
Abstract
Objective:
Alcohol consumption during pregnancy can cause many major severe illnesses to both mothers and their offspring. Despite this, many pregnant women consume both homemade and manufactured alcoholic beverages. We conducted this study to assess the prevalence and determinants of alcohol consumption among pregnant women in Gozamin district, Amhara, Ethiopia, in 2020.
Methods:
Community-based cross-sectional study was employed from 1 to 30 November, 2020. The participants were recruited using a stratified multi-stage sampling technique. A structured and pretested interviewer-administered questionnaire was utilized for data collection. The collected data were entered into Epi-data Version 3.1 and exported to SPSS Version 25 for further analysis. The model fitness was checked by Hosmer and Lemeshow’s goodness of fit test. Then, logistic regression models were considered to determine the associations of independent variables with the outcome variable. Variables with p < 0.25 in bivariable logistic regression were considered for multivariable logistic regression. Finally, variables with p < 0.05 in multivariable logistic regression were considered as determinants of alcohol consumption.
Result:
A total of 555 pregnant women participated in this study, making the response rate of 97.4%. The prevalence of alcohol consumption among the participants was 45.6% (95% confidence interval = 41.4–49.2). The determinants of alcohol consumption among the participants were highest wealth index (adjusted odds ratio = 3.21; 95% CI = 1.68–6.14), pre-pregnancy alcohol consumption (adjusted odds ratio = 3.67; 95% confidence interval = 2.36–5.71), poor social support (adjusted odds ratio = 3.08; 95% confidence interval = 1.60–5.94), and unplanned pregnancy (adjusted odds ratio = 1.66; 95% confidence interval = 1.04–2.66).
Conclusion:
In this study, the prevalence of alcohol consumption was high among the pregnant women. Our findings suggest introduction of policies and interventions that can help reduce alcohol consumption during pregnancy. The health education priority should be creation of awareness about the negative health impacts of alcohol on the health of pregnant mothers and their offspring.
Introduction
Alcohol plays an important role in social bonding and engagement. While many people consider alcohol consumption as a means of feeling pleasure. 1 However, it can cause many severe illnesses and premature deaths especially among socioeconomically disadvantaged populations. 2 The adverse effects of alcohol consumption are stronger when consumed by pregnant women. 3 Alcohol can readily cross the placental barrier and negatively affect the developing embryo and fetus. 4 Thus, its consumption during pregnancy can cause irreversible damages to the fetus along with a range of birth anomalies, known as fetal alcohol spectrum disorder. 5 Other consequences of antenatal alcohol consumption are miscarriage, stillbirth, premature birth, congenital malformation, low birth weight, and intrauterine growth restriction. Alcohol exposure during pregnancy can also cause mental impairments and behavioral disorders during infancy period or even later in life. 6 For these reasons, the World Health Organization and Centers for Disease Control and Prevention have indicated that there is no safe type, amount, and time of alcohol consumption during pregnancy. 1
The global prevalence of alcohol consumption during pregnancy has been estimated as high as 9.8%. 7 According to the previous studies, the prevalence of alcohol consumption among pregnant women ranges from 2.2% in Equatorial Guinea to 80% in Ireland.8,9 In Ethiopia, 8.1%–37.1% of women consume alcohol while they are pregnant.10,11 Most alcoholic beverages in Ethiopia (namely, Tella, Tej, Areki, and wine) are prepared in a traditional way in which the amount of alcohol content is not exactly determined. They are being consumed by many people during different events (i.e. Mehabers, ceremonies, and holidays), commonly and on a daily basis during meals.12,13
It has been suggested that the psychoactive nature of alcohol makes people dependent. 14 Few facility-based studies in Ethiopia revealed that having an alcohol-consuming partner, being married and unemployed, having unplanned pregnancy, and a history of abortion can determine the likelihood of alcohol consumption during pregnancy.10,15–17 However, to our knowledge, there is no community-based study conducted at Gozamin district in Ethiopia to evaluate prevalence and determinants of alcohol consumption in all pregnant women including those who did not visit health care institutions. A community-based research on such important public health problem is vital mainly in the district where health care service utilization is poor. 18 Therefore, the current study aimed to assess the prevalence and determinants of alcohol consumption among pregnant women in Gozamin district, Amhara, in Ethiopia.
Methods
Study area and period
The study was conducted in Gozamin district from 1 to 30 November, 2020. Gozamin is located in the East Gojjam zone, which is 265 and 299 km far from Bahir Dar (the city of Amhara regional state) and Addis Ababa (the capital city of Ethiopia), respectively. The district has 32 kebeles (the smallest administrative unit in Ethiopia). According to the district’s 2020–2021 report, the total population was 164,816, of which 83,232 were females. A total of 5554 pregnant women had antenatal care visits at least once within the six health centers in the district. 19
Study design
This was a community-based cross-sectional study.
Study population
All pregnant women lived in the Gozamin district during the study period were considered for the purpose of this study.
Eligibility criteria
Inclusion criteria
All pregnant women who lived in Gozamin district at least for 6 months and were available during the data collection period were eligible to participate.
Exclusion criteria
Pregnant women who could not communicate due to critical medical or mental illness were excluded from the study.
Sample size
The required sample size for this study was calculated using a single population proportion formula, considering the 34% prevalence of alcohol consumption among pregnant women reported in an earlier study conducted in Bahir Dar town 16

