
Abstract
Alcohol consumption among humans has lasted for several centuries. In Africa, drinking is normal for men despite its consequences. The study is aimed at determining the rate of alcohol consumption in the study area, health consequences of alcoholism and factors that reinforce alcoholism among men. The study, which adopted descriptive survey design, was conducted at Ezeagu, Southeast Nigeria. Quota sampling was used to select participants (400). A questionnaire was used to collect data, and analysis was done using descriptive statistics. The data revealed that men in the area are heavy drinkers, but their level of awareness about its health consequences is low. The study shows that the factors preventing men from quitting alcohol consumption include peer group influence and traditional ceremonies/festivals. The study concludes that alcoholism has adverse health consequences. Men hardly quit alcohol consumption because of factors within their communities, therefore; raising the awareness level about the adverse health implications of alcoholism is a necessity.
Background
Alcohol production and consumption has been an ancient human practice in different societies, which has spanned over 10,000 years (Smart, 2007). In Nigeria, locally produced alcoholic beverages have existed for many centuries (Obot, 2007). Alcohol consumption is a big business in Nigeria with consumers spending a little less than one trillion naira in just 2016 (Adebowale, 2019). Alcohol consumption in most rural societies is seen as normal, especially when people drink it without getting intoxicated. Different kinds of wine, spirit and other fermented alcoholic drinks were consumed in traditional societies and are still being consumed in present-day societies. People have various reasons for consuming alcoholic beverages. Some alcoholic beverages such as palm wine and burukutu are consumed for pleasure. Most people prefer consuming them immediately after tapping or brewing (Odejide, 1999, 2006). In the past, they were not usually sold in the market (World Health Organization [WHO], 2002).
Even though alcohol consumption has been an old tradition, excessive consumption of it was not usually tolerated in the past. Only a few communities permitted it (Willis, 2006). It has been argued that the increase in the intake of alcohol has been a result of the influence of the media, advertising, sophisticated marketing and lack of alcohol policy in most societies (Dumbili, 2014; Nwosu, 2017).
It should be noted that while there are no written rules prohibiting females and adolescents from drinking alcohol in traditional setting, consumption was exclusively reserved for men (Odejide, 2006). In other words, men are prone to drink excessive alcohol than women (Adekanye, 2021; Kennard, 2021). This is mostly because alcohol played complex roles in religious and community rituals that are superintended by men. Alcohol also serves as a conduit for social cohesion, which is vital in the political life of men. This exposes men to the arena of alcohol more often.
According to WHO (2011), there is 61.7% abstention from alcohol consumption among Nigerians. Later studies revealed high episodic consumption among those who drink alcohol. For instance, Obot (2007) reported that the average per capita consumption for adults in Africa stood at 6.2 L, Nigerian’s adult per capita consumption is 12.3 L. This makes Nigerians to rank first in alcohol consumption in Africa. This supports an earlier study (Room & Selin, 2005), which placed Nigeria in the second position in Africa just after Uganda. Federal statisticians in Nigeria posited that Southeast Nigeria spent 44 billion Naira on alcohol consumption; coming behind only the South-South region of the country (Adebowale, 2019).
It is, therefore, clear that excessive intake of alcohol leads to alcoholism. Alcoholism is primarily a chronic and progressive deadly social disease related to the continuous consumption of alcoholic drinks, in which genetic, psychosocial, economical, and environmental factors are correlated to its development and manifestations (White, 2009). This is why Bier (1962) had earlier identified two primary types of alcoholics, which are; Type 1 or milieu-limited and Type II. Type I alcoholics start heavy drinking after the age of 25 years, often in response to setbacks, loses or other external circumstances. They possess personality traits such as shyness, anxiousness, loss of control, guilt, fear, are emotionally dependent, rigid, and slow to anger. Since alcohol reduces their anxiety levels, it serves as a positive reinforcement for continuous use and contributes to the development of alcohol dependence.
