
Abstract
Background:
Occupational noise-induced hearing loss (NIHL) is the second most common medical disability for military veterans and accounts for 24% of all hearing loss in the United States. Hearing loss negatively affects health and billions of dollars are spent annually for direct and indirect medical costs and lost work productivity. Proper hearing protection device (HPD) fit can prevent NIHL. Quantitative fit-testing systems to determine personal attenuation rates (PARs) are available, but not widely utilized. Without quantitative testing, validating appropriate fit and attenuation to a permissible exposure level to prevent NIHL is difficult.
Methods:
A quality improvement project measured 100 employees enrolled in a hearing conservation program (HCP) to determine if they obtained a target PAR after inserting the HPDs in their “usual” fashion. Those who did not obtain target PAR (n = 27) received an evidence-based intervention that demonstrated proper HPD fit by a skilled trainer followed by a repeat attempt by the participant to replicate the feel of the demonstrated HPD placement. PAR was subsequently measured to assess for appropriate noise attenuation.
Findings:
Seventy-one percent achieved target PAR (≥ 20 decibels) at baseline testing. After the intervention, 91 of 100 participants had achieved target PAR, a 20% improvement.
Conclusions/Implications for Practice:
Findings suggest this evidence-based intervention was an effective strategy for improving HPD fit for employees enrolled in HCPs. This intervention may prevent occupational hearing loss and decrease the health and socioeconomic impacts of NIHL.
Keywords
Background
Hearing loss is a major public health concern with significant individual and societal impacts globally. In a prevalence-based costing model in 2019, McDaid et al. estimated the burden of hearing loss exceeded US$981 billion and affected 1.57 billion people worldwide. Nearly 80% of those costs came from direct and indirect effects on health and quality of life while lost productivity was conservatively estimated to cost US$182 billion globally. The authors estimated US$50 billion could be saved if only 5% of hearing loss is prevented.
In the United States, the impact of hearing loss is poorly studied and estimates of costs vary widely. Huddle et al. (2017) estimated direct medical costs of hearing loss in the United States at US$3.3 to US$12.8 billion with lost productivity estimates exceeding several billions of dollars. This cost assessment may not capture the full magnitude of the problem since military service members are not included in these reports. Therefore, these costs underestimate the impact on the veteran population who are notably at increased risk of hearing loss due to occupational hazardous noise exposure. For instance, in 2012, 1.8 million new disability claims were filed through the U.S. Department of Veterans Affairs (VA) amounting to US$1.2 billion in compensation claims (Alamgir et al., 2016). Disability claims for auditory complaints continued to increase and exceeded an additional 1 million claims in Fiscal Years 2015 to 2019; hearing loss and tinnitus, a comorbidity of hearing loss, continued to be the top two service-connected (SC) disabilities at the VA accounting for over 3.4 million claims and one third of the top 10 most prevalent SC disability claims in 2019 (U.S. Department of Veterans Affairs, 2020).
In addition to enormous financial costs, health, quality of life, and social impacts have been reported. Hearing loss can contribute to hypertension, heart disease, depression, isolation, loneliness, grieving the loss of sounds, increased fall risk, dementia, and increased emergency room visits and hospitalizations (Centers for Disease Control and Prevention [CDC], 2019; McDaid et al., 2021; Reed et al., 2018). Employees may experience decreased earning potential and limited advancement opportunities if hearing loss negatively affects effective communication or ability to meet occupational hearing standards (Yankaskas, 2013). When highly trained and skilled employees or leaders are disqualified for work, employers incur substantial costs associated with the time and expense of training replacements (Yankaskas, 2013). Since noise-induced hearing loss (NIHL) is permanent and irreversible, reducing the incidence of NIHL is vital for better hearing as other factors (e.g., medical comorbidities, toxic chemical exposures, and age-related hearing loss) can negatively affect hearing (Cooper et al., 2014).
The significant health, quality of life and socioeconomic impacts of hearing impairment for individuals, society, and employers highlight the need to prevent hearing loss. In the United States, occupational NIHL accounts for 24% of all hearing loss despite Occupational Safety and Health Administration (OSHA) regulations enacted in 1983 to help mitigate the risks from hazardous noise exposure at work (CDC, 2018, 2019). Nelson et al. (2016) estimated that 10% to 20% of NIHL could be prevented with the appropriate use of hearing protection devices (HPDs).
Noise is one of the most prevalent occupational hazards encountered by workers in a variety of settings and industries, especially in the defense industry (Nelson et al., 2016; United States Department of Labor [DOL], Occupational Safety & Health Administration, 2002). Prolonged exposure to noise levels at or above 85 dBA (8-hour time-weighted average) can lead to temporary or permanent hearing loss (United States Department of Labor [DOL], Occupational Safety & Health Administration, 2002). Due to the high cost and impact of hearing loss on military readiness, the Department of Defense (DoD) utilizes the more conservative prevention approach recommended by the National Institute of Occupational Safety and Health, which recommends an 85 dBA action level as well as a 3 decibel (dB) exchange rate when determining exposure limits compared to 29 CFR § 1910.95 (CDC, 2018; Occupational Safety and Health Administration [OSHA], 1983b).
