
Abstract
Objective
This scoping review aims to examine and map existing literature about barriers encountered by migrant farm workers accessing health care services in Canada.
Methods
The search was conducted in multiple databases and grey literature. The PRISMA-ScR was used to document the inclusion and exclusion process. Two or more team members screened and reviewed all articles to ensure accuracy in capturing data.
Synthesis
380 records were screened by examining abstracts and titles, and 325 were deemed irrelevant. Of the remaining records, 55 had full-text assessments; 16 were excluded because they did not meet the inclusion criteria. Thirty-nine articles were extracted. They represented a mix of qualitative and quantitative studies, reviews, and other forms of commentaries and analyses. The thematic analysis revealed barriers that affect migrant farm workers’ access to Canadian health care services: (1) language and literacy challenges, (2) concern of medical repatriation, (3) lack of transportation, (4) barriers to timely care and medical follow-up, (5) restrictive work schedules, and (6) health care coverage issues.
Conclusion
This review provides a synthesis of the barriers experienced by migrant farm workers when accessing Canadian health care services. Canadian health care policy experts and organizations where Canadian migrant farm workers seek care are encouraged to design and implement policies, practice changes and/or educational interventions to address these barriers. This review may also inform public health nursing programming to promote positive health outcomes in the migrant farm worker population.
Introduction
Migrant farm workers (MFWs) represent a diverse population in Canada. They are temporary foreign workers (TFWs) in the agricultural sector (Al-Bazz et al., 2022). Over time, MFWs have been referred to by various names, including seasonal agricultural workers, international agricultural workers, agri-food workers, and agricultural stream workers. For this scoping review, the term MFWs will be used.
Canada's agricultural sector relies heavily on migrant workers in response to labour shortages to cultivate and harvest essential food to sustain the economy (Al-Bazz et al., 2022). In 2023, Canada authorized 70,267 TFW permits for the agricultural industries; most MFWs are from low and middle-income countries, consisting of Black, Latin Americans, and other racialized populations (Amnesty International, 2025). Workers typically enter Canada through the Seasonal Agricultural Worker Program (SAWP), which is part of the Primary Agriculture stream of the Temporary Foreign Worker Program (TFWP).
Temporary Foreign Worker Programs
Temporary Foreign Worker Programs were established in 1973 to enable Canadian employers to fill temporary positions when qualified Canadians are unavailable. Agricultural jobs must be performed on farms, nurseries, or greenhouses and include activities such as operating agricultural machinery and planting, caring for, and harvesting crops for market (Government of Canada, 2023). These programs are known to pose unique migration, health, and safety challenges for MFWs (Mayell et al., 2025). Work permits are tied to a single employer, who can revoke a worker's permit at any time for reasons like insufficient work, refusal to work excessive overtime, or health issues that prevent the worker from continuing (Mayell et al., 2025).
Within the TFWPs, there are five streams: (1) Primary Agriculture (SAWP & Agricultural stream), (2) Low Wage, (3) High wage, (4) Caregivers, and (5) Global Talent. MFWs can enter Canada via the Primary Agriculture or Low Wage streams (Amnesty International, 2025). The salaries and visa lengths vary based on the stream, with SAWP being up to eight months, the Agricultural stream lasting up to three years, and the Low Wage stream offering a one-year visa (Amnesty International, 2025). It is difficult for low-skilled workers to obtain permanent residency as they face barriers to obtaining the neutral requirements, such as a diploma, education, and language proficiency (Amnesty International, 2025). The federal government added the Agricultural stream in the early 2000s, allowing employers to hire MFWs from any country, often through private brokers (Molnar, 2018). Their contracts are not standardized and are typically agreements between the employer and the worker, with final approval from Service Canada (Foreign Agricultural Resource Management Services, 2024). Migrant farm workers under the primary agricultural stream have virtually no access to permanent status, labour mobility, or social services in Canada (Cohen, 2019).
The SAWP is the oldest and most established of the two programs, and was first piloted by the federal government in Ontario in 1966 with Jamaican workers (Cohen & Hjalmarson, 2020). It was subsequently extended to include participating countries such as Barbados, Trinidad and Tobago, and Mexico (Cohen & Hjalmarson, 2020). It did not take long for the program to expand from Ontario to other Canadian provinces (Cohen & Hjalmarson, 2020). Currently, the countries participating in the SAWP include Mexico, Anguilla, Antigua and Barbuda, Barbados, Dominica, Grenada, Jamaica, Montserrat, St. Kitts-Nevis, St. Lucia, St. Vincent and the Grenadines, and Trinidad and Tobago (Government of Canada, 2023). Bilateral agreements between Canada and the participating country ensure a smooth recruiting process (Caxaj & Cohen, 2021a; Caxaj et al., 2020). The SAWP uses a standard, non-modifiable contract to outline each party's rights and obligations, ensuring that all involved understand and agree to the relevant working conditions and responsibilities (Government of Canada, 2023).
