
Abstract
This research was designed to determine the impact of assertiveness training on the mobbing experience of nurses. This study was conducted in two phases. In the first phase, 218 nurses completed the mobbing scale; the education group consisted of 38 nurses who received a score at or above 204 points. A total of 180 nurses were excluded from the education group because they received less than 204 points. The study was conducted with 30 nurses because 8 nurses did not agree to participate in the study. The 30 nurses received the assertiveness training program. Six months after training, the nurses completed the mobbing scale and Rathus Assertiveness Inventory (RAI) again. The assertiveness training positively affected the assertiveness and mobbing scores (p = .000). After the training, the assertiveness scores increased and the mobbing condition score decreased (p < .01). Assertiveness training is an effective method for decreasing mobbing. In line with these results, training programs, which support nurses’ personal development by providing counseling and support to nurse victims of mobbing, are recommended.
Mobbing (i.e., psychological violence) in the workplace is defined as unethical communication and antagonistic action directed by one or several people toward a single individual systematically (Murray, 2009; Yildirim & Yildirim, 2007). Theoretically, mobbing is an extreme type of social stressor at work. Unlike most social stressors, however, mobbing is a long-lasting, escalated conflict with frequent harassing actions systematically aimed at a target individual (Leymann, 1996; Zapf, 1999). Bullying, on the other hand, connotes physical aggression by a single person, most often by a supervisor. Empirical studies have shown, however, that this differentiation is clearly not the case (Zapf, 1999). The term bullying is more often used in the United States, and mobbing is preferred in Europe (Heather, Grau, Finegan, & Wilk, 2010; Vandekerckhove & Commers, 2003). The concept of mobbing was introduced in Turkey between 1998 and 1999. The term mobbing is preferred in Turkish studies (Cevik Akyil, Tan, Saritas, & Altuntas, 2012; Gurhan, 2013; Okanli, Karakas, & Özkan, 2011; Ozturk, Yilmaz, & Hindistan, 2007; Ofluoglu & Somunoglu, 2012).
Mobbing occurs in workplaces almost everywhere in the world (Chappell & Di Martino, 2006), particularly prevalent in health institutions (Camerino, Estryn-Behar, Conway, van Der Heijden, & Hasselhorn, 2008; Efe & Ayaz, 2010; Khorsid & Akin, 2006; Milutinović , Prokes, Gavrilov-Jerkovié, & Filipović , 2009). Mobbing studies conducted in Turkey in recent years have reported various percentages of nurse victims: 70% (253 nurses; Dilman, 2007), 86.5% (505 nurses; Yildirim & Yildirim, 2007), 39% (814 nurses; Ozturk, Yilmaz, & Hindistan, 2007), and 17.4% (218 nurses; Okanli et al., 2011). A possible explanation for the lower frequency of reported mobbing in 2011 (Dilman, 2007; Yildirim & Yildirim, 2007) is exposure to high frequency mobbing in the past (Cevik Akyil et al., 2012; Okanli et al., 2011). The prevalence of mobbing in European Union countries has been reported to be between 4% and 15% (Báguena, Beleña, Toldos, & Martínez, 2011; Randolph Hillard, 2009; Vandekerckhove & Commers, 2003). Studies conducted with nurses who have experienced mobbing have demonstrated that mobbing leads to burnout, decreased job satisfaction, physical and psychological health problems, and post-traumatic stress disorder (Laschinger & Grau, 2011; Pai & Lee, 2011). Mobbing is of concern because it is associated with job satisfaction, performance, and turn over (Simons & Mawn, 2010). Mobbing is meant to force workers to quit their jobs by creating systematic pressure, limiting their ability to perform their jobs. Although mobbing is in general practiced by top-level executive staff, it can also be practiced by peers, subordinates, or a group of workers (Cobanoglu, 2005; Davenport et al., 2003).
Camerino et al. (2008) stated that psychological violence experienced by nurses in their workplaces creates negative working conditions. The most frequently cited individual risk factors for mobbing include low levels of assertiveness, lack of social skills, difficulty coping with difficult situations, and a few individual characteristics such neuroticism, trait anxiety, hostility, and aggression (Mościcka & Drabek, 2010). Other Turkish studies on mobbing have also reported that these individuals are challenged by self-improvement, self-expression, and communication (Adana et al., 2010; Efe & Ayaz, 2010; Ozturk, Yilmaz, & Hindistan, 2007).
