
Abstract
This study investigated addictive substance use by French medical students. A cross-sectional survey was distributed to 255 participants randomly selected from 1,021 second- to sixth-year medical students. Questionnaires were self-administered and included questions on sociodemographic characteristics, mental health, and alcohol (The Alcohol Use Disorders Identification Test [AUDIT test]), tobacco (Fagerstrom test), and illegal substance consumption (Cannabis Abuse Screening Test [CAST test]). The AUDIT scores indicated that 11% of the study participants were at risk for addiction and 21% were high-risk users. Tobacco dependence was strong or very strong for 12% of the participants. The CAST score showed that 5% of cannabis users needed health care services. Cannabis users were also more likely than non-users to fail their medical school examinations (89% vs. 39%, p < .01). One quarter of medical student participants (n = 41) had used other illegal drugs, and 10% of study participants had considered committing suicide during the previous 12 months. Psychoactive substance consumption by French medical students requires preventive measures, screening, and health care services.
Excessive alcohol consumption and binge drinking among adolescents and young adults have been recognized as significant risk behaviors, increasing the likelihood of health problems, drunk driving, aggression, unsafe sexual activity, and accidents (Maddock, Laforge, Rossi, & O’Hare, 2001; Wechsler et al., 2002). Heavy drinking during adolescence and young adulthood is predictive of future alcohol-related problems and academic failure in certain groups (Jennison, 2004).
Heavy drinking is highly prevalent among college and university students (Hingson, Heeren, Winter, & Wechsler, 2005), including medical (Granville-Chapman, Yu, & White, 2001) and nursing students (Oliveira & Furegato, 2008). For many health professions students, alcohol consumption may be a way of coping with the stress of challenging curricula and clinical education (Henriquéz & Carvalho, 2008; Kjøbli et al., 2004). The known interaction between binge drinking and other drug-related behaviors such as cannabis and cigarette smoking is also prevalent among medical students (Newbury-Birch, Walshaw, & Kamali, 2001).
Cannabis use has been associated with a range of adverse effects (e.g., impaired attention, memory and psychomotor performance, traffic accidents, and depression) and social problems (e.g., low educational attainment; Hall & Solowij, 1998). Cannabis can also reduce symptoms of depression, psychopathology, and psychosocial distress (Delile, 2005; Ries, 1993). The harmful effects of substance use by health professions students are well described (Baldwin, Bartek, Scott, Davis-Hall, & DeSimone, 2009; Baldwin et al., 2008; Baldwin et al., 2006; Baldwin, Scott, DeSimone, Forrester, & Fankhauser, 2011). Consumption may be the cause or consequence of individual student challenges and academic success.
In addition, physicians, particularly young physicians, are susceptible to psychological distress and addictions (Brooks, Chalder, & Gerada, 2011). Health professions students experience higher rates of depression, burnout, and mental illness than the general population, with deteriorating mental health during the course of their educational programs (Deasy, Coughlan, Pironom, Jourdan, & Mcnamara, 2014; Dyrbye et al., 2010; Dyrbye, Thomas, & Shanafelt, 2006; Givens & Tjia, 2002; Goebert et al., 2009). Medical students report higher rates of burnout (Dyrbye et al., 2008) and depressive symptoms associated with suicidal ideation (Dahlin, Joneborg, & Runeson, 2005; Tyssen, Vaglum, Grønvold, & Ekeberg, 2001), suicide (Hays, Cheever, & Patel, 1996), and impaired quality of life than age-matched populations. However, it is well documented that physicians are as healthy, or even healthier, than other comparable population groups (Frank & Segura, 2009). A medical career is more frequently associated with good health than with poor health (Aasland, Hem, Haldorsen, & Ekeberg, 2011).
It could be assumed that medical students have ready access to health care in view of their studies and role in the health care system. Unfortunately, the literature does not confirm this assumption (Chew-Graham, Rogers, & Yassin, 2003; Rosenthal & Okie, 2005; Tjia, Givens, & Shea, 2005). Medical students engage in potentially harmful methods of coping, such as excessive alcohol consumption (Kjøbli et al., 2004). Strategies should therefore not only be repressive (i.e., zero tolerance for substance use or suspending and expelling students who transgress), but also provide a global preventive approach including harm minimization (e.g., school-based health promotion taking into account the assessment of the psychological, educational, economic, and social life of the students; Evans-Whipp et al., 2004). Although secondary schools commonly implement alcohol prevention policies to reduce alcohol misuse, the efficacy of these policies has only been rarely evaluated (Evans-Whipp, Plenty, Catalano, Herrenkohl, & Toumbourou, 2013).