Type II alcoholics become heavy drinkers before the age of 25. They drink regardless of what is going on in their lives and have frequent fights and arrests. They do not usually experience guilt or loss of control over their drinking. However, they are impulsive and aggressive risk-takers, curious, excitable, quick-tempered, optimistic, and independent. Alcohol reinforces the feelings of euphoria, pleasant excitement, and often, abuse of other drugs (Bier, 1962). Other studies have classified alcoholism as Type A and Type B. In spite of the differences in name, Type A corresponds to Type I, while Type B is the same as Type II.
Generally, in spite of the type, alcoholic drinks have a lot of health consequences. When an alcoholic drinks too much, the immediate consequence is that he gets intoxicated. Intoxication consists of clinically significant maladaptive behavioral changes, such as inappropriate sexual or aggressive behavior, mood changes, and impaired judgment and social/occupational functioning (Ng’en Dimelu et al., 2011). Similarly, the excessive use of alcohol is the causal factor for more than 200 diseases and/or injuries (WHO, 2022).
Consequently, alcohol beverage acts as a depressant to the central nervous system, which effectively impairs all major body systems. Heavy drinking of alcoholic beverages may lead to hepatitis, which is characterized by inflammation and destruction of liver cells and cirrhosis, which produces progressive scarring of the liver tissues (Baer, 2004). Chronic consumption of alcohol has an adverse effect on the immune system by increasing susceptibility to infections such as pneumonia and tuberculosis. It also affects the brain cells by damaging them; impairing perception, judgment, and motor cells. Heavy drinkers’ white blood cells capability to fight infection is decreased and this causes anemia, interferes with blood clotting, and has even caused cancers, inflammation of the pancreas, increased risk of osteoporosis and stroke. Alcoholism may lead to sleep disorders and even untimely death (Mintz, 2012).
Alcohol is also dangerous to the reproductive tract causing birth defects and may lead to gynecological and obstetrical problems. Alcohol dulls the senses of taste and smell making heavy drinkers often skip meals and develop nutritional deficiencies, diarrhea, gastritis, peptic ulcer, alcohol pellagra, polyneuropathy, constipation, and even fatigue (Wechsler et al., 1995). It has been reported that children of alcoholics are vulnerable to learning disabilities, eating disorders, and addictive behavior. Experience has shown a devastating effect of alcohol upon morals, marriage, family life, and family income; sexual promiscuity is more prevalent after drinking because normal inhibitions are lowered. It has been estimated that three quarter of the cases of sexually transmitted infections (STIs), including HIV/AIDS, have been reported while the persons were under the influence of alcohol (Mintz, 2012). Generally, excessive alcohol intake among men is related with a variety of unfavorable health repercussions such as alcohol poisoning, blackouts, violence, deadly diseases, property damage, criminal repercussions that may endanger life longevity (Adekanye, 2021; Chikere & Mayowa, 2011; Kennard, 2021).
In spite of these consequences, there are various factors that push men to engage in alcoholism. According to Bier (1962), there are elements in rural societies that can lead a person to alcoholism or reinforce the behavior of excessive consumption of alcoholic beverages. These elements include setbacks (misfortunes), loses, pressure, stress, and boredom. In some cases, most rural dwellers who are predominantly farmers drink alcoholic beverages to calm down the work stress. WHO (2022) also pointed out that there are social factors that affect people’s alcohol consumption, and these include level of economic development, culture, social norms, availability of alcohol and enforcement of alcohol policies. It is also established that poorer persons experience greater health risks and social harm from alcohol consumption than rich persons.
Scholars have carried out studies on the health danger of alcoholism (Mintz, 2012), history of alcohol drinking (Dumbili, 2013; Obot, 2007), types of alcoholics (Mulamai, 2009), treatment of alcoholism (Wechsler et al., 1995) and alcohol policies (Nwosu, 2017). In spite of the various health problems that face males as heavy alcohol drinkers and coupled with the fact that for any advocacy campaign to be successful, it is necessary to understand why behavioral change is difficult; no serious study has been undertaken to get information from the men who consume alcohol (actual victims of alcoholism), about their beliefs and perceptions over their use/misuse of alcohol in Southeast Nigeria. It is as a result of these that the present study is focused on understanding the following: the rate of alcohol consumption by men in the study area; health consequences of alcoholism among men; level of awareness of the health consequences of alcoholism by men; and the factors that reinforce men’s alcohol consumption in the area.
