the instrument (TAI) assesses how individuals “generally” feel (Spielberg et al., 1970). The STAI has been translated into many languages, including Spanish, Turkish, Japanese, Arabic, and Dutch (Barnes, Harp, & Junk, 2002). The reliability and validity of the scale have been assessed for the Turkish version. Reliability coefficients for the SAI were measured to be between 0.26 and 0.68 (Aydemir & Koroglu, 2000), 0.73 and 0.86 (Oner, 1997), and 0.83 and 0.87 (Oner & Compte, 1983). For TAI, reliability coefficients were reported to be between 0.71 and 0.86 (Aydemir & Koroglu, 2000), 0.16 and 0.54 (Oner, 1997), 0.94 and 0.96 (Oner & Compte, 1983), and 0.87 (Yakar & Pinar, 2013). Internal consistency and homogeneity coefficients were between 0.94 and 0.96 (Aydemir & Koroglu, 2000) and 0.86 and 0.92 (Oner, 1997) for SAI, and between 0.83 and 0.87 (Aydemir & Koroglu, 2000) and 0.83 and 0.92 (Oner, 1997) for TAI. The scale has been used in many Turkish research studies (Basol, Duygu, & Gökbakan, 2014; Dastan & Buzlu, 2011; Demir & Khorshid, 2010; Fidan, Ceyhun, & Kirpınar, 2011; Gurhan, Akyuz, Atici, & Kisa, 2009; Gurkan, Gulseven, & Eren, 2013; Ilhan, Demirbas, & Dogan, 2007; Issever, Ozdilli, Altunkaynak, Onen, & Disci, 2008; Kilic et al., 2015; Kocabas, 2013; Tasci, Guleser, Tokmakci, Eroglu, & Kaplan, 2012; Yucel & Sennaroglu, 2007).
Statistical Analyses
SPSS 15.0 was used to analyze the data. The compatibility of the mean scores from the questionnaire with a normal distribution was measured by the Kolmogorov–Smirnov test and Lilliefors test. The data were analyzed using t tests, one-way ANOVA, and logistic regression; p < .05 was considered statistically significant. Logistic regression analysis was also used