The SAWP facilitates circular labour migration, allowing workers to work in Canada for up to eight months before heading back to their home countries (Hjalmarson, 2021). Their work permits are exclusively linked to the agricultural sector and designated SAWP employers (Caxaj & Cohen, 2021a; Hjalmarson, 2021). It is almost impossible to transfer to another employer, essentially rendering them as bonded labourers (Cohen, 2019). Employers have specific responsibilities, including providing workers with meals and housing, and registering them for provincial health coverage and workers’ compensation (Caxaj & Cohen, 2021a). Contracted MFWS are covered by employer-arranged private insurance and become eligible for provincial health coverage after three months (Cohen & Caxaj, 2018). However, many remain unregistered because employers fail to complete the process, and workers fear raising concerns (Cohen & Caxaj, 2018). Private insurance alone is often inadequate, as many clinics and pharmacies do not bill insurers directly, forcing workers to pay upfront for costly visits and tests (Cohen & Caxaj, 2018). Reimbursement delays often result in many individuals leaving Canada before being reimbursed, creating significant financial barriers to accessing care (Cohen & Caxaj, 2018).
To return to Canada, workers are requested by name and number and must receive a positive review from the consular or liaison officer (Caxaj & Cohen, 2021a; Hjalmarson, 2021). The specific work permit type, sub-standard housing conditions, and the constant threat of deportation act as control mechanisms, ensuring workers remain silent and compliant (Hjalmarson, 2021). Moreover, the SAWP is known to restrict the freedom of MFWs, create unfair work conditions, and limit access to eligible supports and entitlements (Caxaj & Cohen, 2021a). Many MFWs regard the SAWP as slavery without the whip (Hjalmarson, 2021).
Accessing Health Care Services in Canada
Most of the MFWs that come to Canada are middle-aged males. They are usually poor, racialized, and do not speak or read English, and have low levels of education (Amnesty International, 2025). Most MFWs are generally healthier than Canadians on arrival (Shmyr et al., 2022). However, once in Canada, MFWs face racism, prejudice, and discrimination (Hjalmarson, 2021). Coupled with displacement from their homes, isolation, climate extremes, lack of transportation (Hjalmarson, 2021), language barriers, exploitation, minimal rights, and structural inequities (Nguyen et al., 2021), the health of MFWs can rapidly decline. In addition, demanding and hazardous working conditions and barriers to accessing health care services can further jeopardize health (Al-Bazz et al., 2022). Such working conditions leave MFWs facing a higher risk of illness and injury at work, along with increased challenges in accessing the workers’ compensation to which they are entitled (Hanley et al., 2025; Mayell et al., 2025). Injured workers assigned to light duties are often dismissed and repatriated immediately if they are unable to continue working (McLaughlin & Hennebry, 2013). Those who decide to stay in Canada are left without housing, income, and access to essential services, including health care (Caxaj & Cohen, 2021a; McLaughlin & Hennebry, 2013). These issues catalyze health and safety concerns that impact physical, mental, and social well-being (Al-Bazz et al., 2022). Therefore, it is essential to highlight the barriers that prevent MFWs from accessing health care services in Canada.
This scoping review will map existing literature about barriers MFWs encounter when accessing health care services in Canada. The information obtained can be utilized to improve health care service access for MFWs. Moreover, nurses caring for and involved in public health program planning can utilize the information to target interventions that will combat health care service access issues for this vulnerable population. This scoping review may also reveal knowledge gaps that need further examination. After conducting a preliminary search, to the best of the author's knowledge, no current review has been conducted on this topic.
Methods
This scoping review was conducted in accordance with the JBI scoping review methodological framework (Peters et al., 2021). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (Page et al., 2021) was utilized as a reporting tool and to track the included and excluded sources. This scoping review mapped emerging evidence related to barriers encountered by MFWs when accessing health care services in Canada.
Inclusion Criteria
Sources that discussed MFWs employed in an agricultural setting who entered Canada via the SAWP or other farm-related TFWP with a valid work permit for the agricultural sector were included. Sources that discussed barriers to MFWs’ access to health care were also included. All genders were considered, and no age limits were imposed. Undocumented workers were excluded because this scoping review focused specifically on workers under a valid SAWP or other farm-related TFWP contract.
Search Strategy
Various experimental designs were considered for this scoping review, including cross-sectional descriptive studies, descriptive analysis using a retrospective chart review and interviews, pilot studies involving data gathering through surveys and focus groups, and mixed-method studies. Qualitative studies were also considered, including exploratory studies, grounded theory, critical ethnography, comparative case studies, qualitative description, and a critical realist approach. In addition, several reviews, including critical reviews and scoping reviews, were considered. Reports, expository articles, analyses, editor letters, and news articles were also reviewed. Grey literature search is discussed below.