Data and Method
Research Design
The study adopted descriptive survey design involving quantitative research methods. The survey design is relevant to the study because it is the commonest way of finding out what people think and do; their beliefs, their opinions, actions they have taken, action they are contemplating and so on (Onabajo, 2010). The survey research design involves surveying people and recording their responses for analysis (Cooper & Schindler, 2003). At the onset, random survey method involving the administration of questionnaire was used.
Research Population, Sample Size, and Sampling Procedure
As at the time of the study, there were 2,856 men within the community. Consequently, Taro Yamane (1967) proposed formula for estimating sample size was applied to determine the study sample. The formula is stated as follows:

where: n = sample size,
N = population,
e—margin of error,
1 = constant
Thus: n =
1+2,856 × (0.05)2
n =
7.1425
= 399.9
Therefore, n = 400
The formula yielded 400 samples, which represented about 14% of the entire population. Therefore, only 400 respondents participated in the study. It should be noted that Peretomde and Owojori have maintained that a sample size that is not <10% of the population is a good representation of the population. Quota sampling technique was used to select the participants that formed the sample size. Specifically, the study was conducted in a rural residential setting among the Ezeagu community of Southeast Nigeria. The Ezeagu community is composed of several villages: Akuchie, Amari, Amuofia, Enuagu, Anuogbe, Umuoyiwa, Onuoka, Umuagba, and Okpezi. The majority of the Ezeagu people can understand English language, although they do not necessarily speak English when in their locality. They predominantly speak Igbo language. The sample (n = 400) is made up of adult males within the age range of 16–68 years, with a mean age of 32.3 years.
Research Data and Instrument for Data Collection
Data collection took place between November 2021 and May 2022. Primary data are most suitable for a study of this nature. Therefore, a structured 54-item questionnaire having a modified 5-point Likert-type scale of strongly agreed, agreed; undecided, disagreed, and strongly disagreed was used to generate data. The questionnaire that was adopted from Nwosu et al. (2021) before it was modified has five sections: demographic characteristics of the respondents, rate of alcohol consumption by men, consequences of alcoholism on men’s health, men’s level of awareness of the health consequences of heavy alcohol consumption and factors that reinforce men’s persistent alcohol consumption. The instrument was first validated by three experts in the chosen area of study. Twenty copies of the questionnaire were used in a test–re-test reliability study. The sampling technique adopted for the study was quota sampling. The nine villages were involved and from each village 45 males were selected but 40 males were selected from Akuchie because it has a lesser population than other villages. From each village, five streets or footpaths were selected. From every street/footpath, every second compound was selected and from each compound, one adult male was selected. This selection continued until nine adult males were selected from each street/footpath. But at Akuchie, only eight streets/footpaths were selected and subjects were also selected as it was done in the other nine villages. In other words, the other eight villages produced 360 participants for the sample (i.e., 45 participants per village), while Akuchie produce only 40 participants bringing the total number of participants to 400.
All the selected participants were approached; the essence of the study was explained to them and they all agreed to take part in the study. They were asked to fill the informed consent form, which they did. Upon completing the consent forms, the participants were given copies of the self-designed questionnaire to fill. The researchers guided the participants throughout the survey; clarifying each question where necessary. They were also available to translate and/or explain unfamiliar terms to the participants. In some cases, the researchers read the items of the questionnaire aloud for illiterate participants. Each encounter was completed in about 50 min. All the 400 participants who took part in the survey returned their copies of the questionnaire, but only 369 were valid. The other 31 copies were discarded because those who filled them had never consumed alcohol.
