
Abstract
The purpose of this study was to examine the prevalence of metabolic syndrome among faculty and staff who participated in a university wellness program. In addition, this study identified common correlates of metabolic syndrome in the participating employee population. Knowledge of behaviors and characteristics of individuals with metabolic syndrome is essential when developing health promotion strategies for them. Metabolic syndrome is unique in that it results from a clustering of risk factors that are difficult to address, and each additional risk factor increasingly affects health and well-being. A targeted, comprehensive approach is needed to counteract individual’s predisposition to metabolic syndrome. This research identified the association between employees’ metabolic risks and their demographic, physical, and psychosocial characteristics in an effort to determine metabolic syndrome prevalence, develop population-specific interventions, and decrease the risk of metabolic syndrome among workers.
Metabolic syndrome is a health care crisis of epidemic proportion in Western industrialized societies; it is imperative that metabolic syndrome be addressed to preserve the health and well-being of future generations (Falentin, 2010). Metabolic syndrome is defined as a condition of unknown cause that presents with symptoms of insulin resistance, obesity, hypertension, dyslipidemia, and systemic inflammation (Huether & McCance, 2008; Palaniappan, Wong, Shin, Fortmann, & Lauderdale, 2011). It is estimated that 34% of Americans above the age of 20 years have a combination of these risk factors and therefore metabolic syndrome (Ervin, 2009). Because metabolic syndrome is a major health concern in the United States, employers must address the growing number of workers with the syndrome. Occupational health nurses and health promotion professionals must identify individuals at risk for and with a diagnosis of metabolic syndrome and provide risk reduction strategies. Carter and Kelly (2013) defined the role occupational nurses play when screening employees for a variety of health issues and then providing education to empower employees to decrease disease risk factors.
First recognized in 1920 and then given a description in 1936 by Himsworth, metabolic syndrome has been categorized as insulin resistance. However, it was not named until Reaven referred to it as “Syndrome X” in 1988 (Rountree, 2010). Other terms used to describe the cluster of risk factors include “the insulin resistance syndrome” and the “deadly quartet” (Eckel, Grundy, & Zimmett, 2005). In 1998, the World Health Organization (WHO) recommended the development of a universal definition and changed the name from Syndrome X to metabolic syndrome (Alberti, Zimmet, & Shaw, 2006). Presently, metabolic syndrome is the term used to describe the clustering of risk factors that result in cardiovascular disease and diabetes (Falentin, 2010).
Individuals who have the constellation of risk factors known as metabolic syndrome have been shown to have higher morbidity and mortality rates from cardiovascular disease and Type 2 diabetes than those who do not have metabolic syndrome (Lewis, Rodbard, Fox, & Grandy, 2008). Cardiovascular disease and Type 2 diabetes are leading causes of death in the United States; approximately two thirds of adults in the United States have at least one major risk factor for cardiovascular disease (Berry et al., 2012; Lloyd-Jones et al., 2010), and one in four U.S. deaths is caused by cardiovascular disease (American Heart Association, 2014; Kochanek, Xu, Murphy, Miniño, & Kung, 2011).
In addition to higher morbidity and mortality rates, health care expenses associated with metabolic syndrome increase health care costs. Individuals with metabolic syndrome incur approximately US$2,000 more per year in health care expenses than individuals who do have a diagnosis of metabolic syndrome; these individuals have a 24% increase in health care costs with each additional risk factor. Individuals with metabolic syndrome have more inpatient hospitalizations, primary care visits, and pharmacy expenses (Boudreau et al., 2009). Although metabolic syndrome increases health care costs significantly, each individual metabolic syndrome component has been associated with higher costs, independent of other syndrome components (Nichols & Moler, 2011).