Assertiveness is a communication skill influenced by cultural factors (Alberti & Emmons, 2002; Buzlu, 2006; B. Ozkan & Sevig, 2007; Yamagishi et al., 2007). The results of Turkish assertiveness studies have indicated that nurses who experience mobbing cannot assertively express themselves; they act passively or aggressively, and this behavior causes serious communication problems (Adana et al., 2010; Buzlu, 2006; Efe & Ayaz, 2010; Kutlu, 2009; B. Ozkan & Sevig, 2007). The study results have focused on the importance of assertiveness to nursing and health care (Buzlu, 2006; B. Ozkan & Sevig, 2007; Top, Kaymak, Gollu, & Kaya, 2010; Yamagishi et al., 2007). Assertiveness can strengthen health care team communication and enable workers to actively manage and prevent mobbing episodes and the conflict that can occur within a team (Efe & Ayaz, 2010; Milutinović et al., 2009; I. Ozkan & Ozen, 2008).
Studies about mobbing in Turkey and abroad have generally been descriptive; however, they do include suggestions on how to improve assertiveness and communication skills (Cevik Akyil et al., 2012; Efe & Ayaz, 2010; Heather et al., 2010; Milutinović et al., 2009; Mościcka & Drabek, 2010). Researchers such as Friedman, Wolpe, Lazarus, Liberman, Baker, Fiedler, and Beach who developed pre-testing or rehearsing behaviors also developed assertiveness training methods to increase individuals’ self-confidence, and know that, as a result, mobbing will not worsen. Training to improve assertiveness skills is based on psychoeducation-based programs that improve trainees’ social skills by facilitating interactions with other individuals (Gundogdu, 2012).
Nurses should design assertiveness training programs because (a) nurses need to practice active communication in a participatory setting to better master assertive strategies, and (b) in cognitive-behavioral therapy programs, such as assertiveness training, practical experience (experiential learning) is essential. It was hypothesized that experiential learning would be more effective in a participatory setting (Nishina & Tanigaki, 2013).
Studies of nurses have shown that assertiveness training has various beneficial effects such as boosting self-esteem and assertiveness, and reducing work stress (Nishina & Tanigaki, 2013; Yamagishi et al., 2007). A positive correlation exists between assertiveness, job satisfaction, and role clarity as well as the ability to handle stress and mobbing in the workplace. Assertiveness skills, therefore, can be used to counteract workplace mobbing as well as ameliorate stressful situations and increase empowerment (Begley & Glacken, 2004; Warland, McKellar, & Diaz, 2014). This training was chosen based on study results because it is an effective method for responding to mobbing. In addition, considering the general characteristics of the study group, assertiveness training is also needed. The aim of this study was to teach nurses to cope with mobbing by coaching them on assertiveness skills. This study was designed to determine the effects of assertiveness training on the mobbing that nurses experience.
Method
This study used a quasi-experimental single-group pre-test–post-test design. To define the sample, 218 nurses responded to a mobbing questionnaire; 38 of these nurses scored 204 or above on this scale. The remaining 180 nurses were excluded from the study because they scored less than 204. Only 30 nurses actually participated in the study because the other 8 eligible nurses chose not be participate. Because the study population was small, a sample was not selected. Rather the whole study population that agreed to participate were included.
Sample Inclusion Criteria
Mobbing score at or above 204 points;
No cognitive, hearing or verbal impairment that prevents communication; and
Willingness to participate in the study.
Instruments
A survey form was used to gather socio-demographic data along with the Rathus Assertiveness Inventory (RAI) and the Mobbing Scale, which the authors developed for nurses. The socio-demographic survey was composed of seven questions that recorded age, educational status, marital status, number of children, number of years nurses had worked in their current nursing positions, and the units on which they worked.
The RAI determined the assertiveness level of study nurses. The validity and reliability of the scale was determined by Voltan in Turkey (Oner, 1997; Voltan, 1980). Voltan determined that the Cronbach’s alpha coefficient for the inventory was 0.70 and the test–retest reliability was 0.92. Cronbach’s alpha coefficient of the inventory for this study was 0.70.
