
Abstract
This study assessed commercial welders’ awareness and utilization of personal protective eye devices (PPEDs), and their associations, in Enugu, Nigeria, between January and March, 2011. The participants included 343 males, age 33.9 years ± 10.0 SD years. The participants reported high awareness of welding-associated ocular hazards (99.4%) and PPEDs (75.2%-98.3%), but low PPED possession and utilization rates. Cost and “presumed lack of utility” were the leading barriers to PPED possession; non-utilization was mainly attributed to “user inconvenience” and “presumed lack of protective benefit.” PPED utilization was significantly associated with lower educational status (p = .030) and electric welding (p < .0001). The underlying causes are amenable to preventive occupational eye health education, enhanced ergonomics and affordability of PPEDs, and legislative enforcement of their use.
Welding-exposure-related ocular health hazards remain a critical occupational health and safety issue for welders (Omolase & Mahmoud, 2007; Sabitu, Iliyasu, & Dauda, 2009; M. A. Shaikh & Shaikh, 2005) and other welding workers (T. Q. Shaikh & Bhojani, 1991) in the world’s low- and middle-income countries (Omolase & Mahmoud, 2007; Sabitu et al., 2004; T. Q. Shaikh & Bhojani, 1991; M. A. Shaikh & Shaikh, 2005), and the developed economies (Bull, Hovding, Riise, & Moen, 2004; Lombardi et al., 2005; Mancini et al., 2005; Walls & Dryson, 2002). Consistent with its position as the second leading cause of consumer-product-related ocular trauma (Sastry et al., 1995), various reports in Pakistan (M. A. Shaikh & Shaikh, 2005), the United States (Lombardi et al., 2005), and Italy (Mancini et al., 2005) have identified eye injury in welders as the leading cause of occupational injury compensation claims with 5% to 33% of all compensable occupational eye injuries traceable to welding-related activities. Welding-related ocular and periocular injury or morbidity could result from entry of flying or sharp objects into the eye (Lombardi et al., 2005; Mancini et al., 2005), thermal burns (Lombardi et al., 2005; Mancini et al., 2005) from hot chemical liquids or gases, or exposure to hazardous light or radiations (e.g., arc light and solar, ultraviolet, and infrared radiation; Ajayi, Adeoye, Bekibele, Onakpoya, & Omotoye, 2011). Although workers directly engaged in welding activities are frequently involved, injuries to bystanders, observers, and assistants are common (Lombardi et al., 2005). Apart from the socio-economic and psychological costs of injury (Mancini et al., 2005), work-related eye injuries constitute a significant strain on the public health care system and the nation’s health budget (Lombardi et al., 2005).
Despite technological advances in welder’s personal protective eye devices (PPEDs), machine-incorporated eye protective systems, and established preventive efficacy of PPEDs (Bull, 2007; Forst et al., 2006; Torp, Grogaard, Moen, & Bratveit, 2005; Verma et al., 2011), barriers to their optimal utilization remain largely unaddressed worldwide (Lipscomb, 2000; Okoye & Umeh, 2002; Omolase & Mahmoud, 2007). This lack of PPED utilization has led to a high incidence of otherwise preventable welders’ occupational eye injuries (Lipscomb, 2000; Okoye & Umeh, 2002; Omolase & Mahmoud, 2007) and morbidity (Wang, Yang, Wang, & Shunqing, 2006). Similar surveys have reported awareness of welding-related ocular hazards from 50% to 100% of welders (Isah & Okojie, 2006; Oduntan, 1998; Omolase & Mahmoud, 2007; Sabitu, Iliyasu, & Dauda, 2009). PPED possession by 26.6% to 63.3% of welders (Sabitu et al., 2009) and PPED utilization by 30% to 47% of welders has been documented (Isah & Okojie, 2006; Omolase & Mahmoud, 2007). Especially in developing countries, awareness of ocular hazards, availability, cost and comfort of PPED, and lack of legislative enforcement of safety standards have been variously implicated as barriers to optimal utilization of PPEDs among welders (Ajayi et al., 2011), farm workers (Forst et al., 2006; Verma et al., 2011), other construction workers (Lombardi, Verma, Brennan, & Perry, 2009; M. A. Shaikh, 2001; Yu, Liu, & Hui, 2004), service workers (Lombardi et al., 2009; Ramos, 1999; Torp et al., 2005; Yu et al., 2004), and the general public (Forrest, Cali, & Cavill, 2008). Furthermore, welders’ socio-demographic and job characteristics have been shown to influence their hazard awareness and utilization of PPEDs (Sabitu et al., 2009). Although the majority of previous Nigerian reports were on commercial and freelance welders, the only related report in the study area of southeastern Nigeria focused on industrial (formal sector) welders (Ajayi et al., 2011; Davies, Asanga, Nku, & Osim, 2007; Oduntan, 1998; Omolase & Mahmoud, 2007; Sabitu et al., 2009).
