
Abstract
Background: Worksite wellness programs that target individual employees, rather than worksites, have demonstrated limited long-term success. The purpose of this overview was to describe the theoretical basis for implementing an effective worksite wellness initiative, WorkWell Kansas (WorkWell KS). WorkWell KS is not a traditional worksite wellness initiative, as its goal is to create healthy worksites, rather than target workers. Methods: The WorkWell KS Strategic Framework is based on academic research that identified successful worksite wellness elements that produce sustainably healthy worksites. The curricula were built around the 3-4-80: three modifiable behaviors (tobacco use, poor access to nutritious foods and beverages, and physical inactivity) contribute to at least four chronic diseases (heart disease, type II diabetes, lung disease, and some cancers), which in turn contribute to approximately 80% of the premature deaths in the United States. Findings: To properly address these modifiable behaviors, the WorkWell KS Strategic Framework was developed to guide worksites to first build a solid worksite wellness foundation, which consists of five elements: the wellness committee, exercising leadership, communications, incentives, and data. Once built, worksites are then encouraged to employ a socio-ecological approach to developing a comprehensive, multi-strategy (information, program, benefit design, policy, and environment) intervention, focusing on one health behavior at a time. Conclusions/Application to Practice: The goal of WorkWell KS was to create healthy worksites, which creates environments for employees to practice these healthy behaviors. Worksite wellness committees, occupational health professionals, and others interested in altering health behaviors at worksites have an opportunity to reframe their approach using this framework.
Keywords
Background
WorkWell Kansas (WorkWell KS) is an initiative that partners with employers to create healthy worksites for employees, customers, clients, patients, and/or students. WorkWell KS is not a traditional worksite wellness initiative, which tends to target individual employees (Ablah et al., 2019). Rather, WorkWell KS uses evidence-based curricula designed to create worksite conditions where the healthy behavior is easy for employees to practice and thus becomes the default behavior.
