
Abstract
Acute care delivery creates secondary health risks to patients, health care workers, and the environment through a complex waste stream, intensive energy use, and frequent use of harmful chemicals. Nurses are among the most affected by these risks and are also pivotal change agents in reducing the negative impacts of health care delivery. Assessing nurses’ understanding of health care–associated environmental health risks is essential if care is to be delivered in an environmentally safe and healthy manner, as indicated by published professional standards of nursing practice. However, psychometrically sound instruments that measure nurses’ awareness of the environmental impacts of nursing practice are not available. To address this gap, a prototype of the Nurse’s Environmental Awareness Tool (NEAT) was developed. Seven content experts in environmental health nursing and/or psychometrics were asked to review draft items. Comments were analyzed and applied to the scale items. Several revisions from the original item pool were made. The resulting draft NEAT includes six subscales, in three paired subsets. This article provides a summary of the process of item development and scale design. These findings, although preliminary, provide a foundation for subsequent psychometric testing. The result of this study is the creation of an instrument to measure nurses’ awareness of and behaviors associated with the environmental impact of their practices.
Health care delivery negatively impacts the natural environment (Hall, 2010). Pollution is generated from toxic chemicals and intensive energy use (Healthcare Without Harm, 2006). Excessive waste is produced, linked to pollution from waste management and resource depletion (Practice Greenhealth [PGH], 2012b). A range of toxic chemicals are used in diagnostic methods, therapeutics, and maintenance of practice sites (Wilding, Curtis & Welker-Hood, 2009). Nursing has a professional practice standard stating that “the registered nurse practices in an environmentally safe and healthy manner” (American Nurses Association, 2010, p. 61). Yet little is known about nurses’ awareness of or behaviors associated with these negative impacts of their practice; no psychometrically analyzed tool measuring these issues currently exists. The authors set out to create a tool to measure nurses’ awareness of these impacts and nurses’ behavior in response. This article describes the conceptual framework underlying the instrument, and the item development phase of the instrument, including how content for the items was identified, and changes in items based on findings from interviews with several content experts across the nation.
Conceptual Framework
The Energy, Waste, Toxicants, and Engagement (EWT-E) Wheel
Review of the literature led to the creation of the EWT-E Wheel (Schenk, 2011), a conceptual model incorporating a large number of environmental impacts arising from health care. It sorts environmental impacts into three major concepts: energy/water, waste, and toxic chemicals. These concepts are situated within the concept of engagement, which refers to attitude, awareness, knowledge, and action. The EWT-E Wheel is shown in Figure 1.
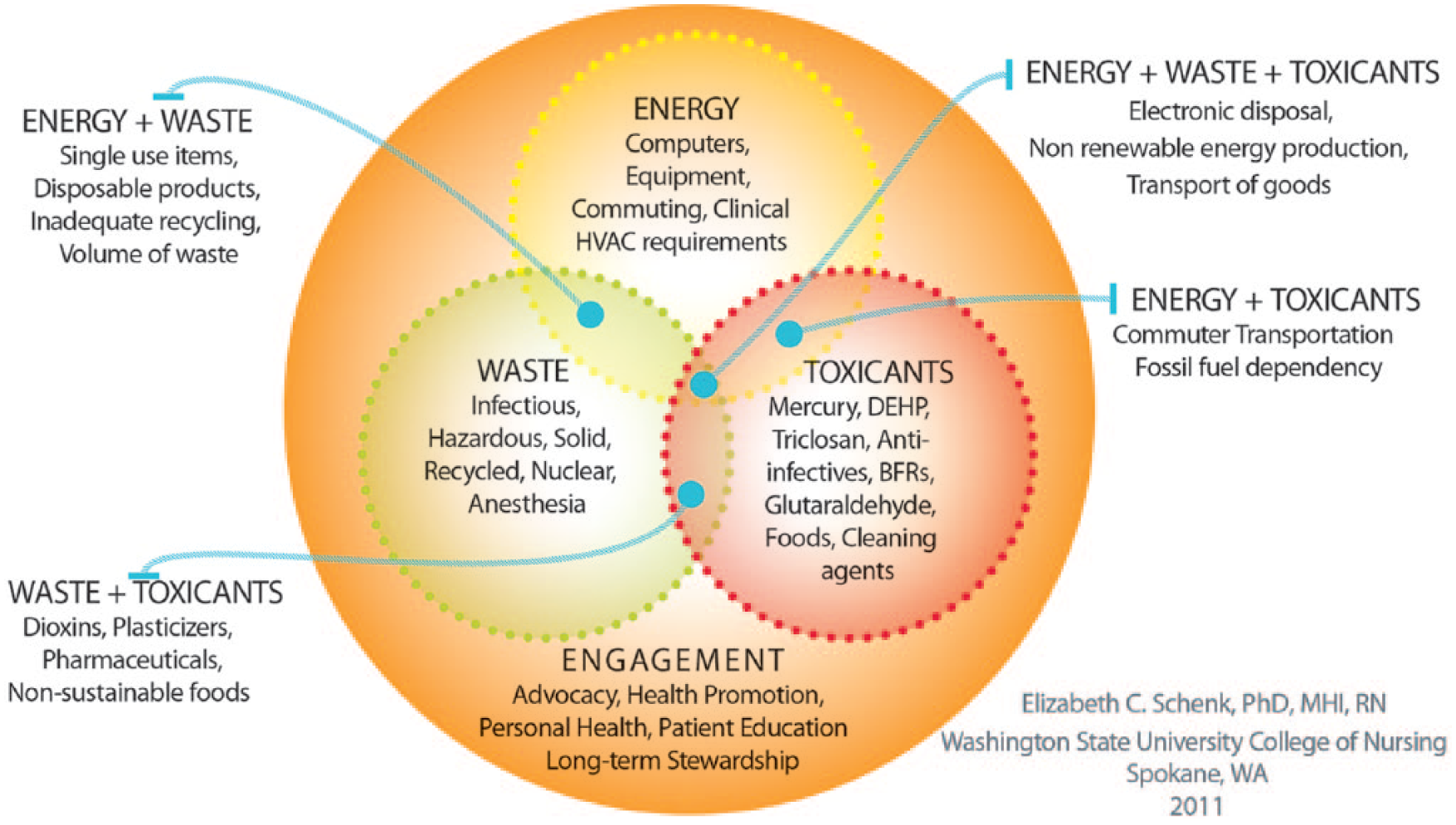
Environmental sustainability in nursing practice: The EWT-E Wheel.