Working adults spend a significant portion of their day at work, making the workplace an ideal setting for screening and prevention programs (Cahalin et al., 2014). As part of their commitment to faculty and staff health and well-being, a large southeastern university established the Office of Health Promotion and Wellness (OHPW) in 2007, launching an employee health screening program in 2009. The overall goal of the university wellness program is to promote and advance the health and well-being of employees (Carter, Kelley, Alexander, & Holmes, 2011). Through the wellness program, employees are eligible for health screenings and health coaching sessions at no charge. As a result of health screenings, participants with abnormal findings, including the diagnosis of metabolic syndrome, are identified. These results provide health coaches and wellness professionals with opportunities to assist workers in setting health-related goals to reduce health-related risk factors. The screenings also identify the prevalence of metabolic syndrome correlates among participants. The American Heart Association (AHA)/National Heart, Lung, and Blood Institute (NHLBI) definition requires three of the following five risk factors be present for diagnosis of metabolic syndrome: waist circumference greater than or equal to 102 cm in men or 40 inches or greater than or equal to 88 cm in women or 35 inches; triglycerides greater than or equal to 150 mg/dL; high-density lipoprotein (HDL) cholesterol less than 40 mg/dL for men, less than 50 mg/dL for women, or prescribed cholesterol-lowering medication; systolic blood pressure greater than or equal to 130 mmHg, diastolic blood pressure greater than or equal to 85 mmHg or taking anti-hypertensive medication; and fasting glucose greater than or equal to 100 mg/dL or taking glucose-lowering medication. Employees with health risks, including metabolic syndrome, were identified, and differences in several parameters (e.g., age, blood pressure, and history of chronic diseases) were compared between individuals with and without metabolic syndrome. The findings of this study provide data to support the design of prevention programs for employees at risk of developing metabolic syndrome and those employees already suffering from metabolic syndrome.
Method
This study was approved by the university’s Institutional Review Board. Data were collected by OHPW staff. The sample for this study met the following inclusion criteria: (a) employee adult men and women 19 years of age or older who (b) attended a university wellness screening and (c) provided a blood sample. University employees participated in the 2009, 2010, or 2011 wellness screenings. After excluding those who did not meet the criteria, the total sample of participants completing the baseline measure was 1,156 employees.
Data Collection
All employees were eligible to be screened at no cost. The employees were provided with an informed consent form describing the use of nonidentifiable data for research purposes. Employees registered, read, and signed the informed consent form, and completed the health screening forms. The two-part university health screening and assessment instrument included a biometric screening score sheet completed by both the participant and the health coach who recorded the biometric measurements and a self-reported health profile completed by the participant. After completion of applicable paperwork, biometric screenings (i.e., height, weight, body mass index [BMI], waist circumference, and blood pressure measurements) were completed, and the results entered on the participants’ score sheets.
Fasting laboratory values were measured using the finger stick method. Triglycerides, total cholesterol, low-density lipoprotein cholesterol, HDL cholesterol, and glucose levels were all tested. Additional recorded data included the use of blood pressure, lipid-lowering, and glucose-lowering medications. A multiple-item survey was completed to assess each employee’s self-reported health profile. Individuals rated their overall physical health, family history of disease, smoking history, physical activity, education, income, comorbid conditions, and sleep in their health profiles. These data collection tools were adapted from the Centers for Disease Control and Prevention (CDC; 2010), Healthier Worksite Initiative guidelines.
Data Analysis
Data from employees who voluntarily completed an annual university wellness screening and met the inclusion criteria were analyzed. Based on the screening results, employees with metabolic syndrome, as defined by the AHA/NHLBI, were identified. The AHA/NHLBI definition requires three of the following five risk factors for diagnosis of metabolic syndrome: waist circumference greater than or equal to 102 cm in men or 40 inches or greater than or equal to 88 cm in women or 35 inches; triglycerides greater than or equal to 150 mg/dL; HDL cholesterol less than 40 mg/dL for men, less than 50 mg/dL for women, or taking cholesterol medication; systolic blood pressure greater than or equal to 130 mmHg, diastolic blood pressure greater than or equal to 85 mmHg or taking anti-hypertension medication; and fasting glucose greater than or equal to 100 mg/dL or taking glucose-lowering medication. Descriptive statistics, t test, and stepwise regression were used to examine which independent variables were predictors of metabolic syndrome.
Results
The sample included a total of 1,156 individuals: 353 men and 803 women. The average age of the individuals was 43 years, and the study sample was comprised of more White (73.90%) than any other ethnicity. Of the total 1,156 employees, 18% were faculty, 75% were staff, and 7% were student workers, retired faculty, or classified as “on leave.” Overall, 37%, or 427 employees, of the 1,156 employees had metabolic syndrome, 272 females and 155 males (see Table 1). Of the total 1,156 employees, 54% had a waist circumference exceeding the metabolic syndrome threshold. The second most common risk factor was low HDL cholesterol levels. Forty-six percent of the screened employees had lower than recommended HDL cholesterol. Twenty-four percent of employees had two risk factors for metabolic syndrome. The lowest percentage of employees had all five metabolic syndrome risk factors with 4.3% falling in this category (Figures 1 and 2).
