
Abstract
Nurses continue to sustain musculoskeletal injuries even with increased emphasis on safe patient handling and mobility (SPHM) and organizational cultures of safety to protect health care workers. Analysis of data from 2011-2014 registered nurse graduates explored hospital safety culture, SPHM education/training, and incidence of new-nurse musculoskeletal injury. Results indicated hospitals provided some type of SPHM education and training, but 46% of study participants were not informed or aware of national SPHM standards or guidelines. Merely 13.9% of participants stated a written “no manual lifting policy” had been implemented; only 32.9% indicated staffing was adequate for SPHM tasks; and only 39.4% stated the hospital had all of the equipment needed to perform SPHM safely. Thirty-nine percent of participants had already sustained a musculoskeletal injury with an additional 35% sustaining but not reporting an injury. More actions are needed to ensure a decrease in musculoskeletal injuries for new nurses.
Keywords
The lifetime potential for musculoskeletal injury increases throughout a nurse’s career and may start as early as the first year of employment (Mitchell, O’Sullivan, Burnett, Straker, & Rudd, 2008; Videman, Ojajärvi, Riihimäki, & Troup, 2006). Most newly licensed nurses begin their careers with initial employment in a hospital.
Because nurses report spending approximately 20% of work time performing patient handling and mobility tasks, adequate preparation to perform these tasks safely is essential (Holman, Ellison, Maghsoodloo, & Thomas, 2010). Safe patient handling and mobility (SPHM) tasks include any physical activity, technique, or maneuver that requires nurses to assist with lifting, transferring, or moving patients (Gallagher, 2013). These tasks become more challenging as nurses age due to a variety of factors (e.g., increased patient acuity and obesity, decreased patient mental status and mobility, and lack of available equipment and staff to assist with these activities (Harrington, Daley, Maltz, Fritz, & Williamson, 2013; Wardell, 2007). In addition, nurses put patients’ safety first, which may prevent both patient and nurse injuries (Daley, 2013; Holman et al., 2010; The Joint Commission, 2012).
Currently, hospitals are focusing more on organizational and environmental aspects to create a culture of safety that includes safe performance of patient handling and mobility tasks. However, nurses, due to the physical demands of their work, are sustaining occupational injuries, particularly musculoskeletal injuries and disorders, at almost twice the national rate of the general population (Bureau of Labor Statistics, 2012). Back injuries were noted as the primary type of injury (Charney, 2009; Gropelli & Corle, 2011; O’Donnell et al., 2012). The American Nurses Association (ANA) 2011 Health and Safety Survey showed that 62% of nurses reported that suffering a disabling musculoskeletal injury was among their top concerns; 56% of nurses had experienced musculoskeletal pain caused or made worse by their work (J. Dawson, 2012).
Statistics for nurses experiencing musculoskeletal injuries or back pain ranged from a 12% prevalence prior to entering nursing, an annual prevalence of 40% to 50% for active nurses, and a lifetime prevalence of 35% to 80% (Branney & Newell, 2009). Other studies of musculoskeletal injury or back pain during the initial career years have found an incidence rate from 57% to 62% (Lövgren, Gustavsson, Melin, & Rudman, 2014; Videman et al., 2006). The actual number of injuries may be even higher than indicated, as many injuries are not reported (de Castro, Cabrera, Gee, Fujishiro, & Eularito, 2009; Menzel, 2008). Nurses who have experienced work injuries may choose to change positions or leave nursing, which results in turnover and replacement costs (Brewer, Kovner, Greene, Tukov-Shuser, & Djukic, 2012). It is estimated that 12% to 18% of nursing personnel leave nursing each year due to chronic back pain (Gallagher, 2013).
Nurses continue to sustain musculoskeletal injuries even with increased emphasis on “no lift” policies, injury prevention guidelines, education, training, and legislation for SPHM (Hunter, Branson, & Davenport, 2010). Some facilities have shown improvement with fewer injuries, but at other facilities, the number of injuries has not decreased to the extent desired (Occupational Safety and Health Administration [OSHA], 2014). Interdisciplinary collaboration between occupational health professionals, hospital nurse educators, and administrators is needed to ensure hospitals maintain an organizational safety culture and new nurses have the essential knowledge, skills, and competence to perform patient handling and mobility tasks safely.Nurses must report musculoskeletal injuries.Nurses should have the right to refuse to participate in unsafe SPHM situations.Hospitals must acquire appropriate safe patient handling equipment and provide adequate staffing to facilitate equipment use.Multiple learning approaches based on national safety standards and guidelines along with actual use of equipment should be incorporated into hospital SPHM orientation and training sessions. Training sessions should also focus on unit-specific client needs.Further information can be found in the ANA document, Safe Patient Handling and Mobility: Interprofessional National Standards Across the Care Continuum (American Nurses Association [ANA], 2013) at https://ana.orgDespite advances in SPHM equipment, such equipment may not be available or used, and policies for use may be inconsistent (Daley, 2013). Systematic SPHM programs should be implemented as the presence of equipment and written policies alone will not protect nurses (Gallagher, 2013).
New nurses’ education and training on SPHM begins during their initial nursing program and should continue throughout nurses’ careers. The Quality and Safety in Nursing Education (QSEN) Safety Competency objectives state nurses should be able to:
Describe factors that create a culture of safety (Quality and Safety Education for Nurses, 2014).
Possess knowledge of national patient safety resources and be able to incorporate these into care settings.
Communicate observations or concerns about patient handling and mobility needs and report injuries or near misses.
Demonstrate the effective use of SPHM equipment.
Perform tasks safely and use other strategies to reduce injury risks.
The ANA (2013) created eight SPHM standards to address the responsibilities of the employer or organization as well as those of health care workers related to lifting, transferring, repositioning, and moving patients. These standards were developed to enhance patient safety, promote patient and employee satisfaction, prevent injury to nurses, lower workers’ compensation costs, and promote the retention of nurses. Standard 1 and Standard 5 are specifically relevant to this study and correlate with select knowledge and skills objectives from the QSEN Safety Competency.
SPHM Standard 1 addresses the need for a hospital culture of safety to promote patient and health care worker safety (Gallagher, 2013). Employers should assist nurses by committing to provide a nonpunitive environment where employees can share concerns. Employers should also provide a system for right of refusal for unsafe situations, stipulate safe levels of staffing, and maintain a system for communication and collaboration.