The search strategy considered published and unpublished studies. An initial limited search was conducted in MEDLINE and CINAHL to retrieve articles relevant to the topic. The text words within the title, abstract, and index terms were analyzed and utilized to develop the final search strategy. This search strategy was then adapted and executed in each relevant database. The reference lists of the included articles were manually screened for additional studies. No limits were placed on date; articles were translated that were not in English. The databases searched included MEDLINE (Ovid), CINAHL (EBSCO), ProQuest Nursing and Allied Health (ProQuest), PsycINFO (ProQuest), Emcare (Ovid), Cochrane Central Register of Controlled Trials (Ovid), Cochrane Database of Systematic Reviews (Ovid), Dissertations & Theses Global (ProQuest), and Scopus (Elsevier). See Appendix A in the supplementary information.
A systematic grey literature search was conducted to ensure that the comprehensiveness of this scoping review was maintained and that all critical data was included. A two-step method was employed. The first step involved searching the topic in Google for relevant authorities, organizations, and stakeholders that pertain to the topic. The second step comprised of three strategies: targeted website searching, an advanced Google search, and contacting knowledge experts.
Screening
Following the search, all identified citations were collated and uploaded into Covidence and duplicates were removed. Titles and abstracts were screened, and full-text reviews were conducted. Two or more independent team members conducted screening and full-text reviews on all sources. Any disagreements between the reviewers at each stage of the selection process were resolved through discussion or by an additional reviewer. Reasons for exclusion of sources at full-text review are listed in the PRISMA-Scr flow diagram (Figure 1).
Extraction
Data from sources included in the scoping review were extracted using an extraction tool created in Covidence. Two team members extracted data from all articles, and a third reviewer compared extracted sources to ensure interrater reliability during extraction. The extraction tool allowed a comparison of the sources related to MFWs in Canada. The extracted data included details regarding author(s), year, title, geographic setting, study design/source, objective, sample, health concern, access point(s) to health care, and the farm workers program. Additionally, details were extracted regarding barriers encountered by MFWs when accessing health care services in Canada. The extracted data is presented below in a descriptive format with tables to summarize the findings. The presentation of the information aligns with the objective of this scoping review, which is to examine the current state of the literature regarding barriers encountered by MFWs when accessing health care services in Canada.
Study Inclusion
There were 589 records identified through database searching. After removing 209 duplicates, the remaining 380 records were screened by examining abstracts and titles, and 325 were deemed irrelevant. Of the remaining records, 55 had full-text assessments completed by two reviewers. There were 16 excluded based on the following reasons: abstract only (n = 1), wrong patient population (n = 8), and did not address access to health care (n = 7). The remaining 39 records were extracted for synthesis as they met the inclusion criteria.
Results
Characteristics of Included Studies
The 39 sources included in this review discussed MFWs; all studies occurred in various locations across Canada. Twenty articles were research studies; eight were mixed methods, nine were qualitative, two were quantitative, and a final research study was a secondary data analysis. The final 19 sources included six reviews, four articles, four analyses (articles), two newspaper articles, and one of each of an opinion piece, a commentary, and a letter to the editor. See supplementary material—Table 1 in Appendix C for the 39 sources used in the scoping review.
Many articles discussed multiple access points. Most articles (n = 19) discussed clinics, followed by public health (n = 15), as the first access point for health care services. Other sources listed access points such as, occupational health (n = 11), hospitals (n = 9), primary care (n = 6), emergency departments/paramedics (n = 6), mental health (n = 3), sexual health (n = 3), health centres (n = 2), and dental care (n = 1). Furthermore, on-site care (n = 1), plastic surgeon (n = 1), and employer-mediated services (n = 1) were mentioned as access points. The most common health concerns were workplace/occupational injury or illness (n = 20) and mental health issues/concerns (n = 20). Also, COVID-19 infection (n = 9), sexual/reproductive (n = 9), and living conditions/climate (n = 5) were listed as health concerns facing MFWs (See supplementary material—Appendix B for details on the studies included).
Barriers to Accessing Health Care
Six themes emerged across all sources about barriers encountered by MFWs accessing health care services in Canada, including (1) Language and Literacy Challenges, (2) Concern of Medical Repatriation, (3) Lack of Transportation, (4) Barriers to Timely Care and Medical Follow-up, (5) Restrictive Work Schedules, and (6) Health Care Coverage.
Language and Literacy Challenges
Viveros-Guzmán and Gertler (2015) identified language barriers as the most challenging aspect for MFWs working and living in Canada. In fact, despite having health care coverage, MFWs were reluctant to access services due to language barriers (Barnes, 2013; Narushima et al., 2016; Pysklywec et al., 2011) and felt that not knowing English was detrimental to their health (Hennebry et al., 2016). Similarly, English-speaking health care providers expressed that language, comprehension, and accents were challenges (Caxaj et al., 2023; Cole et al., 2019). Language barriers prevent MFWs from receiving optimal care when accessing health care (Salami et al., 2015; Zhou et al., 2023). Further, language barriers hinder MFWs from receiving sufficient, equitable, and comprehensive health care services (Edmunds et al., 2011; Gallant et al., 2010).