The WorkWell KS Strategic Framework (Figure 1) and curricula were built around the 3-4-80: three modifiable behaviors (tobacco use, poor access to nutritious foods and beverages, and physical inactivity) contribute to at least four chronic diseases (heart disease, type II diabetes, lung disease, and some cancers), which in turn contribute to approximately 80% of the premature deaths in the United States (Katz et al., 2017; Mokdad et al., 2004; Yach et al., 2004). While extracting best and most promising practices from the academic literature for tobacco, nutrition, physical inactivity, and worksite wellness generally, it became clear that a framework was needed to organize the constructs associated with building an effective worksite wellness initiative. Before addressing any of the health behaviors, worksites need to first build a solid “worksite wellness foundation,” upon which initiatives that modify tobacco, nutrition, and/or physical inactivity can be implemented and sustained.
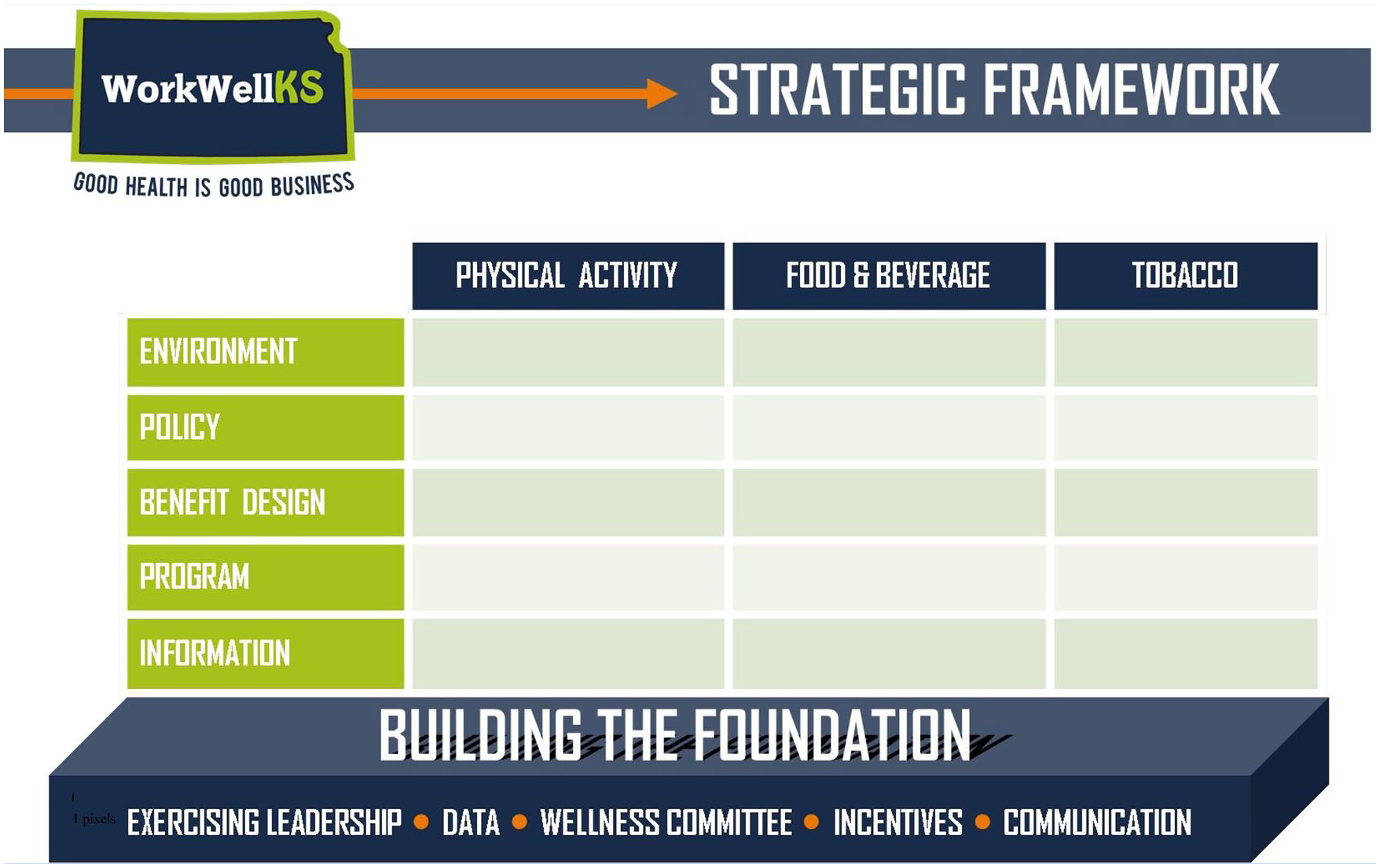
The WorkWell KS Strategic Framework.
As the goal of WorkWell KS was to create healthy worksites, the predominant focus of the work was the worksite rather than the employee. This article describes the theoretical basis for how effective worksite wellness interventions can be developed using the WorkWell KS Strategic Framework.
Build the Worksite Wellness Foundation
The purpose of an organization building the worksite wellness foundation is to develop a solid infrastructure that allows for the integration of health at the worksite. Without this, worksite wellness is disconnected from the “real” work of the worksite. For instance, the wellness committee might provide newsletters that inform employees about the health risks associated with sugar consumption, while concurrently, managers offer cakes, cookies, and doughnuts to employees to recognize birthdays, accomplishments, and non-events. In other words, the wellness initiative must be incorporated into the functioning of the worksite. The foundation serves this purpose and is composed of five elements: the wellness committee, exercising leadership, communications, incentives, and data.
The Wellness Committee
Unlike a task force designed to address a single goal or project, worksite wellness is extremely complex, and it typically has no defined end; therefore, it is best to establish a committee structure that remains active and in place over time. A worksite may adopt one of many possible names for the group tasked with these duties and may want to relate it to associated outcomes or attributes of interest, such as productivity, performance, or safety. For the purposes of this article, this group will be referred to as the wellness committee.