SPHM Standard 5 recommends the establishment of a system for education, training, and maintenance of SPHM competence (Gallagher, 2013). Education, as defined within the SPHM standards, includes acquiring knowledge. Training is synonymous with skill acquisition and should include a performance component to measure competence. To educate and train nurses, employers must create multidisciplinary orientation and ongoing programs. Employers should ensure that nurses have adequate time to attend and participate in SPHM education and training sessions; appropriate SPHM equipment must be available for nurses to use with opportunities for hands-on learning and performance evaluations (OSHA, 2011).
The QSEN and SPHM competencies should be included in all initial nursing education programs and reinforced during new employee hospital and unit-specific orientations (Barnsteiner, 2011). Education and training should be further augmented with the acquisition of new equipment or implementation of new policies. Competence in performing SPHM tasks should be demonstrated and documented to decrease the incidence of musculoskeletal injuries (Gallagher, 2013; Garcia, 2014).
Method
A descriptive survey design was used to elicit information regarding hospital safety culture, SPHM education and training, and incidence of musculoskeletal injury among new nurses. The research instrument was emailed to 435 registered nurses (RNs) who had graduated between 2011 and 2014 from a community college Associate of Applied Science nursing program in southeast Michigan. Study inclusion criteria included employment as an RN in a hospital inpatient or outpatient setting from 2 months to 2 years, and provision of patient care including SPHM tasks. Not all nurse graduates are employed immediately after receiving their nursing licenses; thus, 4 years of graduates were surveyed to ensure that participants had attended hospital new employee orientation and had actual work experience as an RN.
The researcher formulated 45 items for the New Nurse Musculoskeletal Injury and Safety Survey based on the select knowledge and skills components of the QSEN Safety Competency, concepts from Standards 1 and 5 of the SPHM standards, and other relevant information extrapolated from the literature. The survey items elicited demographic data, responses to items related to hospital patient handling and mobility culture of safety, hospital SPHM education and training for nurses, and incidence of musculoskeletal injury among new nurses. Responses to survey items used three formats: 5-point Likert response scale (strongly agree to strongly disagree), Yes-No-Unsure, or numerical fill-in-the-blank responses. Participants could also provide optional comments.
The survey instrument was reviewed by nursing experts and faculty whose knowledge and expertise related to provision of nursing care provided an intuitive grasp of clinical situations related to SPHM techniques. The experts evaluated the instrument for readability, clarity, content, question formatting, sequence, ease of use, and time needed to complete the survey (Plichta & Kelvin, 2013).
A pilot study of the instrument was conducted with a small group of RNs with patient handling and mobility experience in a hospital setting. These findings, in addition to the comments from the nurse educators, were used to make further revisions to the survey prior to implementation with the study population. Efforts were made to control variables that could affect the integrity of the study such as varying levels of nursing education and years of nursing experience.
Cronbach’s alphas were calculated for survey internal consistency after data collection was complete with a goal of alphas to exceed .7 (Plichta & Kelvin, 2013). The Cronbach’s alpha for the survey section on SPHM education and training was .836; the hospital culture of safety section yielded a value of .828; and the incidence of nurse musculoskeletal injuries section had an alpha value of .435, which may have resulted from three “yes, no” response items in this section and fewer participants responding to these items. Optional qualitative data from the comment sections of the survey instrument were aggregated to provide further explanation of study findings.
The Oakland University and Schoolcraft College Institutional Review Board approved this study. The link for the SurveyMonkey®-based New Nurse Musculoskeletal Injury and Safety Survey was distributed to participants on March 20, 2015, with reminders at 1-week intervals until the survey was closed on April 20, 2015. Participants were provided with study information and informed consent procedures were applied. Responses were anonymous and confidentiality of data was maintained.
Data were analyzed using software from SurveyMonkey® and the Statistical Package for the Social Sciences (SPSS) Version 22. Sample characteristics were aggregated using descriptive statistics.
Results
One hundred four individuals (24.9%) responded to the survey, which is within the accepted 20% to 30% response rate for online surveys (Nulty, 2008). Seventy-two participants (69.3%) met the study inclusion criteria of working in a hospital and performing patient-handling tasks as part of their job duties; other participants were excluded. The percentage of study respondents meeting the criteria was similar to the 69% of nurses working in hospital inpatient or outpatient settings as reported in the Michigan Center for Nursing Survey of Nurses 2013 (Michigan Center for Nursing, 2014).
Demographics
The majority (65.4%) of study participants worked in hospital inpatient units and 3.9% worked in outpatient units providing patient care that included patient-handling tasks. Respondents excluded from the study worked at other nonhospital facilities. Most participants were female (86.1%); 76% were between 25 and 44 years of age. Most (76.4%) worked between 33 and 40 hours per week; 47.2% had worked between 0 to 12 months and 23.6% had worked between 13 and 24 months. The highest percentage of nurses (28.3%) worked on medical-surgical, oncology, or hospice units followed by “other” (14.1%) and critical care/emergency units (12.7% each). Participants who marked “other” provided examples such as cardiac care, dialysis, psychiatry, telemetry, and pulmonary units, which were already available for selection within the other categories. Most of the participants worked at hospitals with fewer than 100 beds (27.8%) followed by hospitals with 300 to 399 beds (22.2%) and more than 500 beds (20.8%).
Incidence of New Nurse Musculoskeletal Injury
Incidence of musculoskeletal injury was measured via 7 items with the following results. Seventy-nine percent of participants in this study stated that most nurses would experience a musculoskeletal injury as “part of the job” sometime in their careers. Approximately 39% of this group had already experienced a musculoskeletal injury while performing patient handling or mobility tasks, with over 70% of the injuries to the back.
The highest percentage of participants who stated they had sustained a musculoskeletal injury had 0 to 24 months of experience (54.2%). Approximately 29.2% of participants with 25 to 36 months of experience cited an injury; 16.7% of those injured had 37 to 48 months of experience. Seventy-two percent of study participants had not had an injury prior to becoming a nurse. Only 28% of participants thought they would sustain an injury in the near future.
Approximately 35% of participants stated they had sustained a musculoskeletal injury and had not reported it. Reasons cited for not reporting the injury included lack of realization that an injury had occurred at the time, unwillingness to seek health care or deal with workers’ compensation requirements, inability to be off work for economic reasons, and being unsure if the organization would do anything about the incident.