Current Practice
Among other requirements for a hearing conservation program (HCP), federal regulation requires that employers conduct evaluations of the hearing protection in use to determine effectiveness for reducing noise exposure to acceptable levels (OSHA, 1983a, 1983b; United States Department of Labor [DOL], Occupational Safety & Health Administration, 2002). Employers have historically used the Environmental Protection Agency noise reduction rating (NRR) labeled on the HPD product to calculate an estimate of how well HPDs reduce noise exposure in individuals (OSHA, 1983b; United States Department of Labor [DOL], Occupational Safety & Health Administration, 2002). NRRs are based on estimates of the noise attenuation for subjects tested in a controlled laboratory setting, not real-life work settings (Berger, 2003; CDC, 2015). An estimate of the field value of attenuation based on NRRs established in laboratory settings is a poor indicator of personal attenuation due to variability in the size and shape of individual ear canals (CDC, 2015). Furthermore, HPDs that fit poorly or are improperly worn decrease the likelihood of achieving adequate noise protection (Berger, 2003; Federman & Duhon, 2016).
Evidence-Based Intervention
In 2008, the OSHA Alliance endorsed HPD fit testing as a best practice tool to train employees on proper HPD insertion, to determine and document the hearing protector attenuation levels of HPDs, and assist “training the trainer” to ensure proper HPD fit in employees. In addition to initial training on HPD use, fit testing allows employers to demonstrate effective training as required by regulation when new HPDs are acquired or anytime refitting/retraining is required such as when an employee experiences a decrease in hearing on audiometric testing compared to baseline (i.e., a significant threshold shift [STS]; OSHA, 1983b; OSHA Alliance, 2008).
Since that endorsement in 2008, OSHA issued a letter of interpretation of 29 CFR § 1910.95 in 2017 that supports the use of HPD fit testing to train employees and ensure proper HPD selection and fit. In 2018, the American National Standards Institute (ANSI) published additional guidance on HPD fit-testing systems in ANSI/ASA S12.71-2018. Several studies have been conducted and highlight the benefits of HPD fit testing as a training tool and a way to ensure appropriate noise attenuation from HPDs. Byrne et al. (2017) compared various fit testing systems to assess reliability and variability. Other authors have explored various ways to conduct fit testing with similar conclusions, incorporating an HPD fit-testing program into an HCP improves individual ability to properly fit HPDs and achieve appropriate noise attenuation to avoid both under, and overprotection when working in hazardous noise (Federman & Duhon, 2016; Federman et al., 2021; Gong et al., 2019, 2021; Murphy et al., 2016; Sayler et al., 2018; Smith et al., 2014). Nevertheless, while private sector industries are starting to implement HPD fit testing into their HCPs, the practice is not widely utilized within the military.
In 2016, Federman and Duhon assessed the viability of HPD fit testing in newly enlisted military personnel. For the subjects who failed to achieve the target personal attenuation rate (PAR) on initial self-fit testing, the audiologist researcher inserted the HPDs into the participant’s ears to demonstrate proper HPD fit. Once individuals received reliable validation of proper HPD insertion via expert-fit, they were asked to reinsert the earplugs into their ears replicating the “feel” of properly inserted HPDs. PAR was reassessed to demonstrate the participant had achieved proper HPD fit. The authors’ findings indicated that expert HPD fitting and participant return demonstration with fit-test validation was an effective training method that significantly improved PARs (Federman & Duhon, 2016). Studies by Gong et al. (2019), Gong et al. (2021), Sayler et al. (2018) and Ullman et al. (2021) have confirmed that HPD fit testing is an appropriate training method to ensure proper HPD fit and prevent occupational NIHL.
Need for Improvement
Occupational health nurses frequently encounter workers who are exposed to hazardous noise on the job and suffer the effects of NIHL. HPD fit testing is a valuable, evidence-based practice occupational health nurses can use to ensure appropriate protection from noise hazards, prevent occupational NIHL, and improve the health of this worker population.
For this project, multiple factors contributed to identifying the need for effective and efficient processes to integrate HPD fit-testing in a military occupational health clinic: (a) to protect military and civilian defense industry workers from the significant impacts of occupational NIHL through evidence-based practice; (b) acquisition of a Field Attenuation Estimation System to conduct fit-testing and measure HPD attenuation rates; and (c) the need for standard operating procedures for HPD fit testing due to the anticipated policy mandate within the next 2 years.
The purpose of this article was to discuss a quality improvement (QI) project that was designed and implemented to improve the effective use of HPDs to reduce NIHL.
Methods
Overview of the Project
This QI project took place in an occupational health clinic that served nearly 10,000 federal civilian defense industry and military personnel who were enrolled in the HCP in accordance with OSHA’s noise standard (OSHA, 1983b). Workers served in a variety of roles maintaining and repairing ships and aircraft, and working in industrial, public service and construction jobs. The FitCheck Solo™ was used to measure PAR. This system (previously known as HPD Well-Fit™) was tested by Byrne et al. (2017) and performed well compared to standards designed to measure real-ear attenuation of HPDs and ensured reliability controls were built into the system to achieve consistent and accurate responses (American National Standards Institute [ANSI], 2008).