Energy/water
Health care in general and hospitals in particular are extremely energy intensive, with substantial energy used day and night. Clinical care processes are highly dependent on electronic monitoring systems, intervention equipment, and medical records for documentation and communication. In addition, infection control requirements specify a high number of air exchanges per hour, up to 20 in operating room suites, and at least seven in patient rooms. Consequently, there are tremendous needs for heating, ventilation, and air conditioning (HVAC) equipment, which is typically the single most energy-intensive element of a hospital energy scheme (Healthcare Environmental Resource Center [HERC], n.d.). Nurses, in their roles as staff in acute care and other settings, and in their stewardship of their own practice, can influence energy use in their work through occupational behaviors, process development, and product choices.
Waste
Health care produces significant volumes of waste of multiple types, more than 6,000 tons per day (Hall, 2010), or 33 pounds per patient per day (PGH, 2012b). Some of the volume stems from the many disposable products used in health care. The disposable products are largely made of plastic, including syringes, tubing, tubs, and basins. Some materials are much more expensive and durable but still manufactured for single use.
Health care produces significant amounts of hazardous waste, including infectious (bio-hazardous), chemical, pharmaceutical, and nuclear waste. Treatment and disposal of infectious waste is expensive, costing up to five times as much as disposal of municipal solid waste (Minnesota Technical Assistance Program, 2011). Costs for infectious waste can be decreased through proper segregation of waste, ensuring that only waste that is at risk of being infectious is placed in the collection bins for infectious waste.
Chemical waste must be stored carefully, logged and manifested, and carried by a licensed hazardous waste carrier to a licensed hazardous waste incinerator. Nuclear waste is produced after diagnostic testing and treatment methodologies that use nuclear materials. It is highly regulated; disposal is regulated by the Nuclear Regulatory Commission (2012).
Pharmaceutical waste is a growing concern. Evidence indicates that surface and ground waters contain a variety of pharmaceutical compounds (Nilsen et al., 2007; Shah, 2010; Washington Department of Ecology, n.d.). Researchers are learning more about metabolic processing and optimal treatment and disposal methods. Nurses can play a role in careful stewardship of these chemicals (Becker, Mendez-Quigley, & Phillips, 2010) as well as of the entire waste stream.
Toxic chemicals
Numerous toxic chemicals are used in health care, including mercury, formaldehyde, flame retardants, phthalates, harsh cleaning chemicals, anesthesia gas, pharmaceuticals, pesticides, and others. Some pose a risk to workers or patients. Others pose a risk in the community, region, or planet-wide ecosystem services. Nurses are among the most exposed professions, and nurses can advocate for less harmful chemical use and improved protection from exposures.
Engagement
In the EWT-E Wheel model, the first three concepts, energy, waste, and toxicants, are related to the final concept, engagement. Integration of ideas related to energy, waste, and toxic chemicals requires engagement with the content. This implies increased knowledge and awareness of the related science, and better understanding of how the polluting aspects of health care create risks to personal, patient, and community health, and how nurses can advocate for practice changes. Engagement is depicted as underlying the other three concepts because it is a necessary component of understanding the risks that arise from environmental impacts of health care, and what nurses (and others) can do to reduce those risks.
Changing complex organizations such as hospitals or health care systems is daunting. It requires changing the behavior of many people, changing the structures in terms of policy and procedures, changing work processes, and, ideally, measuring outcomes based on goals. There is an opportunity for education, participation, advocacy, research, and behavior change with every new approach or initiative. Each of these actions is an aspect of engagement with this challenge. Consistent leadership and staff engagement in the process is crucial to the sustainability of any effort (Healthier Hospitals Initiative, 2012).
Clinicians, be they nurses, physicians, pharmacists, or other professionals, are responsible for their own practice and must be involved in decision making related to environmental impacts of their practice. For example, product selection is a complex endeavor, requiring clinical expertise to determine effectiveness of care, while considering resource use and pollution caused by a product or process. Clinical input into waste management is important to prevent harm from exposures to hazardous and infectious materials, and also to address the resource intensity of their professional choices. These contributions require engagement with the topic of environmental impacts of practice so the clinicians have the opportunity to learn, educate, and advocate for more environmentally sound practices.