Measurement of Research Variables
All the variables used in the study—rate of alcohol consumption, effect of alcohol on men’s health, men’s level of awareness of the consequences of alcoholism and factors that reinforce men’s persistent alcohol consumption—were measured using nominal scale—the 5-point Likert-type type rating scale. Specifically, the participants were asked to rate each one of the 9 items on rate of alcohol consumption scale (R), each one of the 14 items on the extent alcoholism affects men’s health scale (E), each one of the 19 items on men’s level of awareness of health consequences of alcoholism scale (A) and each one of the 12 items on factors that reinforce men’s persistent consumption of alcohol scale (F). The responses were evaluated and used to compute the descriptive statistics (frequency, weighted percentage, and percentage of total agreement) for each of the variables.
Data Analysis
SPSS was used to process and analyzed the responses from the questionnaires. To this effect, descriptive statistics in the form of frequency distribution was used to interpret the data, while the Chi-square statistics was employed in the testing of the hypotheses of the study. The hypotheses for the study were tested at 0.05 level of significance.
Ethical Approval and Consent to Participate
The research proposal was submitted to the Research and Ethics Committee of a university in Nigeria. After careful scrutiny, the committee gave approval for the research to be carried out since it does not pose any harm to the participants or the society. The participants (400) were also contacted and briefed about the essence and procedure of the research. Out of the 400 subjects that fell into the sample, having fulfilled the initial inclusion criteria, only 369 persons are qualified to take part in the research because the remaining 31 had never taken alcohol. As part of the ethics regulation, the participants were assured that their participation and their views during the research must be treated with utmost confidentiality. It was also agreed that their real names or anything that will link them to research will not be used in the report of the research.
Results
The researchers collected all 400 copies of the distributed questionnaires. First-level screening revealed that 31 (7.8%) participants never took alcohol. Therefore, their responses were discarded. This left us with only 369 (92.2%) copies of the questionnaire, and these were used for the data analysis using SPSS, after which inferences were made.
Table 1 reveals that 290 (78.6%) of the surveyed respondents agreed that most men in their area drink alcohol every day, and 209 (56.7%) of the respondents also said that most men in the area cannot do without alcohol. The surveyed population also revealed that most men began drinking alcohol as boys. Data also showed that men drink alcohol not only during ceremonies, but the majority drink mostly during the weekend. Some of the respondents (250 or 67.8%) believed that majority of the men drink different types of alcohol.
Rate of Alcohol Consumption by Men.

Source. Fieldwork 2022.
Note. N = total number of participants; A = agreed; SA = strongly agreed; UD = undecided; DA = disagreed; SDA = strongly disagreed; PA = percentage of agreement.
The Consequences of Alcohol Consumption on Men’s Health
The data presented in Table 2 also reveal that 262 (71%) of the respondents believed that men tend to be more aggressive after alcohol intake. Another 260 (70.5%) of the participants said that they usually lose concentration after alcohol intake. Other respondents (234 or 64.5%) pointed out that they do experience low sexual performance when they drink alcohol excessively. They believed that alcohol consumption does affect their libido negatively. Yet, other participants (200 or 54.2%) believed that they do experience constipation after taking alcoholic drinks and another 244 (66.1%) of the respondents said that alcohol makes them irrational especially in decision taking. According to the resultant data, others experience insomnia (237 or 64.2%), frequent urinating (289 or 78.3%), and feverish condition when they consume alcoholic drinks (89 or 24.1%).
The Extent to Which Alcohol Consumption Affects Men’s Health.