The purpose of this QI project was to improve the effective use of HPDs by introducing a fit-test validation and intervention program and to determine if occupational health staff could be effectively trained to implement this program and improve HPD fit for noise-exposed workers. The occupational health nurse practitioner served as project leader (PL), conducted fit testing and intervention, and documented the process. The Plan, Do, Study, Act (PDSA) cycle was used to plan and implement the project, analyze results, and modify actions based on the results throughout the 3-month project (Moran, 2020).
Project Process
Step 1: Training the project team
The PL utilized training obtained through the Council for Accreditation in Occupational Hearing Conservation and U.S. Navy Hearing Conservationist courses and written instructions from the Centers for Disease Control and Prevention (CDC) for fitting hand-formed, moldable ear plugs and pre-molded ear plugs into the participant’s ears (Department of Health and Human Services et al., n.d.). The PL reviewed the FitCheck Solo™ user manual for guidance on utilizing the fit-testing equipment and consulted with an audiologist as needed. Practice sessions were conducted on five clinic employees and proficiency on HPD fitting and use of the equipment was confirmed by an audiologist.
Step 2: Recruitment
One hundred participants were recruited from employees scheduled for occupational audiograms from October to December 2020. All genders and races of military and civilian personnel who worked for the DoD and were between 18 and 70 years old; proficient in English; enrolled in the HCP due to exposure to noise ≥ 85 dBA; utilized commercially available, non-customized earplugs (e.g., hand-formed, moldable or pre-molded); and agreed to participate in the project were eligible for inclusion. Individuals with hearing loss ≥ 55 dB in either ear at the tested frequencies (500 hertz [Hz], 1,000 Hz, and 2,000 Hz), ear complaints that required medical evaluation, or who did not meet the inclusion criteria noted above were excluded. Participants were recruited in a nonrandomized order based on the convenience and availability of staff to conduct the testing. Participants completed a demographics questionnaire before testing.
Step 3: Determining PAR
A Dell® laptop with Windows® 10 software, a wireless mouse, and the FitCheck Solo™ software/device licensed and sold through Michael and Associates (2015a) were utilized to measure and calculate PARs as A-weighted attenuation rates that are comparable to NRRs (Michael and Associates, 2015b). To reduce the time for testing, three frequencies (500 Hz, 1,000 Hz, and 2,000 Hz) were utilized for assessment. Several researchers demonstrated that testing more than these frequencies failed to significantly affect PARs (Federman & Duhon, 2016; Murphy et al., 2016). The system was calibrated daily according to manufacturer instructions before testing was conducted.
Participants were seated in a quiet room, given instructions for the test procedures as noted in the FitCheck Solo™ user manual, and instructed to put on the headset. The clinician confirmed that a good seal of the device earmuffs was obtained prior to performing measurement. Participants were then asked to remove the headset and choose between a wide variety of commercially available, hand-formed, or pre-molded earplugs that most closely resembled the HPDs available to them at work. The HPDs available in the clinic had NRRs labeled 27 dB–33 dB. If the participant brought HPDs from the workplace, the participant utilized those HPDs; NRRs were not available for those products, however, DoD policy mandates that all HPDs have an NRR appropriate for the exposure level. For the occluded measurement, participants were instructed to insert the selected HPDs in their usual fashion and test procedures were repeated. The FitCheck Solo™ calculated the baseline PAR based on these unoccluded and occluded measurements.
Individualized noise exposure levels for each individual were not available to the PL, therefore a target PAR of 20 dB was chosen since military standards require the use of single HPDs when noise exposures are 85 dBA–104 dBA. At noise levels > 104 dBA, double hearing protection is required (Department of Defense Instruction [DoDI] 6055.01, 2014; OPNAV Instruction 5100.19F, 2019; OPNAV Instruction 5100.23H, 2020). A 20 dB PAR indicates that the individual can adequately protect hearing in any setting where single HPDs are required.
Step 4: The intervention
Participants who did not achieve ≥ 20 dB baseline PAR received the intervention which consisted of the PL placing the HPDs into the participant’s ear canals using manufacturer and CDC recommended insertion protocols. Once placed, the occluded test was repeated to determine if target PAR was achieved by the trained user. The individual was then asked to remove and self-fit the HPD replicating the “feel” of the trained-user fitted HPD. Reassessment was performed to assess whether the participant achieved proper fit post-intervention. Those who did not achieve the target PAR via self-fit or PL fit were referred to an audiologist for further evaluation.
Project Framework
As the project progressed, rapid successions of the PDSA cycle allowed for adjustments to improve the process and decrease test time. Manufacturer instructions were modified to better instruct participants on finding the lowest audible threshold. To reinforce the muscle memory aspect of the intervention, the PL inquired whether participants could “feel” a difference between the initial HPD insertion and the PL’s insertion of HPDs. Based on the response, the PL tailored coaching and instruction to help participant’s replicate that feeling in the ear canal.
Data Analysis
Descriptive statistics were used to characterize the continuous and categorical variables of interest. The Wilcoxon signed ranks test was used to compare PARs between baseline and postintervention timepoints. Kendall’s tau correlation was used to examine correlations between age and PARs at baseline, intervention, and postintervention timepoints. Mann Whitney U tests were used to determine if PARs were significantly different between work status (military versus civilian personnel). Partial correlation was performed to explore if age was significantly correlated to postintervention after controlling for work status. Cohen’s d and correlation coefficient (Tb), were computed as a measure of effect size. All statistical analyses were conducted utilizing commercially available software (IBM SPSS® version 27).