to distinguish between anxiety and baseline variables. State anxiety (normal, higher than normal) and trait anxiety (normal, higher than normal) were grouped and included in the logistic regression model as dependent variables. Variables with a p value of <.10 per univariate regression analyses were included in the multiple logistic regression analysis using the conventional method of maximum likelihood and variable selection using backward elimination. A p value of <.10 was used as a criterion for retaining variables in the final model.
Results
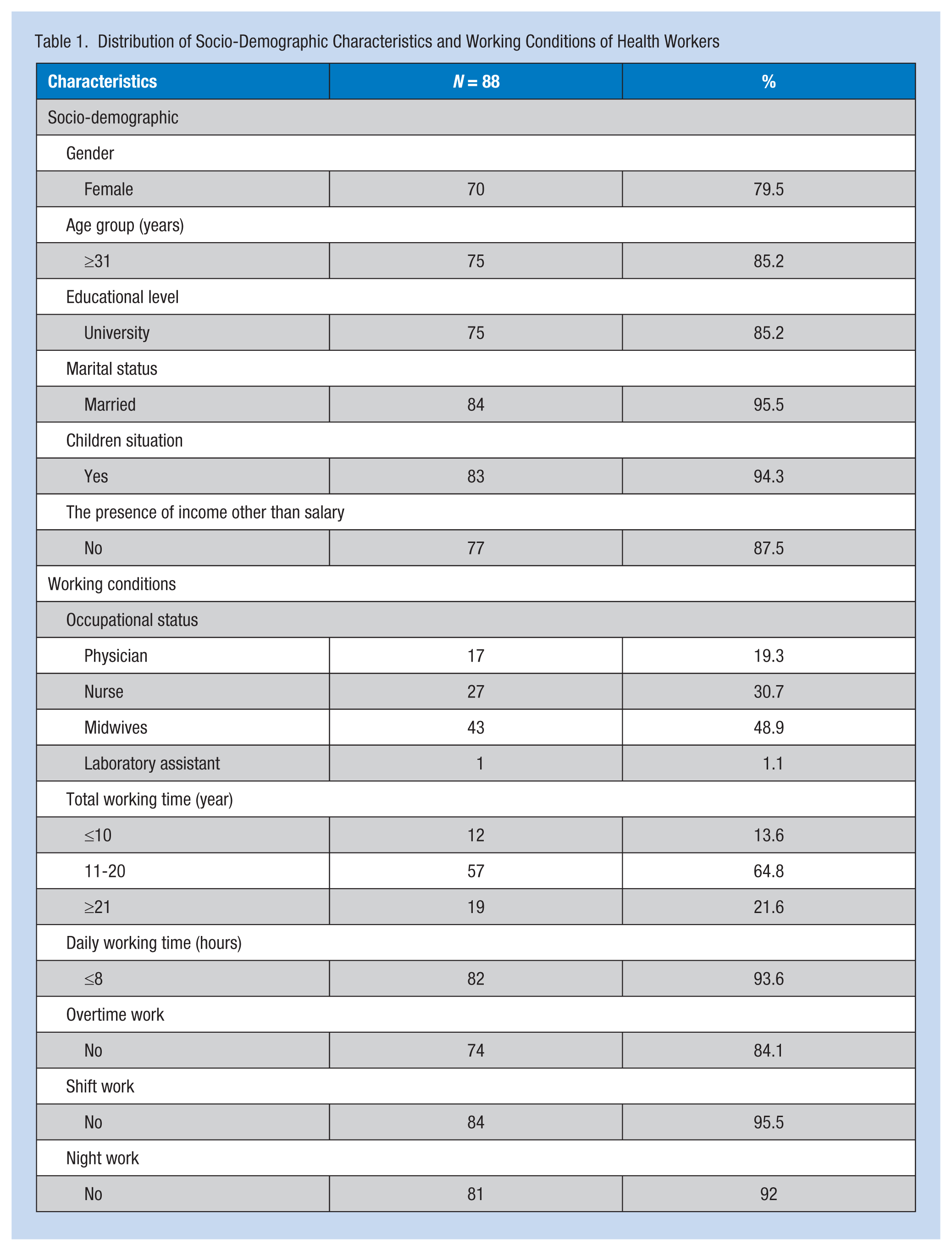
The mean age of the primary health care worker participants was 37.14 ± 6.17. More than 79% of participants were female, 85.2% were 31 years or older, 85.2% had earned university degrees, 95.5% were married, 94.3% had children, and 87.5% reported no income apart from salary (e.g., portfolio income, rental income, or income from real estate). Nearly 49% of the participants were midwives, 64.8% had worked between 11 and 20 years, 93.6% worked 8 hours or less each day, 84.1% had not worked overtime in the last 12 months, 95.5% did not work shifts, and 92% did not work the night shift (Table 1).
Distribution of Socio-Demographic Characteristics and Working Conditions of Health Workers
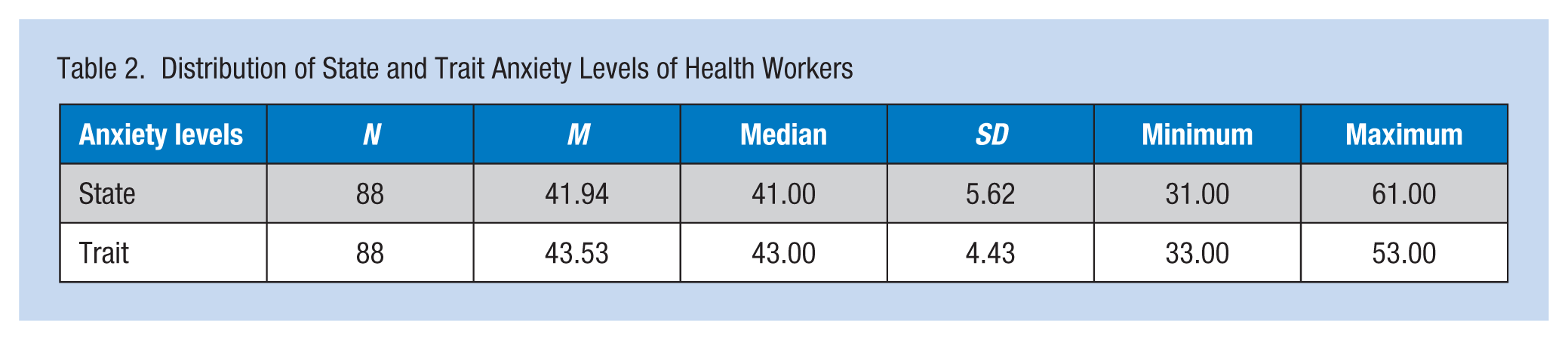
The mean state anxiety score was 41.94 ± 5.62, the median was 41.00, and the range was 31 to 61. The mean trait anxiety score was 43.53 ± 4.43, the median was 43, and the range was 33 to 53 (Table 2). According to the STAI, trait anxiety scores were higher than “normal adult levels” in 64.8% of the participants, and 53.4% of the sample exhibited higher state anxiety scores than “normal adult levels” (Table 3).