The Presence or Absence of Metabolic Syndrome by Sex, Race, Education, and Family History

Note. HS = high school.
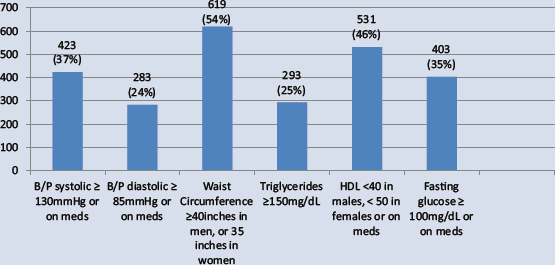
Metabolic syndrome risk factor prevalence for all employees.
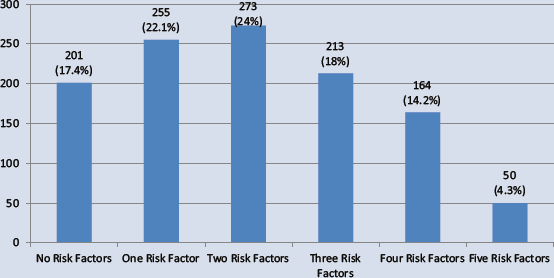
Breakdown of risk factor clustering for all employees.
Self-Perception of Health
Self-perception of health was measured on a 0 to 3 scale with 0 as poor and 3 as excellent. Among employees who had metabolic syndrome, only 9.84% described their overall physical health status as excellent and 55.5% described their overall physical health as good. The remaining employees with metabolic syndrome rated their overall physical health as fair (24.59%) or poor (3.28%). The remaining 6.79% did not answer the question regarding overall physical health status.
Overall perception of physical health was negatively correlated with number of risk factors for metabolic syndrome (r = −.271, p < .001), demonstrating that more risk factors were associated with less positive perceptions of health. Those at risk (3-5 factors) for metabolic syndrome were separated and compared with those not at risk (0-2 factors). t test analysis revealed a significant difference between the groups, t(766) = 7.99, p < .001. The at-risk group (M = 1.77, SD = 0.677) had a significantly lower perception of physical health than the not-at-risk group (M = 2.10, SD = 0.612).
Smoking, Physical Activity, and Sleep
Next, the researchers investigated factors contributing to metabolic syndrome. Smoking was measured by smoking history (3 = never smoked, 2 = former smoker, 1 = still smoke), and a significant difference was present between smoking groups on the number of metabolic syndrome risk factors, F(5, 776) = 3.99, p = .019. A Tukey honest significant difference (HSD) post hoc test revealed a significant difference; those who used to smoke (M = 2.30, SD = 1.54) had more risk factors than those who had never smoked (M = 1.96, SD = 1.45). Number of cigarettes smoked was also collected; however, this measure was excluded as only 43 participants reported actively smoking.
Physical activity was also measured on a 0 (less than one 20-minute session per week) to 3 (four or more sessions per week) scale. Physical activity was found to be negatively correlated with the number of metabolic syndrome risk factors (r = −.194, p < .001), meaning that those who exercised more had fewer risk factors. An ANOVA using physical activity as the independent variable revealed a significant difference between groups, F(5, 1078) = 14.28, p < .001. A Tukey HSD post hoc test revealed that those who exercised most had significantly fewer risk factors than any other group.
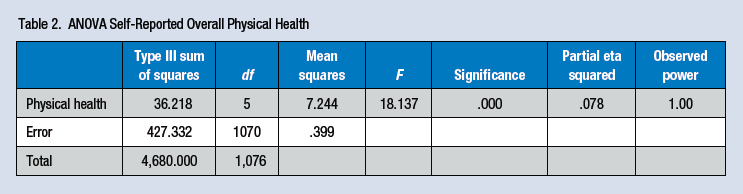
Number of sleep hours was measured on a 0 (6 hr or less) to 3 (9 hr or more) scale. Sleep was negatively correlated with the number of metabolic syndrome risk factors (r = −.085, p = .006), suggesting that more sleep was associated with fewer risk factors. Because too much sleep can be potentially negative, hours of sleep was used as an independent variable in a one-way ANOVA with metabolic syndrome risks as the dependent variable. Overall, a significant group difference, F(3, 1052) = 6.194, p < .001, was found; however, Tukey HSD post hoc testing revealed a curious finding. Those who slept 8 hr per day (M = 1.76, SD = 1.42) reported significantly fewer risk factors than any other group. Those participants who slept 9 hr or more per day had more risk factors than the 8-hr group (M = 2.52, SD = 1.39), and the 6-hr-or-less group had fewer risk factors than the 9-hr-or-more group but more risk factors than the 8 hr of sleep group (M = 2.22, SD = 1.40). This finding suggests that 8 hr of sleep is optimal for avoiding metabolic syndrome risk factors (Table 2).