Statistical correlations were found between select demographic study variables and incidence of musculoskeletal injury. Most of the study participants (62.5%) who experienced injuries were between 25 to 34 years of age. The chi-square test showed a significant correlation between age and incidence of musculoskeletal injuries in nurses performing patient handling or mobility tasks, χ2 = 10.374, p < .05 (0.035). Analysis of variance (ANOVA) showed no significant difference between incidence of nurse musculoskeletal injuries while performing SPHM tasks and SPHM education and training variables (Table 1). A significant relationship was found between the incidence of nurse musculoskeletal injuries and select hospital culture of safety environment variables (p < .05; Table 2):
A nonpunitive environment that allows nurses to raise questions and share concerns was related to SPHM tasks (p = .002)
The presence of a hospital interdisciplinary team or task force that communicates and collaborates on activities to promote a culture of safety (p = .017)
Provision of a hospital environment where nurses have the right to refuse to participate in unsafe patient handling and mobility situations (p = .034)
Adequate staffing (p = .036)
Association Between Safe Patient Handling and Mobility Education and Training Variables and Incidence of Nurse Musculoskeletal Injury
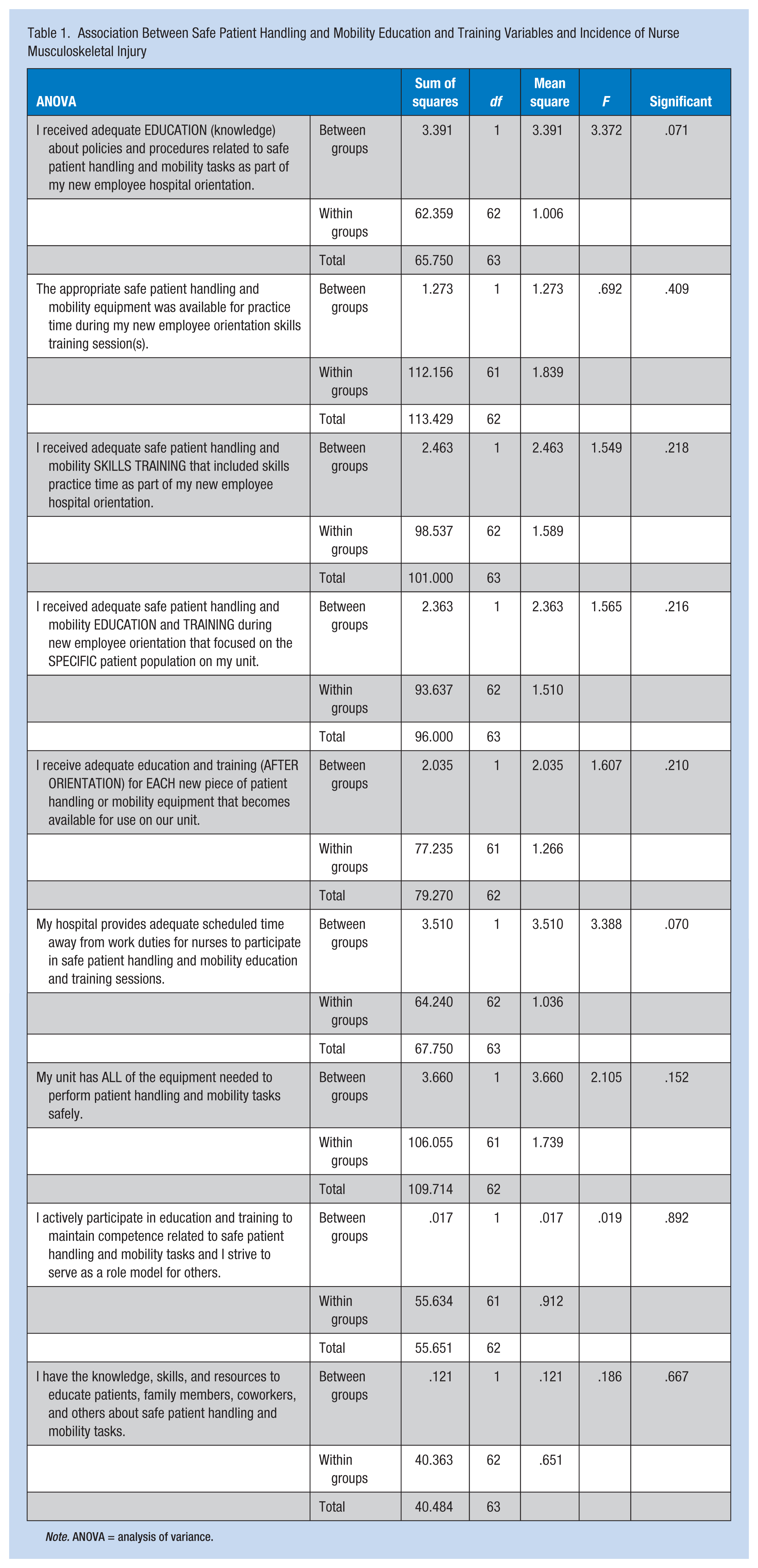
Note. ANOVA = analysis of variance.