Links to Human Health: The EWT-E Shadow
Impacts to the natural environment stemming from health care as identified in the EWT-E Wheel are associated with negative human health risks. Some of the potential resultant health risks are identified in the EWT-E shadow (Figure 2; Schenk, 2013).
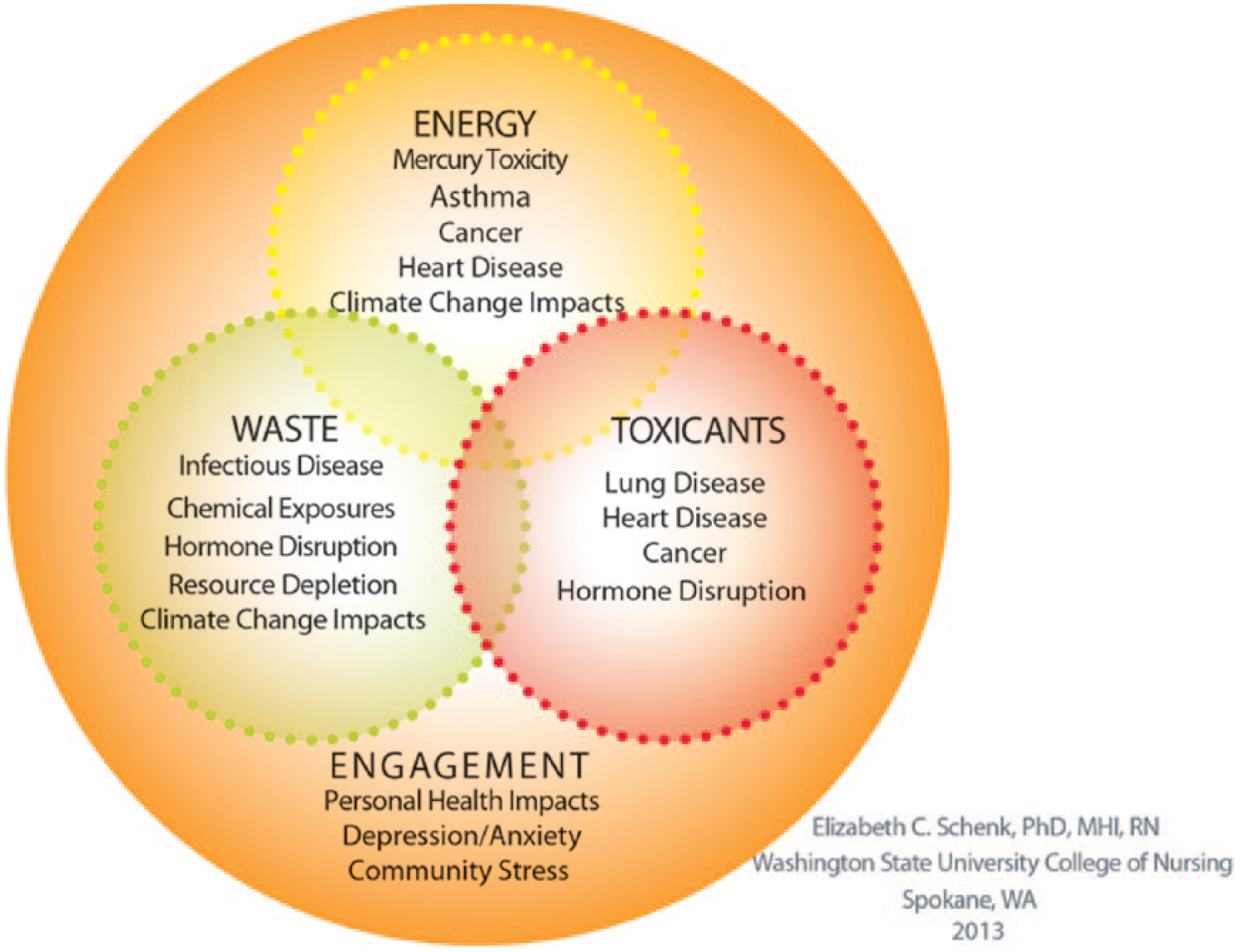
The EWT-E shadow: Health risks from environmental impacts of health care delivery and nursing practice.
Energy/water
Energy use creates risks for human health. The majority of U.S. electricity is fossil fuel derived primarily through the burning of coal but also from natural gas. Burning coal contributes pollutants to the atmosphere including mercury, sulfur dioxide, and nitrous oxides, which harm health (Lockwood, Welker-Hood, Rauch, & Gottlieb, 2009). The Environmental Protection Agency (EPA; 2010) reported that the health care sector’s use of 73 trillion kilowatt hours (kwh) of electricity results in US$600 million per year in additional health care costs. In addition, health care energy use contributes greenhouse gases, which contribute to climate change, which in turn causes significant health problems (Farquhar, 2010; Forastiere, 2010; World Health Organization, 2010). U.S. health care is said to be responsible for 8% of the nation’s greenhouse gases (PGH, 2012a).