ANOVA Self-Reported Overall Physical Health
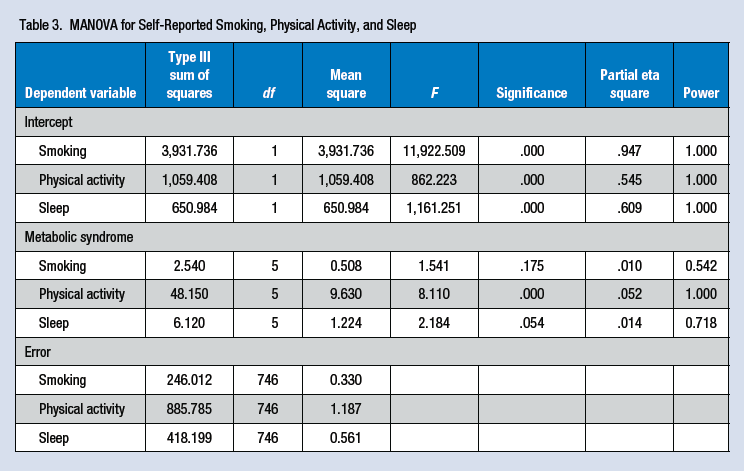
Finally, a multiple regression analysis was conducted to determine which variable(s) best predicted metabolic syndrome risk factors. Smoking habits remained nonsignificant, β = −.07, t(748) = −1.817, p = .07; however, physical activity, β = −.21, t(748) = −6.04, p < .001, rp = −.22, and sleep, β = −.11, t(748) = −2.96, p = .03, rp = −.11, both remained significant, suggesting that both explain a unique proportion of the variance (R2adj= .06) with physical activity being the strongest predictor (Table 3).
MANOVA for Self-Reported Smoking, Physical Activity, and Sleep
Discussion
The prevalence of metabolic syndrome has been termed a health care crisis. This study demonstrated a high prevalence of metabolic syndrome among a population of employees at a large southeastern university. Thirty-seven percent of the employee sample had at least three of the five criteria for metabolic syndrome, higher than the national average of 34% (Ervin, 2009). Comparing these two samples via t test revealed that they were marginally significantly different from each other, t(4577) = 1.85, p = .06, suggesting that the prevalence of metabolic syndrome for this population is most likely statistically higher than the national average.
Of the individuals in this study who were classified as having metabolic syndrome, 28% rated their health as fair or poor compared with only 12% of participants without metabolic syndrome. Nationally, 17% of the population rate their health as fair or poor (CDC, 2011). Quality of life and self-perception of health are essential to determining health status; individuals’ health cannot adequately be assessed without determining how they rate their overall health because self-assessment has been shown to be a representation of health status and mortality and an indicator of future health care use (Idler & Benyamini, 1997; Organisation for Economic Co-Operation and Development [OECD], 2011). Findings from this research improve occupational health nurses’ understanding of the connection between metabolic syndrome and perceived overall health status. More research is warranted to better understand overall health perception and determine whether low perception of health deters individuals from acting to improve their health or whether low perceived health is specifically related to metabolic syndrome risks.
Another significant finding of this research was the need for individuals to participate in physical activity to avoid metabolic syndrome. Physically active employees are at less risk of developing metabolic syndrome. Increasing physical activity and decreasing sedentary behaviors such as nonwork computer and television time can positively affect metabolic syndrome risk (Ford, Kohl, Mokdad, & Ajani, 2005).