Distribution of State and Trait Anxiety Levels of Health Workers
Distribution of State and Trait Anxiety Levels of Health Workers Based on the Mean of Normal Adult Levels
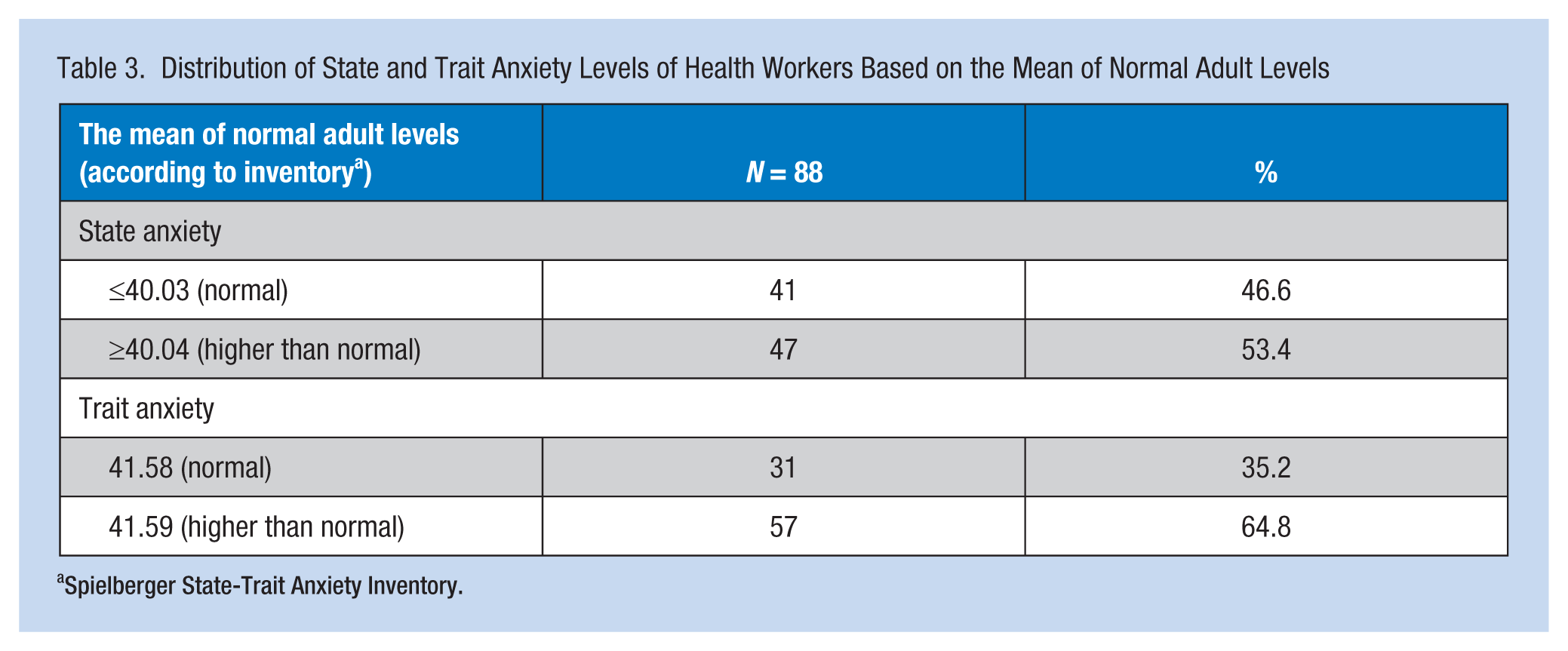
Spielberger State-Trait Anxiety Inventory.