Consequently, baseline comparative data on commercial and freelance welders in southeastern Nigeria was not found despite these welders constituting a significant proportion of the welder workforce. In addition, commercial and freelance welders are potentially vulnerable to welding-related eye injuries because, unlike industrial welders, they are not covered by the government’s legislative enforcement of safety standards in welding practice. Consequently, the investigators embarked on a population-based cross-sectional survey of commercial and freelance welders in Enugu, located in southeastern Nigeria.
The study was designed to assess welders’ awareness, possession, and utilization of PPEDs and explore any association between these variables and welders’ socio-demographic profile, job characteristics, and awareness of welding-associated ocular health hazards. In addition to providing comparative loco-regional data, the findings were expected to provide the basis for changes in the government’s occupational eye health safety interventions and produce a major health policy shift.
Method
Enugu is the former regional capital of Nigeria’s eastern region and the current administrative capital of Enugu state. Enugu state is one of five states of Nigeria’s southeast geopolitical zone. Enugu state has 17 administrative sub-units or Local Government Areas (LGAs); of these, Enugu-North, Enugu-East, and Enugu-South LGAs form Enugu urban.
In Enugu urban, an appreciable number of commercial and freelance welders ply their welding trade in open space road-side welding workshops scattered all over the town. Also, in Enugu urban, numerous untrained welding workers with no welding experience, like pipe fitters and panel beaters, abound.
Study Design and Sample
The study was a population-based cross-sectional survey of commercial and freelance welders in Enugu urban, southeastern Nigeria, conducted between January and March 2011. The sample size of 343 welders was based on a 77.9% awareness level reported in a previous survey (Sabitu et al., 2009). The membership register (Trade list) of the professional association of commercial and freelance welders in Enugu, the study area, served as the sampling frame. To ensure representativeness of the sample, k (sampling interval, skip) was calculated as k = N/n, where N = the population size and n = sample size. After a random start, every third name in the register was selected until the calculated sample size was obtained.
Questionnaire and Questionnaire Development
The study instrument, partly developed by the researchers and partly adapted from a previous survey (Sabitu et al., 2009), was a 17-item researcher-administered questionnaire. The open- and closed-ended survey questions focused on participants’ socio-demographic characteristics, job training, practice profile, and awareness of welding-related ocular health hazards and possession and utilization of PPEDs. The closed-ended questions sought dichotomous (yes/no) responses. In cases of ambiguity, the respondent was shown a picture of the PPED in question.
The questionnaire was developed in English; however, the contents were translated orally into the local Igbo language during data collection from survey participants. Prior to data collection, to ascertain its construct validity and psychometric reliability, the questionnaire was pretested on commercial and freelance welders practicing their service trade in a similar work environment, but outside the study area. The pre-test provided useful feedback that guided modifications in the content and design of the questionnaire to ensure its validity and reliability in assessing respondents’ awareness of welding-associated ocular health hazards, and awareness, possession, and utilization of welders’ PPEDs.
Survey Administration
Participants’ data were obtained through face-to-face interviews by the researchers. To eliminate the possibility of being interviewed more than once, recruited participants were specifically instructed to decline duplicate offers for repeat participation in the study.
The interviews were conducted in the privacy of each respondent’s workshop, and the responses were directly entered into the survey questionnaire.
Data analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) statistical software, Version 18 (SPSS Inc, Chicago, Illinois, USA) to generate rates, frequencies, and percentage distributions. Statistical tests for significance of observed inter-group differences included chi-square test and student-t test or Fisher’s exact test as appropriate. Prior to data analysis, data entry accuracy was ascertained by re-entering data on 30 randomly selected questionnaires.