Significant Difference Between Hospital Culture of Safety Variables and Incidence of Nurse Musculoskeletal Injuries
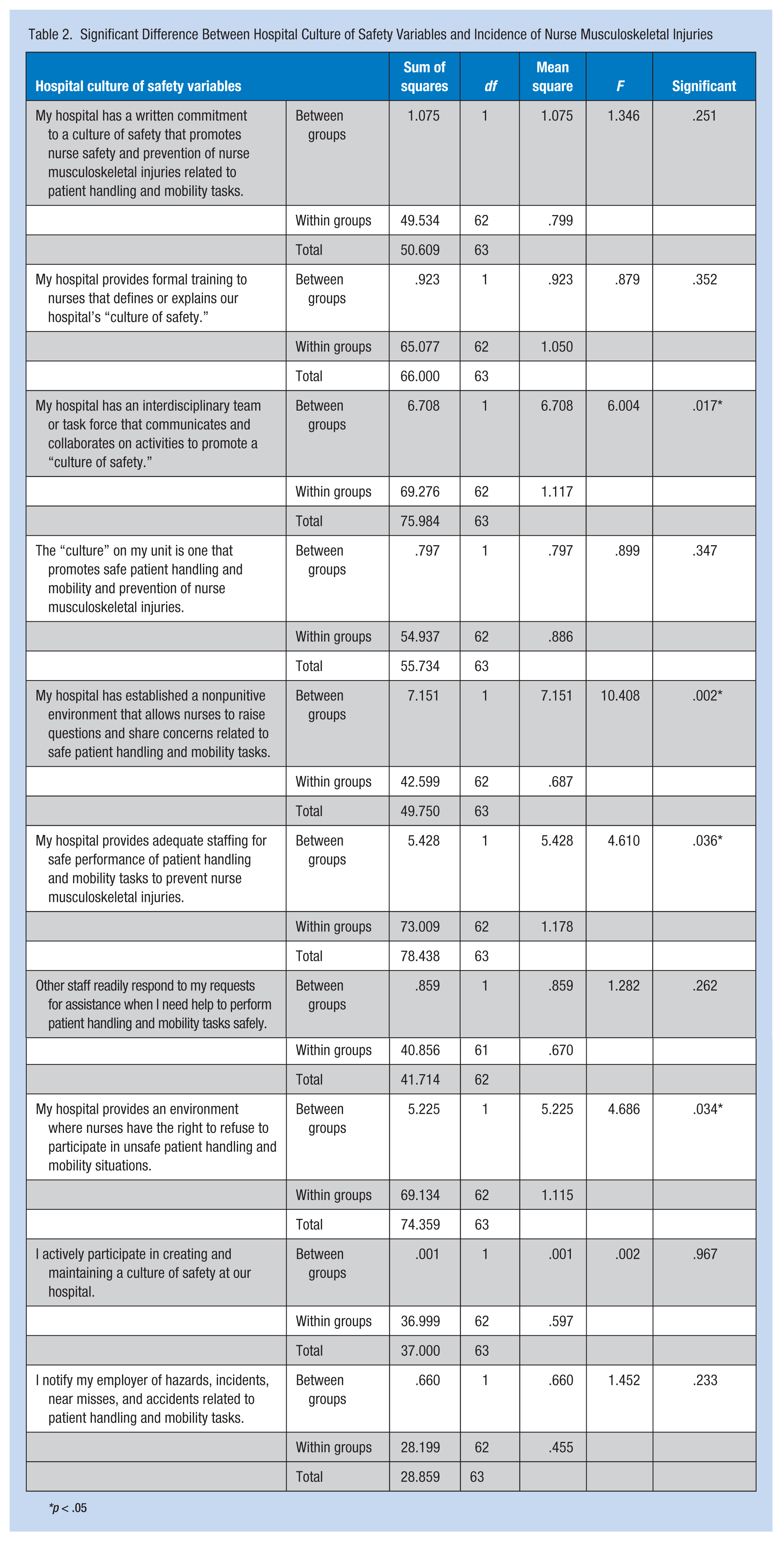
*p < .05
Participant responses relevant to incidence of musculoskeletal injury for nurses included the acknowledgment that injuries may happen on the job and that some nurses will not take time to use available equipment. Responses to the question “What makes it difficult for you to perform patient handling and mobility tasks safely?” included comments focused on inadequate staffing, lack of resources, unavailable equipment, lack of education and continuing education, overweight or cognitively impaired patients, and nurses committed to patient safety above their own well-being.
SPHM Education and Training
The survey included 18 items focused on aspects of SPHM equipment, education, and training. Percentages provided for those who “agreed” included both strongly agreed or agreed for the items. Approximately 74% of participants agreed that adequate information regarding SPHM policies and procedures was included in their hospital orientations, but fewer than half (47.1%) indicated skills training was also provided as part of these sessions. Only 38.2% responded that training focused on specific specialty unit needs. Forty-eight percent of respondents stated that appropriate SPHM equipment was not available for skills practice during orientation, and 60.6% stated they did not have all the equipment needed to perform SPHM tasks safely on a daily basis. Most participants (53%), however, did report adequate education and training were provided when new equipment was introduced to the unit. Figure 1 shows the types of SPHM equipment available to participants.
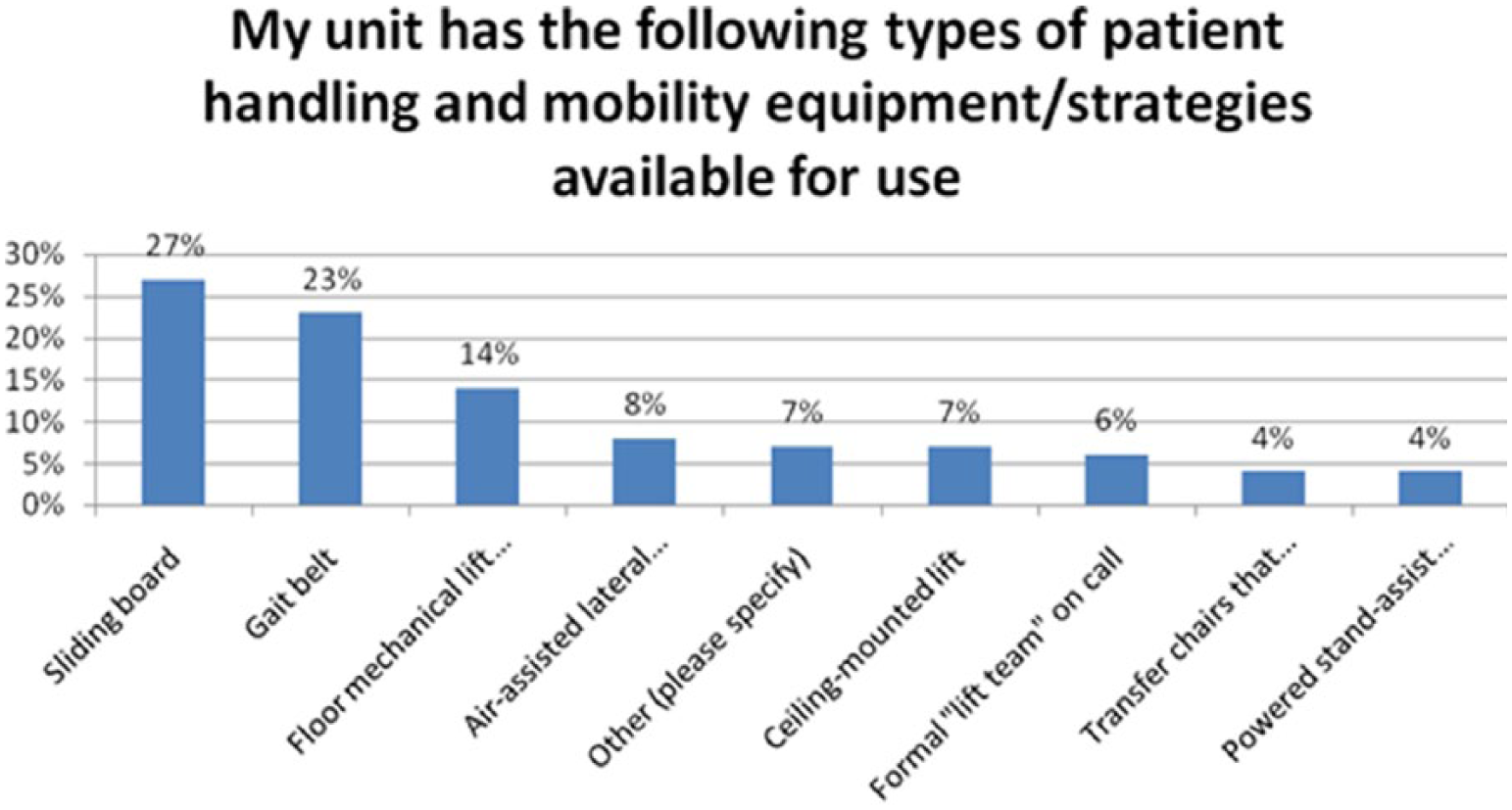
Hospital safe patient handling and mobility equipment available for use.