Challenges are compounded by limited health literacy, which affects MFWs’ ability to navigate the health system (Caxaj & Diaz, 2018; Colindres et al., 2021; McLaughlin, 2009; Salami et al., 2018; Stasiulis, 2020). Low literacy further hinders adherence to treatment plans, understanding of medication instructions, and compliance with workplace safety protocols, which can lead to self-medication (Viveros-Guzmán & Gertler, 2015; Wong et al., 2021). Workers, fearing language difficulties or lacking understanding, preferred not to see a doctor, thus exacerbating health risks and delaying treatment (Viveros-Guzmán & Gertler, 2015). In some cases, language and literacy barriers delayed the reporting of workplace injuries, rendering workers ineligible for compensation (Preibisch & Hennebry, 2011). The reliance on non-certified interpreters (employers or co-workers) often leads to miscommunication, breaches of privacy, and dissatisfaction with care (Caxaj & Cohen, 2021b; Caxaj et al., 2022a; Mysyk et al., 2009; Narushima & Sanchez, 2014). Also, the absence of multilingual health care services, including language training (Hennebry & Preibisch, 2012), exacerbates inequities, contributing to the underutilization of health benefits and perpetuating disparities in access and outcomes (Landry et al., 2021; Preibisch & Otero, 2014).
Furthermore, a COVID-19 outbreak at a garden center in British Columbia highlighted that language barriers placed MFWs in a vulnerable position (Mema et al., 2021). Their access to medical services during the pandemic was also hindered (Mema et al., 2021). Without access to adequate translation services, health care providers struggled to provide proper care to MFWs (Caxaj et al., 2022a). In one instance, a MFW who had a severe case of COVID-19 pneumonia with poor oxygen saturation declined intubation (Caxaj et al., 2022a). The worker thought he had to pay for this potentially life-saving intervention (Caxaj et al., 2022a). Language barriers and inadequate access to technology also prevented MFWs from utilizing telemedicine, which was the preferred method for health care providers to complete a COVID-19 assessment (Landry et al., 2021).
Concern of Medical Repatriation
The concern of medical repatriation and being regarded as disposable negatively impacts the trust relationship between workers and service providers (Salami et al., 2016). Between 2001 and 2011, 25 workers were repatriated due to mental health concerns (Salami et al., 2015, 2018). Furthermore, of 14 critically ill MFWs admitted to local hospitals, five were repatriated shortly after diagnosis, forcing them to seek treatment in their home countries (Zhou et al., 2023). Between 1996 and 2011, 1,198 MFWs were repatriated without legal recourse (Glauser, 2014).
Concern of repatriation deters workers from seeking care (Edmunds et al., 2011) or reporting occupational health and safety issues (Caxaj & Cohen, 2021b; Cecco, 2024; Colindres et al., 2021; McLaughlin, 2009; Mysyk et al., 2009; Preibisch & Hennebry, 2011). Many MFWs continue to work despite illness or injury due to fear of termination and repatriation (Caxaj et al., 2022a, 2022b, 2023, 2024; Cole et al., 2019; Gallant et al., 2010; Hennebry & Preibisch, 2012; Hennebry et al., 2016; Mema et al., 2021; Stasiulis, 2020; Vosko et al., 2022; Wong et al., 2021). The workers rely on their employers to be renamed so that they may return in subsequent growing seasons (Caxaj et al., 2022a). Their precarious and temporary status may prompt employers to reinforce threats and intimidation, including that of repatriation (Caxaj et al., 2022a).
Job insecurity discourages reporting illness or injury, applying for workers’ compensation, or requesting modified duties or time off (Landry et al., 2021; Preibisch & Otero, 2014; Pysklywec et al., 2011). Additionally, employers actively discourage workers from reporting injuries due to concerns about legal and financial repercussions (McLaughlin, 2009; Preibisch & Otero, 2014). Moreover, workers risk losing health coverage once their contracts end or if they leave their employers (Zhou et al., 2023). The SAWP offers limited protection, leaving workers vulnerable to being fired, blacklisted, or deported without cause (Barnes, 2013; Doyle, 2020; Hennebry & Williams, 2015; Lee et al., 2022; Narushima et al., 2016). Additionally, listing names in SAWP penalizes workers who report health concerns, jeopardizing future hiring (Hennebry & Williams, 2015; Holmes-Hill, 2024; Narushima & Sanchez, 2014).
During the COVID-19 pandemic, MFWs reported a fear of disclosing COVID-19 symptoms, as this might lead to medical repatriation (Doyle, 2020; Istiko et al., 2022; Mema et al., 2021; Vosko et al., 2022). Another study revealed that MFWs purposefully avoided COVID-19 public health measures such as testing or monitoring (Vosko et al., 2022). These issues confirm that health care access in Canada remains at a low standard for MFWs (Lundqvist & Day, 2010).