In the formula, n = sample size, p = proportion of alcohol consumption (0.34), q = 1–p, d = margin of error (0.05) and Z = 1.96 at 95% confidence interval (CI). Based on the above formula, we calculated to need 345 participants. Due to the multi-stage sampling technique employed, we multiplied this number by 1.5 to consider the design effect and assure the representativeness of the participants. Therefore, the final sample size considering a 10% non-response rate was calculated to be 570 pregnant women.
Sampling procedure
We used multi-stage sampling technique. First, two urban and eight rural kebeles (30%) were selected from six urban and 26 rural kebeles of the district through a simple random sampling technique. We approached the health extension workers in these kebeles to access potential study participants. Finally, participants from the selected kebeles were recruited using a systematic random sampling technique (Figure 1).

Schematic representation of the sampling procedure for alcohol consumption and its determinants among pregnant women in Gozamin district, Amhara, Ethiopia, 2020.
Alcohol consumption
Use of any amount and type of alcohol at least once during the last pregnancy. Respondents who answered “Yes”’ to the question “Have you ever consumed alcohol during the last pregnancy?” were considered as they consumed.20,21
Data collection tools
Alcohol use Disorder identification test
We used a 10-item alcohol use screening instrument to measure the frequency of alcohol consumption and alcohol use disorder. The first three questions (1–3) explore the quantity and frequency of alcohol consumption. Those who answered “never” to the first question on the tool, were considered alcohol non-user. 22 The second three questions (4–6) explore signs of alcohol dependency and the last four questions (7–10) explore other alcohol-related problems. Response options for each item ranges from 0 to 4 resulting in a total maximum score of 40. A score of 1–7 indicates social drinking, a score of 8–15 indicates hazardous drinking, a score of 16–19 indicates harmful drinking and a score of 20 or above indicates alcohol dependence problem. 22 To make it more appropriate, the last 12 months after confirming the pregnancy was taken as the time of alcohol use disorder identification test (AUDIT).
Social support during pregnancy
We used Oslo Social Support Scale (OSSS-3) during pregnancy and categorized social support as poor support (scored 3–8), moderate support (scored 9–11), and strong support (scored 12–14). 23
Violence
According to abuse assessment screen (AAS) during pregnancy, if the participants responded “yes” to at least one of the three physical or sexual abuse questions, the violence was indicated. 24
Mental distress
An Ethiopian validated Self-Reporting Questionnaire (SRQ-20) was used to screen mental distress. 25 It helps to diagnose mental distress in primary health care settings and communities of low-income countries with a cut-off score of 7 and above indicating mental distress.26,27
The wealth index
This tool is a composite measure of a household’s cumulative living standard. The wealth index was calculated using the data collected on a household’s ownership of selected assets using principal component analysis. Wealth quintiles were compiled by assigning the household score to each usual (de jure) household member, ranking each person in the household members by her or his score, and then dividing the distribution into five equal categories, each comprising 20% of the members. Finally, the household’s wealth index was categorized into 1 = poorest, 2 = poor, 3 = middle, 4 = rich, and 5 = richest.28,29
We confirm that we obtained permission from the respective copyright holders to use all the above-mentioned tools in this study.
Variables
Dependent variable
Alcohol consumption during pregnancy.
Independent variables
The independent variables were grouped as follows:
Socio-demographic variables
Age, religion, marital status, number of children, ethnicity, educational status, occupation, having an alcohol-consuming partner, area of residence, and wealth index.
Obstetric and gynecological variables
Type of pregnancy (planned or unplanned), gravidity, parity, being informed about the teratogenic effect of alcohol consumption during pregnancy, gestational age, number of antenatal care visits for the current pregnancy, and history of miscarriage.