It is a best practice for the wellness committee to have an on-site coordinator, chair, or facilitator (Terry et al., 2008), and to have worksite wellness as a job responsibility of those serving on the committee (Berry et al., 2010; Sorensen et al., 2004). As the work of the wellness committee needs to be integrated into the infrastructure of the worksite, there must be accountability for all wellness committee members to perform their work adequately. Each member of the wellness committee has a specific and defined role (e.g., facilitator, secretary, liaison to executive). A process needs to be in place that ensures duties are performed satisfactorily. Linking committee work to job responsibilities ensures that these performance criteria can be measured and evaluated.
The wellness committee needs to reflect the worksite; members need to represent different departments and levels of management, various shifts and locations, levels of interest in worksite wellness, in addition to gender, age, and race/ethnicity (Centers for Disease Control and Prevention, 2012; Goetzel et al., 2007; HERO Health, 2016). To achieve this level of representation, wellness committee members need to be appointed to serve on the committee as a component of their job responsibilities and based on the specific skills required. This is different from simply asking volunteers to participate. For example, when volunteers are requested, those who volunteer tend to be interested in worksite wellness; this often creates an unnecessary chasm between the perceived “healthy” versus the “unhealthy” employees at the worksite. Moreover, by appointing employees who are representative of the worksite to the wellness committee, the work becomes more integral to the vision of the worksite and reflective of the employee population.
The wellness committee needs to be guided by a vision statement that more fully directs their work. The vision statement can be linked to, or independent from, the worksite’s vision, mission, and/or objectives (Goetzel et al., 2007; O’Donnel, 1997; Seaverson et al., 2009). Moreover, the wellness committee needs to be recognized as an essential function of the worksite by the executive or administrative team and upper management (Goetzel et al., 2007); having their support and commitment is critical to the success of the initiative (Centers for Disease Control and Prevention, 2012; HERO Health, 2016; Wierenga et al., 2013). The wellness committee also needs executive buy-in and broad support from middle management to encourage employee participation and involvement (McLellan et al., 2012).
Although not required, it is a best practice for the wellness committee to be responsible for an operating budget (Centers for Disease Control and Prevention, 2012) and to have access to aggregate-level data to inform the direction of the wellness initiative. Such data might include employee needs and interests regarding physical activity, nutrition, and tobacco use, as well as human productivity, absenteeism, and/or morale measures.
Exercise Leadership
One of the key components frequently cited in worksite wellness literature is the importance of having “leadership” engagement and buy-in (Centers for Disease Control and Prevention, 2012; Goetzel et al., 2007; HERO Health, 2016; O’Donnel, 1997). The WorkWell KS Strategic Framework includes a leadership component, but its aim aligns with the Kansas Leadership Center’s (KLC) definition of exercising leadership, mobilizing others to make progress on (difficult) adaptive challenges (Heifetz & Linskey, 2002). Instead of solely relying on authority figures to lead the way, the concept of exercising leadership places responsibility in the hands of everyone, at every level of the organization, and encourages those at all levels to engage in making difficult culture changes (O’Malley & Cebula, 2015).
As the KLC (2013) suggests, “leadership isn’t a role, or position, or a fancy title on your business card—it’s a muscle that you can train and develop. Anyone can lead. Anytime. Anyplace.” Consider the need to build the leadership capacity of individuals on the wellness committee. Regardless of their role, whether they have management authority or not, intervening to shift the status quo and create a healthier workplace requires wellness committee members to exercise leadership. This type of leadership is fundamental. The wellness committee, executives, and others who are attempting to disrupt the status quo may feel pushback, which in turn may feel uncomfortable and risky. Therefore, they need to learn the behaviors and skills, such as “leadership competencies” as KLC calls them, that help mitigate the risk involved with disrupting the status quo. Some of these leadership competencies include “raising the heat,” in other words, bringing enough attention to the cause to initiate change, or engaging unusual or otherwise silent voices.
Another skill in exercising leadership is developing faction maps and using them to engage stakeholders. Faction mapping can be utilized to successfully identify and engage stakeholders for change (Aligica, 2006), which is an essential part of a worksite wellness initiative (Goetzel & Ozminkowski, 2008; HERO Health, 2016; McLellan et al., 2012). Faction or stakeholder mapping allows change agents, such as wellness committee members and other interested parties, to explore who is critical to the success of the initiative, who are potential decision makers and stakeholders, what are stakeholders’ concerns and interests (e.g., improved productivity, lowering health care costs, being healthy enough to play with grandkids), how a worksite wellness initiative might align with those concerns, and how to meaningfully engage each of these stakeholders, including executives and administrators.