This QI project was approved by the institutional QI Project Review Committee and was determined to fit within the parameters of an evidence-based QI project.
Results
Demographics
One hundred participants (N = 100) were recruited and completed the baseline PAR. For all participants, mean age was 33.93 years and ranged from 19 to 68 years; 78% were active duty and 22% civilian workers; 32% were in aviation or aviation support, 21% supported ships, and 47% were in manufacturing support roles or public service jobs. Median time to complete baseline testing was 10 minutes, which included demographic input and recordkeeping post-test. Seventy-one percent achieved a target baseline PAR ≥ 20 dB (n = 71, M = 30.46, Mdn = 29.6; SD = 7.25). After the intervention, 20 additional participants achieved target PAR for a grand total of 91% (N = 100) of project participants achieving target PAR (i.e., 20% more than baseline).
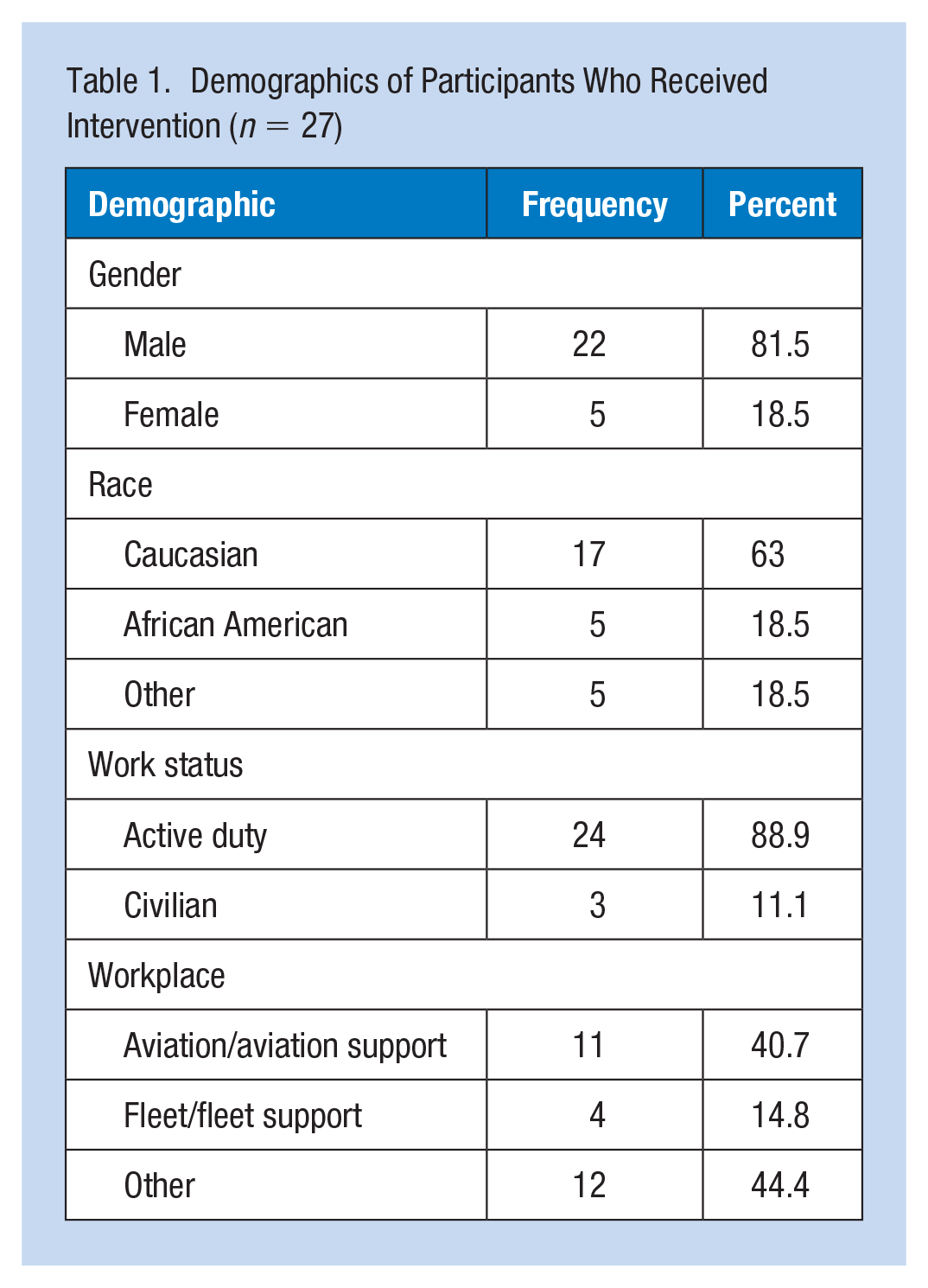
Twenty-nine participants were referred for refit due to < 20 dB PAR. Two received the intervention but did not complete postintervention fit testing and were excluded from analysis; therefore, a total of 27 completed the postintervention test and were included in the analyses for intervention and postintervention timepoints. The mean age of the intervention group was 31.07 years (Mdn =30; SD = 9.88). For the intervention group, the average time to complete testing (baseline PAR, intervention PAR, and postintervention PAR was 16.8 minutes (Min = 11 minutes, Max = 20 minutes). Frequency data are listed in Table 1 for the intervention group (n = 27). Occupations represented in the intervention group included aviation, industrial manufacturing trades, construction workers, firefighters, and police officers.