Waste
Infectious and hazardous waste, if not disposed of and treated properly can lead to health risks from exposures to infective agents or toxic chemicals. Although some aspects of the hazardous waste stream are regulated (nuclear, chemical hazard, and infectious), others are not (non-designated pharmaceutical waste, electronic waste). Responsible segregation, including beyond what is required by law, is an attribute of safe practice. In addition, waste in landfills creates significant greenhouse gases through methane formation, a potent greenhouse gas (EPA, 2015). Greenhouse gases have been associated with climate change (Energy Information Administration, 2004; Solomon, 2007) and numerous associated health risks (Barna, Goodman, & Mortimer, 2012; Maccabee, 2010; Portier et al., 2010).
Toxicants
As recently as 2002, health care was responsible for 10% of mercury, a potent neurotoxin, in the environment (World Health Organization, 2005). Polyvinyl chloride (PVC) and plasticizer phthalates are heavily used in many plastic health care products. On the creation and destruction (if incinerated) of PVC, carcinogenic dioxins are released into the atmosphere. Phthalates are hormone-disrupting chemicals, which can enter the bloodstream of patients who are subjected to these chemicals in intravenous line tubing and other devices, such as ventilator tubing, oxygen cannulas, and indwelling catheters (Healthcare Without Harm, 2006). Pharmaceuticals often have carcinogenic, teratogenic, and genotoxic risks, requiring safe handling and personal protective equipment (American Journal of Health-System Pharmacy, 2006).
Engagement
Human health risks related to
Engagement in the workplace to improve environmental health is important (Chenven & Copeland, 2013; Dunphy, 2013). Supporting staff to decrease the environmental impacts of their work, and decrease environmental exposures with the potential to impact their health, may provide new opportunities for job satisfaction and self-efficacy. The level of engagement nurses have in decreasing the environmental impacts of their workplaces is unknown, though it may be an important element of satisfaction.
The Integrated Change (I-Change) Model
In the I-Change Model (deVries et al., 2003), awareness is one of several precursor conditions to behavior change. Although not the only element affecting the likelihood of adoption of new behaviors, it is a necessary one. The I-Change Model has been used to describe behavior change in skin cancer prevention (deVries, Lezwijn, Hol, & Honing, 2005) and breast feeding (Kools, Thijs, Kester, & deVries, 2006). The linkage between awareness and behavior in the I-Change Model supports the development of subscales in a measurement instrument that relates awareness of environmental impacts of nursing practice to mitigating behaviors practiced by the responding nurses.
Purpose of Study
By studying nurses’ awareness of environmental impacts of nursing practice, the profession will be better prepared to develop goals, plans, and strategies to mitigate harm. A broad-scale survey instrument will allow researchers to assess nurse awareness and behavior regarding the environmental impacts of nursing practice. The Nurses’ Environmental Awareness Tool (NEAT) will provide the first psychometrically evaluated tool by which to gather data on this topic. NEAT will offer a foundation for further research, education, advocacy, and practice changes that could decrease unintended harmful environmental impacts of nursing practice.
Method
Item Development Phase
An extensive review of related theory and instruments was performed. Several databases were searched, including CINAHL, PubMed, PsychInfo, and GreenFILE, an EBSCO database focusing on human impact to the environment. Search terms such as nursing theory, environmental health, environmental sustainability, nursing practice, green hospitals, awareness, and behaviors were used. No theories or conceptual frameworks were identified that directly support the area of research interest. However, as mentioned above, the I-Change Model linked awareness and behavior, and the EWT-E Wheel provided a framework for the content of items pertinent to the environmental impacts of nursing practice. The structure of the subscales in NEAT were developed to link awareness of environmental impacts of nursing practice to associated behaviors in each of the concepts outlined by the EWT-E Wheel: energy/water, waste, toxic chemicals, and engagement.
Item Pool Generation
Item pool generation for this proposed study was organized by the concepts of the EWT-E Wheel: energy/water, waste, toxicants, and engagement. Two constructs were addressed: awareness of environmental impacts of nursing practice and ecological behaviors—actions that exert no or low impact on the natural environment. A pool of 160 items reflecting the four concepts of the EWT-E Wheel in the two constructs listed above were generated, including some redundant items. The items were written using the criteria for developing clear items.
Likert-type scales were defined for each subscale, using a range of five options in each case. The responses were parallel for the different sections, with “1” always the least and “5” always the most, whether the item addressed awareness or behavior.
For the NEAT, two elements were used that serve to decrease the risk of participants answering in a biased manner. First, respondents were asked to what degree they were aware of a factual statement versus being asked whether they agreed with the statement. Second, to reduce respondent tendency to over-report ecological behaviors, each question about behavior was followed by an assessment of the difficulty of the behavior. The assumption was that if participants can clarify that a behavior is difficult, they would be less likely to exaggerate how much they carry out that behavior.
Participants
For this research study, interviews with several content experts (n = 7) from around the nation were conducted. The experts were recruited through professional contacts, from identification of contributing authors in the literature, and from snowball recruitment by which one expert suggested others.
Process
After institutional review board (IRB) exemption was obtained, interviewees were individually contacted by email to ascertain their interest in participating. Hour-long phone interviews were scheduled with those who responded that they were willing and interested in participating. Notes were kept for each interview, identified by date and initials.