Alcohol consumption in the World Health Organization (WHO) European regions is high (Rehm, Taylor, & Patra, 2006). Mortality due to diseases related to excessive alcohol consumption in the study university is significantly higher than that in other parts of France (Beck, Legleye, Le Nézet, & Spilka, 2005). A reduction in alcohol consumption, especially among young people, is one of the five regional health priorities. In France, the sale of alcohol and tobacco is prohibited to individuals less than 18 years of age. French law prohibits smoking in all public places and the possession of drugs, including cannabis, is prohibited and illegal.
Consumption of alcohol and other addictive substances by students is a major concern at the study university. To define the most appropriate prevention and health care strategies, the researchers asked medical students about their alcohol, smoking, and drug-related behaviors. The use of psychoactive substances raised questions about the ability of these students to succeed in medical school and meet their future professional responsibilities.
This study investigated addictive substance consumption by French medical students and possible associations between this consumption and personal and school-based characteristics in an attempt to identify patterns that could guide prevention policies and strategies.
Method
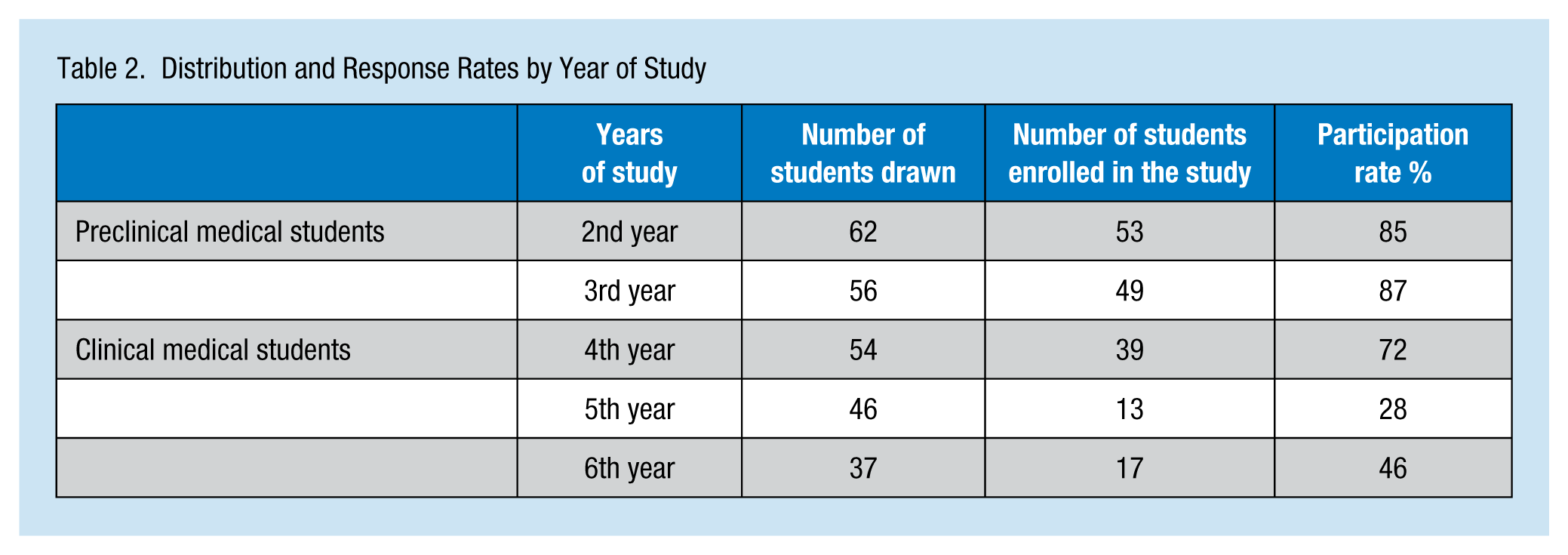
A cross-sectional survey was conducted from March 2011 to May 2011 by randomly selecting (using an interval of 4) 255 medical students from the 1,021 students enrolled in their second to sixth year in a French medical school. Second- and third-year medical students are enrolled in the preclinical phase of their education; fourth-, fifth-, and sixth-year students are enrolled in the clinical phase and are preparing for a highly competitive national examination.
This research was conducted in the context of a public health course. Eighteen students, supervised by a public health faculty member, designed and implemented this study. The study was approved by the University Medical School Board. Participants did not receive any financial compensation. Students were told the questionnaires were anonymous and their participation was entirely voluntary.
Students were invited to participate primarily via an email invitation sent to all randomly selected students. Students were sent up to four email reminders that ceased with completion of the survey or their refusal to participate.
Because the survey responses were anonymous, specific monitoring or referral to mental health resources for students who reported depression or suicidal ideation was impossible. However, participants were provided with systematic information, inviting them to seek care at the university health service in the case of alcohol, tobacco, drug, or mental health problems.