Fifty-three percent of participants stated they actively participated in education and training to maintain competence and serve as role models for others. Only 25.3% stated that adequate scheduled time away from work duties was provided to participate in SPHM education and training sessions. Overall, 67% of participants reported having the requisite knowledge, skills, and resources to educate patients, family members, coworkers, and others about SPHM tasks.
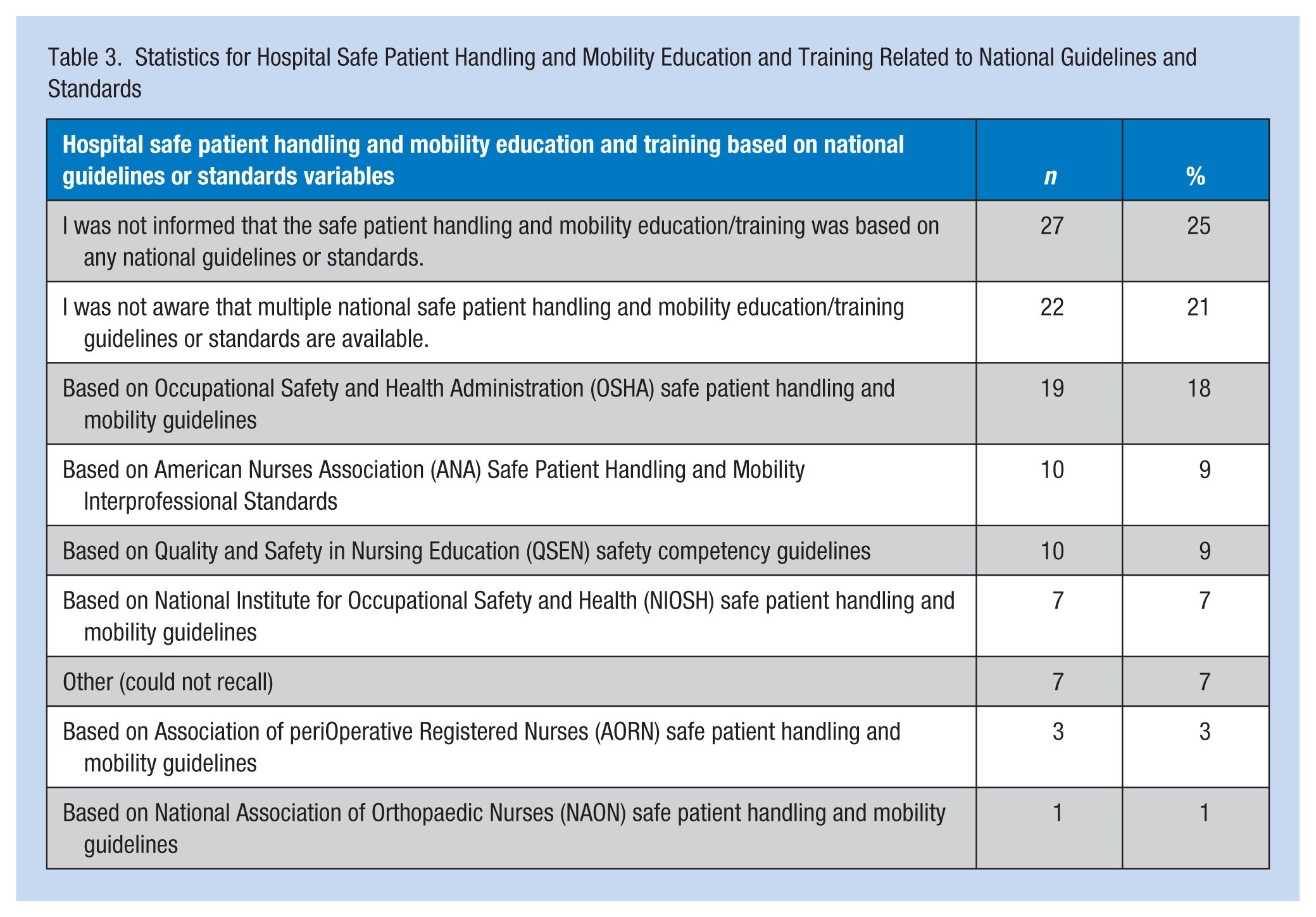
Respondents reported that safe patient handling education during orientation included multiple individual or combined educational strategies: lecture/presentation (73.4%), computer module (63.8%), and/or handouts (50.7%). More than one option could be selected for this survey item. Participants were also asked which national guidelines or standards served as the evidence-based foundation for their hospitals’ SPHM education and training; 46% of nurses reported having no knowledge of guidelines or standards, with no information provided during orientation sessions. Table 3 reports findings for specific guidelines and standards.