The draft item pool (n = 160) that was created following a literature review, as well as samples of the content expert interview questions, was sent to the participants. A series of questions were asked of the content experts to understand their perspective on the relevance of the proposed items, the clarity of wording, and ideas about what topics or areas may be missing, or alternatively, inappropriate for inclusion. Suggestions were made regarding selection of items, wording, order, and format based on interview discussions.
After each interview, the notes were reviewed and the draft pool updated to reflect those suggestions that fit with the overall purpose and strategy of the tool. For each ensuing interview, the updated item pool was sent after modifications from prior interviews were made. In this way, the draft instrument moved closer to representing a view reflective of the input of all interviewees. At the end of the item development phase, the draft of NEAT was completed and contained 48 two-part items.
Results
Several primary changes were adopted from the first five interviews, leading to the Midpoint Draft Item Pool, examples of which are shown in Table 1. Comments from the content experts and changes in the draft tool resulting from those interviews are summarized in Table 2. Significant changes included (a) reducing items in each section (from 160 items in original pool to 66 items in the midpoint draft, excluding demographic questions), (b) linking environmental impacts to human health risks by using a two-part response format, (c) adding several items on topics the experts felt were missing, (d) separating home and work behaviors and establishing the two-part response format in that section, (e) eliminating items that were felt to be too specific to a particular nursing focus, and (f) deleting items from the Connectedness to Nature Scale (CNS; Mayer & Frantz, 2004) that were included in the initial draft items but found to fit poorly with the EWT-E concepts.
Summary of Content Expert Input
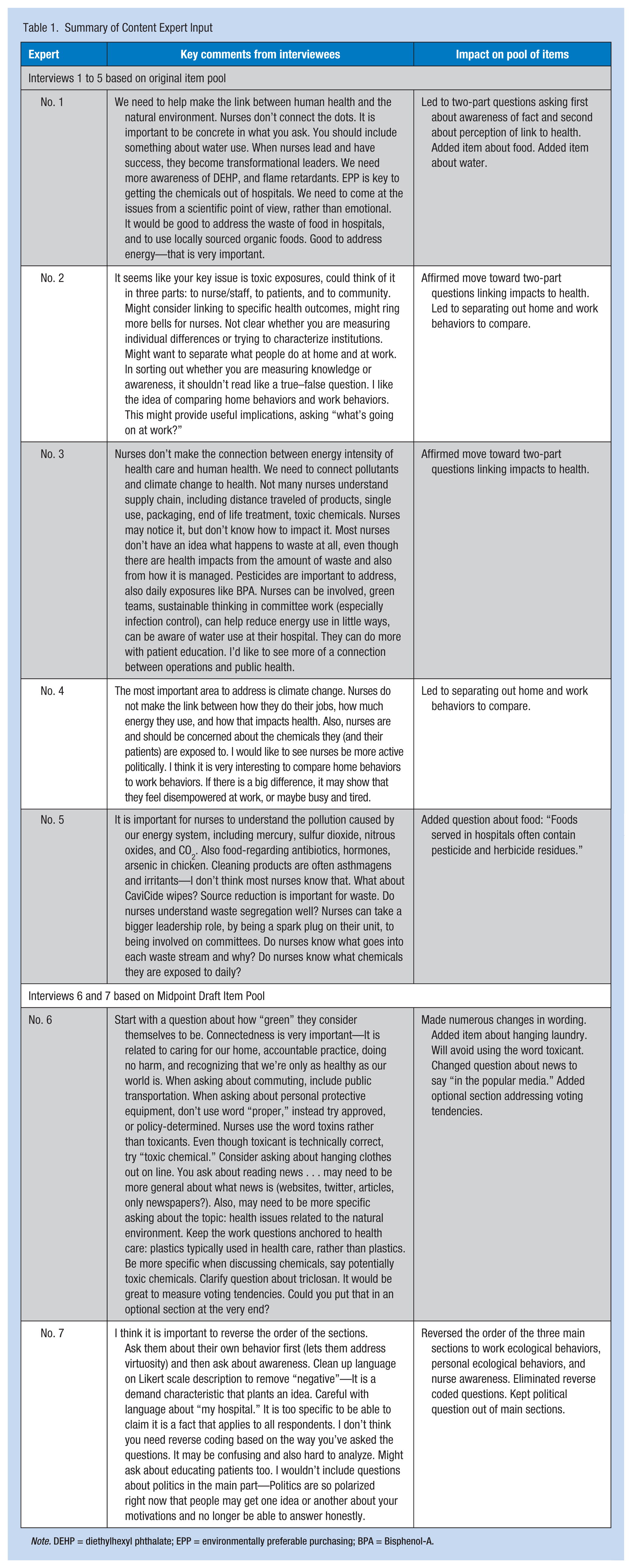
Note. DEHP = diethylhexyl phthalate; EPP = environmentally preferable purchasing; BPA = Bisphenol-A.