Survey Instrument
Questionnaires were self-administered and included questions on student sociodemographic characteristics, their well-being and mental health, as well as standardized instruments on alcohol, tobacco, and illegal substance consumption. Well-being and mental health were assessed with simple closed-ended questions. To validate the results, multiple questions on the same topic were included for participants to answer.
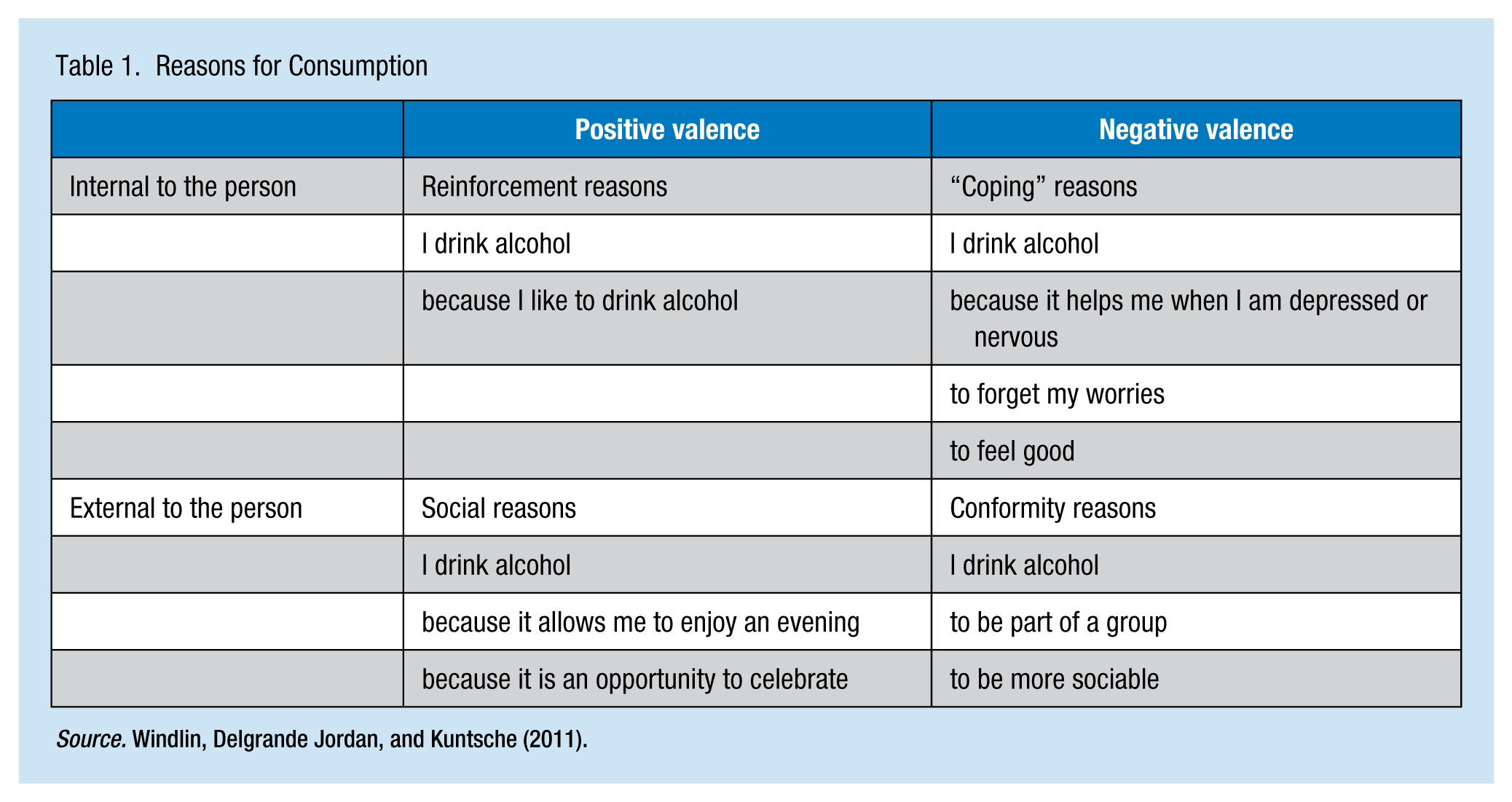
Alcohol consumption was assessed via the Alcohol Use Disorders Identification Test (AUDIT), a 10-item questionnaire that covers the domains of alcohol consumption (Questions 1-3), drinking behavior and dependence (Questions 4-6), and alcohol-related problems (Questions 7-10; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). Each question was scored from 0 to 4; the range of possible scores was 0 to 40. The AUDIT test distinguishes between normal drinking, hazardous drinking, and harmful drinking. The French version of the AUDIT tool recommends a score of 13 to identify alcohol-dependent individuals. The accepted score to identify hazardous drinkers is 7 for males and 6 for females (Gache et al., 2005). The WHO recommends a score of 11 or more in the original version to identify a potential alcohol problem, but currently the generally accepted score for adults with potential alcohol problems is 8 (Reinert & Allen, 2002). The AUDIT tool is widely used and has been validated in student populations. The study by Kokotailo et al. suggested that AUDIT is a valid instrument for alcohol screening in a college-age population (Kokotailo et al., 2004). Students at risk were identified in accordance with the internationally accepted score of 8. The conventional score of 8 has a sensitivity of 0.82 and a specificity of 0.78 to detect high-risk drinkers. Participants were also asked about their reasons for drinking. The reasons for alcohol consumption were classified as internal or external to the individual according to their “positive” or “negative” valence (Table 1; Windlin, Delgrande Jordan, & Kuntsche, 2011). “Positive” valence included the following reasons for alcohol consumption: “because I like it” or “because it allows me to celebrate or enjoy a party.” “Negative” valence included the following reasons for alcohol consumption: “because I am nervous or depressed,” or “because it’s a way to be a part of a group.”