These leadership behaviors and skills are needed to overcome resistance, listen to those resisting, and engage stakeholders to become supporters of the desired change. Those exercising leadership are changing a system, and systems do not easily change. These leadership competencies are designed to achieve sustained culture change.
Communication
In the foundation of the WorkWell KS Strategic Framework, before information or campaigns are shared about a specific health behavior, it is important to establish health communications capacity among the wellness committee. This involves determining whether the wellness committee is ready to begin delivering specific messages not related to a specific health topic (e.g., tobacco). For example, when the wellness committee is ready to announce their presence to the worksite, the best primary message is tailored to match a desire of the target population. For some, sharing the wellness committee’s vision, “[Worksite] will have healthy and productive employees” might resonate with employees. For a worksite and employees motivated by the need to lower health care costs, a message of “We are working to reduce your health care premiums” might resonate best. Occasionally, worksite wellness committees will enact a policy and/or environmental change before announcing their presence to the entire worksite.
Establishing health-related communications capacity also involves the wellness committee identifying the most accessed communication channels (e.g., newsletters, posters, intranet). For example, delivering a broad message through multiple communication delivery channels, such as face to face, communication from the executive team, intranet announcement, or paycheck inserts, is more likely to reach a more diverse target audience (Seaverson et al., 2009; Terry et al., 2008). Research suggests that important messages need to come from at least four different delivery channels (Seaverson et al., 2009). Employees often regard messages from authority figures as more important than messages from other sources, signaling that the content is in line with the values and practices of the worksite (McLellan et al., 2012). Therefore, the wellness committee must share the broad message with the worksite’s authority figures such as executives, human resources, a board of directors, or middle managers who are then, in turn, asked to deliver the message to the target population.
Incentives
Incentives can be used as rewards to influence the health behavior decision-making process of employees, fuel participation, and/or improve adherence (Goetzel & Ozminkowski, 2008; Mattke et al., 2013; Pronk, 2004). Incentives traditionally include trinkets, such as water bottles and t-shirts; however, these are considered least effective in encouraging participation (Goetzel et al., 2007). Some incentives are more meaningful to employees and are more influential than others, such as health benefit plan design or health savings account (HSA) contributions (Goetzel et al., 2007; Mattke et al., 2013). These incentives generally have a higher value and are more fully integrated into the worksite. In the foundation, worksites may benefit from having a list of potential financial (HSA contribution, reimburse employees who bicycle to work, premium reductions, paid time off) and non-financial (recognition at a ceremony, jeans day) incentives of interest to their employees.
After the foundation has been established, the wellness committee needs to consider incentives that (a) reinforce the intended behavior (HERO Health, 2016), (b) reward behavior rather than outcomes over a sustained period of time, (c) offer an intermittent reward structure, and (d) are worksite rather than individual-level incentives (e.g., installing trail markers vs. providing pedometers). These incentives are thought to affect more populations and generate a greater return on investment.
Data
The fifth element of the foundation in the WorkWell KS Framework is data. It is important for the wellness committee to have access to data, as its members will be responsible for the development, implementation, and evaluation of the intervention. Data can be used to first understand the scope of the problem(s) and then, in a follow-up, determine whether the initiative’s interventions are effective. However, the way data have been traditionally used to inform worksite wellness initiatives may not maximize funds or time.
Traditionally, data have been derived from a variety of sources, including health risk assessments (HRAs), biometrics, aggregate employee health, and claims (Chenoweth, 2011). Gathering some or all of these data can help wellness committees determine a starting point or baseline. However, these data are not necessary. For instance, consider HRAs and biometric data, which are traditional worksite wellness measurement best practices (Kaiser Family Foundation and Health Research & Educational Trust, 2015; Mattke et al., 2013). Health risk assessments and biometric data target the employee and rely on two assumptions: (a) employees care enough about/are motivated by their results that they will make behavior changes, and (b) the results will inform the direction of the worksite wellness initiative.