Example Items and Format From Midpoint Draft of NEAT
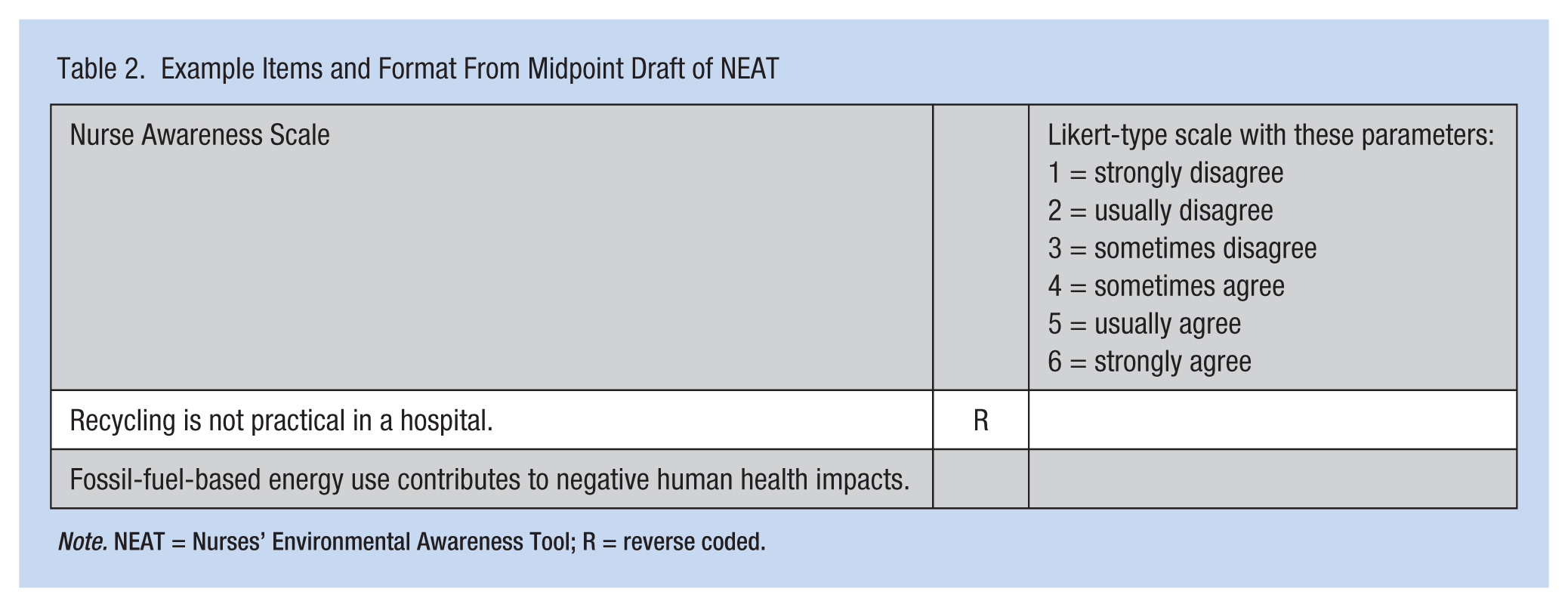
Note. NEAT = Nurses’ Environmental Awareness Tool; R = reverse coded.
The remaining two interviews addressed the content expert questions starting from the midpoint draft of NEAT. Several other significant changes were made at this point. Reverse-coded items had been included in the first two drafts to deter respondents from answering with a uniform blanket response. It was decided that the two-part response format would address the issue of uniform responses and reverse coding was eliminated. Several additional wording changes were made to the items based on suggestions from the last two interviews. Last, an optional demographic section was added at the end of the instrument to inquire about voting tendencies. Example items are presented in Table 3.
Example Items and Format From Final NEAT
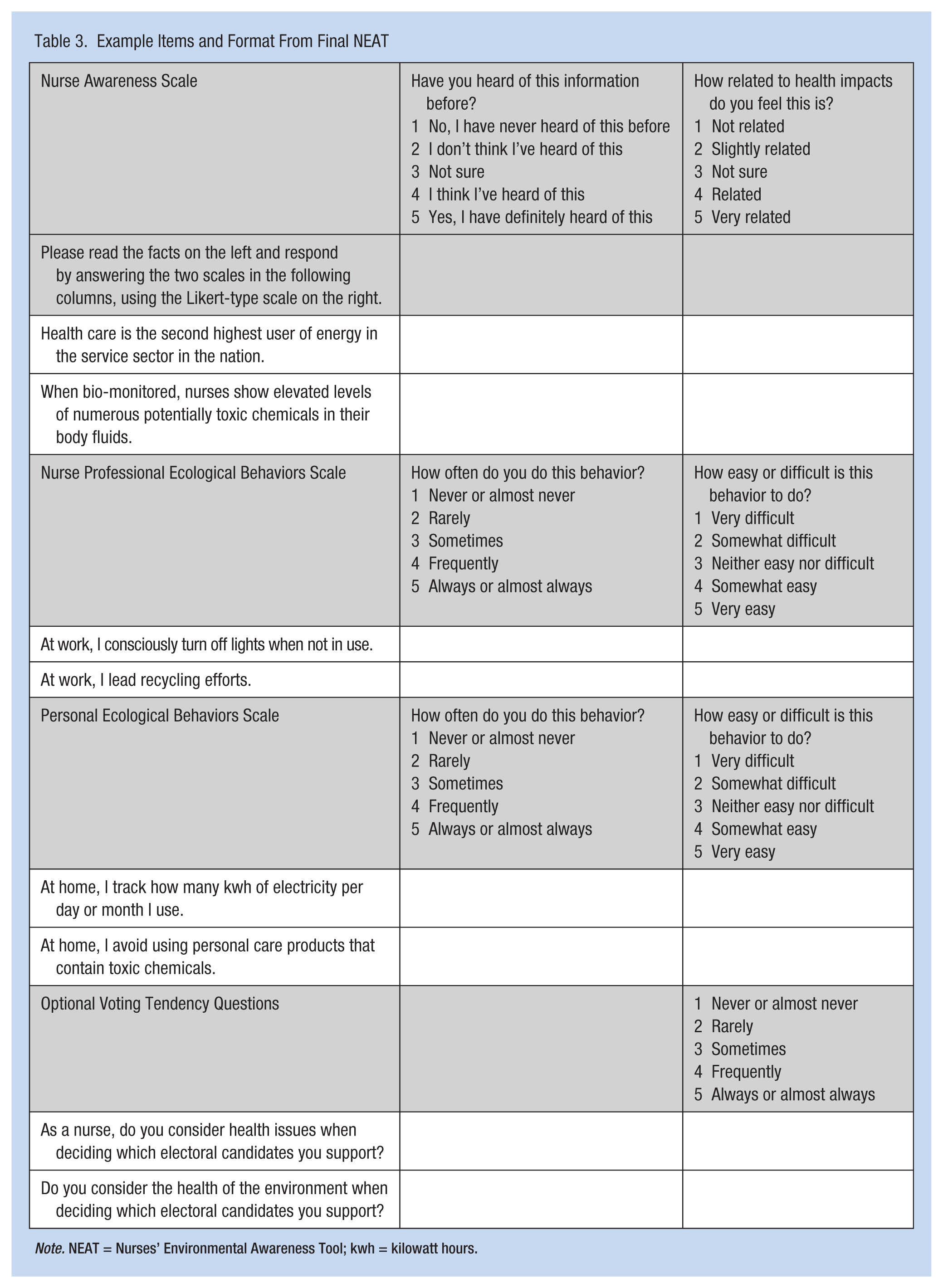
Note. NEAT = Nurses’ Environmental Awareness Tool; kwh = kilowatt hours.
The two-part response format was a significant change in the development of the NEAT. It emerged from conversations with content experts who said that it was important to link awareness of environmental impacts to awareness of the health risks of those impacts. The format for the nurse awareness paired scales offered a statement of fact about a particular environmental impact of nursing practice. Each statement was followed with a question asking about the respondent’s familiarity with that fact, and second, about the respondent’s belief that the environmental impacts are linked to human health effects. The two-part format helped establish a link between environmental impacts and human health risks. Examples of paired awareness items are shown in Table 3.
Another set of paired scales addresses nurses’ professional ecological behaviors. A behavior is listed, and participants are first asked how often they perform that behavior. A second inquiry asks how easy or difficult doing that behavior is for them. The final set of paired scale items repeats this format for personal ecological behaviors. Structuring the behavioral items in this format may reduce a tendency to answer with a socially desirable bias, as each respondent has the opportunity to comment if a behavior is particularly difficult, which may help avoid answers based on desirability.
Discussion