Reasons for Consumption
Smoking was assessed by the Fagerstrom test for nicotine dependence, a widely used and validated six-item questionnaire (Heatherton, Kozlowski, Frecker, & Fagerström, 1991). The accepted score for identifying nicotine dependence is 4 or more and 6 or more for severe nicotine dependence.
Cannabis consumption was assessed by the Cannabis Abuse Screening Test (CAST), a six-item scale (Legleye, Karila, Beck, & Reynaud, 2007) that identifies patterns of cannabis use leading to negative social or health consequences for the user or others. The researchers used the binary version of CAST. The binary and the full version of CAST are equally useful for cannabis-related disorders screening (Legleye, Piontek, & Kraus, 2011). The accepted score for cannabis-related screening is 4. The questionnaire also included questions on other illegal substance use and the frequency of consumption during the previous 12 months.
Data Analysis
Descriptive statistical analysis was used on responses to closed-ended questions and qualitative analysis was used on responses to open-ended questions. Quantitative variables were expressed as the mean and standard deviation or as percentages. A Pearson’s Chi-square test or a two-tailed Fisher’s exact test was used to compare percentages after assessing the conditions of test use. Student’s t test or Mann–Whitney two-tailed test was used to compare means. Statistical significance was set at p < .05. All analyses used the Statistical Package for the Social Sciences (version 11.0, SPSS, Inc).
Variables were dichotomized and included stage of medical education, gender, study years repeated, scholarships, stress, and substance use. Substance use was defined as abuse of at least one of the three substances, namely, alcohol, tobacco, and cannabis. Simple linear regression was used to assess the links between substance use, stress, socioeconomic status, gender, and examination success. Multiple logistic regression was also used with significance set at p < .05.
Results
In this group of 255 randomly selected medical students, 171 complete questionnaires were returned (67%). The distribution and response rates by medical school classification are summarized in Table 2.
Distribution and Response Rates by Year of Study
The sex ratio was 0.79 (75 males/95 females) and the average age was 22.1 years ± 1.7 (range = 17-28). Fifty-three percent of students had never repeated a year during medical school; 35% had repeated once, and 12% had repeated at least twice. One quarter of students had a scholarship, 30% of students lived with their parents, 32% came from families in which at least 1 parent was a health care professional, and 10% came from families in which both parents were health care professionals.
Alcohol Consumption
The majority (97%) of students consumed alcohol. The results of the AUDIT score indicated that 11% of students were hazardous drinkers, 21% were harmful drinkers, and 68% were not at risk.
Seventy-eight percent of students had been drunk on at least one occasion during the previous 12 months. The average number of drunk episodes during the previous year was 11.8 (±12.6). Over the past 12 months, 17% of students with a driver’s license had driven while drunk.
Preclinical medical students more frequently engaged in risky or hazardous alcohol consumption (47%) than clinical medical students (16%; p < .05). No significant difference in alcohol consumption by economic status or parental occupation was observed.
Analysis of responses to the various questions on the AUDIT tool showed a difference between male and female students in terms of the frequency of alcohol consumption, the number of drinks on each occasion, the ability to stop drinking, a history of being injured or having injured someone else in an alcohol-related context, and type of consumption (Table 3).