Results
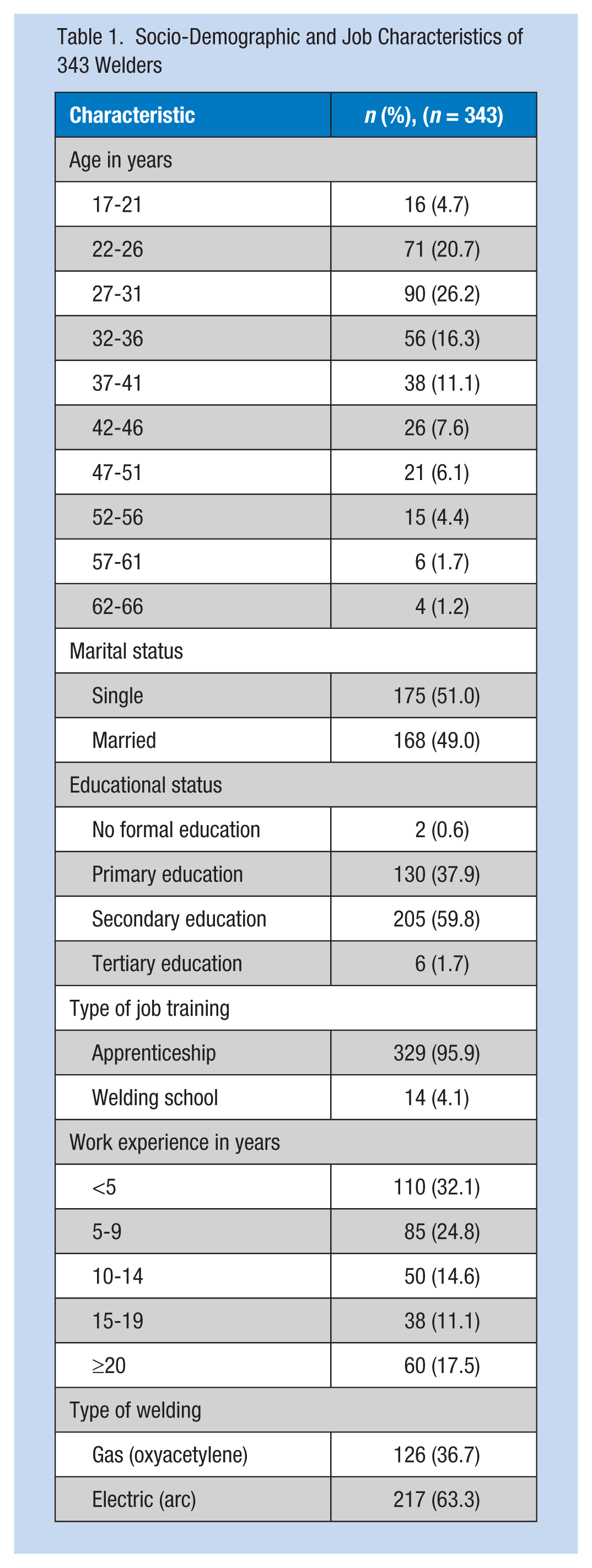
The result of the pre-test showed that the survey instrument had good validity and reliability, with Lawshe’s content validity index of 0.99 and Cronbach’s alpha coefficient of 0.8. All 343 study participants in the final survey were male with a mean age of 33.9 ± 9.7 SD years (range = 17-66 years) and modal age group of 27 to 31 years. The participants were predominantly of Ibo ethnic extraction; the majority (341, 99.4%) had completed primary education. The majority (329, 95.9%) of participants had completed apprenticeship welding training, had less than 10 years of work experience (195, 56.8%), and were more frequently electric (arc; 217, 63.3%) than gas (oxyacetylene; 126, 36.7%) welders. Table 1 displays the participants’ socio-demographic and job characteristics. An overwhelming majority of participants (341, 99.4%) reported an awareness of ocular health hazards associated with welding exposure. Of the three PPEDs whose awareness, possession, and utilization profiles were assessed in this survey, eye goggles had the highest score and helmets had the least score across the three assessment parameters (Table 2).