Demographics of Participants Who Received Intervention (n = 27)
Intervention Group PARs (n = 27)
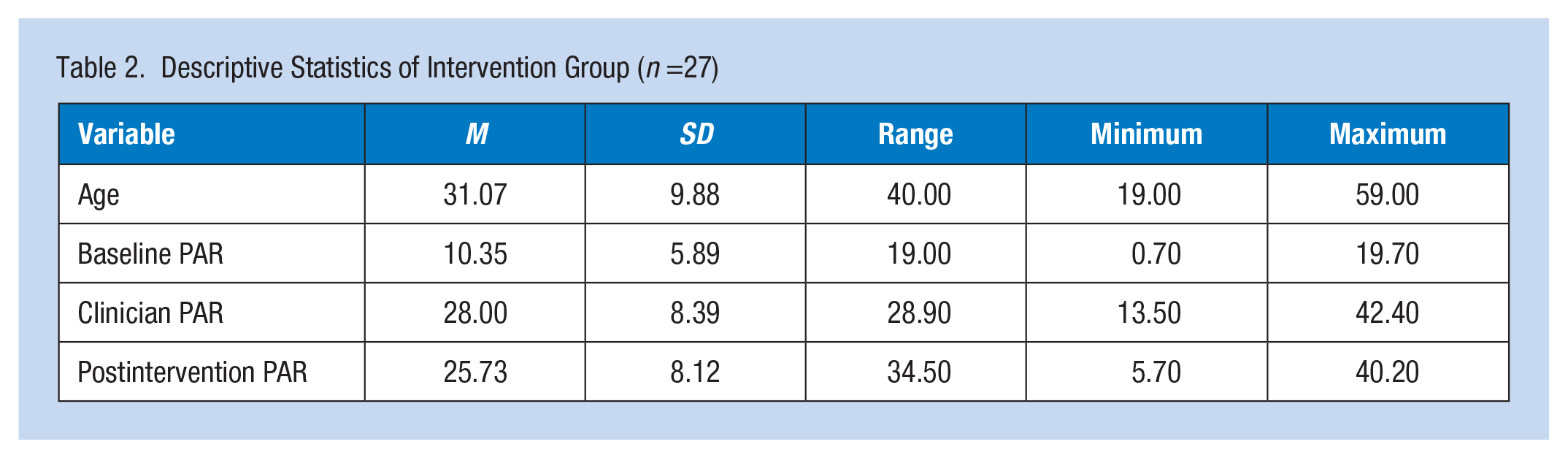
Eighty percent of participants selected hand-formed HPDs and 20% chose preformed HPDs, including two participants who brought their personal preformed HPDs, for testing. Table 2 shows PARs for the intervention group. Baseline and postintervention PARs were compared to examine the success of the intervention. Analysis showed a statistically significant difference between the two timepoints (p < .001) with a large effect size (Cohen’s d = 1.566). For the military personnel (n = 24), 76.4% (n = 20) achieved target postintervention PAR, but none of the civilian personnel (n = 3) achieved target postintervention PAR despite two thirds achieving target PAR when the clinician inserted HPDs. Table 3 shows the success rates for intervention and postintervention PAR. Sixty-seven percent (n = 18) passed both intervention and postintervention PARs while 11% (n = 3) failed both PARs.
Descriptive Statistics of Intervention Group (n =27)
Frequency of Success Rates (%) Between Intervention and Postintervention PAR
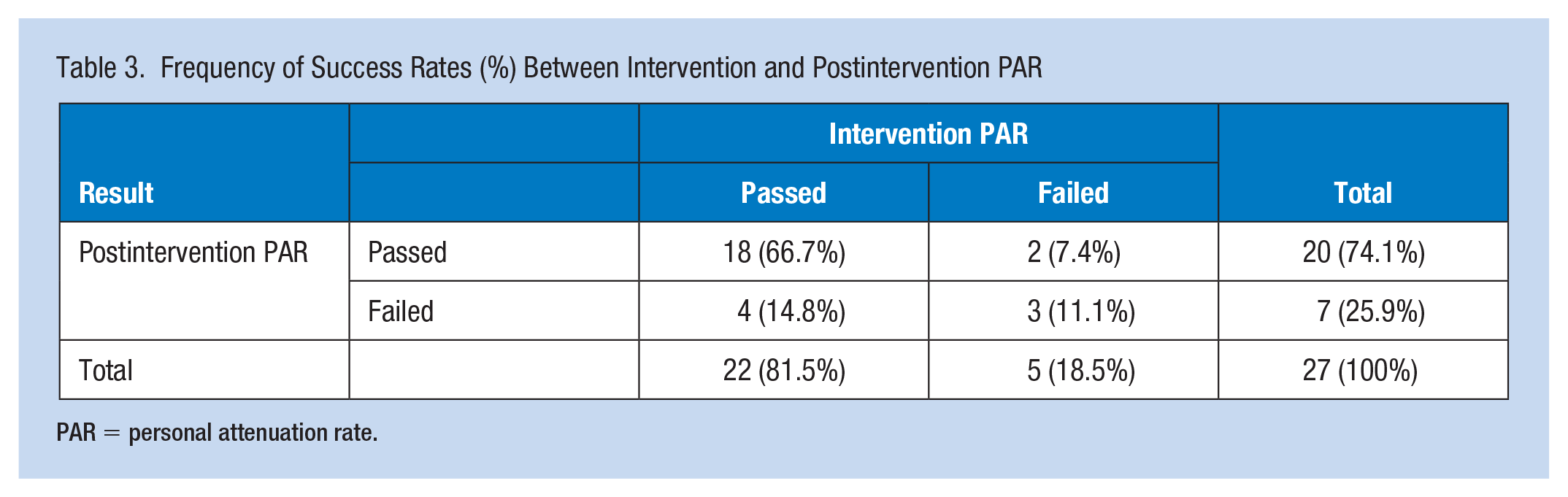
PAR = personal attenuation rate.