The inventory can be used with both adult and teenage participants. This 30-item instrument has a range between −90 and +90. Passivity is denoted by the −90 end of the range and assertiveness by the +90 end of the range. Options range from −3 to +3. Items 1, 2, 4, 5, 9, 11, 12, 13, 14, 15, 16, 17, 19, 23, 24, 26, and 30 are reverse scored to create a total score. Summing the minus and plus points and subtracting them from each other gives the total inventory score. Those who scored below +10 were classified as tentative, those who scored above +10 were classified as assertive, and those who scored +70 were classified as aggressive (Oner, 1997; Voltan, 1980). In this study, the power analysis for the RAI was found to be 0.97 with a 5% error-margin.
Ozturk et al. developed a mobbing scale in 2007, and validity and reliability studies were conducted. Ozturk reported a Cronbach’s alpha for the instrument of 0.97. The scale detects mobbing episodes and includes 68 items. The scale consists of positive statements; the possible responses are, “I definitely agree,” “I agree,” “I’m not sure,” “I don’t agree,” and “I definitely don’t agree.” The Mobbing Scale is based on a 68 to 340 score range. Those who scored above 204 demonstrated that they had experienced mobbing; those who scored below 204 had not experienced mobbing (Ozturk, Yilmaz, & Hindistan, 2007). The internal consistency of the mobbing instrument was found to be 0.95 in this study; the power analysis of the Mobbing Scale was found to be 1.00 with a 5% error-margin.
Data Collection
Pre-tests of the survey form, Mobbing Scale, and RAI were given to 218 nurses at Yakutiye Research Hospital of Ataturk University Medical Faculty and Erzurum Regional Training and Research Hospital between February 15 and April 30, 2010. Post-tests of the same instruments were administered 6 months after 30 nurses who had experienced mobbing based on their pretest scores completed assertiveness training (May to June 2010).
Eight sessions of assertiveness training were conducted between May and June 2010 by the researcher with the 30 nurses determined to have experienced mobbing and who agreed to participate in the program. The researcher, who ran the assertiveness training, had received a certificate from the Ministry of Health after completing a Management in Nursing and Leadership Instructor Training program. The sessions were offered in a seminary hall with seating for 20 individuals organized in the form of a “U” in accordance with adult training norms. The duration of each session was 2 to 2.5 hours. The 30 study participants were divided into two groups with 15 individuals in each group. However, after taking the nurses’ work schedules into account, the same session was offered to four groups each week, with at least 5 nurses and at most 15 nurses in each group.
The purpose of the assertiveness training is to teach individuals to express their own thoughts and feelings confidently but in a manner appropriate for the social environment; how to take criticism well; ways to cope with stress; positive self-communication; to understand the difference between withdrawn, assertive, and aggressive behaviors; and to protect their rights without any conflicts or disturbing others and by not allowing others to hurt themselves (Adana et al., 2010; Buzlu, 2006). Actual topics included:
Creating a positive training environment
Non-verbal communication
Non-verbal behaviors
Assertive compliments
The expression of positive and negative feelings
First-person communication
Self-knowledge
Receiving opinions and suggestions (Bozkurt, 2006)
Participants were expected to complete homework about the day’s content after each session. Audio-visual presentations, role-play, and interactive methods were used for training. The homework and feedback were evaluated at the beginning of each session. Six months after the training, post-tests of the Mobbing Scale and RAI were given to the 30 nurses who had participated in the assertiveness training program.
Statistical Analysis
The study data were analyzed using SPSS 17 (Statistical Package for Social Science). Percentages, means, Pearson correlations, and the paired t test were used to evaluate the data.
Ethics
The university institutional review board approved the study, and the hospitals provided written permission to conduct the research. After explaining the research objectives, the nurses were informed that they were free to attend the educational sessions or not. The 30 nurses who participated in the research were assured their personal information would not be disclosed to others.
Results
The average pre-assertiveness training mobbing score of nurses who had experienced mobbing was 226.4 ± 27.7, which decreased to 159.6 ± 47.9 after assertiveness training; the pre–post difference was statistically significant (p = .000; Table 1). It was observed during the training that the nurses who exhibited passive behavior made comments such as, “I preferred to remain silent,” “I experienced this because I cannot say no,” and “I remained silent as I thought that I could not get any results.” Looking at the results of the mobbing scale before training, the mean score of items related to social relationships, health, and living (e.g., I don’t trust anyone, I feel unhappy, I’m frustrated and furious, I feel I lose my courage, life is meaningless) was the highest; the mean score of these items were significantly lower after training.