Socio-Demographic and Job Characteristics of 343 Welders
Awareness, Possession, and Utilization (Regular Use) of Personal Protective Eye Devices, and Factors Associated With Utilization
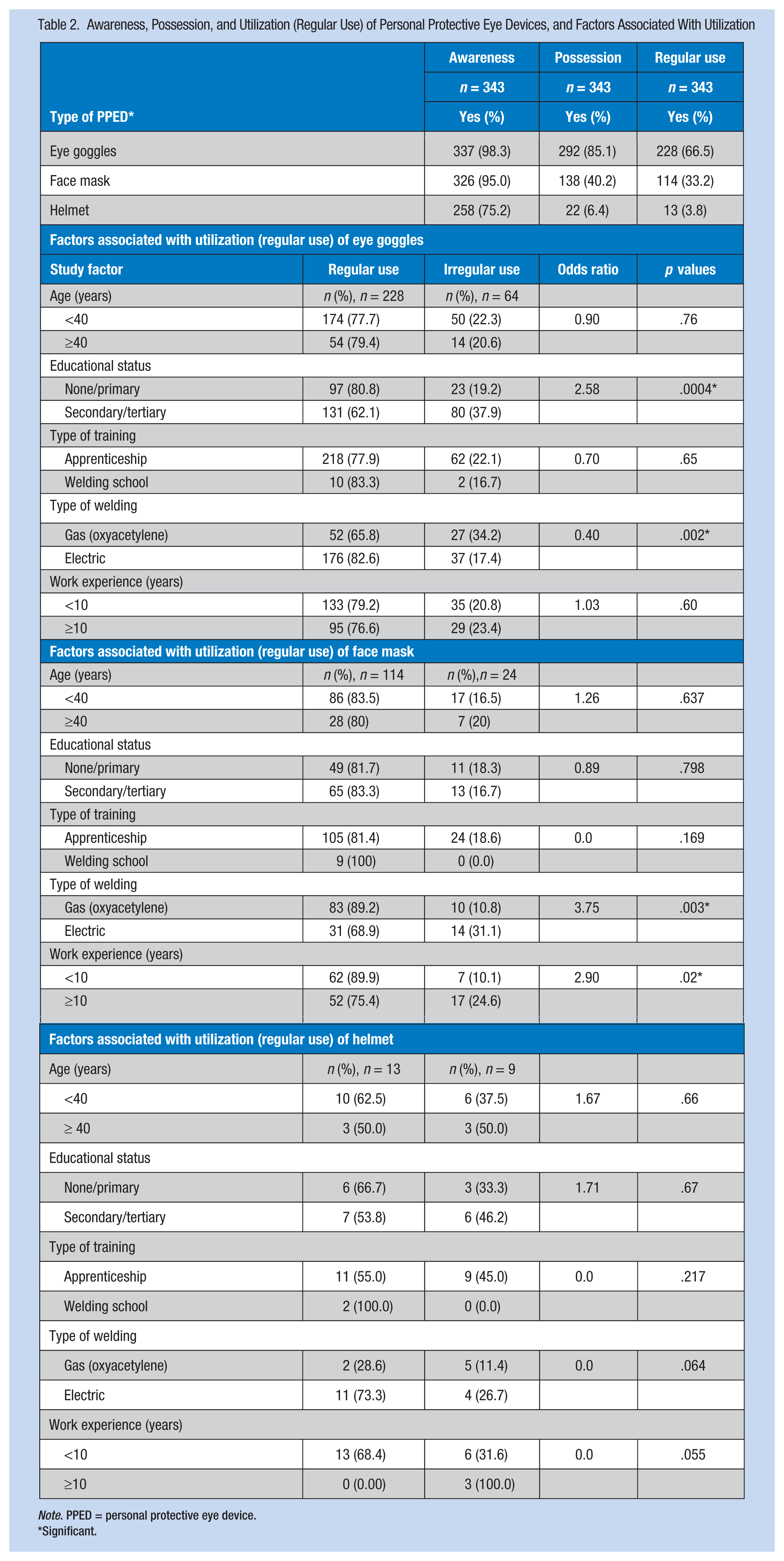
Note. PPED = personal protective eye device.
Significant.
Statistical tests for significance of the observed associations between participants’ awareness of welding hazards and their awareness, possession, and utilization of each PPED did not reveal any significant (p < .05) associations. However, tests for significance of observed associations between awareness and “regular use” (utilization) of each PPED was significant for face masks (awareness vs. utilization, 34.9% vs. 5.9%; χ2 = 6.13; p < .05) but not for helmets (3.9% vs. 11.8%; χ2 = 2.76, p > .05) or goggles (67.2% vs. 52.9%; χ2 = 3.01, p > .05). However, “regular use” had a significant association with “possession” across the three PPEDs: goggles (possession vs. regular use, 77.7% vs. 1.9%; χ2 = 111.87, p < .01), helmets (59.1% vs. 0.6%; χ2 = 168.3, p < .05), and face masks (82.6% vs. 0.5%; χ2 = 249.58, p < .001).
