
Abstract
The purpose of this study was to explore the relationship between occupational exposure to welding fumes and pulmonary function in an effort to add supportive evidence and clarity to the current body of research. This study utilized a retrospective chart review of pulmonary function testing and pulmonary questionnaires already available in charts from preplacement physicals to the most recent test. When comparing smokers to nonsmokers, utilizing multiple regression and controlling for age and percentage of time using a respirator, years welding was statistically significant at p = .04. Data support that smoking has a synergistic effect when combined with welding fume exposure on pulmonary decline.
One of the most common occupations associated with developing occupational lung disease is welding. An estimated one million workers worldwide perform some type of welding as part of their work (Antonini, Taylor, Zimmer, & Roberts, 2007). Multiple research reports have described the relationship between welding fumes and decline in pulmonary function (Bradshaw, Fishwick, Slater, & Pearce, 1998; Chinn, Cotes, Gamal, & Wollaston, 1995; Christensen, Bonde, & Omland, 2008; El-Zein, Gautrin, Infante-Rivard, & Malo, 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian, Loukzadeh, Shojaoddiny-Ardekani, & Aminian, 2011; Thaon, Demange, Herin, Touranchet, & Paris, 2012; Vallières et al., 2012). Because little has been published in the literature about specific effects of welding fumes, identifying the cause of pulmonary alteration among welders is essential in preventing lung disease and promoting health. Exposure to welding fumes is completely preventable. By completing additional studies in this area, further supporting evidence regarding prevention could be established.
Welding exposure over prolonged periods of time is cause for concern. Research illustrates that the health of workers is impacted by continued exposure to welding fumes. The term welding fume refers to any fume released by the cutting or connecting of metal using a welding technique (e.g., Tungsten Inert Gas [GTAW, TIG], Gas Metal Arc [GMAW, MIG], Shielded Metal Arc [SMAW or “stick”], and Flux Core Arc Welding [FCAW]; Occupational Safety and Health Administration [OSHA], 2015; Vallières et al., 2012). An arc is electricity that passes through a rod and “sparks” at the point of contact creating a temperature of up to 7000° F (OSHA, 2015). Stick welding describes the joining of two metals using a flux-covered electrode which is melted by an electric arc to fuse the two pieces being welded.
In addition to the types of welding, various metal compositions are used for a variety of construction types. Fumes are emitted during the heating and melting process of welding (OSHA, 2016a). The specific composition of fumes being released during welding is determined by the type of welding, nature of the base metal, composition of the welding rod, location, air movement and ventilation, and the use of filler fluxes and electrodes and their coverings (Vallières et al., 2012). The variety of metals used for welding include aluminum, antimony, arsenic, beryllium, cadmium, chromium, cobalt, copper, iron, lead, manganese, molybdenum, nickel, silver, tin, titanium, vanadium, and zinc (OSHA, 2016a).
Problem Statement
Current research has reported conflicting data related to welding fume exposure and lung decline. Most research has found a relationship between welding fume exposure and lung decline, but other studies have shown no relationship. The state of current research leaves several gaps in the literature. First, several articles do not delineate the specific type of welding in their studies (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Nakadate et al., 1998; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Second, most articles do not specify the specific amount of time workers weld daily but rather roughly estimate years of welding (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Finally, most articles do not use a standardized form to collect background participant data and reach more meaningful comparisons for future research (Bradshaw et al., 1998; Chinn et al., 1995; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011). The pertinent pulmonary information on this study’s form included job title with type of welding, previous worker health conditions, pulmonary symptoms, vision changes, years of welding, and previous occupations and exposures. The standardization provided by the pulmonary form improves instrument reliability. This study provided additional findings to add to the current body of research by including pulmonary function testing (PFT) and pulmonary questionnaires from participants’ charts.
Purpose
Occupational health and safety is a unique area of nursing and health care. Employees are at risk when exposed to welding fumes, dust, or chemicals. Continued exposure to these substances can place employees at risk for permanent lung changes. It is the responsibility of occupational health providers in collaboration with safety managers to assess the risk of illness and injury by evaluating employees via PFT. The purpose of this study was to explore the relationship between occupational exposure to welding fumes and pulmonary function to add supportive evidence and clarity to the current body of research. The research question was “What is the relationship among welding fume exposure, smoking, and pulmonary function among welders in a medium-sized company in southeast Tennessee?”