Lack of Transportation
MFWs often reside in rural, remote, or segregated areas; accessing safe public transit is difficult, and hinders their ability to access health care services (Arya et al., 2021; Caxaj et al., 2022a, 2022b, 2024; Cole et al., 2019; Colindres et al., 2021; Edmunds et al., 2011; Hennebry et al., 2016; McLaughlin, 2009; Mema et al., 2021; Narushima et al., 2016; Preibisch & Hennebry, 2011; Preibisch & Otero, 2014; Salami et al., 2015). To address this barrier, Pysklywec et al. (2011) propose introducing mobile clinics to transport health care providers directly to the workers.
Many workers depend on employers for transportation to medical facilities, thus giving employers control over health care access (Barnes, 2013; Caxaj et al., 2022a; 2024; Colindres et al., 2021; Cole et al., 2019; Glauser, 2014; Landry et al., 2021; Lee et al., 2022; Stasiulis, 2020; Viveros-Guzmán & Gertler, 2015; Zhou et al., 2023). In some cases, employers refusing to transport sick or injured workers delayed critical medical care (Caxaj & Diaz, 2018; Colindres et al., 2021). Employers felt obliged to assist with appointments, leading to strained relationships (Narushima & Sanchez, 2014). Further, workers without independent transportation often miss follow-up appointments, leading to untreated or worsening health conditions (Caxaj et al., 2024; Gallant et al., 2010). Without accessible and affordable transit options, many MFWs could not obtain timely medical care (Caxaj et al., 2023).
During the COVID-19 pandemic, MFWs faced difficulties accessing medical services, including COVID-19 testing centers (Arya et al., 2021; Mema et al., 2021). To further illustrate this, when a worker fell ill with COVID-19, workers from another bunkhouse contacted researchers they had met in the past growing season (who lived thousands of miles away in another province) to help call for an ambulance (Caxaj et al., 2022a). MFWs were often blamed for not accessing health care services during the COVID-19 pandemic, even though they relied heavily on their employers for assistance (Istiko et al., 2022).
Barriers to Timely Care and Medical Follow-Up
Many workers were unaware of their insurance coverage and available services, leading to confusion and underutilization of medical resources (McLaughlin, 2009; Salami et al., 2016). Workers lacked basic knowledge regarding workplace safety insurance and compensation claims, preventing them from accessing the care they were entitled to (Barnes, 2013; Landry et al., 2021). Additionally, some employers controlled whether workers could seek medical attention or file insurance claims (Narushima et al., 2016). Cultural differences, limited education, literacy, and inadequate health literacy were additional factors that hindered workers from navigating the health care system (Arya et al., 2021; Caxaj & Diaz, 2018; Caxaj et al., 2022a, 2022b; 2023; Cole et al., 2019; Edmunds et al., 2011; Hennebry et al., 2016; Landry et al., 2021; Mema et al., 2021; McLaughlin, 2009; Narushima et al., 2016; Preibisch & Hennebry, 2011; Pysklywec et al., 2011; Salami et al., 2015; Salami et al., 2016; Salami et al., 2018; Stasiulis, 2020). Many workers also struggled to understand medical terminology and procedures, leading to miscommunication and reluctance to seek care (Caxaj et al., 2022a; Preibisch & Hennebry, 2011). Workers found it difficult to access primary care, as physicians often required a formal, continuous rostering of the workers, where their health would be regularly monitored (Cole et al., 2019). Access to health care services often did not coincide with the workers’ off-duty hours (Caxaj et al., 2023; Preibisch & Hennebry, 2011) and the MFWs often could not maintain follow-up care (Cole et al., 2019). As a result, MFWs often self-medicated with painkillers or herbal medications from their own country and continued working without proper investigations or diagnoses (Viveros-Guzmán & Gertler, 2015).
The COVID-19 pandemic was found to disproportionately affect MFWs, and their limited knowledge about accessing health services contributed to this issue (Arya et al., 2021). Often, workers did not know where to get tested or how to book a COVID-19 test (Arya et al., 2021). This made testing, an essential public health measure, inaccessible to this vulnerable group (Arya et al., 2021). The COVID-19 deaths of nine MFWs in Ontario between January 2020 and June 2021 highlighted the seriousness of the issue (Caxaj et al., 2022a). During the pandemic, these workers struggled to navigate, advocate for themselves, and access medical care quickly, which led to some losing their lives (Caxaj et al., 2022a).