One hundred eighty-two (53.1%) participants possessed only eye goggles and 35 (10.2%) only face masks but none (0.0%) owned a helmet. One hundred ten (32.1%) participants owned multiple PPEDs: goggles and face mask (88/110; 80%), goggles and helmet (7/110; 6.4%), and all three PPEDs (15/110; 13.6%). The percentage distribution of type of PPED used by type (gas or electric) of welding showed goggles (gas 40.5%, electric 81%), face mask (gas 63.3%, electric 14.2%), and helmet (gas 2.4%, electric 5.3%).
Only 7 (0.02%) participants used all three types of PPEDs regularly. Of those who used any of the three PPEDs regularly, regular use of eye goggles or face mask was significantly (p < .05) associated with lower educational status and electric (arc) welding. In addition, shorter (<10 years) work experience was significantly (p < .05) associated with regular use of face masks. Regular use of helmets did not show any significant association with any of the participants’ socio-demographic or job characteristics (Table 2). Compared with gas welders, electric welders were significantly more likely to regularly use goggles (electric 81.9% vs. gas 40.5%; likelihood ratio χ2 = 63.49, p < .001) and face masks (electric 13.9% vs. gas 2.3%; likelihood ratio χ2 = 103.095, p < .001) but not helmets (electric 5.5% vs. gas 2.3%; likelihood ratio χ2 = 2.18, p > .05).
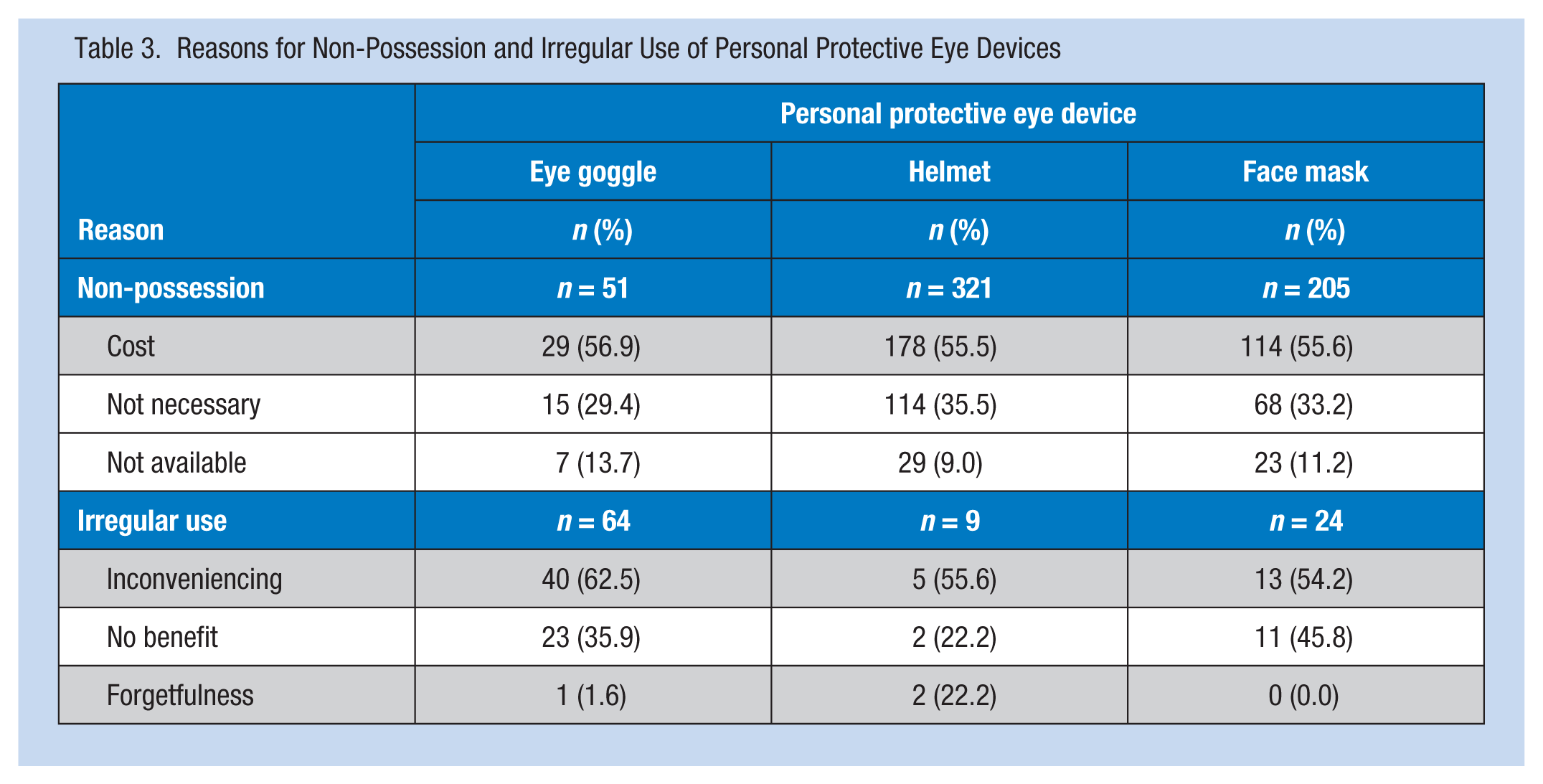
Of the participants who did not possess at least one of the three PPEDs, cost was the most frequently reported reason for not owning PPED followed by “presumed non-utility” and “non-availability.” Compared with those who possessed PPED, those who did not possess eye goggles were significantly (p < .05) less educated; those who did not possess helmets or face masks had significantly (p < .05) longer work experience. Participants’ age was not significantly associated with possession across the three PPEDs investigated.