Sample Characteristics of AUDIT Scores by Gender
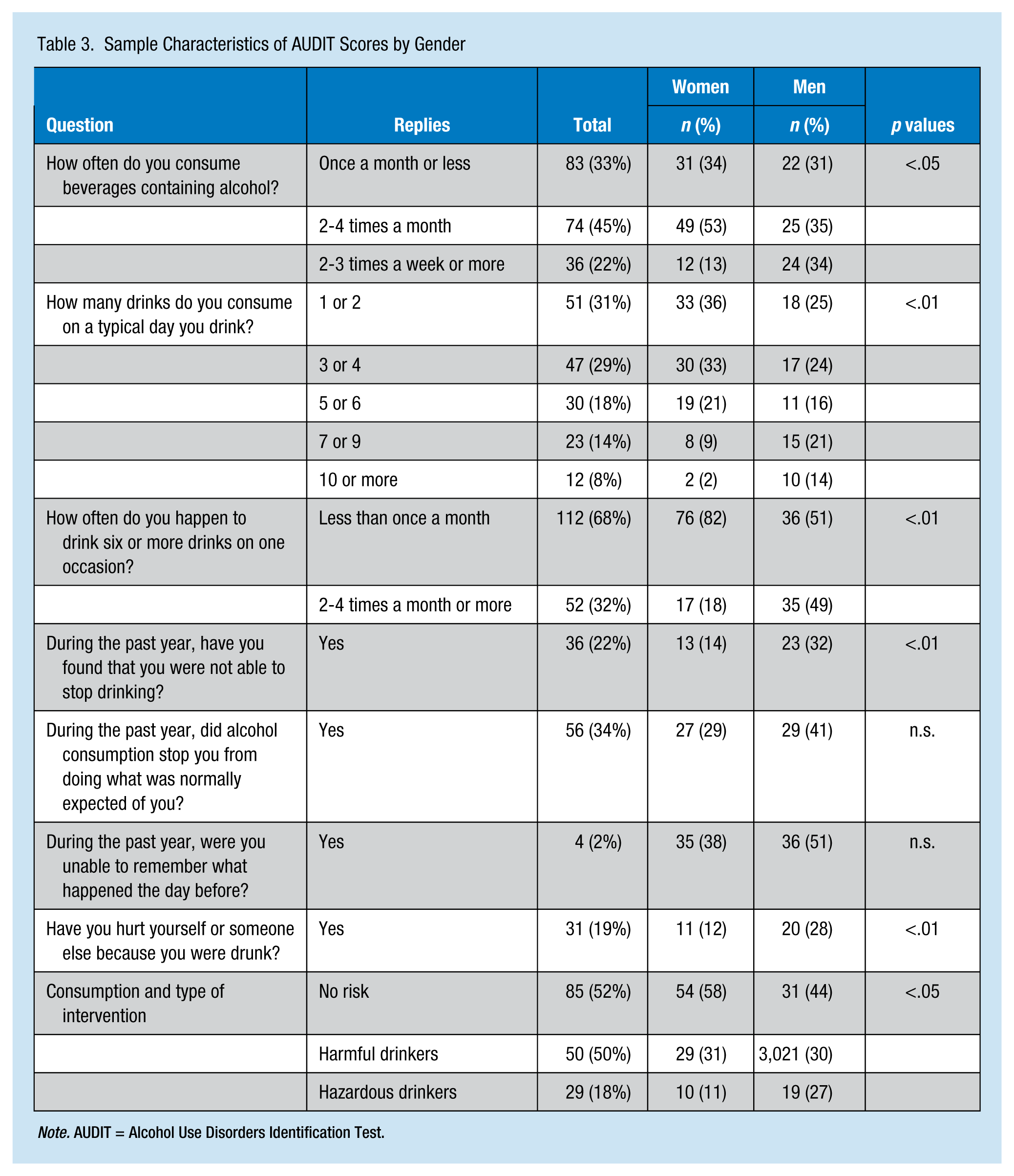
Note. AUDIT = Alcohol Use Disorders Identification Test.
The reasons for alcohol consumption are summarized in Figure 1. Students at at greater risk of hazardous or harmful alcohol consumption more frequently reported the following reasons for drinking compared with students reporting normal drinking
to forget their worries (26% vs. 12%, p < .05),
pressure from friends (24% vs. 6%, p < .01),
to enjoy a party (99% vs. 69%, p < .01),
to be more sociable (71% vs. 35%, p < .01),
because they like to drink alcohol (95% vs. 61%, p < .01),
to fit into a group (70% vs. 27%, p < .01),
to feel good (61% vs. 32%, p < .01).