Restrictive Work Schedules
Long workdays were the norm for MFWs (Arya et al., 2021; Pysklywec et al., 2011; Salami et al., 2016), and most were unwilling to take time off to access health care services, fearing loss of employment, hours, or wages (Arya et al., 2021; Caxaj & Cohen, 2021b; McLaughlin, 2009; Mema et al., 2021; Preibisch & Otero, 2014; Pysklywec et al., 2011; Salami et al., 2016). Employers were not willing to give MFWs time off unless it was a life-threatening situation, and taking time off resulted in pay deductions; workers expressed wishing that clinics were open in the evenings and on weekends (Narushima et al., 2016). Restrictive work schedules also limited MFWs’ access to various health-promoting programs and services (Caxaj et al., 2024). Employers often showed disinterest in such programs, stating that workers could not attend programs that ran during work hours (Narushima & Sanchez, 2014). This forced MFWs to prioritize earning wages over their health (Salami et al., 2016; Stasiulis, 2020). With long working hours (50–60 per week), strict schedules, and no paid sick leave, taking time off to seek medical care was not feasible (Caxaj & Diaz, 2018; Caxaj et al., 2024; Cecco, 2024; Edmunds et al., 2011; Gallant et al., 2010; Hennebry et al., 2016; Vosko et al., 2022; Wong et al., 2021).
MFWs were regarded as front-line staff during the COVID-19 pandemic, a role that made them vulnerable (Arya et al., 2021). They needed more time off to access COVID-19 testing centres (Arya et al., 2021). Even when tested, they feared isolation, missing work, and losing wages (Arya et al., 2021). An outbreak investigation at a nursery and garden center in British Columbia revealed that workers feared losing their jobs and wages if they reported COVID-19 symptoms, resulting in a total of 26 confirmed COVID-19 cases in this agricultural setting (Mema et al., 2021).
Health Care Coverage
Despite being legally entitled to health care, MFWs often struggle with delayed insurance coverage, employer interference, and limited insurance acceptance (Caxaj & Diaz, 2018; Caxaj et al., 2023; Edmunds et al., 2011; McLaughlin, 2009; Mema et al., 2021). Many MFWs do not have, or struggle to use, an OHIP card (Wong et al., 2021). Workers, employers, and health care providers also require more knowledge regarding processing claims, health coverage, and accessing health benefits (Barnes, 2013; Narushima et al., 2016; Salami et al., 2015). Further, a three-month waiting period for OHIP leaves workers uninsured upon arrival, forcing them to pay for medical expenses (Caxaj & Cohen, 2021b; Cole et al., 2019; Colindres et al., 2021; McLaughlin, 2009; Preibisch & Hennebry, 2011; Preibisch & Otero, 2014; Pysklywec et al., 2011; Salami et al., 2015; Stasiulis, 2020; Zhou et al., 2023). Coverage lapses upon job termination or repatriation, cutting workers off from necessary medical follow-up (Doyle, 2020; Glauser, 2014; Hennebry & Preibisch, 2012; Hennebry & Williams, 2015; Zhou et al., 2023). During the COVID-19 pandemic, out-of-pocket expenses limited access to health care (Colindres et al., 2021).
Few MFWs receive compensation when using a health card due to health providers’ lack of knowledge on processing claims, absence of a private address, or worker repatriation (Barnes, 2013). Some hospitals and clinics refused private insurance, leaving workers unable to receive treatment unless they could afford to pay upfront (Caxaj et al., 2023; Hennebry & Williams, 2015). Employers also withhold workers’ health cards, requiring them to disclose injuries before granting access to care, which discourages health care-seeking behaviour (Glauser, 2014; McLaughlin, 2009). Limited access to health coverage also restricts the affordability of prescription medications and dental care (Salami et al., 2018).
Contracted MFWs are covered by private insurance arranged by their employers and are also eligible for provincial health coverage after living in the country for three months (Cohen & Caxaj, 2018). In some cases, workers remain unregistered for provincial health care despite being eligible. Although the employer is responsible for enrolling them, many do not complete this process. Workers often hesitate to raise the issue with their employer, fearing it may affect their work status (Cohen & Caxaj, 2018). Private insurance coverage alone is inadequate, as many walk-in clinics, labs, and pharmacies do not directly bill private insurance companies. This means workers must pay for doctors’ visits, lab tests, and medications upfront and then submit claims for reimbursement later. This creates a financial barrier to accessing health care, especially when a single doctor's visit can cost upwards of $100, with lab tests being even more expensive (Cohen & Caxaj, 2018). By the time these claims are submitted and processed, the workers have often finished their contracts and left the country. Ultimately, private health insurance is meant to supplement, not replace, provincial health coverage, as it usually does not cover certain medical and surgical procedures.
Discussion
This scoping review mapped current literature regarding barriers that MFWs encounter when accessing health care services in Canada. Six themes emerged, including (1) Barriers Related to Language and Literacy, (2) Concern of Medical Repatriation, (3) Lack of Transportation, (4) Barriers to Timely Care and Medical Follow-Up, (5) Restrictive Work Schedules, and (6) Health Care Coverage. This review is novel in its examination of barriers to health care access for MFWs.
Sources used in the scoping review supported barriers previously noted in other studies. An older study by England et al. (2007) reported fear of medical repatriation as a barrier to health care access. This fear continues to be a barrier, and is reported more recently by 33 of the 39 sources in this review. In fact, fear of repatriation is the barrier mentioned most often in the sources in this review. Due to the workers’ fear of medical repatriation, they did not disclose an illness or injury and continued to work. Further, some clinicians participated in medical repatriation by creating care plans to support the employer rather than focus on the patient (Colindres et al., 2021). This leads to additional complications, including the spreading of disease, which happened with the COVID pandemic.