Similarly, the participants’ main reasons for irregular use of any of the three PPEDs were reported to be “inconvenience of use” followed by “presumed lack of protective benefit” and “forgetfulness.” Table 3 reports the reasons for non-possession and irregular use of PPEDs.
Reasons for Non-Possession and Irregular Use of Personal Protective Eye Devices
Discussion
The socio-demographic profile of the survey participants showed they were all males, predominantly age 40 years or younger, with a minimum of primary education. The participants’ age characteristic mirrors previous reports in Nigeria (Ajayi et al., 2011; Davies et al., 2007; Isah & Okojie, 2006; Oduntan, 1998; Omolase & Mahmoud, 2007; Sabitu et al., 2009), France (Boissini, Peyresblanques, Rollin, & Beaufils, 2002), and Pakistan (M. A. Shaikh & Shaikh, 2005). However, the absolute male gender dominance differs from a Hong Kong report (Yu et al., 2004) probably due to between-survey differences in case mix and socio-cultural settings. The observed age distribution likely reflects the age group capable of withstanding the physical stress inherent in welding. The restriction of participation in the present survey to qualified welders, although consistent with the survey methodologies reported in Nigeria (Sabitu et al., 2009) and Pakistan (M. A. Shaikh & Shaikh, 2005), precludes the extrapolation of survey results to trainee or apprentice welders. Therefore, data on this select sub-group of welders are needed because they practice in the same work environment and share similar risk exposure characteristics with workmen welders.
The respondents were predominantly apprenticeship-trained arc welders whose work experience ranged from 1 to 10 years. The observed pattern of participants’ job training is similar to the report in Kaduna, Nigeria (Sabitu et al., 2009); however, further comparisons with other Nigerian and other reports (Davies et al., 2007; Isah & Okojie, 2006; Oduntan, 1998; Omolase & Mahmoud, 2007; M. A. Shaikh & Shaikh, 2005; Wang et al., 2006) were not possible due to lack of comparable job training data in these reports. The preponderance of electric welders in the present survey corroborates previous reports on commercial and freelance welders in Kaduna (Sabitu et al., 2009), Ile-Ife (Ajayi et al., 2011), and Calabar, Nigeria (Davies et al., 2007). However, reports elsewhere (Davies et al., 2007; Dixon & Dixon, 2004; Isah & Okojie, 2006; Oduntan, 1998; Omolase & Mahmoud, 2007; M. A. Shaikh & Shaikh, 2005) did not categorize their survey participants by type of welding, thus restricting further comparisons between surveys. The inherent inconvenience, and risk of gas explosions associated with gas welding, probably explain the dominance of electric welders. This finding has occupational health implications for welders because of the established comparatively higher risk of welding exposure-associated ocular hazards (Davies et al., 2007) and illnesses (Davies et al., 2007; Dixon & Dixon, 2004) among electric welders. Therefore, health education and training strategies should target this predominant, vulnerable sub-group. In addition, similar future population-based surveys should categorize respondents by type of welding.