Due to the sensitivity of biometric data, employees are often concerned that their employers will have access to their individual health data (Hill-Mey et al., 2013), despite the employer’s responsibility to maintain their employees’ privacy and confidentiality through the Health Insurance Portability and Accountability Act of 1996 (HIPAA, 1996) and Genetic Information Nondiscrimination Act of 2008 (GINA, 2008). This focus on biometric data may interfere with the initiative by calling motives and trust into question rather than focusing on improving health, morale, or productivity.
Moreover, worksite interventions focus on macro-level, population-based changes, so why would we collect micro-level biometric data to demonstrate improvements? Consider instead administering a more cost-effective and perhaps more useful assessment. A behavior-based needs assessment based on the 3-4-80, can engage employees and enable the worksite to target interventions to the identified population, which can increase participation (Rongen et al., 2014). Everyone benefits from the worksite improving their tobacco, physical activity/sedentary, and food and beverage environment.
Socio-Ecological Approach
Taking a socio-ecological approach (Sallis et al., 2008) and addressing health behaviors in a comprehensive manner means using multiple strategies: information, program, benefit design, policy, and environment. The strategies are listed on the y-axis of the Strategic Framework.
Providing information is the most basic approach to health promotion. It can increase knowledge, but knowledge is not strongly linked to behavior change (Sallis et al., 2008). Providing employees with a pamphlet on the benefits of physical activity is not likely going to promote activity. Program is the second most basic strategy. It can promote behavioral change, but this is generally temporary (Sallis et al., 2008). A physical activity program might be a step challenge to increase physical activity among employees. Those who opt-in and complete the program might have increased their activity while the program is in effect, but upon completion, their inactive behavior is likely to revert (Behrens et al., 2007; Green et al., 2007). The next level is benefit design. Benefits can formally institutionalize incentives, such as providing free gym memberships. Designing benefits requires a substantial commitment and a thorough wellness initiative, and the payoffs can substantially influence health care claims (Baicker et al., 2010). Policy changes can become integral components of the worksite. They codify what behaviors are considered appropriate, they have lasting effects, and policies are enforced at an institutional level. Policies that allow employees to walk on the clock or use flex-time to be physically active can increase physical activity (Bale et al., 2014; Grzywacz et al., 2007; Lucove et al., 2007). Environmental changes, including physical changes to the worksite such as offering adjustable-height desks or marked walking routes in and outside of the worksite, surpass all of the other changes because people tend to adapt to our environments (Golaszewski et al., 2003). Changing the physical space can be an essential strategy for a wellness initiative and can sustain behavior changes, as employees do not need to self-select into a program (Glanz & Mullis, 1988). These effects can be especially impactful when combined with policy (Brownson et al., 2006; Matson-Koffman et al., 2005; Sallis et al., 2008). Although all strategies can be important, the strategies at the top of the framework are likely more effective, more strategic, and more sustainable (Sallis et al., 2008). However, when multiple interventions in each strategy (such as information, program, benefit design, policy, and environment) are directed at one health behavior (e.g., physical activity), the initiative can have a larger and more sustainable impact (Goetzel & Ozminkowski, 2008; Sallis et al., 2008).
Address One Behavior Comprehensively
Once a solid worksite wellness foundation has been developed, a comprehensive and sustained worksite wellness intervention can begin, one health behavior at a time. Focusing on one health priority at a time and developing a comprehensive, research-informed, multi-strategy intervention will help the worksite achieve its wellness goals and have the most impact (Goetzel et al., 2014; HERO Health, 2016; Sallis et al., 2008; Sorensen et al., 2004; Terry et al., 2008).
Traditionally, worksites pursuing worksite wellness address a variety of health topics and are typically reliant upon the lower strategy levels (e.g., providing information and programs). This disjointed approach spreads wellness efforts too thinly and diminishes progress for any single health behavior. Consider also the faction mapping process; would all of the stakeholders who need to be engaged to address physical inactivity be the same stakeholders who need to be engaged to address tobacco at the worksite?