The researchers determined that state anxiety scores were not related to education, marital status, having children, source of income, daily work hours, overtime, or shift work. Compared with other groups of health care workers, state anxiety scores for males (p = .016), workers aged 31 and older (p = .035), nurses (p = .043), and workers with 11 or more years of experience were significantly higher (Table 4).
Distribution of State and Trait Anxiety Levels of Health Workers Based on Socio-Demographic Characteristics and Working Conditions
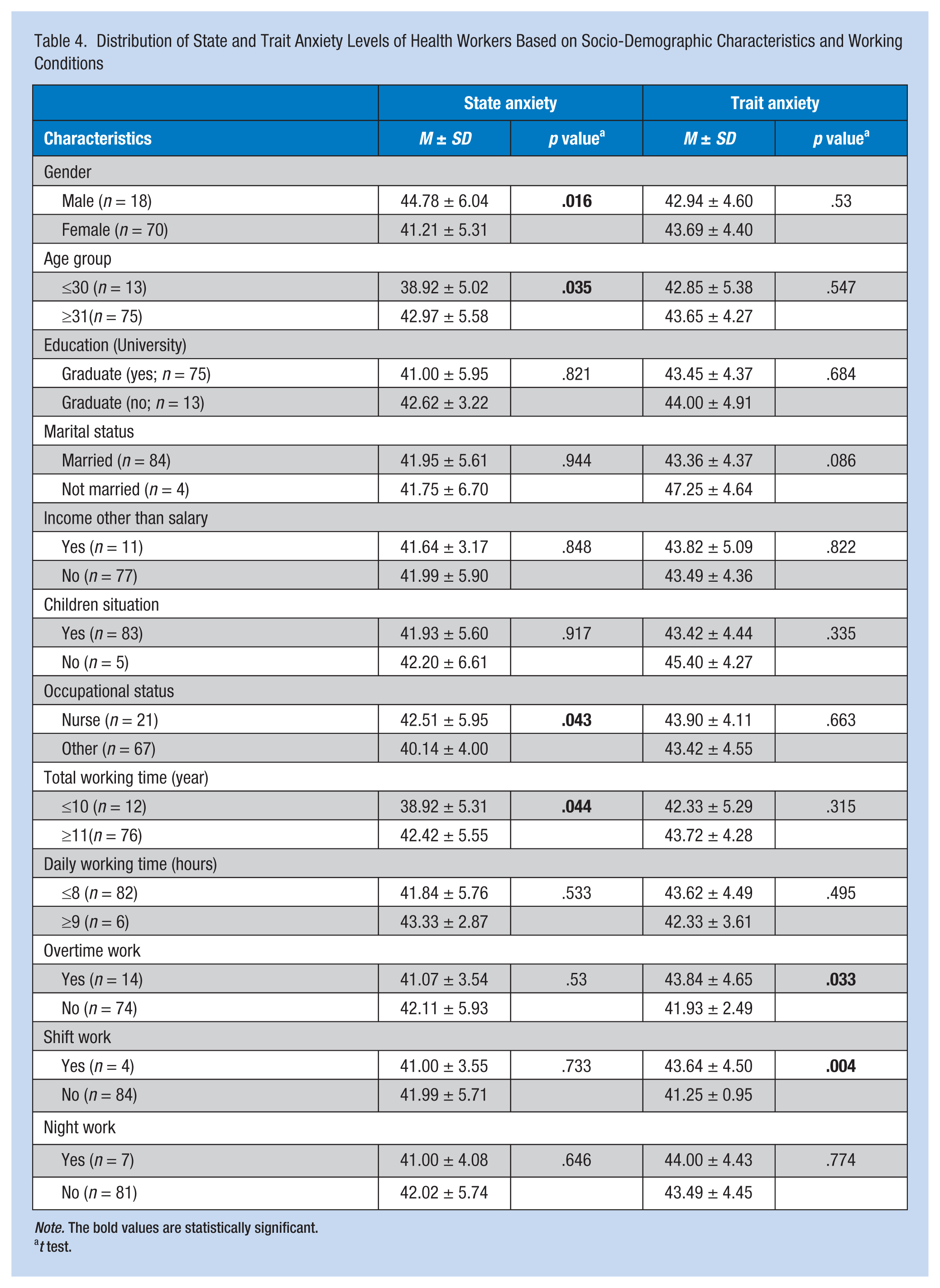
Note. The bold values are statistically significant.
t test.
