
Abstract
“The study’s findings support the idea that increased CVD prevalence rates among young and middle-aged U.S. adults may be associated with the use of substances such as non-cigarette tobacco products and cannabis among this population group.”
Introduction
Cardiovascular disease (CVD) persists as the leading cause of morbidity and mortality in the United States (U.S.).1,2 In the past two decades, the incidence of CVD has increased among young and middle-aged adults in contrast to declining rates of CVD among adults aged 60 years and older.3-5 Given that CVD imposes a significant health and socioeconomic burden and is multifactorial in etiology,1,6 identifying modifiable risk factors is important for the prevention and treatment of CVD. Substance use is one of the primary preventable risk factors for CVD, and among young and middle-aged adults, substance use prevalence remains high with increasing rates over the past decade.7-11 Specifically, the deleterious impacts of cigarette smoking on cardiovascular health have been well-documented,12-15 leading to public health efforts and health promotion interventions that have been successful in reducing cigarette smoking rates among U.S. adults. 16 However, with the decline in cigarette use, use of other substances such as non-cigarette tobacco products (i.e., electronic cigarettes and smokeless tobacco) and cannabis has become increasingly popular among young and middle-aged adults, perhaps due to perceptions that these products are less harmful and a safer alternative for cardiovascular health.8,17-19 Although non-cigarette tobacco and cannabis may not be as toxic as cigarettes, each substance contains different harmful compounds that can induce endothelial dysfunction, oxidative stress, and atherogenesis.20-22 Similarly, evidence suggests that illicit drugs contain toxic components that may be detrimental to health including cardiovascular health. 4 Therefore, research that focuses on use of these alternative substances is important as they may be linked to the rising rates of premature CVD among young and middle-aged adults. 4
Despite the increase in the use of non-cigarette tobacco products, cannabis, and illicit drugs, important knowledge gaps on their cardiovascular health effects remain. 23 Previous studies investigating the associations between cannabis, non-cigarette tobacco, and illicit drug use and CVD among adults have produced mixed results, with some studies finding positive associations between these substances and CVD,4,24 and other studies finding no associations.21,25,26 Furthermore, prior work suggests that there is variability in the types of cardiovascular event depending on the substance used. 27 Hence, attempting to understand the potential unique differences in the relationships between each of these substances and CVD is important for tailoring substance use prevention interventions and policies prioritizing CVD control among young and middle-aged adults.
Notably, substance use-related CVD disproportionately impacts certain subpopulations such as members of racial and ethnic minority and sexual minority groups, women, low-income individuals, and individuals with lower educational levels. 1 Given the popularity of cannabis, non-cigarette tobacco, and illicit drug use among adults and harm-causing potential, concerns exist regarding potential impact on cardiovascular health, particularly among younger adults and certain sociodemographic groups.1,4,28 Consequently, this study aimed to examine the association between lifetime use of non-cigarette tobacco, cannabis, and illicit drugs and CVD using nationally representative data on young and middle-aged adults in the U.S. The study also characterized CVD diagnosis by sociodemographic and behavioral characteristics. We hypothesized that young and middle-aged adults who ever used electronic cigarettes, cigars, smokeless tobacco, cannabis, or illicit drugs have higher odds of coronary heart disease, stroke, or hypertension than those who have never used these substances.