Conclusion
The WorkWell KS Strategic Framework uses research to inform an evidence-based, worksite wellness initiative. The purpose of WorkWell KS was to create a framework for worksite wellness committees and occupational health nurses to develop healthy worksites, where the healthy behavior is the easiest behavior. The WorkWell KS Strategic Framework proposes that worksites interested in health, productivity, or reduced health care costs need to first build a solid worksite wellness foundation (consisting of a wellness committee, exercising leadership, communications, incentives, and data). Once the foundation is solid, worksites are able to focus on one health behavior at a time (e.g., physical activity, tobacco, foods and beverages), developing comprehensive interventions with multiple strategies (e.g., information, program, benefit design, policy, environment).
Application to Occupational Health Nursing Practice
Occupational health nurses and occupational health professionals in worksites across the United States are recognizing the importance of addressing worksite wellness to improve workers’ health and/or the worksite’s profit. Existing worksite wellness interventions offer an approach that addresses many health topics at a time and focuses primarily on the individual employee (i.e., offering biometric screenings). Occupational health practitioners have long proven the feasibility (and cost savings) of targeting populations, rather than individuals, in improving health outcomes. The WorkWell KS Strategic Framework addresses behavioral change at a worksite level and provides guidance to worksites to develop a sustainable worksite wellness initiative. This framework guides worksites to first focus their worksite wellness “foundation” efforts that will sustain the initiative in the long run. Once the foundation is established, the framework instructs worksite wellness committees and occupational health professionals to address a single health topic with multiple, comprehensive strategies. Once one health topic has been fully addressed, worksites are encouraged to move to another health topic.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Kansas Health Foundation.
Author Biographies
Elizabeth Ablah - Dr. Elizabeth Ablah is an associate professor in the Department of Population Health at the University of Kansas School of Medicine - Wichita. Dr. Ablah received a Bachelor of Arts with distinction from St. Olaf College, a Master of Public Health from the University of Kansas School of Medicine - Wichita, and a Master and Doctorate in Community Psychology from Wichita State University. Her research interests include community-based participatory research, physical activity and healthy foods, the built environment, health impact assessments, and worksite wellness.
Elizabeth Wilcox - Elizabeth Wilcox received a Bachelor of Science from Wichita State University and a Master of Public Health from Kansas State University. She has experience in community health and development, worksite wellness, and physical activity promotion.
Emily Umansky – Emily Umansky received a Bachelor of Arts in Psychology from Lewis and Clark College and a Master of Public Health from the University of Kansas School of Medicine - Wichita. Her research interests include developing and assessing strategies that effectively encourage the adoption of healthy behaviors.
Allison Honn - Allison Honn is a program manager in the Department of Population Health at the University of Kansas School of Medicine - Wichita. She received a Bachelor of Arts from Wichita State University and a Master of Business Administration from Tabor College. She has broad experience in marketing, market research, and project management. Her focus is on worksite wellness under the WorkWell KS initiative helping to create healthy worksites across Kansas.
Ed O’Malley - Ed O’Malley is the founding President and Chief Executive Officer of the Kansas Leadership Center. Formed in 2007, the center now works with over 2000 Kansans each year in extensive leadership development trainings. Prior to forming KLC, Ed served two terms in the Kansas legislature and was also an aide to Kansas Governor Bill Graves. Ed is the co-author of three books related to the work and mission of the KLC: For the Common Good: Redefining Civic Leadership, Your Leadership Edge: Lead Anytime, Anywhere and What’s Right With Kansas: Everyday Citizens Transforming Their State.
Jeff Usher - Mr. Usher’s responsibilities include working with the Kansas Health Foundation staff to develop program initiatives. He also provides technical assistance to applicants and grantees, reviews proposals and monitors existing grants. Mr. Usher serves as senior program officer for the Foundation’s leadership, healthy behaviors and growing community philanthropy Initiatives. In the last twenty-one years, he has supervised a portfolio of nearly 800 approved grants totaling more than $170 million to support the mission of improving the health of Kansans.