Significance of the Problem
Occupational lung disease is a significant topic of study for nurses and other occupational health professionals. Research about welding fume exposure included randomized controlled trials and systematic reviews. Previous research studies included a variety of welders, with and without personal protective equipment, in a variety of welding environments. This study includes welders, specifically welding steel, who were exposed to hexavalent chromium (Cr[VI]), a material added to alloy steel to increase corrosion resistance and hardenability (OSHA, 2016b). The main organs affected by Cr(VI) are the eyes, skin, liver, kidneys, and respiratory tract (OSHA, 2016b). The welders in this study worked in a building with side-by-side welding cubicles, increasing the possibility of higher concentrations of chromium fumes. Welders use full-face respirators when welding during their 8- to 12-hour shifts. These variables (e.g., shift length, environment, personal protective equipment) are unique to this study and will add to the current body of knowledge.
Current OSHA and NIOSH Recommendations
OSHA’s final Cr(VI) rule establishes an 8-hour time weighted average permissible exposure limit (PEL) of 5 ug/m3 measured as Cr(VI). This means that over the course of any 8-hour work shift, the average exposure to Cr(VI) cannot exceed 5 ug/m3. (OSHA, 2009)
The OSHA (2009) requires employers to provide respirators in the following situations: in emergencies, periods while installing or implementing engineering or work practice controls, when work operations for which engineering or work practice controls are not feasible, in situations where workers are exposed for less than 30 days per year and the employer has opted not to implement engineering or work practice controls, and in operations where all feasible controls have been implemented and are still not sufficient to reduce to or below the PEL. The OSHA (2009) recommends that employees have medical evaluations within 30 days after initial assignment to a Cr(VI) job, annually, whenever an employee is showing signs of exposure, within 30 days after a provider recommends re-evaluation, and at termination of employment to protect against possible chronic effects including lung cancer and liver damage (OSHA, 2009).
The National Institute of Occupational Safety and Health [NIOSH] & Education and Information Division (2013) recommends respirator use while performing any task for which the airborne exposure concentration is unknown or has been documented to be higher than the NIOSH PEL of 0.2 µg Cr(VI)/m3 8-hour time-weighted average (TWA) during a 40-hour workweek. Respirators should not be the primary means of minimizing exposures. Other control measures (e.g., engineering controls) should also be implemented to reduce exposure to at or below PEL before the use of respirators are required (NIOSH & Education and Information Division, 2013).
Background and Context
The literature review, using the Cumulative Index to Nursing and Allied Health Literature (CINAHL), included the key words “welding fumes” and “pulmonary.” PubMed, Google Scholar, and the Oxford Journals were searched using the terms welding fumes and pulmonary decline. Approximately one hundred fifty articles were analyzed for this research review. The most difficult aspect of retrieving the articles was the plethora of studies on welding fume exposures. However, each research study suggested differing strategies to mitigate the threat of exposure.
Literature Review
Documents from various databases were sorted by occupation of the participants and instruments used for evaluation. More specifically, welders spending most of their work time welding were evaluated via pulmonary questionnaires and PFT testing. Studies not meeting these criteria were excluded.
A critical appraisal provides a balanced review of the benefits and strengths of the research as well as its flaws and weaknesses (Holly, 2014). Welding exposures are a significant risk to welders (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). According to research studies, welding exposures can be minimized by using respiratory protective equipment and appropriate environmental ventilation; smoking cessation can minimize the effects of welding exposures (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
The research articles chosen were relevant to welding fume exposures and provided guidance in answering the research questions. Multiple articles highlighted an increase in respiratory symptoms and reduction in PFT values (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012) validating welders’ pulmonary decline and supporting the hypotheses. The article by Erkinjuntti-Pekkanen et al. (1999) was a 2-year replication of a study conducted by Bradshaw et al. (1998). Each study found a high prevalence of chronic bronchitis and respiratory symptoms with reduction of the peak expiratory flow (PEF) and significantly lower forced expiratory volume (FEV) and forced vital capacity (FVC). Again, these studies support the hypothesis that welding fumes are related to decline in pulmonary function.
Many of the articles provided new, supporting ideas (Christensen et al., 2008; El-Zein et al., 2003; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). In addition, research was consistent across studies and validated the research hypothesis that welding fume exposure is related to pulmonary decline. The majority of studies were retrospective chart reviews with small to moderate sample sizes. This study was designed to provide further evidence supporting the hypothesis that welding fume exposure is related to pulmonary decline and to clarify the risk of exposures to reduce the possible long-term effects of welding fumes.
Critique Across Studies
The hypothesis for each chosen article was that exposure to welding fumes is related to acute and chronic pulmonary symptoms and pulmonary decline (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Data illustrated no significant difference in the results between gas metal arc welding and other types of welding (Bradshaw et al., 1998). Welders complained of chronic bronchitis, which is more prevalent in current welders who also smoke (Bradshaw et al., 1998). Reports of work-related respiratory symptoms were more prevalent in current welders who did not smoke (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Results revealed no significant differences by ethnicity. On the contrary, several studies illustrated significant differences in smoking habits and years of work experience between welders and nonwelders (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Smoking and years welding significantly impact pulmonary decline.