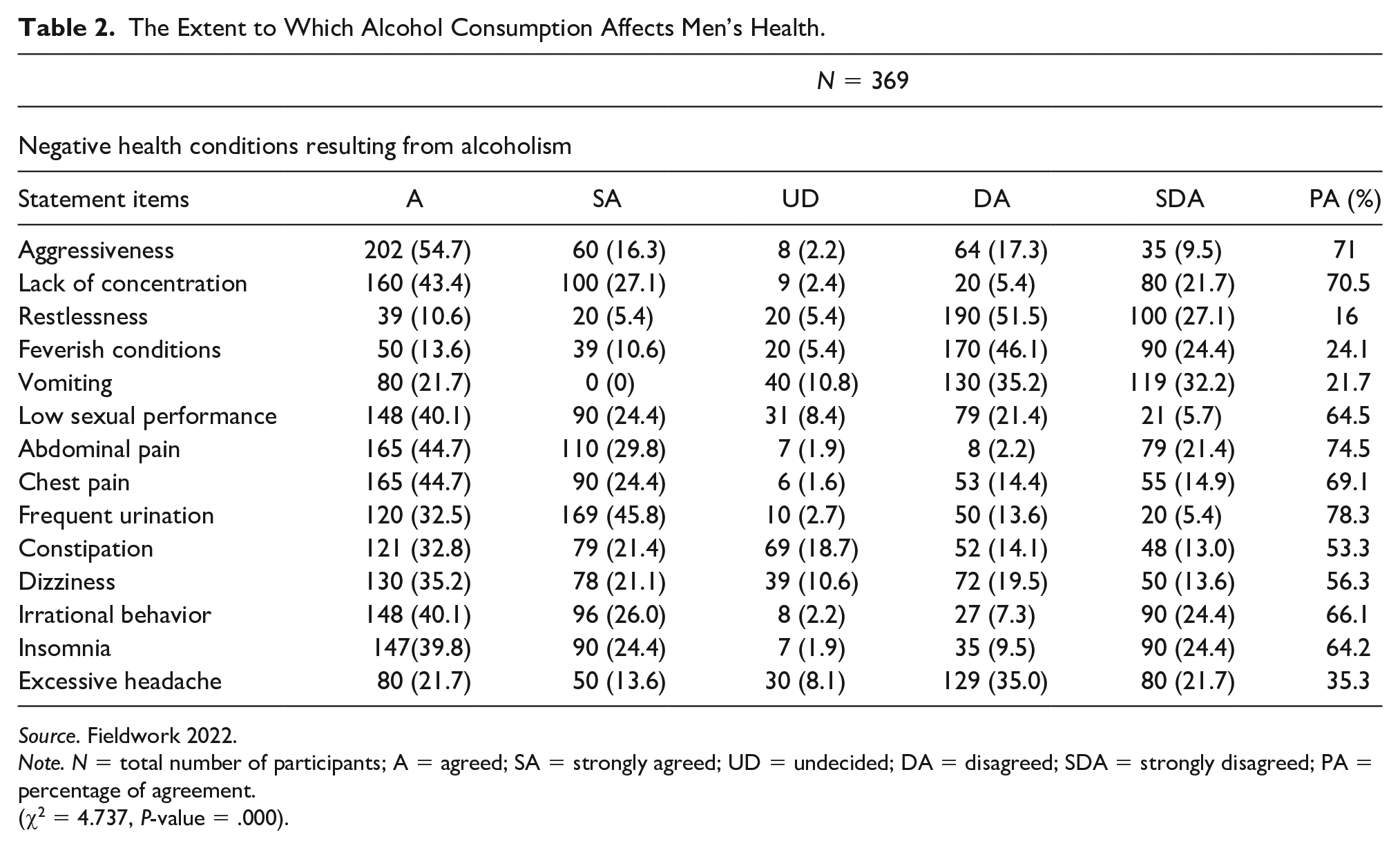
Source. Fieldwork 2022.
Note. N = total number of participants; A = agreed; SA = strongly agreed; UD = undecided; DA = disagreed; SDA = strongly disagreed; PA = percentage of agreement.
(χ2 = 4.737, P-value = .000).
In terms of the relationship between men’s ill-health and alcohol consumption, the result from the regression test analysis indicates that χ2 = 4.737, while P-value = 0.000. Here, it can be seen that the P-value is less than the level of significance (0.05). As a result, we conclude that alcohol consumption has a significant relationship with the ill-health of male consumers. Therefore, binge drinking of alcohol can lead to ill-health in men.