Age, Work Status (Military vs. Civilian Personnel), and PARs
Age was not significantly correlated to baseline PAR (p = .266) and intervention PARs (p = .387); however, age showed a significant negative correlation to postintervention PAR (p < .001) indicating younger participants achieved better PARs at the postintervention. Average age of participants who achieved target PAR was younger (n = 20, M = 28.15, SD = 7.93) than those who did not achieve target PAR (n = 7, M = 39.43, SD = 10.68) at the postintervention. There was no significant difference between work status and PARs on baseline (p = .220, Cohen’s d = −.283) and intervention PARs (p = .174, Cohen’s d = 0.98); however, PARs were significantly different between military (n = 24, M = 26.85, SD = 7.88) and civilian at postintervention (n = 3, M = 16.77, SD = 2.80) (p = .031) with the large effect size (Cohen’s d = 1.33). After controlling for work status, age was still significantly correlated to postintervention PARs, r(24) = −.485, p = .012. Figure 1 shows clustered boxplot of age by achieving target PAR and work status at the postintervention test. Young military personnel were more likely to achieve target PAR (≥ 20 dB).
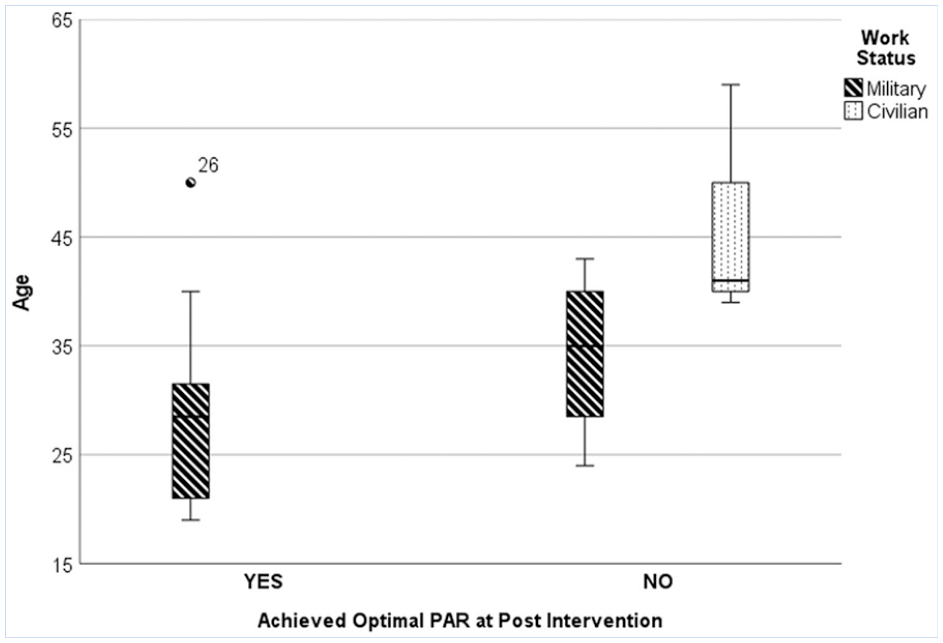
Clustered boxplot of age by achieving target PARs and work status at the postintervention test.
Discussion
Generalizability and Benefits
Although a large percentage of participants in this project achieved the target PAR at baseline, an additional 20% of participants achieved that target postintervention demonstrating the effectiveness of this evidence-based intervention. In addition, findings suggested that training personnel earlier in their career may be more beneficial since older participants were less likely to achieve target noise attenuation rates after intervention. These findings emphasized the importance of high-quality initial training at the beginning of hazardous noise exposure, as well as intervening to fit test an employee when annual audiogram results show early warning for hearing loss instead of waiting for hearing injury to occur. Ullman et al. (2021) noted that higher PAR values were correlated with lower rates of hearing loss reiterating that early training through HPD fit testing may improve employee health and quality of life throughout their lifetime. More research on the long-term benefits of fit testing to reduce the incidence of NIHL is still needed.