Over time, the fear of repatriation has been mentioned in literature; however, it is still as much of a concern in 2025 as it was in 2007. This barrier will continue to be prevalent until changes are made to the TFW programs that perpetuate the barrier. It is imperative that health care providers, including nurses, understand the notion of medical repatriation and its violation of human rights. Although framed as a win-win-win program, policies created under the SAWP contain structural flaws that exacerbate the workers’ risk of being medically repatriated (Hennebry & Williams, 2015). These policies do not protect the worker if an illness or injury is diagnosed. Therefore, a thorough review of the SAWP policies is necessary.
Barriers related to language and literacy were frequently mentioned in our sources after the fear of repatriation. Such barriers arise predominantly due to translation issues and comprehension. Accessible, high-quality language translation services are essential to facilitate communication; these services would reassure and boost the confidence of health care providers, including nurses, regarding the quality of care they deliver (Mota et al., 2015). Currently, services such as the Migrant Worker Community Program offer interpretation and translation services for various appointments. The continuation and expansion of translation services reduces barriers related to language and literacy, allowing better access to health care.
A notable barrier in the literature was the workers’ lack of transportation to access health care services. Many MFWs reside in remote locations far from public transit, thus making it difficult for them to access health care. The lack of transportation has also led to MFWS being killed while walking or riding their bicycles; many were hit-and-run cases (Barnes, 2013). Mobile clinics that transport health care providers directly to the workers alleviate the need for the MFW to go to a health care facility. Mobile clinics allow MFWs equitable and affordable access to health care services. There are currently several mobile health clinics operating in various locations across Canada, with the first created in 1996; in 2021, there were 26 mobile clinics in operation, with most in Ontario (Nguyen et al., 2021). The addition of mobile clinics should provide better health care access. Additional research is needed to assess the effectiveness of mobile clinics. Besides mobile clinics, launching the support model intervention shows promise. The percentage of workers using support groups for help with translation, transportation, or legal advocacy has increased from 15% (Colindres et al., 2021) to 60.8% (Caxaj et al., 2022a).
Sources in our scoping review described challenges that MFWs encounter when navigating Canada's complex health care system. Challenges occur because of limited education, low literacy rates, and being new to the country. Comparably, Shmyr et al. (2022) found limited knowledge of preventative health and seeking help only after a chronic disease had developed. Current health care practices are falling short of accommodating and caring for individuals with limited education and literacy levels. Considering their vulnerability, MFWs would benefit from increasing health literacy through health promotion programs implemented by public health nurses. Nurse practitioners can play a crucial role by implementing screening for chronic diseases, mental illness, sexually transmitted diseases, and occupational injuries in primary care settings.
Regarding the COVID-19 pandemic, it is important to note that it does not constitute an additional barrier. The barriers outlined in this scoping review are longstanding and were intensified for MFWS during the pandemic.
Limitations
There were limitations to this review. This review did not assess the quality or risk of bias in the studies included, which limits the authors’ ability to comment on the strength or validity of the evidence. Due to the inclusion of diverse study designs, grey literature, and non-peer-reviewed sources, variability and consistency across findings can increase. The researchers’ interpretation can influence thematic synthesis, which may affect reproducibility. The database searches were conducted on July 24th, 2024, with no specified start date. Articles published after this search date would have been missed. Although several websites focus on MFWs, keywords related to the topic might have limited access to grey literature sources. Similarly, specific journal articles would have also been missed and omitted if they did not contain the keywords utilized for the search. The health sciences librarian designed and conducted the search to ensure the robustness of the search strategy. All relevant databases were searched, including Scopus, which covers interdisciplinary areas not well covered by the comprehensive nursing and allied health database.
Conclusion
Migrant farm workers represent a growing and essential demographic in Canada, filling critical labour shortages, cultivating the nation's food supply, and playing a vital role in reducing food insecurity. This scoping review identified specific barriers that MFWs face when accessing health care services in Canada. These include language and literacy challenges, concerns of medical repatriation, transportation issues, delays in care and follow-up, restrictive work hours, and problems with health coverage. Recognizing these particular obstacles is essential for developing interventions that are responsive, culturally safe, and effective. A deeper comprehension of these challenges can serve as a catalyst for designing tailored health strategies that promote better health outcomes. Given their vulnerable position, a key implication from this scoping review is to ensure that MFWs have timely and equitable access to comprehensive health care services while living and working in Canada, regardless of their employment or immigration status. Moreover, by bringing these barriers to light, this review offers a valuable map of the scope, nature, and complexity of the obstacles confronting MFWs in accessing health care in Canada.