The Extent of Men’s Awareness of the Health Consequences of Alcoholism
The study assessed the level of men’s awareness of the health consequences of consuming alcoholic beverages. The data presented in Table 3 indicate that most men are aware that consumption of alcohol can cause intoxication (365 or 98.9%), aggressiveness (264 or 71.5%), lack of concentration (272 or 73.8%), vomiting (270 or 73.2%), sexual dysfunction (281 or 64.5%), abdominal pain (234 or 63.4%), frequent urination (289 or 78.3%), constipation (248 or 67.2%), dizziness (254 or 68.8%), and insomnia (247 or 66.9%). It was also found from the resultant data that majority of the participants are not aware that consumption of alcohol can lead to other health problems such as excessive headache, vehicular accident injury, sexually transmitted diseases (STDs), liver diseases, kidney diseases, and even death. If we put together the number of those that were completely unaware with those who were undecided, we will get the following percentage of participants that were really unaware of the health consequences of alcohol consumption: excessive headache (239 or 64.8%), vehicular accident injury (299 or 66.2%), STDs (349 or 94.6%), liver diseases (335 or 90.8%), kidney diseases (303 or 82.1%), and death (352 or 95.4%).
Men’s Level of Awareness of Health Consequences of Excessive Alcohol Consumption.

Source. Fieldwork 2022.
Note. N = total number of participants; A = agreed; SA = strongly agreed; UD = undecided; DA = disagreed; SDA = strongly disagreed, percentage of agreement; STDs = sexually transmitted diseases.
This result shows that the participants are aware of minor health conditions that result from alcohol consumption. Most of them are not aware of the chronic health challenges that do result from alcohol consumption. Almost all the respondents (352 or 95.4%) were not even aware that alcohol consumption could lead to death. Generally, the level of awareness can be rated as low.
Socio-Cultural Factors That Reinforce Men’s Alcohol Consumption
The data presented in Table 4 revealed that 269 (72.9%) of the respondents drink alcohol because their family members take alcohol. Also many of the men in Ezeagu (280 or 75.9%) have been influenced into taking of alcohol by friends. The survey also showed that a cumulative of 270 (73.2%) respondents drink alcohol because of peer group influence. It is clear that most men in the study area drink alcohol because of social factors such as the nature of their job, ceremonies that involve alcoholic drinks, and even to please friends and spouse.
The Extent to Which Socio-Cultural Factors Contribute to Men’s Persistent Alcohol Consumption.

Source. Fieldwork 2022.
Note. N = total number of participants; A = agreed; SA = strongly agreed; UD = undecided; DA = disagreed; SDA = strongly disagreed, percentage of agreement.
(Social Factors: χ2 = 6.722, P-value = .000. Cultural factors: χ2 = 5.001, P-value = .000).
The data presented in Table 4 revealed that most men take alcoholic drinks mostly when they are exposed to certain cultural events such as traditional marriage (280 or 75.9%). However, few number of the participants take alcoholic drinks because of certain cultural events such as child naming (150 or 40.7%), praying to the gods/ancestors (90 or 24.4%) and when pouring libation (97 or 26.3%). The result shows that the cultural factors that strongly force men to continue drinking alcohol are traditional marriages, traditional festivals (such as new yam festival), and traditional kingship/chieftaincy enthronements. This may be due to the fact that alcoholic drinks form the nucleus of such events.
The result of the regression analysis also revealed that in terms of the relationship between social factors and men’s persistent drinking of alcohol, χ2 = 6.722, while the P-value = 0.00. Again, the P-value is less than the level of significance (0.05). As such, social factors within the society have a significant relationship with men’s inability to quit drinking alcohol.
Similarly, it was found that in terms of the relationship between cultural factors and men’s inability to quit drinking alcohol, χ2 = 5.001, while the P-value = 0.000. The result shows that the P-value is less than the level of significance (0.05). Therefore, cultural factors have a significant relationship with men’s inability to quit drinking alcohol. As such, we resolve that cultural factors have remained some of the major reasons why men do not want to quit alcohol consumption.