T Test Comparison of Average Pre- and Post-Assertiveness Training Mobbing Scale Scores (n = 30)
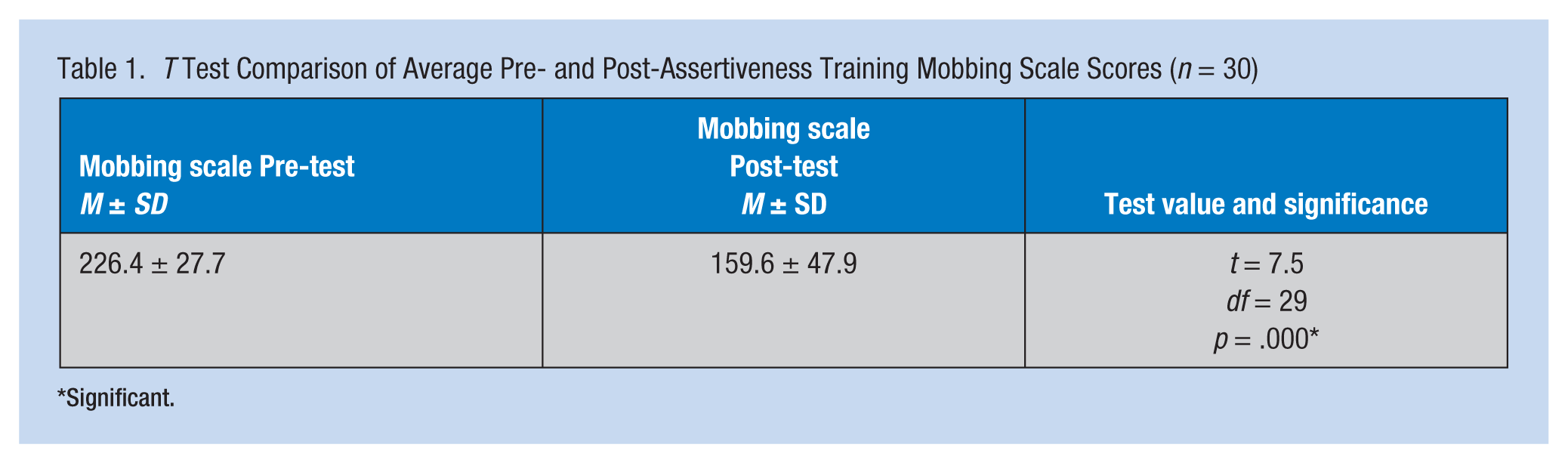
Significant.
The average pre-training assertiveness score was 6.23 ± 15.6, which increased to 17.0 ± 16.06 after assertiveness training; the pre-post difference was statistically significant (p = .001; Table 2). In addition, it was determined that 73.3% (22) of study participants exhibited a passive behavior pattern before training. After training, the participants were more aware of their passive behaviors, gained the courage to say “no,” and better expressed themselves.