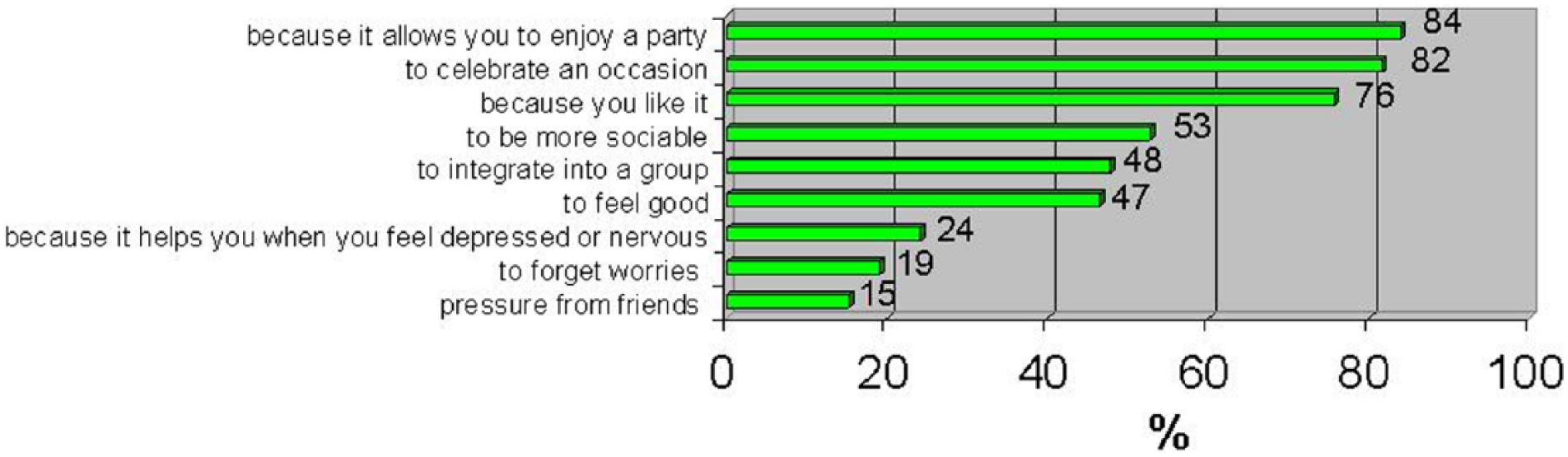
Reasons for alcohol consumption.
Cigarette Smoking
In this study population, 21% of students were regular tobacco smokers and another 16% were occasional smokers. Dependence scores were strong or very strong for 12% of students, and nearly two thirds of students (65%) reported very low dependence scores. The majority (74%) of smokers wanted to quit smoking. No significant difference was observed by gender, economic status, or parental occupation.
Illegal Substances
The majority of students (77%) had used cannabis during the previous 12 months: 7% at least once a day, 14% several times a week, 12% several times a month, and about two thirds of students (65%) had used cannabis once a month or less.
The responses to the CAST tool showed that 5% of cannabis users required health care and 10% should seriously consider the consequences of their consumption. No significant difference was observed by gender, economic status, or parental occupation. Cannabis users were found to more frequently fail their medical school examinations (89% vs. 39%, p < .01).
One quarter of students (n = 41) had also used other illegal drugs during the previous 12 months, most commonly “poppers” (93%; alkyl, cyclic or aliphatic nitrites), followed by magic mushrooms (14%), LSD (lysergic acid diethylamide-25) and cocaine (12%), misused prescription medications (9%), ecstasy (6%), and heroin (3%). Poppers were the most common illegal drug used: 2% used several times a week, 12% several times a month, and 78% once a month or less. Other illegal drugs (e.g., magic mushrooms, LSD, cocaine, prescription medication misuse, ecstasy, heroin) were used once a month or less.
Evaluation of Student Health
Nearly one of six students (58%) reported problems with stress, and 54% were distressed when thinking about their future. Over the previous 30 days, one in three students reported sleep disorders, 38% reported being easily tired, 29% felt sad and/or depressed, 47% were tense and/or nervous, and one in three was easily discouraged. Over the previous 12 months, 10% of students had considered suicide and 5% had made at least one suicide attempt during their lifetimes. Students who had considered suicide during the previous 12 months were more likely to be anxious about their futures than other students (81% vs. 52%, p < .05).
Clinical students had been more often discouraged during the previous 30 days than preclinical students (44% vs. 24%, p < .05). Similarly, clinical students reported more stress-related health problems than preclinical students (71% vs. 49%, p < .05)
Discussion
Psychoactive substance consumption by medical students is of concern. Alcohol was most frequently used by medical students in this study and was frequently consumed in large quantities in festive settings. Tobacco use also remains a concern as one in five medical students are regular smokers. Although experimentation with cannabis was a widespread phenomenon, regular use was exceptional among these students.
Substance use is high among French youth and adults; a representative national study conducted among 17-year-olds reported 12-month prevalence of 29% for regular tobacco smoking, 49% for binge drinking, and 25% for cannabis use (Beck, Guilbert, & Gautier, 2007). In a community sample of French young adults (age 22-35 years) in 2009, 35.8% regularly smoked tobacco, 14.3% showed signs of alcohol abuse, 6.3% reported problem cannabis use, and 12.4% used at least two psychoactive substances. In this study, with the exception of tobacco smoking, participants who were not in the labor force, such as students and unemployed individuals, systematically presented a higher prevalence of substance use than employed individuals. Students had the highest prevalence (40.5%) of alcohol abuse when compared with other groups (Redonnet, Chollet, Fombonne, Bowes, & Melchior, 2012).