The revisions made in items included in the final draft were each important to create a tool that was thought to be easy and satisfying to answer, while collecting the desired range of data. The decision to link the environmental impacts to human health risks in a paired set of questions solved several problems. First, knowledge of nurses’ awareness of environmental impacts is interesting but does not point to a relevant clinical action. When coupled, item by item, with nurses’ perception of related health risks, knowledge will be gained about what risks nurses may be willing to address based on expected patient outcomes. Second, by formatting the paired questions in an easy to follow sequential set, intuitive flow of the questioning was achieved, which set the pattern for the other two pairs of scales.
Through the interviews with content experts, it was decided to approach home and work behaviors separately (rather than behaviors in general), allowing comparisons to be made between home and work behaviors that will lead to questioning about potential organizational barriers to ecological behaviors in the workplace. It will also allow comparisons to be made based on work unit, or factors related to home life.
Some items were added if several content experts thought they were important. These included asking about sustainable food systems and water conservation. Others were dropped, particularly if too specific to a particular area or focus of nursing practice.
An optional section was added about voting tendencies, and at the recommendation of one of the content experts, this was placed at the end of the instrument, lest respondents feel agitated or suspicious that a particular political motivation was intended by the measurement.
Each of these changes strengthened the draft tool, including a broad range of questioning in an efficient and meaningful format. The changes led to creating a more coherent tool, with repeating patterns of questioning across the three sets of paired scales, lending a unified voice to the items.
Compelling evidence suggests that environmental degradation creates risks for human health. Health care and nursing practice contribute to environmental degradation and subsequently exert unintended detrimental effects on public health and nurses’ health. The nursing profession is accountable for its practice and any unwanted risks associated with it. However, this topic has been only minimally addressed in the scientific literature. Little is known about nurses’ awareness of the environmental impacts that result from nursing practice. An instrument, NEAT, has been developed to measure nurses’ awareness of these issues and nurses’ related behaviors. The tool is now ready for testing and psychometric analysis. It is believed that the NEAT will substantively advance the ecological science of nursing practice, contributing to nurses’ understanding of the profession’s awareness of and behaviors toward mitigating the environmental impacts of nursing practice.