T Test Comparison of the Average Pre- and Post-Assertiveness Training Rathus Assertiveness Scale Scores (n = 30)
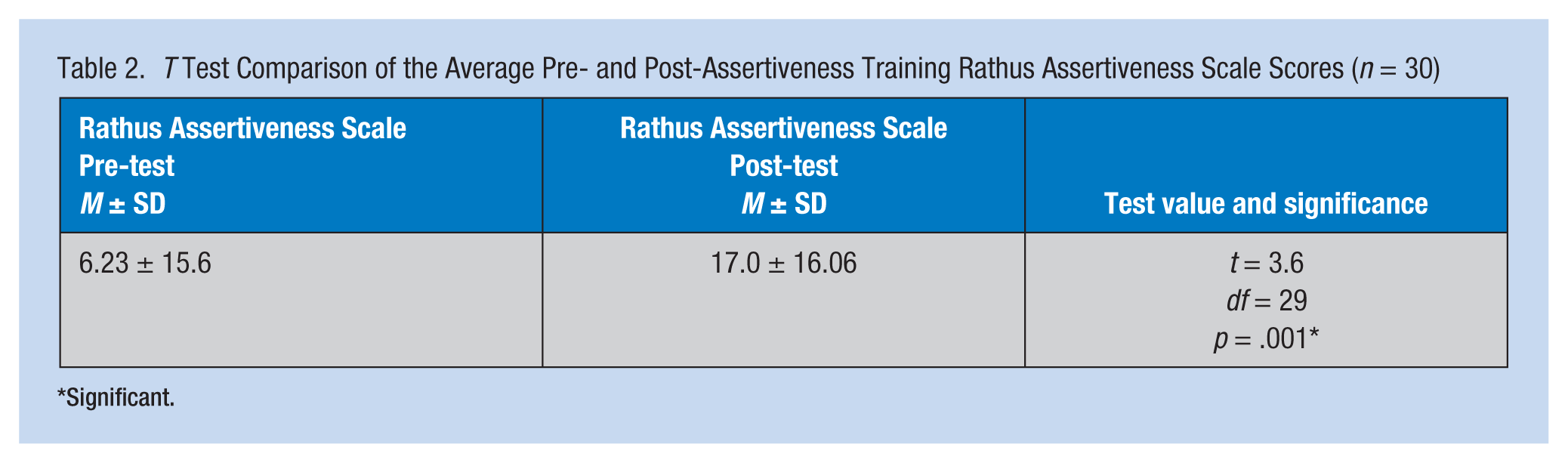
Significant.
The researchers found a negative significant correlation between the average scores of the Mobbing Scale and RAI (p < .01). As the level of assertiveness increased, the risk of mobbing decreased (Table 3).
Correlation Between Average Mobbing Scale and Rathus Assertiveness Inventory Scores
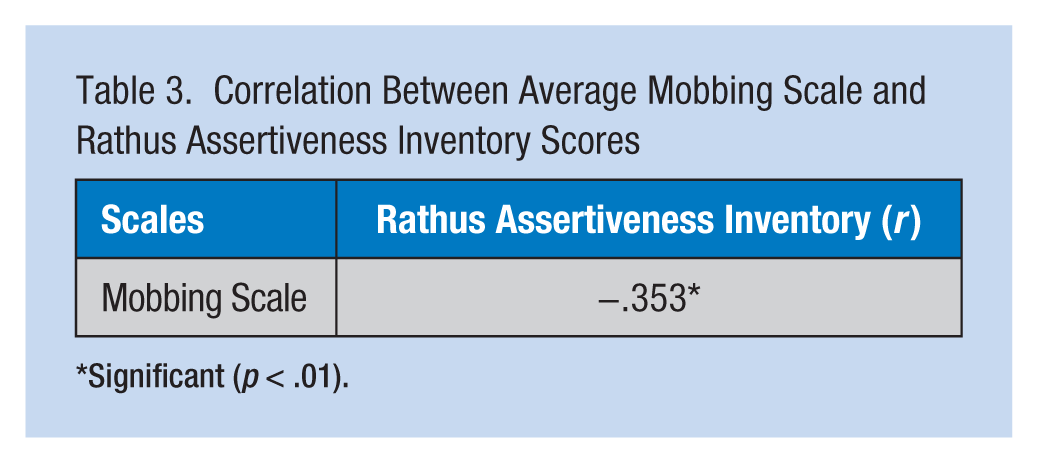
Significant (p < .01).
Discussion
The assertiveness training offered to nurses who had experienced mobbing was shown to be effective in reducing the incidence of future mobbing. Before training, the mean score of the items related to social relations, health, and living (i.e., I don’t trust anyone, I feel unhappy, I’m frustrated and furious, I feel I lose my courage, life is meaningless) were the highest; the mean scores of these items were significantly lower after training. Assertiveness training was effective in improving communication skills, and in realizing and expressing negative and positive feelings effectively, similar to other studies (Lin et al., 2004; Shimizu, Mizoue, Kubota, Mishima, & Nagata, 2003; Yamagishi et al., 2007).
In studies on psychological violence in the nursing profession, it was found that developing training and consultancy skills can help nurses cope with mobbing (Pai & Lee, 2011; Sofield & Salmond, 2003). In addition, the need for intervention in mobbing situations was supported in a study of psychological violence in eight European countries (Camerino et al., 2008).