An overwhelming majority of the respondents were aware of welding-associated ocular health hazards. This finding is comparable with previous Nigerian reports in Owo (100%; Omolase & Mahmoud, 2007) and Benin City (91%; Isah & Okojie, 2006), but differs from 77% in another Nigerian report (Sabitu et al., 2009) and 50% in Pakistan (M. A. Shaikh, 2001). Although the present survey and the other two Nigerian surveys (Isah & Okojie, 2006; Omolase & Mahmoud, 2007) with comparable awareness levels were conducted in southern Nigeria, the Kaduna (Sabitu et al., 2009) report included participants from northern Nigerian. Thus, the observed similarities in southern Nigerian surveys and data discrepancies with northern Nigerian and Pakistani surveys could be attributed to cross-setting differences in accessing occupational health information, time interval between surveys, or both. In addition, between-survey variations in participants’ socio-economic characteristics might further explain the observations. The high level of awareness of welding-related ocular hazards suggests that occupational eye health safety interventions to reduce welding-related ocular hazards should focus on overcoming the identified barriers to PPED acquisition and utilization, not creation of hazard awareness. However, to sustain the high level of hazard awareness, a definite need has been identified for reinforcement through periodic targeted and tailored health education campaigns (Ajayi et al., 2011; Yu and colleagues, 2004).
Although a significant majority of respondents demonstrated PPED awareness, overall and by device type, wide variations were reported for specific PPED type. The findings could only be partly compared with a Nigerian survey (Ajayi et al., 2011), which reported a 90.6% general PPED awareness, but not by PPED type. Further comparisons with other survey results (Forst et al., 2004; Oduntan, 1998; Omolase & Mahmoud, 2007; Sabitu et al., 2009) could not be made as they reported data on PPED possession and utilization, not awareness. This omission suggests that the present findings on PPED awareness are new data. Although awareness does not invariably translate to behavioral change, awareness remains an essential prelude to possession and utilization of welding task-appropriate PPED. Therefore, baseline PPED awareness data, overall and by PPED type, should be captured in future surveys. This approach would assist in planning and implementation of proactive occupational eye safety interventions through precise identification of intervention points to reduce ocular injury and morbidity among welders (Lombardi et al., 2005).
For each of the PPED investigated, the participants’ possession rates were lower than their corresponding awareness rates. Also, wide between-device variations in the participants’ possession rates were found in this study. The participants’ possession rates for eye goggles and face masks were higher than reported rates (i.e., goggles [63.3%] and face masks [26.6%]), in Kaduna, Nigeria (Sabitu et al., 2009); however, the 29.1% helmet possession rate in the Kaduna report is far higher than the 6.4% in the present study. Wide gaps between participants’ PPED awareness rates and possession rates continue to exist. The present report identified cost and “presumed lack of need” as the major barriers to PPED possession. The role of cost in PPED possession has been variously reported (Forst et al., 2006; Lombardi et al., 2009; Verma et al., 2011), especially in developing countries (Ajayi et al., 2011; Omolase & Mahmoud, 2007; Sabitu et al., 2009) with limited financial resources. Presumed limited preventive utility of PPED has been identified as a potent barrier to PPED use in developing (Ajayi et al., 2011; Omolase & Mahmoud, 2007; Sabitu et al., 2009) and developed (Forst et al., 2006; Lombardi et al., 2009; Verma et al., 2011) countries. Therefore, provision of free or low-cost PPEDs by the government’s public health department is instructive.
Similarly, PPED utilization rates, which lagged behind their respective possession rates, varied widely between the three types of PPED, highest for goggles and least for helmets. Lower educational status, electric welding, and shorter work experience were significantly associated with regular use of PPED. The leading reasons for non-use were “inconvenience of use” and “presumed lack of protective benefit.” Although the overall utilization rate could not be compared with previous reports due to lack of equivalent correlative data, the observed between-device differences in utilization rates is consistent with the utilization pattern reported in Nigeria (Sabitu et al., 2009). To overcome barriers to utilization, the authors suggest improvements in the ergonomics of PPED (Forst et al., 2006; Sabitu et al., 2009; Yu et al., 2004), enhancement of welders’ knowledge of PPED maintenance and care, and provision of deterrent to PPED non-use through enforced legislation (Lipscomb, 2000; Sabitu et al., 2009; M. A. Shaikh, 2001).
The generalizability of the conclusions drawn from this report is restricted by worldwide loco-regional differences in welders’ education and job training curricula, legislative enforcement of safety rules, and PPED availability and affordability. Specifically, participants’ recall bias inherent in self-report surveys and the questionable reliability of self-report and knowledge data are additional issues presenting further limitations to data extrapolation. An additional limitation could have arisen from respondents’ possible misunderstanding of the meaning and spectrum of ocular injury, despite elaborate explanation by the investigators. In the present survey, the “healthy worker effect” was minimal as the majority of participants selected from the prepared trade list were available for recruitment. Therefore, the enrolled sample was reasonably representative of the entire welders’ population in the study area. However, factoring these issues into future studies is warranted.