Generalizability
The degree to which results of a study group can be used to represent the entire population is termed generalizability (“Exposure,” 2015). Welders engage in a wide variety of welding types and work in diverse environments. Each of the studies reviewed detailed the inclusion criteria for the participants and the environments in which they worked. Because multiple factors were identified for both the welders and their environments, the conclusions from the chosen studies are generalizable to the population of interest.
Unfortunately, no studies to date were conducted in Appalachia. The studies reviewed were from various areas around the world including both smoking and nonsmoking welders in a variety of jobs and from a variety of environments. Research participants were divided into samples with some wearing respirators and some not. This variety of inclusion also supports generalizability of study findings: Welding fumes are linked to pulmonary decline.
Common Themes and Approaches
Multiple variables and themes were common throughout the articles. One constant theme was pulmonary decline as a result of exposure to welding fumes (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Several studies used pulmonary questionnaires to assess patient-reported symptoms (Christensen et al., 2008; El-Zein et al., 2003; Hedmer et al., 2014; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Questionnaires allowed the researchers to correlate historical information (e.g., demographics, smoking status, time welding, and symptomatology). However, study questionnaires were not standardized (e.g., measuring the same information such as years of exposures vs. hours per day of exposure).
In addition, PFT was frequently used to assess changes in pulmonary function. Pulmonary function testing prior to beginning a job and at regular intervals during employment allowed researchers to establish when welding fumes affected pulmonary function (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Although lung function can be assessed in a variety of ways, PFT was the most common test reported.
Another recurring theme was the recommendation for welders to stop smoking to prevent pulmonary decline (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Smoking in combination with welding fume exposure increases lung inflammation and resulting pulmonary decline (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Therefore, welders should be encouraged to reduce or discontinue smoking.
Correlation With Research Questions
According to the reviewed research related to welding fume exposure, PFT consistently identifies decline in lung function (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Several research articles illustrated that smoking increases the incidence of pulmonary decline (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). The use of particulate respirators could prevent or reduce exposures and decrease the risk of pulmonary decline (Bradshaw et al., 1998; Erkinjuntti-Pekkanen et al., 1999; Ozdemir et al., 1995; Sharifian et al., 2011; Vallières et al., 2012). Research has not reported on the type of welding affecting the rate of exposure. Because a number of welding types exist, research studies must include each type of welding to provide evidence regarding rate of exposure. For this study, participants were exposed specifically to Cr(VI) which is emitted during the welding of steel.
It is unclear how willing employees would be to use masks during welding. If education illustrated safety risks, perhaps welders would be more likely to use respiratory protection. Research has shown that improper ventilation increases welding fume exposure (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Research has not concluded that a history of pulmonary disease compounds the effect of exposures to welding fumes. Research is difficult to conduct with workers who had respiratory illnesses prior to welding fume exposure.
Validity Issues
Bias
As with any study, bias could affect the selection of participants (Chinn et al., 1995). Because several of the studies were retrospective or longitudinal, participants were lost for a variety of reasons (Bradshaw, Fishwick, Slater, & Pearce et al., 1997; Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Selection criteria can introduce bias due to the elimination of exclusion criteria (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Participants’ recall of information also poses a limitation by affecting data accuracy and potentially the inclusion of participants in the study (El-Zein et al., 2003). Questionnaire data are used differently in each article and can affect results depending on how the data are used in the study (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Comparison Issues
Smoking complicates the interpretation and comparison of results specifically regarding the etiology of symptoms and the measurement of lifetime exposure (Bradshaw et al., 1997; Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Smoking status often changes during workers’ lifetimes and can become a compounding factor with exposures.
Physical activity and body composition change over time (Chinn et al., 1995). Cardiovascular exercise (e.g., running) can affect lung function and PFT values. Because several of the studies reported PFT comparisons, long-term exercise could have altered research results (Chinn et al., 1995). In addition, studies may span workers’ worklife when lung function is naturally changing (Chinn et al., 1995). Most PFTs account for age, body mass index, and smoking status but it is unknown what role age-related changes have on research data (Chinn et al., 1995).