With regard to trait anxiety scores, no significant differences were found by gender, age, education, marital status, presence of children, source of income, profession, work tenure, or daily work hours. Trait anxiety scores for health care workers who worked overtime and were assigned shift work were significantly higher than other groups (Table 4).
The logistic regression analysis showed that male participants 31 years and older were most likely to report significantly higher state anxiety (odds ratio [OR] = 3.9, confidence interval [CI] [1.03, 14.74], and OR = 5.8, CI [1.13, 30.01], respectively). Participants 31 years and older were significantly more likely to experience trait anxiety (OR = 7.8, CI [1.27, 24.19]; Table 5).
Risk Factors Affecting Anxiety According to Logistic Regression Analyses
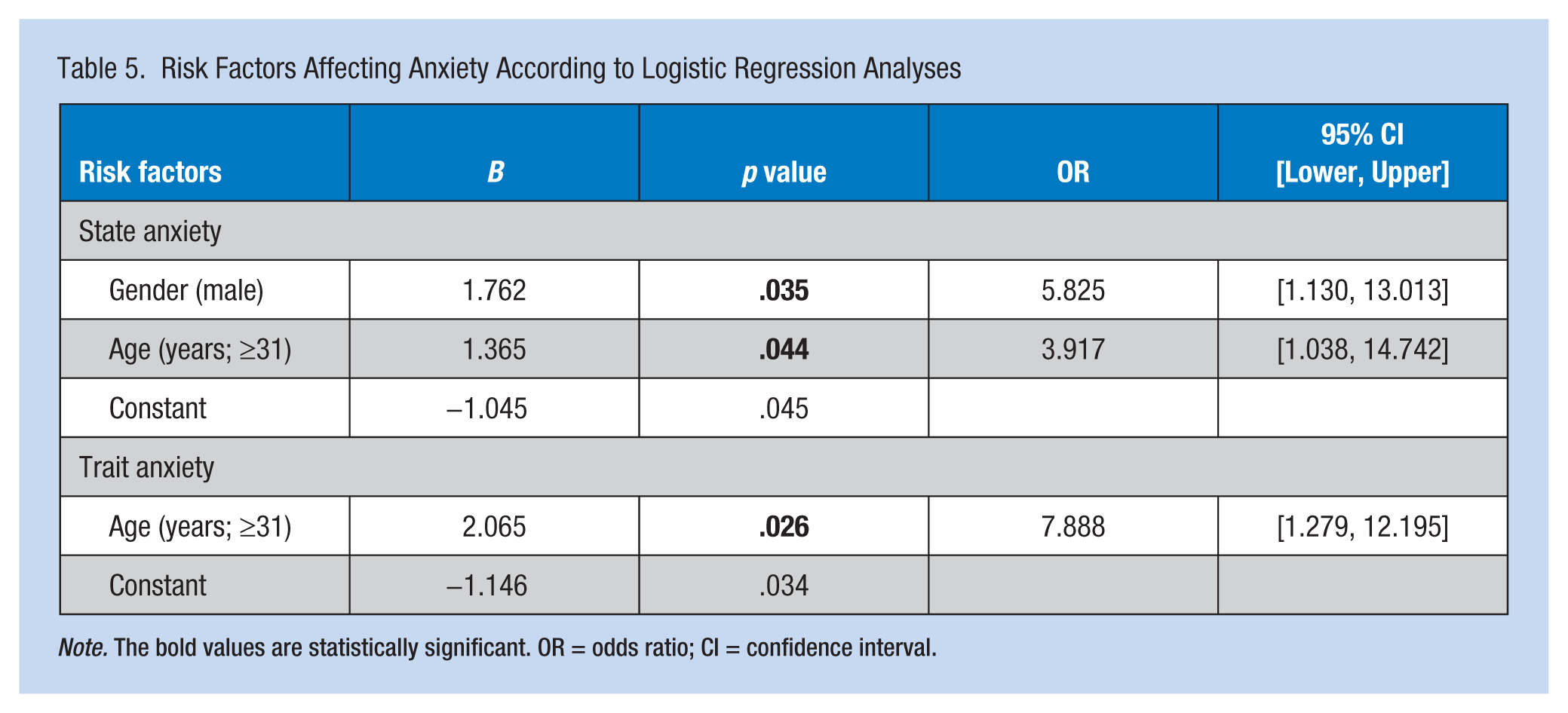
Note. The bold values are statistically significant. OR = odds ratio; CI = confidence interval.