Conclusion
The majority of commercial and freelance welders in Enugu, southeastern Nigeria are aware of welding-associated ocular health hazards and devices to protect the eyes during welding. However, their awareness of these devices did not translate to possession, nor did possession translate to utilization. Cost and presumed non-utility were the main barriers to possession; “user inconvenience” and presumed “lack of protective benefit” were the main causes of low utilization. These findings have critical implications for all stakeholders in planning and implementing welders’ occupational eye health safety programs. Provision of affordable PPEDs with enhanced ergonomics and legislative enforcement of PPED use are suggested. Additional research via future nationwide surveys is urgently needed.
Applying Research to Practice
Commercial welders in southeastern Nigeria report high awareness of welding-related ocular health hazards and PPEDs. Awareness, possession, and utilization differ widely by PPED type. Critical gaps exist between PPED awareness and possession, and between possession and utilization. The identified barriers to utilization of PPEDs are preventable through multi-faceted interventions including occupational health education, provision of cost-free PPEDs with enhanced ergonomics, and legislative enforcement of their use.
Study Definitions
This study included formally trained commercial and freelance welders practicing their trade in the study area.
Privately owned industries are further subdivided into highly organized and structured large-scale industries (formal private sector) and medium- or small-scale industries (informal private sector).
Apprentice welders, welding school trainees, welding assistants, and other welding workers like panel beaters and pipe fitters who, although engaging in welding activities, did not receive any formal training in welding, were excluded from the study because their untrained work experience could confound the data (Sabitu et al., 2009; M. A. Shaikh & Shaikh, 2005).
Formal welding training implies satisfactory completion either through an apprenticeship or welding school.
Apprenticeship training requires agreement-bound certificated welding training provided by a qualified workman welder.
Electric (arc) welding uses a welding power supply to create an electric arc between an electrode and the base metal to melt the metals at the welding point.
Gas (oxyacetylene) welding uses the high temperature produced by burning a mixture of oxygen and acetylene to melt metals at the welding point.
Awareness of welding-associated ocular hazards requires knowledge of potential hazards to the eye associated with welding exposure.
PPEDs are personal appliances like welding goggles, masks, or helmets used to protect the eyes from potential ocular health hazards of welding exposure.
Welding goggles are special protective eyewear worn during welding to protect the eyes.
Welding face masks are worn during welding to protect the eyes and face.
Welding helmet is headgear worn during welding to protect the eyes, face, and neck from welding injuries.
Awareness of PPED includes knowledge of PPED and its usefulness in protecting workers against welding-associated ocular hazards.
Possession of PPED includes the ownership and unhindered access to functional PPED.
Utilization (regular use) of PPED is defined as wearing PPED during every welding exposure. It is not necessary to wear more than one PPED at a time; used singly, each device provides adequate protection against ocular hazard.
In Nigeria, formal education includes 6 years each of primary and secondary education, and 3 to 6 years of tertiary education depending on the cadre of training institutions and course of study.
Implications for Occupational Health Nurses
Occupational eye health interventions targeting commercial or freelance welders in low- and middle-income countries should build on their existing awareness, factoring in their socio-demographic and job characteristics. To maximize the public health impact of these interventions, the peculiar needs of arc welders, the dominant type of welders, should be prioritized. Specific interventions to address possession and utilization of PPED should include financial and legal advocacies to appropriate authorities to provide cost-free PPEDs and enforce utilization. In addition, specific occupational health education on the protective utility of PPEDs and improvement of PPED ergonomics could further enhance utilization.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Boniface I. Eze is a senior lecturer in Department of Ophthalmology, College of Medicine, University of Nigeria, and consultant ophthalmologist to University of Nigeria Teaching Hospital. He has research interest in occupational eye health.
Obiekwe Okoye is a senior lecturer in Department of Ophthalmology, College of Medicine, University of Nigeria, and consultant ophthalmologist to University of Nigeria Teaching Hospital. He has research interest in occupational eye health.
Emmanuel N. Aguwa is a senior lecturer in Department of Community Medicine, College of Medicine, University of Nigeria, and consultant community physician to University of Nigeria Teaching Hospital. He has research interest in occupational health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.