Methods
Study Design
Data were obtained from the 2017-2018 National Health and Nutrition Examination Survey (NHANES). NHANES is a cross-sectional, nationally representative survey of the noninstitutionalized civilian U.S. population. NHANES uses a complex, multistage stratified sample design to estimate national prevalence of health, nutritional status, and potential risk factors. Data on sociodemographic characteristics, lifestyle factors, body measurements, and medical conditions were obtained through household interviews and physical examinations at a mobile examination center during the data collection cycle. 29 NHANES was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and the study was deemed exempt from review by the University of Mississippi Medical Center Institutional Review Board as the data are publicly available. Additional information about NHANES sampling methods and survey design can be found online. 29 We used the STROBE cross-sectional reporting guidelines. 30
Participants
A total of 9254 participants completed the 2017-2018 NHANES. For this analysis, participants were excluded if they were ages 19 and younger (n = 3685) or ages 60 and older (n = 2150) to restrict the sample to adults ages 20 to 59 years old as this study focused on young and middle-aged adults. CVD-related questions were included for participants aged 20 years and older; thus, we were not able to include young adults aged 18 or 19 years old. Further, participants who had missing information on substance use (n = 459), coronary heart disease (n = 2), stroke (n = 4), hypertension (n = 4), sociodemographic characteristics (n = 16), and behavioral characteristics (n = 1) were excluded. Details of exclusion criteria are shown in the study flow chart (see Figure 1). The final analytic sample included 2933 adults. Study flow chart 2017-2018 U.S. Adult National Health and Nutrition Examination survey.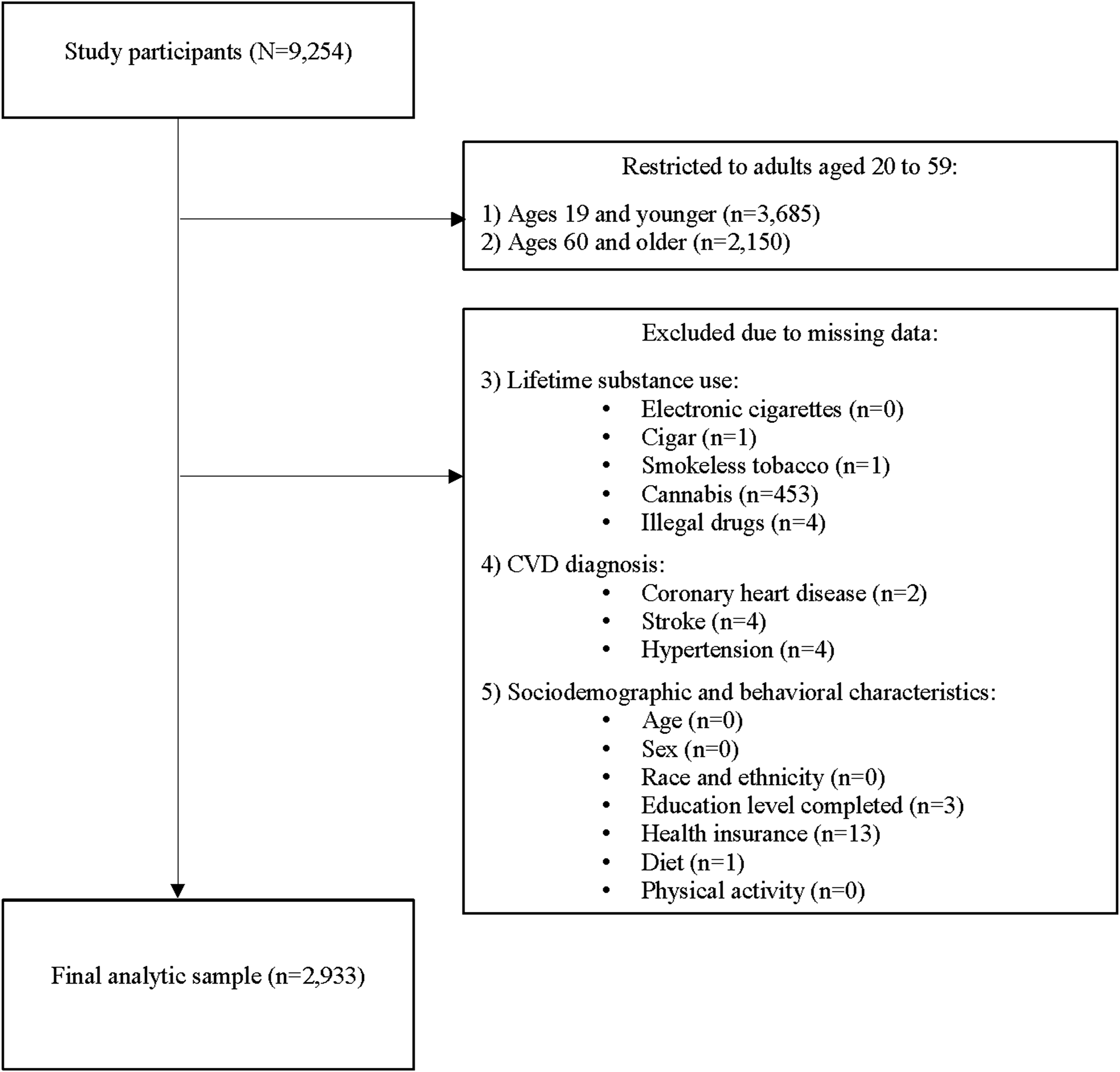
Measures
Cardiovascular Disease
Hypertension was defined from participants’ responses (yes or no) to the following question, “Have you ever been told by a doctor or other health professional that you had hypertension, also called high blood pressure?”. Coronary heart disease was defined from participants’ responses (yes or no) to the following question, “Has a doctor or other health professional ever told you that you had coronary heart disease?”. Similarly, stroke was defined based on participant responses (yes or no) to the following question, “Has a doctor or other health professional ever told you that you had stroke?”. Additionally, we created a composite variable to represent any CVD (i.e., yes in response to one or more of the above questions) and no CVD (i.e., no in response to all three questions).