Discussion
State anxiety scores of male health care workers were found to be significantly higher than female workers’ state anxiety scores. A few studies have confirmed this finding (Baturlu & Erden, 2007; Donmez et al., 1996; Sun, Ful, Ying Chang, & Wang, 2012; Uskul, Selvi, & Melikoglu, 2006). This finding may be explained by the lower number of males participating in the study because males are more often assigned to mobile health services than females (e.g., violence and harassment are more common when providing mobile health services). Examples of anxiety-producing traumatic events that have occurred during work hours are documented in the literature (Taino et al., 2014; Wicker et al., 2014). Both stress at work and outside of work contribute to anxiety experienced by health care staff (Weinberg & Creed, 2000). However, anxiety, in general, has been more often observed in females than males (Canbaz et al., 2008; Foot & Koszycki, 2004; Olatunji & Wolitzky-Taylor, 2009; Sahin, Batigun, & Uzun, 2011; Stewart, Taylor, & Baker, 1997; Tasdemir, Erakgun, Deniz, & Certug, 2013). Women have reported higher levels of anxiety than men in studies of physician interns in Istanbul (Hayran et al., 1994), general practitioners in England (Sutherland & Cooper, 1992), and physicians in China (Gong et al., 2014). One explanation for this gender difference may be that psychiatric disorders are reported more often in women than men in the general population (American Psychiatric Association [APA], 2013).
Compared with younger workers, older workers reported higher levels of anxiety. Health workers, 31 years and older, were found to have statistically higher state anxiety scores than younger workers. In Ankara, nurses 46 years and older reported higher anxiety scores than younger nurses (Gorgulu, 1998). In Turkey, older workers in emergency units had higher anxiety scores than younger workers (Canbaz et al., 2008). As the proportion of older employees in the workforce increases, researchers have become increasingly interested in the association between age and anxiety. The curvilinear nature of this relationship has been documented in the literature with employees in their late 20s to early 40s generally reporting lower levels of anxiety than older employees (APA, 2013; Kouri, Di Giampaolo, Toto, Cerrone, & Boscolo, 2001; Zacher, Jimmieson, & Bordia, 2014). A few studies have reported that anxiety is not affected by age (Picakciefe, Ergor, Kilic, & Yemez, 2006; Uskul et al., 2006).
No significant difference was detected for mean STAI scores by health workers’ educational status (p > .05). Some studies have confirmed this finding (Sirin, Kavak, & Ertem, 2003; Tuncer & Yucel, 2014; Turhan, 2007; Uskul et al., 2006). However, health workers with the lowest mean STAI score were university graduates. Similar studies have supported the same result (Ay, 1992; Gorgulu, 1998; Picakciefe et al., 2006). In the literature, it is reported that individuals with more education better cope with the stress and anxiety of diagnosing and treating illness and injury (Pan et al., 2013; Stafford et al., 2014). Similarly, in another study, it was found that individuals with higher educational levels have better coping mechanisms, and they use these mechanisms to improve their quality of life (Malik & Kiran, 2013).
When researchers assessed primary health care workers, nurses had higher state anxiety scores compared with other workers (Taghavi, Sharifi Neiestanak, Aghajani, & Mehran, 2009; Yalcin & Ilhan, 2008). More than 80% of primary health care workers in this study had practiced for 11 years or more. Assessing anxiety levels based on senority, the longer workers had worked, the higher their anxiety levels. Similar studies have supported the same result (Durmuş & Günay, 2007; Issever, Onen, & Sabuncu, 2002; Issever, Sabuncu, & Onen, 1999; Ocaktan, Keklik, & Çol, 2002), which may be explained by the increased exposure to stress workers with longer tenure experience.
Under Article 99 of Law No. 657 on Civil Servants and the European Union’s Council Amending Working Time Directive 1993/104/EC and 2003/88/EC, every worker is entitled to work 40 hours a week and 8 hours a day (Ekici & Ozcelik, 2011); 15.9% of health care workers in this study worked overtime. Frequent overtime violates regulations regarding standard work hours and could endanger workers’ health, security, and well-being (Clerk, 1989). Trait anxiety was higher for workers who worked overtime in this study.