Discussion
This study set out to determine the rate of alcohol consumption in Ezeagu community. The resultant data revealed that most men in Ezeagu community take alcohol daily and they started drinking alcoholic beverages before the age of 18 years. It was also found that most men cannot do without alcohol. This means that most men in the area are heavy drinkers. This supports the view of Adekanye (2021); that men are prone to excessive alcohol intake. This is also in line with the Type 1 milieu-limited type of alcoholism, which states that heavy drinking starts early in life often in response to set-backs, loses, pressure, stress, or other external circumstances (Bier, 1962). This statement could be relational as result of the fact that most of the respondents were farmers who toil the soil every time. They tend to use the alcoholic drinks to calm down the work stress. Again, they were peasant farmers with low incomes. As a result, they take more of local dry gin and palm wine that are cheap and readily available within their area to reduce the pressure of economic difficulties. This result is a slight shift from the idea of Dumbili (2013), who was of the view that heavy drinking is a result of the influence of the media, advertising, sophisticated marketing, and lack of alcohol policy. Many of the men in Ezeagu are not educated and do not have access to the media and sophisticated marketing, and as such, heavy drinking was the result of some external factors such as stress from their jobs, boredom during the weekends, and other social and cultural factors. Similarly, the result also indicated that most of the men drink alcohol because their friends drink and they do not want to appear odd when they are in the midst of friends. This result also aligns with the social learning theory of Bandura (1977), which posit that people learn from one another, via observation, imitation, and modeling. However, the result did not support the report of Yasmeen (2022) that alcohol consumption among men is reducing. It also shows that, while alcohol consumption among men dropped during COVID-19 pandemic (Tucker, 2022), it has actually begun to increase again.
The study also investigated the health consequences of alcoholism among men in Ezeagu community, Southeast Nigeria. The result revealed that the health consequences of alcohol consumption in the area are aggressiveness, lack of concentration, sexual dysfunction, abdominal/chest pain, constipation, frequent urination, irrational behavior, and insomnia. This result is in line with the report of Sampson and Davis (2018) and Kennard (2021) when they pointed out that frequent drinking of excess alcohol is harmful to health and that alcohol does have an impact on every system in the body. According to them, when the human body takes in excess alcohol than it can metabolize, the excess alcohol accumulates in the bloodstream. Therefore, when the heart circulates this alcohol-stained blood throughout the body, it causes changes in the chemistry of the body and alters the normal functioning of the body’s system. Sampson and Davis (2018) also posited that apart from these few health conditions identified by the study, alcohol has been reported to contribute to at least 60 different health conditions in different parts of the world. It is believed that few health conditions identified in the area by the participants could be as a result of their level of awareness.
Based on this, the study also set out to determine the level of awareness of the people about the health implications of excessive consumption of alcohol. Data revealed that most men are aware that excessive alcohol could lead to intoxication, aggressiveness, lack of concentration, vomiting, sexual dysfunction, abdominal/chest pain, frequent urination, constipation, dizziness, and insomnia. This is similar to the findings of Eze et al (2017) who studied the level of awareness of health consequences of alcohol among secondary school students. They found that the students are not fully aware of the major and more severe consequences of excessive alcohol consumption. In the case of this study, the participants are only aware of minor health conditions that result from excessive alcohol consumption. In other words, they are not aware that excessive alcohol consumption could cause liver disease, alcoholic hepatitis, cancer diseases, ulcers, heartburn, gastritis, immune system dysfunction, brain damage, osteoporosis, heart/cardiovascular disease, accidents/injuries, gout, kidney disease, and even death. These health conditions have earlier been highlighted as major dangers resulting from alcohol consumption (Sampson & Davis, 2018; WebMD, 2019). This finding is in line with the observation of Coomber et al, (2017) when they said that most alcohol consumers lack sufficient knowledge of the real and potential negative effects of alcohol use. However, the result is a departure from the views of Ferreti et al (2018), when they noted that consumers who get high with alcohol reported greater awareness about its negative effects. In addition, Shmerling (2018) pointed out that alcohol consumption can also result in high blood pressure, dementia, homicide/suicide, lapses of judgment, risky sexual behavior, anxiety, and alcohol poisoning. He also noted that excessive alcohol intake can cause health problems, not only for the drinker but also for their family, friends, co-workers, and employers. Similarly, WHO (2018) observed that about three million deaths occur in different parts of the world annually due to the harmful use of alcohol. This represents 5.3% of all deaths worldwide. However, this level of awareness is lacking among the people studied. In other words, their level of awareness of the negative consequences of excessive alcohol consumption is insufficient and can, therefore, be rated as low.