Statistics for Hospital Safe Patient Handling and Mobility Education and Training Related to National Guidelines and Standards
Participants were also asked the maximum weight in pounds that could be lifted without the use of an assistive device. The majority (81.4%) of respondents did not know the correct answer per National Institute for Occupational Safety and Health (NIOSH) guidelines, which lowered the limit from 50 pounds to 35 pounds in 1994 (Waters, 2007). A fifty pound limit was cited by 11.4% of participants; 6% selected 20 pounds to 25 pounds, and 1% selected 70 pounds.
Methods for SPHM skills training during new employee orientation included those listed in Figure 2. Most of the skills training (40.3%) used demonstration with SPHM equipment followed by return demonstration (28.2%). Interactive scenarios in a patient room accounted for 19.2% of training; 16.1% used a simulation laboratory. Approximately 18% stated “other” for this item with half stating they received no skills training, 22% received only video information pertaining to the skills, one participant had a physical therapist discuss safe bending and lifting, and others did not recall events. The majority (62%) stated the duration of time spent practicing skills ranged from no time to 30 minutes, 21% stated skill practice time lasted from 31 to 60 minutes, and 18% reported 61 to 270 minutes of practice.
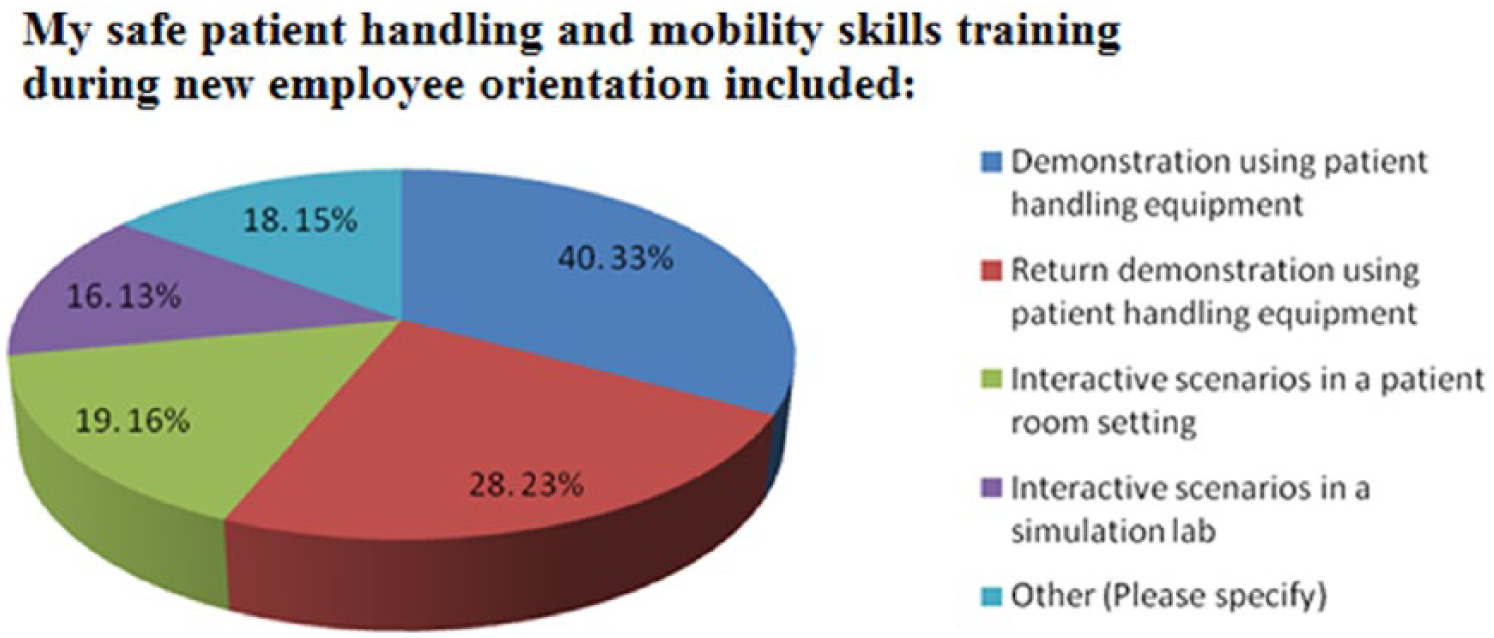
Safe patient handling and mobility skills training methodologies.
Participants reported SPHM competence was documented as part of their new employee orientation process 55.2% of the time, 28.4% stated it was not documented, and 16.4% were unsure if documentation occurred. Annual SPHM competency training was required and documented 43.9% of the time but not required or documented 25.8% of the time; 30.3% of participants were unsure if such training occurred on an annual basis.
Comments related to SPHM education and training included the following responses:
“All new hires have to practice with the Hoyer lift.” “We had to demonstrate proper use of the equipment.” “There was no training session.” “We had a 20-minute workshop with 60 people attending.” “I have not seen some of the equipment on the unit since orientation.” “Physical therapy may get patients out of bed but nurses are responsible for placing them back in bed without the proper equipment.” “We have a lift team that has almost all of the equipment needed.” “Equipment is often shared between units.” “We have no assistive devices available; all lifting/turning/transferring is done manually.” “We need more equipment.”
Hospital Culture of Safety
Eight survey items pertained to culture of safety within participants’ hospitals, and two items focused on respondents’ involvement with safety culture. Responses to each item, along with means on a 1 to 5 scale (5 = strongly agree, 1 = strongly disagree) and standard deviations, are provided in Table 4; mean scores were calculated for this section as many participants (5%-35%) chose to select “neutral” for these items. Scores ranged from a low of 2.83 to a high of 4.22; the lowest score (2.83) indicated that nurses were unsure if they had the right to refuse to participate in unsafe patient handling and mobility situations. The next lowest score (2.87) indicated inadequate staffing for SPHM tasks to the extent deemed appropriate by nurses to prevent potential injuries, although other staff “readily respond to requests for assistance” (4.22). Comments pertaining to this section included the following:
“We watch videos on safe handling once a year, but we are expected to lift and move patients daily without lifts.” “While the hospital does push for safety, they have done nothing to promote it.” “As a new employee to this hospital, nothing was done or implied during orientation to promote safety.” “Culture of safety is briefly covered in orientation and a small packet about back safety is given, but more time should have been spent on the subject.” “Lifts and slide sheets are available but rarely used.” “Getting help to lift depends on how busy people are and if we are short-staffed.” “A lot of unsafe lifting goes on every day on my floor.”