Few study respondents worked shifts or at night (i.e., 4.5% and 8.0%, respectively). However, trait anxiety was significantly higher for workers in this study who worked shifts. Shift work may be associated with mental health; however, limited research on this issue was found in the literature, and the results so far are inconclusive. A recent review on the topic concluded that causal relationships between shift work and mental health are not well established due to the correlational cross-sectional design of the majority of these studies (Vogel, Braungardt, Meyer, & Schneider, 2012). Some findings on this topic are nonetheless reported in the literature. Individuals working shifts have been found to report high levels of fatigue (Shen et al., 2006; Yuan et al., 2011); employee fatigue contributes to accidents and injuries and affects occupational performance, safety, and health (Yumang-Ross & Burns, 2014) In addition, shift work may negatively affect concentration and be associated with depression, anger, and anxiety (Houry, Shockley, & Markovchick, 2000). A study by Bara and Arber (2009) found that women who worked more than 2 years of shift work and men who worked more than 4 years of night work were more likely to report depression and anxiety.
Study Limitations
This study had several limitations. First, the study was conducted in a single city’s primary health care centers; hospitals and private facilities were not included. The inability to generalize may affect the findings of this study. Second, the interviews were conducted during working hours, which may have affected the number of workers who participated in the study. Third, the study was based on self-reported information, so the findings may not be completely accurate. Fourth, recall bias may have affected the accuracy of the data collected. Fifth, meaningful statistical analyses were constrained due to the small sample size and the resulting lack of statistical power. Sixth, because this is a cross-sectional study, the researchers cannot establish causality between anxiety and related risk factors. Future longitudinal studies should be conducted to confirm the conclusions from this study. Finally, because this study was conducted only in Mugla, Turkey, these results cannot be generalized to all Turkish primary care workers. Future studies are needed using larger samples in several health care centers in different regions of Turkey.
Conclusion
This study established a connection between socio-demographic characteristics, working conditions, and anxiety. Anxiety affects workers’ mental health and general well-being. Therefore, risk factors for anxiety should be identified and ameliorated to protect workers from illness and injury. Health care workers should be monitored for the effects of anxiety on worker health. Workers should learn effective ways of coping with occupational stressors, including strategic problem solving, developing a social support network, and exercising self-control, escape-avoidance, and distancing. In addition, access to an Employee Assistance Program for early identification and treatment of anxiety-related disorders should be instituted. Commitment from employers is essential to adequately measure the scope of anxiety-related disorders among health care workers. The implementation of reporting mechanisms that foster the identification of stressful events is necessary for developing targeted prevention strategies as well as testing their effectiveness. Occupational health nurses are essential members of the occupational safety and health team, which must address this serious public health issue (AAOHN, 2014).
Applying Research to Practice
Health care workers should be monitored for the effects of anxiety on worker health. Workers should learn effective ways of coping with occupational stressors, including strategic problem solving, developing a social support network, and exercising self-control, escape-avoidance, and distancing. In addition, access to an Employee Assistance Program for early identification and treatment of anxiety-related disorders should be instituted. Commitment from employers is essential to adequately measure the scope of anxiety-related disorders among health care workers. The implementation of reporting mechanisms that foster the identification of stressful events is necessary for developing targeted prevention strategies as well as testing their effectiveness. Further information can be found on the OSHA website (https://www.osha.gov/).
Footnotes
Acknowledgements
The authors thank all workers who participated in this study and the reviewers for their insightful and helpful comments. Thanks to all those who cooperated in this research, including the Provincial Director of Mugla City Health and Mugla Governorship and Mugla S.K University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Metin Picakciefe is MD, PhD, associate professor, Head of Department of Public Health, Faculty of Medicine, Mugla S.K. University, Turkey.
Aynur Turgut, RN, is a nurse, School of Health Sciences, University of Mugla S.K., Turkey.
Emel Igneci, RN, is a nurse, School of Health Sciences, University of Mugla S.K., Turkey.
Fatih Cayli, RN, is a nurse, School of Health Sciences, University of Mugla S.K., Turkey.
Artuner Deveci is MD, associate professor, Department of Psychiatry, Faculty of Medicine, Celal Bayar University, Turkey