Lifetime Non-Cigarette Tobacco, Cannabis, Illicit Drug Use
Lifetime use included ever use of e-cigarettes, cigars, smokeless tobacco, cannabis, or illicit drugs (i.e., cocaine, heroin, methamphetamine).
Sociodemographic and Behavioral Characteristics
Sociodemographic characteristics included age in years (20-29, 30-39, 40-49, 50-59), sex (female, male), education level completed (< than high school, high school/GED, associate degree, college degree), having health insurance (yes or no), and race and ethnicity (Mexican American, Other Hispanic, non-Hispanic White, non-Hispanic Black, another race/ethnicity). Another race/ethnicity included non-Hispanic Asian, non-Hispanic multiracial, and those not self-identifying as any of the above-mentioned races/ethnicities.
Behavioral characteristics assessed were physical activity and diet. Physical activity was defined based on participants’ responses (yes or no) to each of the following questions, “In a typical week do you do any moderate-intensity sports, fitness, or recreational activities that cause a small increase in breathing or heart rate such as brisk walking, bicycling, swimming or volleyball for at least 10 minutes continuously?” and “In a typical week do you do any vigorous-intensity sports, fitness, or recreational activities that cause large increases in breathing or heart rate like running or basketball for at least 10 minutes continuously?”. Physical activity was categorized in the analysis as physical activity (i.e., yes in response to one or more of the questions) and physical inactivity (i.e., no to both questions). Diet was defined based on participants’ responses (excellent, very good, good, fair, poor) to the following question, “In general, how healthy is your overall diet?”. Diet was categorized as good (i.e., good to excellent) and poor (i.e., fair to poor).