Respiratory Symptoms
Chronic bronchitis and other work-related respiratory symptoms among welders are often the result of a combination of dusts from various sources (Bradshaw et al., 1997). Dusts are irritants much like tobacco smoke. Individual susceptibility plays a role in how the effects of dust exposure are expressed (Bradshaw et al., 1997; Chinn et al., 1995). An example is the potential for an individual employee to have respiratory hyper-responsiveness to dust, cigarette smoke, and other inhaled irritants. The specific inhaled metal particles may vary among welders as well as their particular welding type and work environment (Antonini et al., 2007; Bradshaw et al., 1997).
Several changes in welding techniques have occurred over the years (e.g., the removal of asbestos from welding rods, no longer applying harmful surface treatments to steel, providing new workplace ventilation systems, and changing the composition of metals; Antonini et al., 2007; Chinn et al., 1995). These changes in turn alter the potential composition of dust and the amount and type of worker exposures.
Exposure to welding fumes poses a significant risk to employee health. Research illustrates a wide variety of pulmonary effects related to welding fume exposures (Christensen et al., 2008; El-Zein et al., 2003; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). The primary variable used to assess pulmonary decline among welders in this study was PFT. Previous studies linked welding fume exposures to impaired lung function (Christensen et al., 2008; El-Zein et al., 2003; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Several studies included smoking and nonsmoking welders engaged in a variety of jobs (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Respiratory Testing
Analysis of welders who underwent PFT demonstrated an increased risk of reported respiratory disorders, lung infections, bronchitis, asthma, and obstructive lung disease (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Multiple reports found that welding fumes were a risk factor for lung disease even among nonsmoking welders (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Occupational exposure to welding fumes is considered a risk factor for chronic obstructive pulmonary disease (COPD; Vallières et al., 2012). Study participants complained of multiple symptoms including chronic cough with sputum production, persistent wheeze, airflow obstruction, respiratory symptoms, emphysema, bronchitis, asthma, siderosis, and gas trapping (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Also, pulmonary infections were more frequent and severe, and lasted longer among welders. The mixture of metals used in welding was a significant determinate of potential pneumotoxic responses (Antonini et al., 2007).
It can be concluded that improving workplace ventilation, smoking cessation, respiratory protective devices and periodic medical surveillance using health history questionnaires and PFT could decrease welding-associated lung symptoms (Bradshaw et al., 1998; Chinn et al., 1995; Christensen et al., 2008; El-Zein et al., 2003; Erkinjuntti-Pekkanen et al., 1999; Hedmer et al., 2014; Nakadate et al., 1998; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Method
Between January 2016 and July 2016, the health records of 39 chromium welders employed by an upper East Tennessee company were selected for this study which compared PFT results of two groups of Cr(VI) welders: those who smoked (17) and those who did not smoke (22). Of these welders, 38 were male, and one was female. Ages ranged from 20 years to 69 years with a mean age of 43.3 years.
Materials and Procedure
Consent for the de-identified chart review was secured from the company’s chief medical officer and the Lincoln Memorial University Institutional Review Board. Charts of welders were selected from the employee database, and numbers were assigned to replace employee identifiers. Data were then collected from the selected charts and entered into a Microsoft Excel spreadsheet. Data collected from each chart included years welding, years smoking, percentage of time wearing a respirator, pulmonary symptoms, first and last PFT values, chronological age, and lung age. Because the sample welders did not list any pulmonary symptoms or history of asthma, lung symptoms were not included in the analyses. The design of the study was a retrospective analysis using multiple regression to control for confounding variables. Microsoft Excel Version 14 Analysis ToolPak 32 was used to analyze data.
Results
When comparing smoking welders, and controlling for age and percentage of time using a respirator, years welding was a statistically significant predictor of PFT (p = .04; Figure 1). When comparing nonsmoker welders and controlling for years welding and percentage of time using a respirator, age was a statistically significant predictor of PFT (p = .03; Figure 2). Thus, smoking and welding fume exposures had a synergistic effect on pulmonary decline among smoking welders. Among nonsmoking welders, age and welding fume exposure affected pulmonary decline. Use of a respirator was not a statistically significant factor for either group. When comparing smokers to nonsmokers, PFT showed a larger decrease in smokers’ lung function compared to nonsmokers’ lung function.
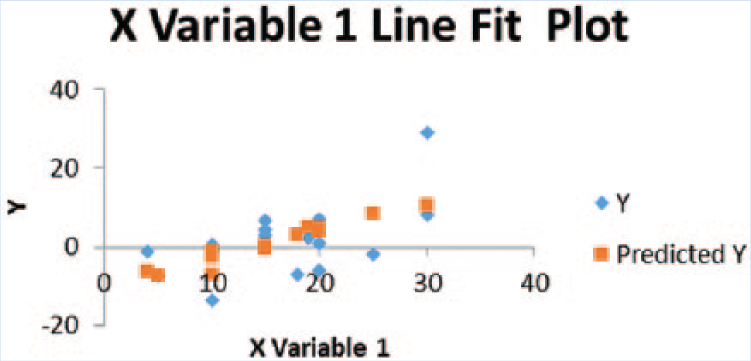
Results for smokers.