PRISMA-Scr diagram. Source: Page MJ, et al. BMJ 2021;372:n71. This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/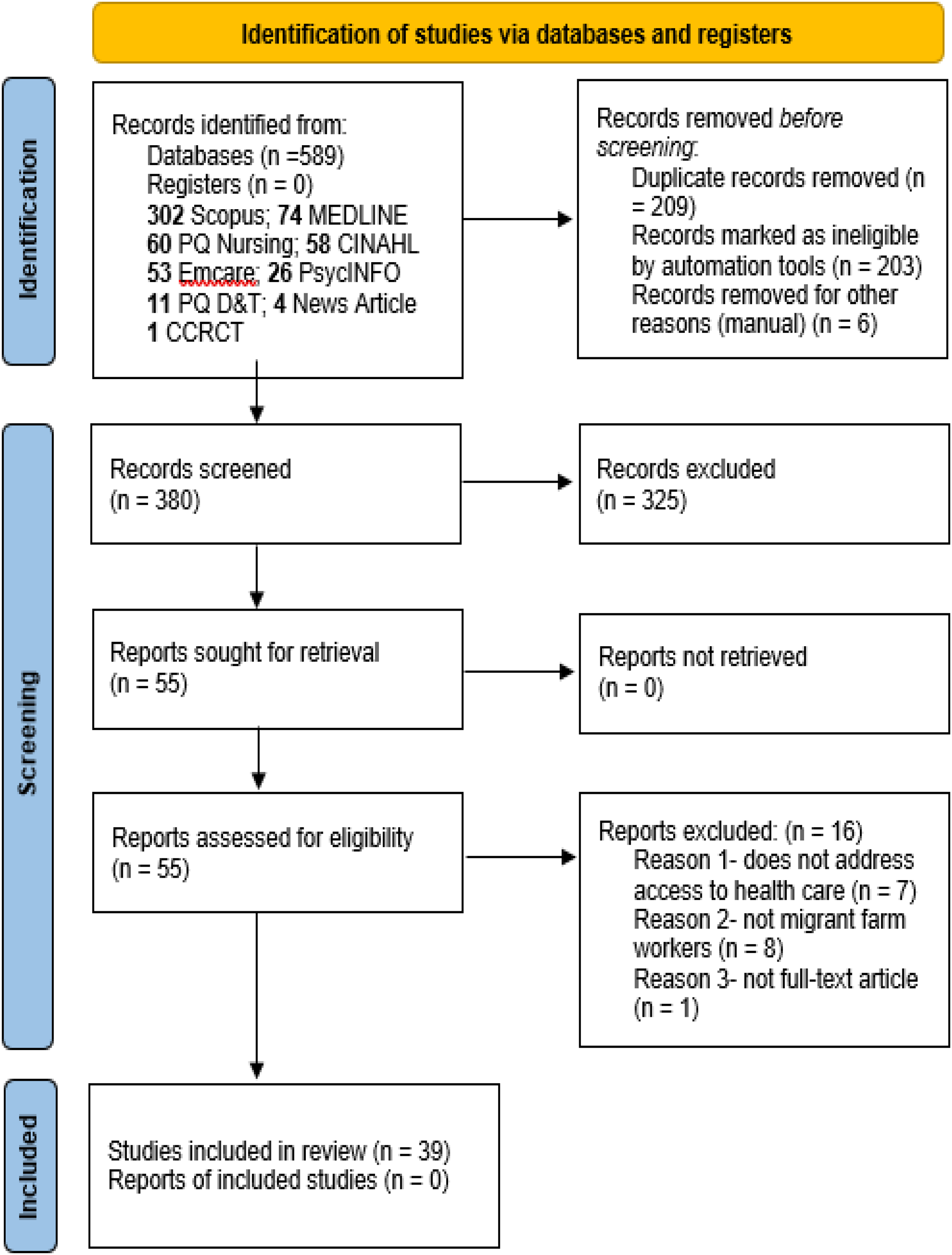
Supplemental Material
sj-docx-1-cjn-10.1177_08445621251415252 - Supplemental material for Barriers Encountered by Migrant Farm Workers When Accessing Health Care Services in Canada: A Scoping Review
Supplemental material, sj-docx-1-cjn-10.1177_08445621251415252 for Barriers Encountered by Migrant Farm Workers When Accessing Health Care Services in Canada: A Scoping Review by Sharona Naidoo, Sherry Morrell, Jamie Crawley, Gina Pittman, Adam Mulcaster, Kathryn Pfaff, Joanne Tay, Gauri Kumar and Kaitlynn Scott in Canadian Journal of Nursing Research
Footnotes
Ethics Approval
Ethical approval was not required for the scoping review
Consent to Participate
‘Not applicable’
Consent for Publication
‘Not applicable’
Author Contributions
SN: design, screening, full-text review, extraction, writing, editing; SM: screening, full-text review, extraction, writing, editing; JC: screening, full-text review, extraction, writing, editing; GP: writing, editing; AM: search strategy, writing, editing; KP: writing, editing; JT: writing, editing; GK: extraction, editing; KS: extraction, editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
‘Not applicable’
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.