Analysis
Weighted percentages and confidence intervals of substance use, CVD, and sociodemographic and behavioral characteristics were examined. Each CVD by substance use and sociodemographic characteristics was evaluated using chi-square tests of independence or Fisher’s exact tests when appropriate. Multivariable logistic regression models were performed to examine associations of lifetime cannabis, non-cigarette, and illicit drug use and each CVD (i.e., coronary heart disease, stroke, and hypertension individually). Further, multivariable logistic regression examining the associations between lifetime cannabis, non-cigarette, and illicit drug use and any CVD diagnosis was conducted. Each of the models was adjusted for age, sex, race and ethnicity, education level completed, health insurance, diet, and physical activity. Adjusted odds ratios and 95% confidence intervals are reported. Results were considered statistically significant at α = 0.05. Data were analyzed using Stata 18.0. We accounted for the NHANES complex survey design and adjusted for the probability of non-response by using the svy command and sample weights for the NHANES 2017-2018 data.
Results
Distributions of Participant Characteristics
Distributions of Participant Characteristics, Substance Use, and Cardiovascular Disease of Young and Middle-Aged Adults From National Health and Nutrition Examination Survey, 2017-2018 (N = 2933).
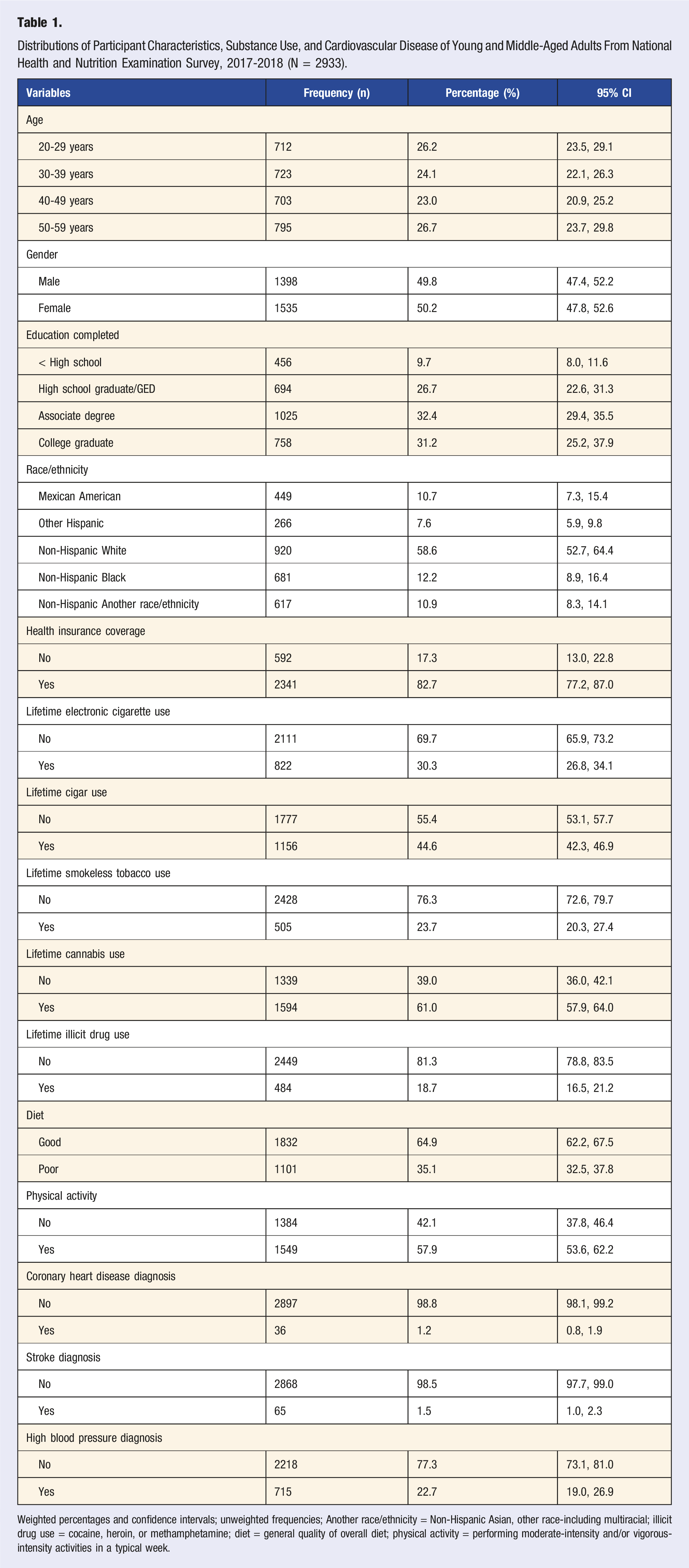
Weighted percentages and confidence intervals; unweighted frequencies; Another race/ethnicity = Non-Hispanic Asian, other race-including multiracial; illicit drug use = cocaine, heroin, or methamphetamine; diet = general quality of overall diet; physical activity = performing moderate-intensity and/or vigorous-intensity activities in a typical week.