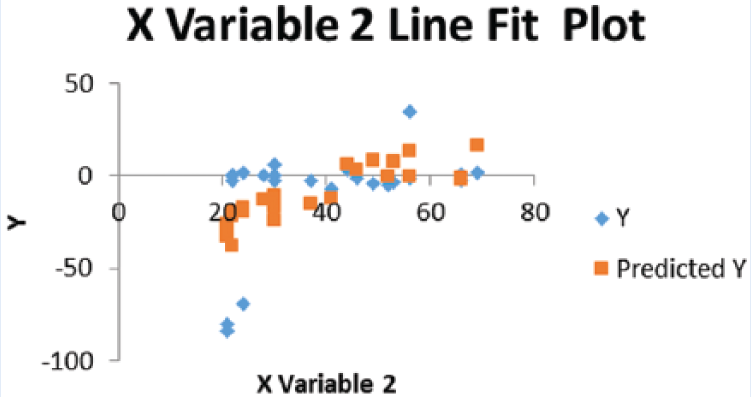
Results for nonsmokers.
Discussion
This study supports the hypothesis that smoking and welding fume exposure have a synergistic effect on pulmonary decline. Thus, smoking welders must be strongly encouraged to quit smoking and only nonsmokers should be employed as welders for this company.
The company provided the results of this study to employees and may modify company policies based on the findings. The researcher has strongly advised management to hire welders who do not smoke. However, it is essential for the company to reduce welding fume exposures to levels that will not affect pulmonary function using environmental, administrative, or worker (personal protective equipment) controls. For current welders who smoke, the company should provide access to smoking cessation programs. Examples might include support groups, health coaches, and smoking cessation medications. Not only does smoking cessation improve welder health but also overall employee health, more break time, and better workplace productivity. The occupational health clinic could provide health coaching services along with employee support and encouragement.
Study findings were comparable to current literature. First, study data supported previous findings that exposure to welding fumes increases pulmonary decline. In addition, data supported the synergistic effect of welding fume exposure and smoking. Although it is likely well known among welders that smoking is an unhealthy behavior, welders may be unaware of the increased risks of smoking and welding fume exposure; education on smoking and welding fume exposure is essential for this worker population. Although data were inconclusive regarding the use of respirators, personal protective equipment could prevent welding fume exposure. With this knowledge, companies should educate their employees regarding smoking cessation and the prevention of welding fume exposures.
Future research should include a larger sample from multiple companies in various geographical locations. In addition, it is unknown how welding fume exposures actually affect the pulmonary system as workers age. In terms of application to occupational health nursing practice, the findings should be incorporated into health promotion and disease prevention programs as well as programs on healthy aging.
Limitations
Several limitations of this study were identified. First, several participants quit smoking during their employment. Those individuals were considered smokers for the purposes of this study. Second, some participants did not estimate their use of respirators during welding. For data purposes, 50% was substituted for their respirator use. Third, years smoking, estimated time of respirator use, and years welding were figures reported by participants and were subject to participant recall. Age-related pulmonary decline was not measured in this study and could have impacted the statistical data. Fourth, little research has been conducted with women welders specifically. Finally, the small sample size used for this study was also a limitation.
Conclusion
Exposure to welding fumes poses a significant risk to employee health. Research illustrates a wide variety of pulmonary effects related to welding fume exposures (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012). Pulmonary function tests are useful tools for assessing pulmonary decline in welders. Previous studies on smoking and nonsmoking welders provided evidence linking exposure to welding fumes and lung function (Christensen et al., 2008; El-Zein et al., 2003; Ozdemir et al., 1995; Sharifian et al., 2011; Thaon et al., 2012; Vallières et al., 2012).
Although this study has several limitations, the researcher concluded that welding fume exposure and smoking negatively impacted the pulmonary systems of relatively young healthy workers. Welders should be strongly encouraged to quit smoking due to the risk of pulmonary decline. It could be concluded that even though respirator use was not a statistically significant predictor of lung function in this study, welders should practice safe respiratory measures by ensuring adequate ventilation and respirator use. Safe respiratory measures were found to be significant predictors of pulmonary function in other studies.
Terminology
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Laura L. Roach is an occupational health provider in Kingsport, TN, for Core Occupational Medicine. She is a member of AAOHN, Sigma Theta Tau, and Lincoln Memorial University Alpha Chi Honor Society.