Implications for Practice
The American Nurses Association Scope and Standards of Practice addresses environmental health in Standard 16, which states, “The registered nurse practices in an environmentally safe and healthy manner” (American Nurses Association, 2010, p. 61). This study, and the future testing of NEAT, will help nurses measure and analyze aspects of the environmental health and safety of their practices.
Opportunities for research and education will emerge based on findings from this study. Nurse researchers may more deeply analyze environmental impacts stemming from nursing practice. Researchers may study effective mitigation strategies to reduce harm. Researchers may examine more closely risks to nurses’ health, such as those arising from exposures to chemicals in the workplace. Educators may include more environmental health content into courses, study projects, and clinical learning situations. Nurses may evaluate their practice and increase awareness of environmental issues through ongoing education about or intermittent focus on these topics. Clinical nurses, with nursing leadership, may analyze what organizational barriers to environmentally safe and healthy practice exist in their workplace, and how they might be removed.
To date, most clinical education does not address the environmental impacts of practice, so clinicians are typically ill prepared to consider the environmental impacts of their work. Educational curricula need to include content about how practice impacts the environment and why nurses should be concerned. Effective educational strategies will include examples of best practices and an exploration of innovative solutions not yet in place. A focus on environmental impacts of nursing practice presents an opportunity to educate about health system operations and how clinicians may adopt more ecologically sustainable behaviors at work and at home.
It is established in the scientific literature that environmental degradation harms health, and that health care and nursing practice contribute to environmental degradation. Nurses around the nation have contributed to understanding this phenomenon better, and to asking hospitals and health care institutions to reduce these negative impacts. However, this conversation has not, to date, been held in the scientific literature. Use of the NEAT will help nurses, with scientific rigor, analyze their awareness of these impacts, and behaviors they are currently taking to reduce them.
Limitations
There were several limitations to the study. There was little guidance in the literature for the topic of nurses’ awareness of the environmental impacts of nursing practice. Language used in item development has not been previously tested, so it is unclear what will be most effective. The content addressed in the instrument is broad, making it challenging to organize into a usable form. Although narrowed after consultation with content experts, further study is required to determine the practicality of its use.
Conclusion
In summary, the NEAT consisting of 48 two-part items has been developed. Interviews with content experts in the field contributed to content validity of the instrument. The tool consists of three sets of paired scales. The Nurse Awareness Scales (NAS) are developed to measure nurses’ awareness of several environmental impacts of nursing practice and their perception of relatedness of these risks to human health. The Nurse Professional Ecological Behaviors Scales (NPEB) measures nurses’ workplace behaviors to mitigate environmental impacts, as well as how difficult or easy nurses perceive it is to perform them. The Personal Ecological Behaviors Scales (PEB) measures nurses’ behaviors outside of the workplace to mitigate environmental impacts, and how difficult or easy nurses perceive it is to perform those behaviors. Next steps in developing the NEAT include testing and psychometric analysis of the scales. Refinement and use of the scales will allow researchers to measure nurse awareness and behavior in this otherwise under-researched area.
Applying Research to Practice
Environmental degradation harms health, and healthcare and nursing practice contribute to environmental degradation. However, it is not known to what degree nurses are aware of this phenomenon. The Nurses Environmental Awareness Tool (NEAT), a group of six scales to measure nurse awareness of the environmental impacts and nurse behaviors to reduce these impacts at work and home, is in development. Item development is complete after this study, reflecting the input of content experts from around the nation, as reviewed here. The NEAT will give practicing nurses, educators, and researchers a tool to analyze nurses’ awareness of environmental impacts of their practice and behaviors they are currently taking to reduce them.
Footnotes
Acknowledgements
The authors thank the content experts interviewed for this study for their valuable insights: Denise Choiniere, MS, RN, Director, Materials Management and Sustainability at the University of Maryland Medical Center; Jane Dixon, PhD, Yale University College of Nursing; Kevin Dohr, PhD, Missoula, Montana; Anna G. Hall, RN, formerly Executive Director of Practice Greenhealth; Jocelyn Orb, RN, Sustainability Coordinator of Saskatoon Health Region; Joan Plisko, PhD, Director of Maryland Hospitals for a Healthy Environment; Barbara Sattler, DrPH, RN, University of San Francisco School of Nursing and Health Professions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Elizabeth Schenk is an assistant research professor at Washington State University and a nurse scientist at Providence Health & Services. Her research interest is the environmental impacts of nursing practice.
Patricia Butterfield is a professor and Dean Emerita at the Washington State University College of Nursing. Her work addresses conceptual foundations of environmental health, the reduction of household environmental health risks through nursing actions, and occupational and environmental epidemiology.
Julie Postma is an associate professor at the Washington State University College of Nursing. Her scholarship is focused on environmental health promotion and environmental justice.
Celestina Barbosa-Leiker is an assistant professor and PhD program director at the Washington State University College of Nursing. Her research interest is in identifying psychosocial predictors of substance abuse, cardiovascular and kidney disease, and other adverse health outcomes.
Cindy Corbett’s research focuses on health services interventions to improve health care quality and patient outcomes. She is currently a professor and the interim dean at Washington State University College of Nursing.