CVD by Substance Use and Sociodemographic and Behavioral Characteristics
Cardiovascular Disease by Sociodemographic and Behavioral Characteristics, Lifetime Substance Use Among Young and Middle-Aged U.S. Adults (N = 2933).
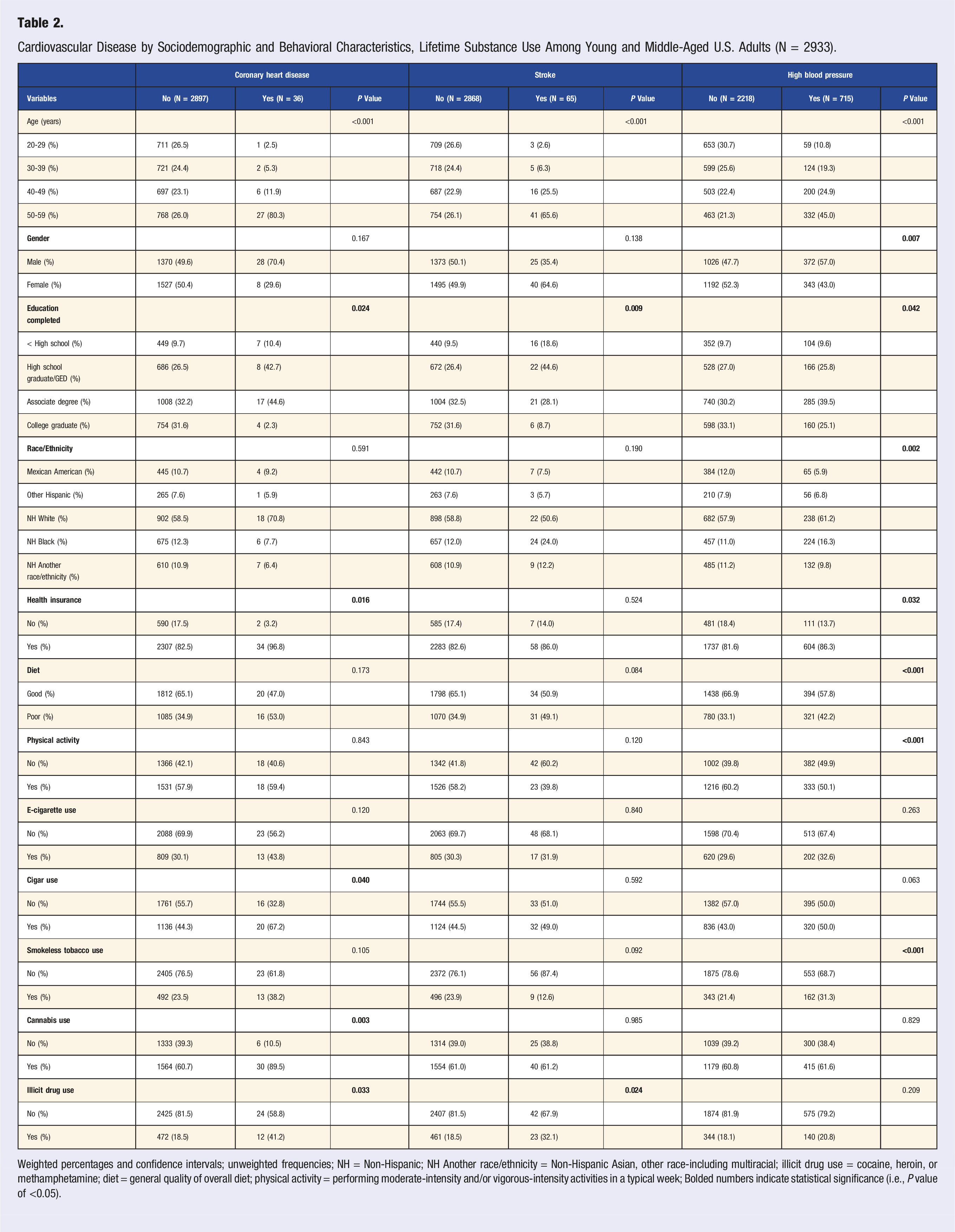
Weighted percentages and confidence intervals; unweighted frequencies; NH = Non-Hispanic; NH Another race/ethnicity = Non-Hispanic Asian, other race-including multiracial; illicit drug use = cocaine, heroin, or methamphetamine; diet = general quality of overall diet; physical activity = performing moderate-intensity and/or vigorous-intensity activities in a typical week; Bolded numbers indicate statistical significance (i.e., P value of <0.05).
Multivariable Logistic Regression
Multivariable Logistic Regression Estimating the Associations Between Non-cigarette, Cannabis, and Illicit Drug Use and Cardiovascular Disease in Young and Middle-Aged U.S. Adults (n = 2933).
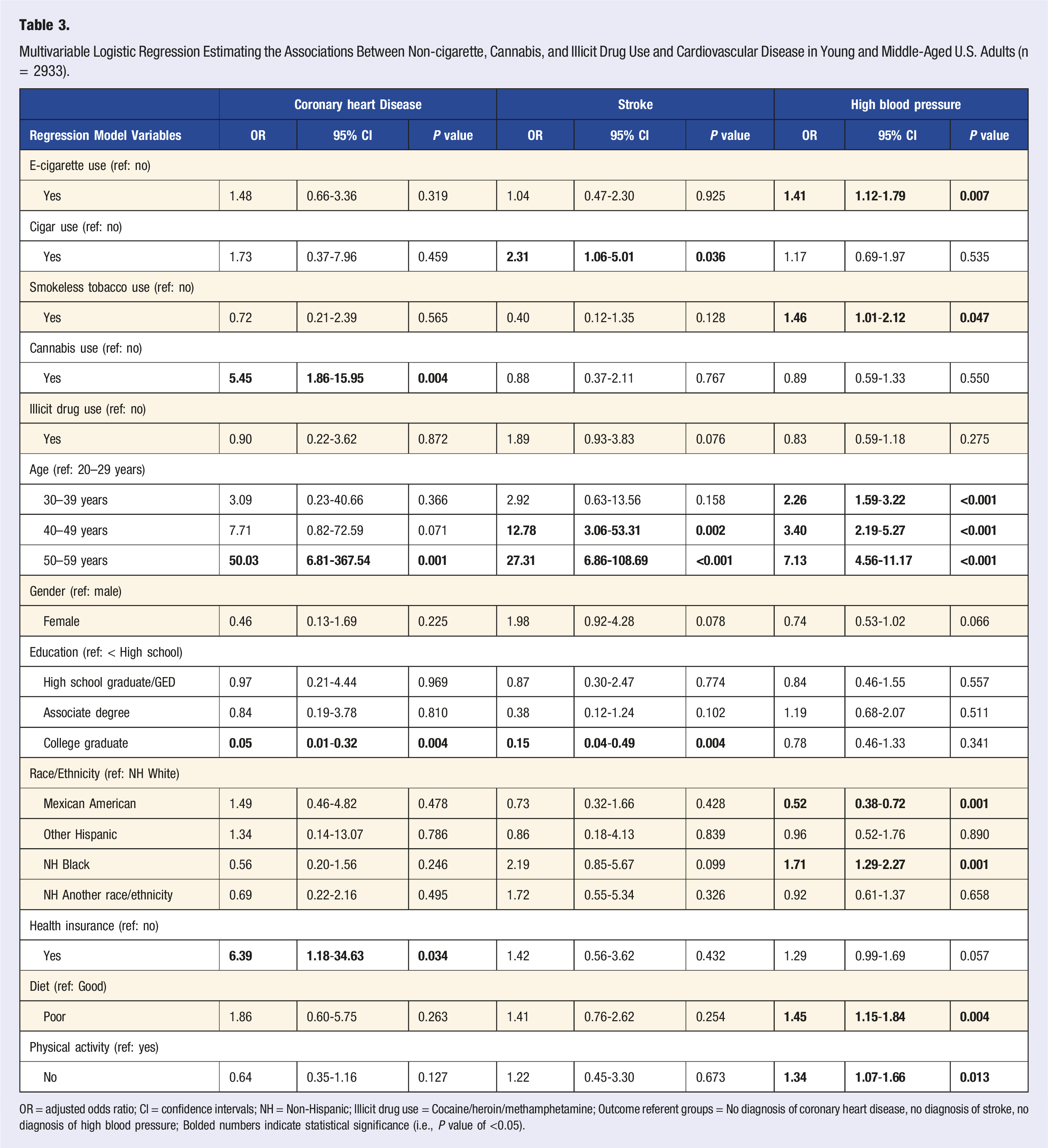
OR = adjusted odds ratio; CI = confidence intervals; NH = Non-Hispanic; Illicit drug use = Cocaine/heroin/methamphetamine; Outcome referent groups = No diagnosis of coronary heart disease, no diagnosis of stroke, no diagnosis of high blood pressure; Bolded numbers indicate statistical significance (i.e., P value of <0.05).
Adults who used cigars (OR: 2.31, 95% CI: 1.06-5.01) had higher odds of being diagnosed with stroke compared to those who never used cigars. Adults who used electronic cigarettes (OR: 1.41, 95% CI: 1.12-1.79) and smokeless tobacco (OR: 1.46, 95% CI: 1.01-2.12) had higher odds of being diagnosed with hypertension compared to adults who never used electronic cigarettes and those who never used smokeless tobacco, respectively. In addition, adults who reported poor diet (OR: 1.45, 95% CI: 1.15-1.84) and were physically inactive (OR: 1.34, 95% CI: 1.07-1.66) had higher odds of being diagnosed with hypertension compared to adults who reported good diet and were physically active, respectively.