Hospital Culture of Safety Statement Analysis
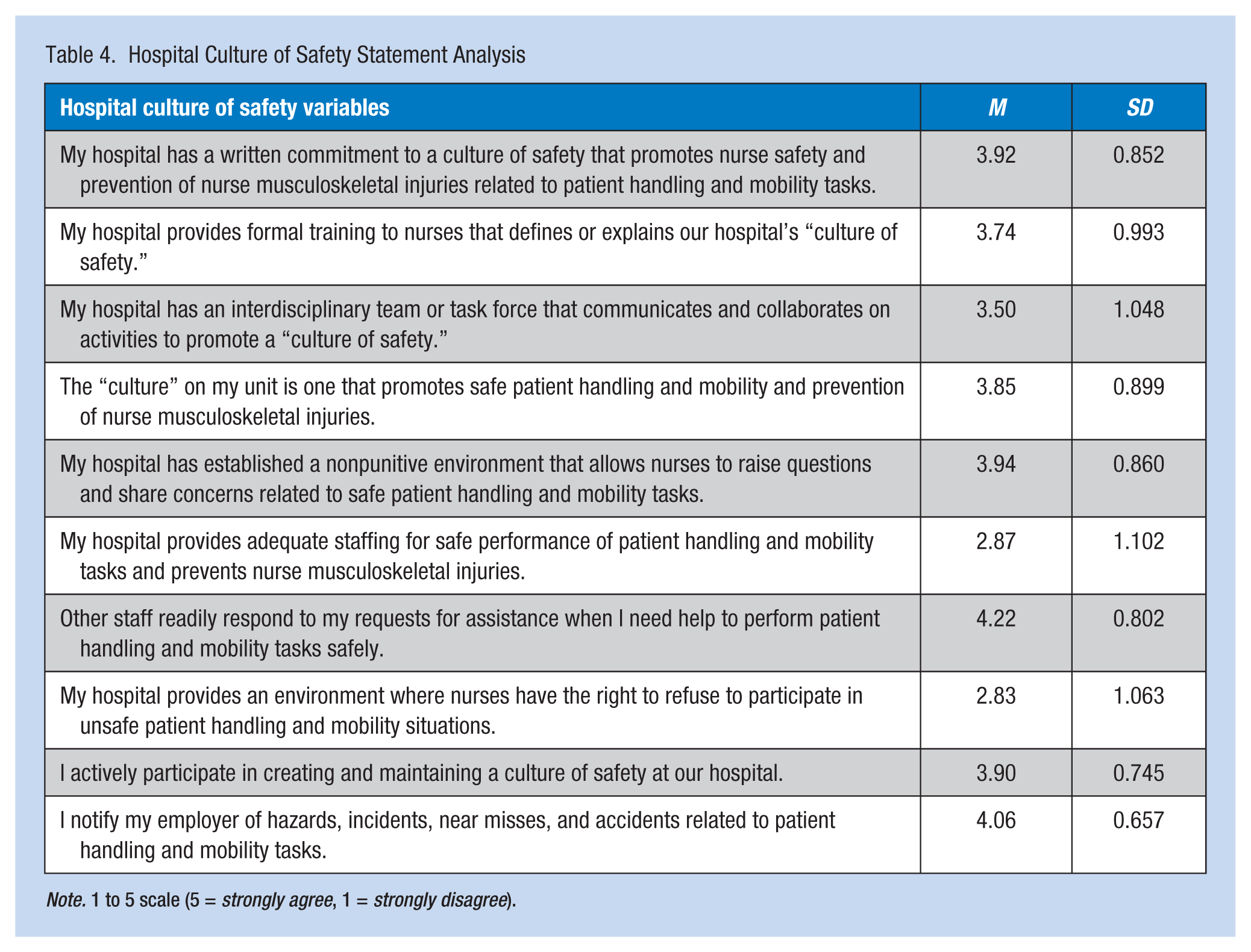
Note. 1 to 5 scale (5 = strongly agree, 1 = strongly disagree).
Discussion
This study explored the incidence of nurse musculoskeletal injuries and correlations to SPHM education and training provided to new nurses within a hospital culture of safety. Study data indicated new RNs continue to be at risk for injuries while performing SPHM tasks, with 39% of those surveyed having already experienced a musculoskeletal injury within the first 2 years of employment. This statistic is within the “lifetime prevalence” of musculoskeletal injury of 35% to 80% cited by Branney and Newell (2009). With today’s emphasis on safety and the increase in available SPHM equipment, the prevalence of injury should decrease in the future.
More than half of the study respondents who had sustained a musculoskeletal injury (54.2%) had 0 to 24 months of experience. Approximately 29.2% of participants with 25 to 36 months of experience cited an injury, and 16.7% of those injured had 37 to 48 months of experience. These findings are similar to the 57% of nurses injured within 2 years of RN employment as reported by Videman et al. (2006). Another study also associated higher risk for injury with those who had worked less than 2 years (Boyer et al., 2009).
The only demographic variable found to statistically correlate with incidence of nurse musculoskeletal injury was age 25 to 34 years. This finding is similar to results by Karahan, Kav, Abbasoglu, and Dogan (2009), who noted that workers between 17 and 34 years of age experienced a higher incidence of injury. The correlation in that study was attributed to nurse inexperience and workers in this age group working in direct care positions.
Seventy-two percent of study participants had not had an injury prior to becoming a nurse. Only 28% indicated they would sustain an injury “in the near future,” but 79% stated most nurses would experience an injury as part of the job. Thirty-five percent of nurses indicated they had sustained an injury that they did not report. These findings correlate with previous research; Kay, Evans, and Glass (2015) and Menzel (2008) found that many nurses do not report injuries, are frequently reluctant to voice opinions about patient handling concerns, or feel management does not ask nurses for input. Nurses have the responsibility to communicate and collaborate with employers by participating in activities and notifying employers of workplace hazards and incidents. A culture of safety should include procedures for staff to report safety concerns in a blame-free environment (Garcia, 2014).