Over time, employer costs may be offset through lower worker compensation claims when validated HPDs are documented in the medical record, and retention of qualified employees who otherwise could be disqualified from work as occupational NIHL occurs or is aggravated by nonoccupational confounding factors. In addition, the project confirmed that fit testing provided a feasible method of documenting that an employer had met the regulatory requirements of training to ensure appropriate HPD selection and fit (OSHA, 1983b). Differences between military and civilian postintervention PAR may be due to motivational factors, but further investigation is required to fully understand. Nine percent of participants failed to achieve target PAR postintervention. Although the wider variety of sizes/shapes of HPDs may have improved that rate, some participants may have required custom-made HPDs to achieve appropriate attenuation. Overall, this project is generalizable to personnel looking to implement a fit-testing program into an HCP across a wide variety of industries.
Strengths
Similar to other findings, the results in this QI project demonstrated that HPD fit testing was an effective method for training employees to properly insert HPDs (Federman & Duhon, 2016; Federman et al., 2021; Gong et al., 2019, 2021; Murphy et al., 2016; Sayler et al., 2018; Smith et al., 2014). In addition, this project showed that an evidence-based practice (i.e., using HPD fit testing to validate expert-fitted HPDs followed by participant return demonstration of self-fit using muscle memory to replicate proper fit) outlined by Federman and Duhon (2016) could be successfully implemented by staff in an occupational health clinic. Using PDSA cycles to evaluate and adapt as the project progressed was an effective framework to improve processes.
One key benefit of HPD fit testing noted in the OSHA Alliance (2008) Best Practice Bulletin is that HPD fit testing can be used as a “train the trainer” tool. This project demonstrated that staff could easily learn and develop proficiency to perform HPD fit testing by reviewing the equipment manufacturer instructions and consulting another trained user for questions. As an occupational health nurse learns to do fit testing, the knowledge can easily be used to train others.
Limitations
One limitation of this project was the small sample size (N = 100) from a wide variety of workplaces. Due to the volume of work centers represented, actual noise exposure levels for individuals were unavailable. It is possible that 20 dB of attenuation may represent overprotection for noise exposure, especially if participants worked in low to moderate levels of hazardous noise. For safety-sensitive jobs where hearing is critical, a fit-testing program provides a way to tailor the HPDs to the noise levels encountered ensuring employees achieve target protection that allows for safe listening and situational awareness (Gong et al., 2021; OSHA Alliance, 2008; Sayler et al., 2018). Overcoming the barrier of determining the actual noise attenuation needed on an individual basis is crucial to avoid both under- and overprotection. One possible solution is to utilize safety professionals in the workplace to conduct fit testing since they have access to noise level measurements and HPD options that are routinely available. The occupational health nurses can serve as a trainer and resource for safety professionals should questions or concerns arise. Occupational health nurses can also help facilitate referrals to an audiologist for complicated fittings or medical issues.
Another limitation of the project was the lack of actual HPDs used by participants in their workplace. Although similar HPDs were available, it is possible that HPDs in the project varied significantly in size, composition, and attenuation ratings from those available in the workplace. To ensure that employees can achieve adequate noise protection, fit testing with the actual HPDs available in the workplace is required. For the purposes of this project, however, the primary objective of demonstrating that staff could be trained to conduct fit testing and improve PAR results was achieved. Future cycles of the project will develop methods for utilizing HPDs actually available in the workplace.
Assumptions that a single fit-testing intervention is adequate to ensure a reproducible HPD fit over the span of a person’s career cannot be made. Even with proper training, there is no guarantee that employees will continue to insert HPDs to achieve adequate protection in real-life workplaces, therefore supervisors and safety personnel are critical to monitoring and enforcing appropriate use of HPDs. Additional studies should examine periodicity for fit testing to ensure continued proficiency in self-fitting HPDs.
This project excluded workers with hearing loss in the designated HPD fit testing frequencies. Generally, HPDs should attenuate noise to around 75 dB to maximize ability to communicate and allow workers to hear alarms and warning signals (Sayler et al., 2018). Since overprotection can be as significant as under protection from hazardous noise, understanding how hearing loss affects HPD noise attenuation is a critical area that requires further study (Gong et al., 2021; Sayler et al., 2018).
Implications for Occupational Health Nurses
Occupational health nurses promote employee safety, health and wellness, and intervene to reduce employer costs associated with occupational illnesses and injuries. Occupational NIHL injuries account for significant worker compensation claims and can have devastating effects on an individual’s health and career. Using the evidence-based practice of HPD fit testing allows occupational health nurses to protect worker health, prevent occupational NIHL in employees and document employer compliance with federal regulations related to HCPs.
To implement a fit-testing program, adequate resources for equipment costs and time for personnel to complete HPD fit testing must be considered. Equipment cost estimates range from US$2,500 to US$4,000 (Murphy et al., 2013). Numerous varieties of HPD fit-testing equipment are commercially available and new products are added each year. Occupational health nurses must ensure that equipment utilized for fit testing is validated and will provide reliable results for the testing environment using applicable guidance (ANSI, 2018; Berger, 2003; Berger, in press; EPHB Report No. 360-11a, 2015).