Multivariable Logistic Regression Estimating the Associations Between Lifetime Non-cigarette, Cannabis, and Illicit Drug Use and Diagnosis of Any Cardiovascular Disease (n = 2933).
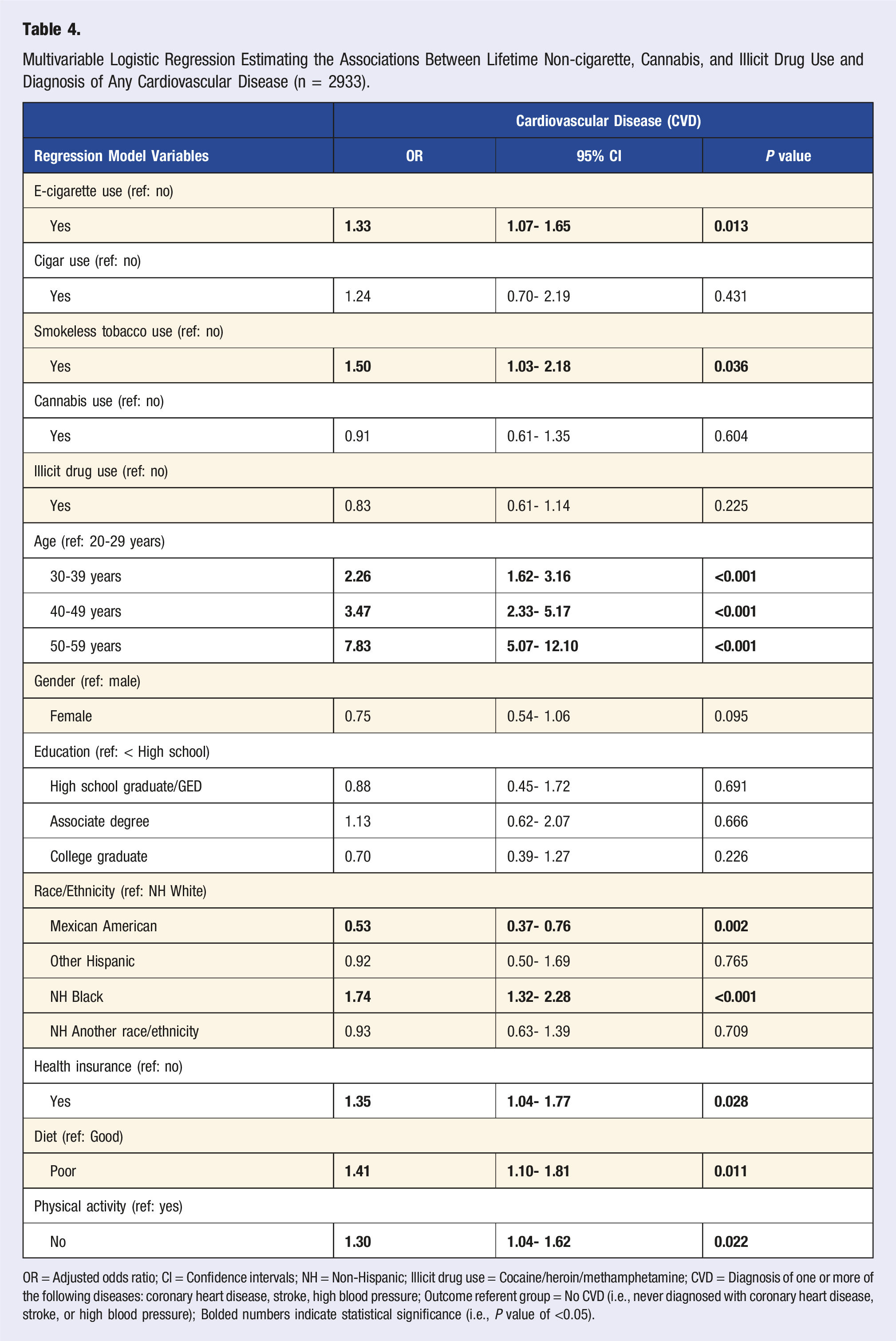
OR = Adjusted odds ratio; CI = Confidence intervals; NH = Non-Hispanic; Illicit drug use = Cocaine/heroin/methamphetamine; CVD = Diagnosis of one or more of the following diseases: coronary heart disease, stroke, high blood pressure; Outcome referent group = No CVD (i.e., never diagnosed with coronary heart disease, stroke, or high blood pressure); Bolded numbers indicate statistical significance (i.e., P value of <0.05).
Discussion
This study examined the association between lifetime substance use and CVD among U.S. young and middle-aged adults, using nationally representative survey data adjusted for sociodemographic and behavioral characteristics. Notably, a significant number of young and middle-aged adults in this study used cannabis, cigars, electronic cigarettes, smokeless tobacco, or illicit drugs (lifetime range: 18.7% illicit drug use and 61.0% cannabis use). Furthermore, cannabis use was found to be associated with coronary heart disease, cigar use with stroke, and electronic cigarette and smokeless tobacco use with high blood pressure. The study’s findings support the idea that increased CVD prevalence rates among young and middle-aged U.S. adults may be associated with the use of substances such as non-cigarette tobacco products and cannabis among this population group. These findings also indicate that more work is needed to prevent and address substance use among young and middle-aged adults in the U.S. to reduce substance use-related morbidity and premature mortality.