The majority of participants agreed adequate SPHM policy and procedure information was provided during new employee orientation and with the introduction of new equipment. Participants also reported they had the knowledge, skills, and resources to educate patients, family members, coworkers, and others about SPHM tasks. However, approximately 38.2% stated they needed more training focused on specific unit needs and more SPHM equipment should be available during training session practice. As 46% of those surveyed stated they did not have any knowledge of SPHM national standards or guidelines and 81.4% did not know that lifting over 35 pounds requires assistive devices, further evaluation and revisions to include QSEN and SPHM components in SPHM education and training programs are indicated.
Most participants stated that lectures, handouts, and demonstrations, including return demonstrations, were provided and required as part of SPHM education and training. However, only 47.1% stated that they had any actual training with SPHM equipment, and fewer than 30% had interactive scenarios in a patient room or simulation laboratory incorporated into sessions. Of those participants whose training included the use of equipment, 61.8% stated that training time ranged from no time to 30 minutes; fewer than half stated that SPHM equipment was even available during education and training sessions. As multifaceted sessions improve outcomes, more equipment should be available and additional time provided for interactive skills practice (Gallagher, 2013). With only 25.3% of participants stating that adequate time away from work duties for SPHM education was provided, flexible work schedules are essential to meet adequate education and training requirements.
Culture of safety environment factors that were significantly related to incidence of nurse injury included the presence of a nonpunitive environment, a hospital interdisciplinary team, the ability to refuse to participate in unsafe SPHM situations, and adequate staffing. The majority of participants indicated most components of a safety culture were present at their hospital; however, only 13.9% stated a written “no manual lifting policy” had been implemented. Participants stated they actively participated in creating and maintaining the safety culture and reported issues to management; however, it is unclear how this commitment to a culture of safety translates into actual processes when injuries continue to occur at such high rates.
Study participants stated they could raise questions and share concerns related to SPHM tasks, but only 27% felt they had the right to refuse to participate in unsafe patient handling and mobility situations. Adequate staffing was a concern for most participants; only 32.9% agreed the hospital had enough staff available for safe performance of SPHM tasks. Most respondents (82.5%) stated that staff who were available were willing to assist others. Only 39.4% of participants stated the hospital had all the equipment needed to perform SPHM safely. A strong culture of safety is imperative to improve organizational outcomes and promote employee satisfaction (Powers & Perez, 2013).
Limitations
Study data were derived from a convenience sample of RNs who had graduated from an associate degree nursing program and may not represent all RNs. The study relied on participants’ memories of events, which may have limited accuracy of the data collected. Results of the study may be generalized only to new nurses. The survey instrument was designed by the researcher and needs further validation by other researchers to document reliability. Narrowing the number of survey items could potentially increase the number of item responses. Replicating the study with a larger population from a larger, more varied geographic area is recommended. Further research should be conducted on additional QSEN and SPHM components with correlation to the incidence of musculoskeletal injuries among RNs.
Implications for Practice
Results of this study indicate that nurses are continuing to sustain musculoskeletal injuries while performing SPHM tasks, even when equipment is available. With only 39.4% of nurse participants stating their institution had adequate SPHM equipment, more hospitals must acquire appropriate equipment to prevent injuries. Musculoskeletal injuries result in personal, emotional, and financial burdens to injured nurses, costing health care organizations billions of dollars a year (Kuehn, 2013). The Michigan Center for Nursing Survey of Nurses 2013 (Michigan Center for Nursing, 2014) indicated 20.1% of nurses left their job in 2012 due to physical demands of the job, an increase from 16.3% in 2011. Employers, who must replace nurses who leave, estimate that replacement costs range from $27,000 to $103,000 per nurse (Li & Jones, 2012).
Occupational health professionals should collaborate with hospital nurse educators and administrators to ensure that new nurses have the essential knowledge, skills, and competence to perform patient handling and mobility tasks safely. Inexperience and an overall lack of education and training on SPHM tasks have been linked to higher nurse injury rates (A. Dawson et al., 2007; Zontek, Isernhagen, & Ogle, 2009). Orientation sessions should be based on national safety standards and guidelines (Gallagher, 2013). Education and training sessions should include multifaceted approaches to learning with actual use of SPHM equipment and more focus on specialty unit needs. Consistent measures for documenting competence are indicated along with scheduled time for education and training. An effective system for educating, training, and maintaining competence could provide measurable practice expectations and prevent future injuries.
Hospitals must further integrate and implement culture of safety components. Nonpunitive environments with the right to refuse to participate in unsafe SPHM situations are essential (Gallagher, 2013). Interdisciplinary SPHM teams are needed along with adequate staffing to prevent nurses’ musculoskeletal injuries.
Conclusion
Results of this study indicate new nurses are at high risk for musculoskeletal injuries. Improving SPHM education and training plus enhancing the hospital culture of safety will enable nurses to preserve their own health and continue to provide safe, quality care for others. A decrease in musculoskeletal injuries among new nurses will also benefit hospitals by promoting job satisfaction, increasing nurse retention, and decreasing lost workdays and associated organizational costs. Future research with larger sample to further clarify findings should be conducted.
Applying Research to Practice
Interdisciplinary collaboration between occupational health professionals, hospital nurse educators, and administrators is needed to ensure hospitals maintain an organizational safety culture and new nurses have the essential knowledge, skills, and competence to perform patient handling and mobility tasks safely.
Nurses must report musculoskeletal injuries.
Nurses should have the right to refuse to participate in unsafe SPHM situations.
Hospitals must acquire appropriate safe patient handling equipment and provide adequate staffing to facilitate equipment use.
Multiple learning approaches based on national safety standards and guidelines along with actual use of equipment should be incorporated into hospital SPHM orientation and training sessions. Training sessions should also focus on unit-specific client needs.
Further information can be found in the ANA document, Safe Patient Handling and Mobility: Interprofessional National Standards Across the Care Continuum (American Nurses Association [ANA], 2013) at https://ana.org
Footnotes
Acknowledgements
The authors thank the nurses who participated in the study plus staff and management for their assistance and support.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.