From all indications, men are aware of some of the dangers of alcohol consumption, yet they continue to take alcohol, even daily. Therefore, the study tried to find out why men could not quit consuming alcoholic beverages in spite of the little consequences they know about. The study revealed that both social and cultural factors prevent men from quitting alcohol intake. These factors include the influence of extended family, friends, age-grade activities, ceremonies, and traditional marriage/festivals. The extended family influences continued drinking of alcohol because most often, people bring alcoholic drinks to the family and it is expected to be shared by members of the extended family. In other words, the presence of free drinks in the family makes one vulnerable to drinking alcohol. In some cases, if one refuses to take the drink, others may interpret it differently; that the person is not happy with other members of the family. Similarly, social ceremonies and traditional festivals also make alcoholic drinks available most frequently and enticing to men. This supports the postulation made by Odejide (2006) when he noted that even though there is no written rule prohibiting women from drinking alcohol in traditional settings, the consumption of alcoholic drinks is exclusively reserved for men. According to Odejide (2006), this is mostly because alcohol plays a complex role in religious and traditional festivals/rituals that is superintended by men. The results also support the views of WHO (2022), when it noted that there are social factors that influence the people’s use of alcohol. In other words, such ceremonies, festivals, and rituals expose men to the arena of alcohol more often. Again, since women and children are not always permitted to drink alcohol without the strict supervision of an adult male, the men always have a lot of alcoholic drinks available for themselves.
The study has shown that there is a strong relationship between socio-cultural factors and men’s persistent drinking of alcohol. In other words, these factors have been part of the major reasons why men do not quit drinking alcohol. This is contrary to the submission of CARF International (2017) that people find it difficult to quit alcohol consumption because of withdrawal symptoms. In addition to these socio-cultural factors, the low level of the people’s awareness of the health implications of excessive intake of alcohol is another major factor that has made men not to quit drinking excessive alcoholic beverages. Their knowledge of the adverse health conditions associated with excessive alcohol intake is too limited and not strong enough to deter them from excessive alcohol consumption.
Limitations of the Study
The study was not able to carry out medical checkup on the participants to determine their state of health. The results were based on self-reports from the male drinkers. The study also did not assess the changing patterns in men’s consumption of alcohol in the study area. Again, the research only assessed the socio-cultural factors but did not cover psychological and economic factors that reinforce alcohol consumption among men.
Conclusion
The rate of alcohol consumption in the study area is quite high. Most of the men take alcoholic drink every day and some cannot do without drinking alcohol. This has actually posed a great danger to their health. This is because the study has established that there is a strong relationship between excessive alcohol intake and ill-health. A lot of diseases have been identified to result from excessive use of alcohol. Unfortunately, the people’s level of awareness about these health problems that result from drinking alcohol is quite low and narrow. People are not aware of major health problems that result from consuming alcohol; such as liver disease, kidney disease, cancers, gastritis, immune system dysfunction, brain damage, seizures, infections sleep disorders, death among others. This in effect means that most men are not fully aware of the dangers that they are exposing themselves to when taking alcoholic beverages. As a result, low level of awareness and socio-cultural factors are the major reasons why men find it difficult to quit drinking alcohol.
Noting the low awareness level of the people concerning the health implications of alcohol consumption, the study recommends that it is necessary to raise the awareness level of health problems resulting from excessive use of alcohol. There should also be qualitative alcohol policies in Nigeria. Traditional rulers and community opinion leaders should also help to ensure that men are not constantly exposed to alcoholic drinks by adjusting some of their cultural practices to involve less alcoholic drinks. This is because most men over drink whenever free drinks are available. There should be a strong effort to provide accessible and affordable treatment for people, especially men, who have developed alcohol use disorders. This will be a success if there is provision for screening and brief intervention programs for hazardous and harmful drinking at health facilities. Generally, there is an urgent necessity to regulate and restrict the availability of alcohol through the formulation of an effective policy on alcohol use. All these will help to save lives and lead toward the achievement of the health target 3.5 of the sustainable development goals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.