Our finding that e-cigarette use may be linked to high blood pressure is consistent with prior research.18,31,32 Potential mechanisms for this association are nicotine induced sympathomimetic effects, vasoconstriction, and the release of catecholamines that increase blood pressure.17,33,34 A meta-analysis of 14 studies found that electronic cigarette use increased systolic and diastolic blood pressure and heart rate among 441 adult participants. 18 Further, pre-clinical studies have found that e-cigarette use can induce cytotoxicity, inflammation, platelet activation, and endothelial dysfunction resulting in CVD development.33,35 However, in this study we did not find an association between e-cigarette use and stroke or coronary heart disease, analogous to prior research done on young and middle-aged adults.36,37 Furthermore, research suggests that using other tobacco products, such as smokeless tobacco, delivers significant nicotine to the cardiovascular system,38,39 and, thus, our finding of an association between smokeless tobacco use and high blood pressure among young and middle-aged adults adds to the literature. Cigar use, on the other hand, was associated with stroke in this study, similar to previous work with U.S. adults. 40 Still, there is a scarcity of research on substance use and CVD, especially among young and middle-aged adults using nationally representative samples; however, one recent study of adults 40 years and older found no associations between cigar use and CVD. 41 More research is needed that utilizes nationally representative data to investigate the associations and effects of non-cigarette tobacco product use on CVD development among young and middle-aged U.S. adults.