Moreno-Jiménez et al. reported that social anxiety and assertiveness moderated the relationship between bullying and its effects on health (Moreno-Jiménez, Rodríguez-Muñoz, Moreno, & Garrosathe, 2007). At the same time, it was determined that victims of mobbing adopt passive behaviors and ineffective coping strategies (Zapf & Gross, 2001). Factors such as lack of self-defense, lack of autonomy, role conflicts, lack of effective coping, self-efficacy, and management skills were found to be significant for individuals affected by mobbing (Moreno-Jiménez et al., 2007). Based on these results, it has been suggested that assertiveness training has a positive effect by providing autonomy and control, and consequently, nurses who completed assertiveness training are less likely to experience mobbing. In this study, training was observed to have a positive effect by creating awareness that strengthened assertiveness skills; this finding was supported by other studies (Adana et al., 2010; Gundogdu, 2012; Lin et al., 2004; F. Ozturk, Efe, & Koparan, 2007; Shimizu et al., 2003; Timmins & McCabe, 2005; Yamagishi et al., 2007).
As a result of the research, it was determined that the majority of nurses who encounter mobbing act passively. Similar to findings in this study, it has been reported in other studies that nurses who are timid are more likely to experience mobbing in the workplace (Efe & Ayaz, 2010; Heather et al., 2010). In addition, this study demonstrated that mobbing increases as the level of assertiveness decreases. In Kukulu et al.’s study, the most significant factor influencing assertiveness was communication skills (Kukulu, Buldukoglu, Kulakac, & Koksal, 2006). Even though no published study has compared the experience of mobbing to individual assertiveness, studies on mobbing have shown that when individuals do not effectively employ communication skills (i.e., self-expression, assertiveness), mobbing may increase (Efe & Ayaz, 2010; Milutinović et al., 2009; Okanli et al., 2011; Simons & Mawn, 2010). In studies of assertiveness, self-expression and assertive behavior were found to be crucial elements of effective communication (Kukulu et al., 2006; Suzuki et al., 2009).
This study was conducted in Erzurum, one of the provinces in Turkey’s eastern region with a traditional lifestyle. The researchers found that the majority of nurses reported passive behavior perhaps because until recently only females were nurses in this region and women are expected to exhibit passive behaviors to meet societal expectations. Thus, mobbing is more likely among this population because their personal traits are dictated by cultural expectations (Moscicka & Drabek, 2010; Ofluoglu & Somunoglu, 2012). Consequently, preparation, support, and training are effective in preventing and intervening during mobbing (Moreno-Jiménez et al., 2007).
Study limitations included the following: The study was conducted in two hospitals in Erzurum and lacked a control group. Although a control group was planned at the beginning of the study, the control group could not be formed due to insufficient number of nurses who had been affected by mobbing, the confidential nature of mobbing experiences, and the unwillingness of eight nurses to participate in the study.
Conclusion
In this study, it was posited that nurse mobbing was prevalent, and the majority of nurses demonstrated passivity. Mobbing against nurses decreased after they developed assertiveness skills through training. The researchers suggest that nurses receive regular training to prevent and manage mobbing as well as support after a mobbing experience.
Applying Research to Practice
It was determined that the rate of mobbing is quite high among nurses, and they respond passively. As the level of assertiveness decreases, the rate of mobbing increases.
Following the assertiveness training given to nurses who were exposed to mobbing, the rate of mobbing decreased.
Assertiveness training is effective in coping with mobbing, and after training, nurses experience less mobbing.
Footnotes
Author Contributions
Study conception/design: Sibel Asi Karakas and Ayse Okanli; data collection/analysis: Sibel Asi Karakas and Ayse Okanli; drafting of manuscript: Sibel Asi Karakas and Ayse Okanli; critical revisions for important intellectual content; supervision: Ayse Okanli and Sibel Asi Karakas; statistical expertise: Ayse Okanli and Sibel Asi Karakas; administrative/technical/material support: Sibel Asi Karakas and Ayse Okanli.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sibel Asi Karakaş, PhD, RN, is presently working at the Atatürk University Faculty of Health Sciences Psychiatric Nursing in Turkey. She received her PhD in 2011.
Ayşe Okanli, associate professor, is presently working at the Atatürk University Faculty of Health Sciences Psychiatric Nursing in Turkey. She became associate professor in 2011.