Previous studies on medical students have reported that about 80% to 90% of these students drink alcohol (Pickard, Bates, Dorian, Greig, & Saint, 2000; Thakore et al., 2009; Voigt et al., 2009; Webb, Ashton, Kelly, & Kamali, 1997). Medical students consume more alcohol than non-students of the same age (Voigt et al., 2009). The prevalence of high-risk alcohol use among medical students varies from 15% to 52% by mode of detection (Granville-Chapman et al., 2001; Shah, Bazargan-Hejazi, Lindstrom, & Wolf, 2009). Preclinical medical students more frequently reported risky or hazardous alcohol consumption (47%) than clinical medical students (16%; p < .05). Consumption tended to decrease as students progressed through medical school. However, alcohol consumption during the study may be for some people the beginning of addiction. All studies assessing alcohol problems or dependence in adulthood found statistically significant associations with late teenage drinking (McCambridge, McAlaney, & Rowe, 2011).
The prevalence of cannabis use ranges from 15% to 42% (Di Pietro, Doering-Silveira, Oliveira, Rosa-Oliveira, & Da Silveira, 2007; Kjøbli et al., 2004; Petroianu, Reis, Cunha, & Souza, 2010) among medical students or higher (>50%) for students reporting frequent heavy consumption of alcohol (Keller, Maddock, Laforge, Velicer, & Basler, 2007). Tobacco use in France does not appear to be lower among medical students than the general population of the same age. A study in a Paris medical school showed that more than one third of students were smokers (35%); 21% were daily smokers and 14% were occasional smokers (Josseran, Raffin, Dautzenberg, & Brücker, 2003). This rate is similar to that reported in a European study (Germany, Italy, Poland, and Spain), with 29% of the sample reported to be smokers (La Torre et al., 2012).
The use of psychoactive substances raised questions about the ability of these students to meet their future professional responsibilities, particularly in terms of health promotion and education. La Torre et al. (2012) found that most medical students recognized that health care professionals are role models for the general population. In this study, 74% of smokers wanted to quit smoking. According to Warren, Jones, Chauvin, and Peruga (2008), medical schools have a moral duty to assist students quit smoking.
The researchers wondered whether consumption may be the cause or consequence of student difficulties including academic failure. In this study, cannabis users more frequently failed examinations than those students who did not use cannabis (89% vs. 39%, p < .01). However, it is unknown whether cannabis use is the result of personal or academic difficulties or the cause of these difficulties. Stress is inevitable in professional education (Stecker, 2004).
Ill-being is common among students, but no significant association with substance use was established. No risk profile to guide prevention efforts was identified in this study. Stress is a risk factor for headache, gastrointestinal disorders, coronary heart disease, depression, impaired judgment, absenteeism, and self-medication with drugs and alcohol (Firth-Cozens, 2001). In addition, medical students and physicians who fail to manage their stress are less likely to be safe or competent health care providers (Firth-Cozens, 2003). Stress management for medical students is a challenge affecting the health of future physicians. Teaching students how to manage stress may also contribute to high-quality safe care.
One quarter of study medical students had also used other illegal drugs during the previous 12 months. Nevertheless, the use of illegal drugs remains exceptional and marginal. With the exception of poppers, students who consumed illegal drugs have done so less than once per month. However, this level of consumption is worrying because these future health professionals have or will have access to drugs such as morphine and ketamine.
Limitations of the Study
Selection bias was limited by randomization. However, the participation rate was a source of bias, especially for fifth- and sixth-year students. The use of a self-administered questionnaire was also a potential bias. To avoid an excessively long questionnaire, a validated scale was not used to assess mental health, which limits interpretation of these results. It could be interesting to use an instrument such as the Medical Student Stress Profile (MSSP; O’Rourke, Hammond, O’Flynn, & Boylan, 2010). A response bias was also possible due to non-responders.
This study was based on a small sample from a single French medical school, and cannot claim to be representative of the general population of medical students globally. These results and conclusions should therefore be viewed with caution. Although this cross-sectional study provides interesting findings to guide local preventive actions, monitoring a multicenter prospective cohort would be particularly useful to identify characteristics and trends regarding medium- and long-term addiction and burnout. This survey study should be replicated at other universities to provide comparisons and guide the development of preventive actions.