The cardiovascular effects of cannabis use are not fully known; however, perhaps due to more states legalizing cannabis for both medicinal and recreational purposes, use among young and middle-aged adults is rapidly increasing.7,14,42 The current study’s finding that cannabis use is associated with higher odds of coronary heart disease among young and middle-aged adults is consistent with previous research.24,42 One potential mechanism behind this association is tetrahydrocannabinol (THC) induced endothelial inflammation, vasospasms and atherosclerosis resulting in coronary heart disease.24,42,43 Cannabis use may have significant adverse effects on the cardiovascular system, and prior analyses with Behavioral Risk Factor Surveillance System survey data found that cannabis use was associated with higher odds of stroke and myocardial infarction in young adults ages 18-44.44,45 However, this study’s findings of no significant associations between cannabis use and stroke or high blood pressure among young and middle-aged adults mirror the results of other studies on middle-aged adults and CVD.21,26 Given that the cardiovascular effects of cannabis use are not well understood in this age group, health programs and educational campaigns that inform the public and health care providers about the potential cardiovascular consequences of cannabis use are warranted.
The current study findings reveal significant disparities in CVD by sociodemographic and behavioral characteristics among young and middle-aged adults. Notably, the CVD disparities for young and middle-aged adults who identify as non-Hispanic Black and male as well as those with lower educational attainment are consistent with prior research done on adults.1,46 These disparities are a cause for concern and indicate the need for CVD prevention programs prior to or in young adulthood that are focused on substance use control. Furthermore, efforts that address structural causes that contribute to sociodemographic and behavioral differences in substance use and CVD may reduce the burden borne by minority populations. Culturally appropriate and sensitive community-based interventions focused on engaging young and middle-aged adult members of minority and underserved population groups are critical for addressing the growing inequities in substance use and CVD across population groups in the U.S. 47 Overall, health care policies that promote early screening for substance use among young and middle-aged adults are crucial to reducing CVD morbidity and premature mortality. Communication campaigns that increase awareness about unhealthy lifestyle behaviors including substance use may be useful in improving cardiovascular health outcomes for all adults. Health care provider screening and counseling for substance use may be pivotal in substance use control for young adults.48-50
Limitations
The current study has some limitations. First, the cross-sectional nature of the NHANES data precludes causal inference. Second, the study relied on self-reported responses which may be subject to recall and social desirability bias. Third, although the study adjusted for covariates, such as sociodemographic and behavioral characteristics, it is possible that other unmeasured confounders may remain that affected our findings. Fourth, the study’s design cannot account for the possibility that people who used cigarettes may have switched to using cannabis and non-cigarette substances in response to a CVD diagnosis.
Conclusion
This study found that lifetime cannabis use is linked to coronary heart disease, cigar use is linked to stroke, and electronic cigarette and smokeless tobacco use are linked to high blood pressure among young and middle-aged U.S. adults. These findings emphasize the need for health care provider screening and counseling for substance use among this population. The development and implementation of policies and interventions focused on engaging young and middle-aged adult members of minority and underserved population groups are critical for addressing CVD disparities and premature mortality. Further, public health campaigns that increase awareness about unhealthy lifestyle behaviors including substance use may be helpful in improving cardiovascular health outcomes for all adults.
Consent to Participate
All participants in the NHANES gave full consent to participate.
Footnotes
Acknowledgments
This research was supported, in part, by a grant from the National Institutes of Health (NHLBI) and the Center for Tobacco Products (U54HL120163). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Food & Drug Administration. The funding sponsors had no role in study design; data collection, analyses, or interpretation; manuscript preparation; or the decision to publish the results.
Author Contributions
Osayande Agbonlahor: Conceptualization, Methodology, Formal Analysis, Data interpretation, Writing—original draft, Writing—review and editing. Delvon T. Mattingly: Conceptualization, Methodology, Writing—review and editing. Joy L Hart: Conceptualization, Methodology, Writing—review and editing, Supervision. Maggie K. Richardson: Conceptualization, Writing—review and editing. Alison C. McLeish: Conceptualization, Writing—review and editing. Kandi L Walker: Conceptualization, Writing—review and editing, Supervision. All authors have read and approved the final manuscript as submitted to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by a grant from the National Institutes of Health and the Center for Tobacco Products (U54HL120163).
Ethical Considerations
Ethical approval was obtained from the National Center for Health Statistics (NCHS) Research Ethics Review Board, and the University of Mississippi Medical Center Institutional Review Board deemed the study exempt from review due to use of public, deidentified data.
Data Availability Statement
Data will be made available on request.