In the present study, more sleep was also related to fewer metabolic syndrome risks. Previous research by Santos, Ebrahim, and Barros (2007) indicated that individuals need an average of 7 to 8 hr of sleep to decrease their risk for metabolic syndrome. For this study of participants with metabolic syndrome, 24% slept 6 hr or less per night, whereas, nationally, 35% of Americans report not enough sleep (CDC, 2010). Sleep is a modifiable variable that is often overlooked but can be targeted successfully (Strine & Chapman, 2005).
Study Limitations
This cross-sectional study did not provide a historical perspective on this population and thus does not allow inferences regarding causality on the associations found. The screening initiative in the present study was available to all employees at the university, but the sample included only those employees who voluntarily participated in the employee wellness program. Therefore, the study sample may or may not be representative of all employees of the organization or the general working public. Individuals who did not participate may have a higher risk of metabolic syndrome, or healthier employees may not be represented in this sample. Of the 1,156 study employees, 37% (427) had at least three of five risk factors for metabolic syndrome indicating a diagnosis of metabolic syndrome and suggesting that this sample had a higher rate of metabolic syndrome than the national average. The higher prevalence of metabolic syndrome in this sample may be attributed to geographic location. The southeastern United States has higher rates of hypertension, diabetes, and obesity than the rest of the country, which all contribute to metabolic syndrome (Ervin, 2009).
Implications for Occupational Health Nurses
This research has several implications for researchers and clinicians with an interest in improving the overall health of individuals. Metabolic syndrome has been shown to increase the incidence of cardiovascular disease and diabetes (Lewis et al., 2008). Decreasing just one risk factor associated with metabolic syndrome can increase life expectancy, decrease the risk of developing chronic health conditions, and improve overall well-being (Klein, Klein, & Lee, 2002). Workplace health promotion programs can play a significant role in reducing health risks and creating an environment of wellness for all employees.
To improve workplace health, the behaviors and characteristics of employees with metabolic syndrome should be explored when developing health promotion strategies that target decreasing metabolic syndrome risk factors. Metabolic syndrome is unique in that it is a clustering of risk factors that can be difficult to address; each addition of a risk factor increasingly affects health and well-being. A targeted, comprehensive approach is warranted to address individuals’ predisposition to metabolic syndrome.
The workplace is often an ideal setting to promote long-term behavior change for the prevention of chronic diseases for which metabolic syndrome is a precursor. Occupational health nurses can design and deliver effective interventions, including exercise and healthy eating programs that target healthy lifestyles, particularly to high-risk employees. As rates of metabolic syndrome increase in the United States, preventing metabolic syndrome should be a priority to improve the overall health of the working population, with occupational health nurses playing a vital role in health promotion and disease prevention.
Applying Research to Practice
Worksite wellness programs should screen for the cluster of risk factors known as metabolic syndrome. Identifying high-risk employees is essential prior to implementing targeted health promotion initiatives. In addition, noninvasive assessments of employees’ self-perception of health should not be discounted. This assessment is an informative measurement of overall employee health.
Footnotes
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rebecca Kelly is a consultant for O’Neal Industries, employed by Element Health, and has received payment for lectures from the Midwest Business Group on Health and the American Psychological Association.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Paige Johnson, PhD, RN is an Assistant Professor at the Capstone College of Nursing at The University of Alabama. Dr. Johnson has graduate degrees in nursing and health education. Dr. Johnson currently teaches in the community health nursing course where she works closely with senior nursing students teaching them the importance of health education and promotion in nursing.
Lori Turner is a Registered Dietitian and a Professor of Health Science at The University of Alabama. She has graduate degrees in nutrition and health education. She has authored over 75 articles in national, peer-reviewed journals in disease prevention and health promotion.
Melondie Carter, PhD, RN is the Assistant Dean of Undergraduate Programs and a professor in the Capstone College of Nursing. Dr. Carter served as the Assistant Director of the Office of Health Promotion and Wellness and co-led the WellBAMA program. Dr. Carter continues in the role of Assistant Director of WellBAMA research.
Rebecca Kelly, PhD, RD is Assistant Professor and Director of Health Enhancement Planning, The University of Alabama, Tuscaloosa AL. She has over 20 years of hands-on experience in health and wellness program strategy, communication campaigns, innovative program development, and program evaluation.
Patrick J. Ewell is an experimental psychologist specializing in statistics and research methodology. He is from Delaware and is beginning a position at Kenyon College as a visiting assistant professor.