Implications for Occupational Health Nursing Practice
These study findings are consistent with international literature. Psychoactive substance consumption by medical students is worrisome. Preventive and educational programs at the university may be required to prevent and eliminate substance abuse among medical students. Students and practicing physicians could benefit from consultation about and screening for psychoactive substance consumption at an occupational health service.
Some medical schools include self-care programs in their curricula (Hassed, de Lisle, Sullivan, & Pier, 2009). It could be beneficial to introduce education on the risks of alcohol, tobacco, cannabis, and other substances. Accurate knowledge on these risks would be useful for the practices and personal health of future health care professionals.
Screening and brief counseling could also reduce excessive alcohol consumption and are therefore recommended by the U.S. Preventive Services Task Force (U.S. Preventive Services Task Force, 2004). Medical schools should assist their students in quitting smoking by providing encouragement and information to students and assisting those students who are motivated to quit.
Programs designed to assist physicians addicted to tobacco, alcohol, and illegal drugs have been developed in many countries, including all U.S. states and Canadian provinces, in collaboration with medical associations and regulatory bodies (Brewster, Kaufmann, Hutchison, & MacWilliam, 2008; Puddester, 2001; Schattner, Davidson, & Serry, 2004). Several Australian universities have created “personal and professional development” programs to encourage self-care for health professionals (Gordon, 2003).
Medical students who consume psychoactive substances are of particular concern and require preventive measures, screening, and treatment. Medical schools should offer screening and assistance to students to improve their health and provide care and health education messages.
Students should learn how to manage stress and contribute to the quality and safety of the health care they provide. Students’ well-being and stress must be considered by medical schools when creating their educational cultures. Medical schools should ensure that their organization (e.g., schedule, communication with students, examination schedule) is not a source of unnecessary stress.
Data about physicians’ health could be used to develop programs to reduce psychosocial risks. Not only could study data and resulting programs benefit health care professionals but could raise awareness of the psychosocial risks for others. Finally, a strong consistent correlation between physicians’ personal health practices, including their practices with alcohol (Frank et al., 1998), and their counseling practices (Frank, 2004), has been found. Sotos et al. found that students can improve their knowledge and ability to detect hazardous drinking by quantifying alcohol consumption using a simple educational intervention. After assessing their own consumption, a considerable proportion of students realized they were indulging in excessive alcohol consumption, which could in turn increase awareness of the problem among future health professionals (Rabanales Sotos et al., 2015). Eliminating the consumption of psychoactive substances among health professions students could be an interesting area of study for occupational health nurses.
Conclusion
Substance use and stress are major challenges for medical students, as they threaten the health and practices of future physicians. Medical schools should address the health of their students and provide support for students in need. These actions could be implemented with the active participation of students in occupational health and public health programs.
Applying Research to Practice
Psychoactive substance consumption by medical students is worrisome. Preventive and educational programs at the university may be required to prevent and eliminate substance abuse among medical students. Students and practicing physicians could benefit from consultation and screening for psychoactive substance consumption at an occupational health service. Students’ wellbeing and stress must be considered by medical schools. Teaching students how to manage stress could be included in the curriculum. Medical schools should also ensure that their organization is not a source of unnecessary stress. A strong consistent correlation between physicians’ personal health practices, including their alcohol intake, and their counselling practices has been found. Healthier caregivers are better caregivers for their patients.
Footnotes
Acknowledgements
The authors thank the following persons who helped design and implement this study: Pauline Decaigny, Rodolphe Chartier, Juliette Boulenger, Amédée Didaux, Mario Gaudière, Yannis Abir, Nacera El Bouzegaoui, Valérie Baudry, Elodie Carpentier, Simon Antide, Cédric Rakotondrantoanina, Camille Desbonnets, Anne-Claire Poupart, Charles Delahaye, Chloé Werner, Typhaine Georges, Karim Astar, and Mrs. Catherine Dubois.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
M. Gignon is an associate professor in public health, specializing in prevention and health education. He is a member of the medical education department at the University of Picardie.
E. Havet is a full professor of anatomy. He is a member of the Amiens Medical School board, in charge of the preclinical cycle. He is a member of the medical education department of the University of Picardie.
C. Ammirati is a professor of emergency medicine. She has a PhD in educational sciences. She is the head of the medical education department at the University of Picardie.
S. Traullé is a medical doctor specializing in cardiology. She takes part of the clinical cycle education at the University of Picardie.
C. Manaouil is a professor in forensic medicine at the Amiens Medical School. She is also a Juris Doctor. She takes part of the clinical cycle.
T. Balcaen specializes in public health and epidemiology at the Amiens University Hospital.
G. Loas is a professor in psychiatry. He is in charge of training in addiction.
G. Dubois is a professor in public health. He is a specialist in tobacco control. He is a member of the French National Academy of Medicine.
O. Ganry is a professor in public health. He is the head of the Public Health Department at the Amiens University Hospital.