Time to conduct fit testing varies by system and with the number of trials an individual needs to achieve appropriate PAR. Time to complete fit testing using FitCheck Solo™ in this project was comparable to other studies using this system showing minimum time of 5 minutes for baseline testing and maximum of 30 minutes for up to four fit tests (Gong et al., 2021; Michael and Associates, n.d.; Murphy et al., 2016). Considering cost of equipment, personnel and time, the cost–benefit ratio for a 20% improvement in participants who achieved target PAR appears worthwhile.
Obtaining adequate HPD attenuation levels is key to a successful program. Several factors affect an employee’s HPD use including comfort, convenience, availability, compatibility, and the employee’s beliefs about the ability to properly insert HPDs to prevent NIHL without compromising safe and effective communication (Hudak, 2005). Effective protection requires that HPDs be worn 100% of the time in hazardous noise exposure (OSHA Alliance, 2008). If employees remove earplugs in hazardous noise situations to better hear communication, overexposure occurs. These factors must be considered when occupational health nurses implement a fit-testing program and conduct training. Additional resources are available for occupational health nurses seeking to implement a fit-testing program (ANSI, 2018; Berger, 2003; Berger, in press; EPHB Report No. 360-11a, 2015).
Since occupational health nurses are more likely to be onsite than other hearing professionals who provide services as needed, they are well positioned to provide high-level point of care continuity and corporate knowledge for staff enrolled in HCPs. To broaden impact, occupational health nurses can train other occupational safety and health personnel in the workplace to conduct HPD fit testing and intervene to support and train employees who fail to achieve adequate noise attenuation with HPDs. Stakeholder buy-in and interdisciplinary collaboration with OSH professionals are critical to implementing a successful HPD fit-testing program. With a comprehensive team approach and this evidence-based practice to improve HPD fit, occupational health nurses can make significant progress toward reducing the impact of occupational NIHL.
Applications for Professional Practice
Occupational noise-induced hearing loss costs billions of dollars each year and has significant negative impacts on employee health, safety, and quality of life. Using HPD fit testing to validate proper HPD fit demonstrated a significant improvement in PARs for those who did not initially achieve target noise attenuation. This evidence-based practice provided tangible feedback to employees regarding how proper HPD insertion “felt” in the ear canals and tested their ability to replicate that perception. This technology and intervention can improve safety and communication by customizing HPD fit to actual noise exposure levels in the workplace. An HPD fit-testing program documents effective employee training and compliance with federal regulations for HCPs. The benefits for employee and employer are likely to outweigh the costs of implementation. Occupational health nurses are well suited to promote best practices and lead the implementation of a successful HPD fit-testing program.
Footnotes
Acknowledgements
The authors would like to thank the participants in this project and the leaders and staff at Naval Hospital Jacksonville and Navy Medicine Readiness and Training Unit Mayport for their support throughout this project.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Some of the authors received tuition (Hayes) and salary (Hammond) funding through grant number T42OH008436 from the Deep South ERC. Otherwise, the Deep South ERC had no role in the study design; collection, analysis, and interpretation of data; writing the report; and decision to publish this project report.
Disclaimer
I am an employee of the U.S. Government. This work was prepared as part of my official duties. Title 17, U.S.C., §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C., §101 defines a U.S. Government work as a work prepared by an employee of the U.S. Government as part of that person’s official duties. The views expressed in this paper are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, the U.S. Government, or the Deep South Education and Research Center (ERC). Human Subjects Review This project was reviewed by the Quality Improvement Committee at the University of Alabama at Birmingham School of Nursing and deemed to be exempt from human subjects review and designated as an evidence-based, Quality Improvement initiative.
Author Biographies
Hayes completed this work while employed as the Occupational Health Program Director at Navy Medicine Readiness and Training Unit (NMRTU) Mayport. She now works as an Advanced Practice Nurse with the Office of Occupational Medicine and Nursing at OSHA. Her interests include regulatory and legislative policies to improve worker health and implementing evidence-based practices to reduce occupational noise-induced hearing loss, heat-related illnesses, and health care worker stress and burnout. She completed the project in partial fulfillment of the requirements of the Doctor of Nursing Practice degree and was responsible for the conception and design of the work, conducting the project (including data collection and analysis), and preparing the manuscript for publication.
Stephenson is an occupational audiologist and Hearing Conservation Program Manager for Navy and Marine Corps personnel. She works as a clinician, program consultant, and researcher to identify and integrate evidence-based conservation practices into Department of Defense policy. She assisted with the initial concept for the project and contributed subject matter expertise throughout all aspects of the project and manuscript development and revision.
Montgomery is a postdoctoral fellow at UAB and a statistical consultant for PhD dissertations and DNP projects as well as a data analyst for many research projects. Her research area is on burnout, well-being, circadian misalignment, and patient safety among nurses and nurse managers. She contributed to data analyses, interpretation, and revising the manuscript critically.
Hammond is an assistant professor at the University of Alabama at Birmingham (UAB) School of Nursing where she coordinates the Occupational Health Nursing Graduate Program. She was the faculty advisor and mentor for this project and was substantially involved in the project during design, implementation, analysis, and manuscript preparation. She also provided substantial support for critically reviewing the work for intellectual content and editing. All authors approved the final version and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.