Psychiatric, psychosocial, and behavioral variables
Mental distress, smoking, pre-pregnancy alcohol consumption, a societal belief of alcohol consumption during, antenatal care visit, having information about the teratogen of alcohol consumption out of health institutions, social interaction/situation in which pregnant women mostly consume alcohol, violence, and social support.
Procedure
The data were collected through structured interviews using pre-tested Amharic version of the standardized questionnaires.15,16,23–27,30–34 A total of six diploma degree midwives collected the data and two registered nurses supervised the study progress and data collection procedure. National coronavirus disease 2019 (COVID-19) protocols were implemented throughout the study.
Data quality control
The questionnaires were prepared in English and translated into Amharic and back to English by the language experts. Two days of training and orientation about the tool and data collection procedure were provided to all data collectors and supervisors. The questionnaires were tested on 29 pregnant women (5% of the total sample size) in non-selected kebeles within the district, 1 week ahead of the actual data collection period. Then, unclear questions and ambiguous words were modified and corrected. Finally, the data were collected under close supervision of the registered nurses. Every evening after data collection, each questionnaire was reviewed and cross-checked for completeness, accuracy, and consistency by the supervisors and the investigators. The necessary corrective measures were taken before the next data collection day.
Statistical analysis
Data were coded and entered using Epi-Data version 3.1 and exported into SPSS version 25 for further data cleaning and analysis. The model fitness was checked using the Hosmer and Lemeshow goodness of fit test. Descriptive statistics of continuous variables were summarized using a median and interquartile range. Likewise, the descriptive results for categorical variables were presented using proportions and frequency and presented using graphs and tables. The binary logistic regression was conducted to test the association of each independent variable with the dependent (outcome) variable. Then, variables with a p-value < 0.25 were considered for the multivariable logistic regression analysis. Finally, a p-value < 0.05 in the multivariable logistic regression analysis was considered as statistically significant. The results of the regressions were presented using an odds ratio with 95% CI.
Results
Socio-demographic characteristics of the participants
A total of 555 pregnant women participated in this study, yielding a 97.4% response rate. The median age of the participants was 25 years (interquartile range (IQR) = 9). Almost all (99.6%) participants were Orthodox Christianity followers. Similarly, the majority (92.8%) of participants were from the rural community (Table 1).
Socio-demographic characteristics of pregnant women participated on alcohol consumption and its determinants in Gozamin district, Amhara, Ethiopia, 2020.

Single, divorced, and widowed.
Obstetrical and gynecological characteristics
More than two-thirds (77.5%) of the reported pregnancies was planned. Nearly, one-fourth of the participants were gravida 2 (26.8%) or primigravida (23.6%). About 89 (16%) pregnant women reported they had no antenatal care visit during their current pregnancy (Table 2).
Obstetrical and gynecological characteristics of pregnant women participated on alcohol consumption and its determinants in Gozamin district, Amhara, Ethiopia, 2020.

ANC: antenatal care.
Psychiatric, psychosocial, and behavioral characteristics
Among the participants, 95 (17.1%) pregnant women reported having mental distress. More than two-thirds (68.6%) of pregnant women had a history of pre-pregnancy alcohol consumption, 65 (11.7%) of them were victims of physical or sexual violence, and almost half (52%) of them had moderate level of social support (Table 3).
Psychiatric, psychosocial, and behavioral characteristics pregnant women participated on alcohol consumption and its determinants in Gozamin district, Amhara, Ethiopia, 2020.

ANC: antenatal care.
Alcohol consumption
According to our findings, 253 (45.6%) pregnant women drank alcohol during the current pregnancy, of whom 150 (59.3%) reported to become drunk in ceremonial events (mehabers) (Figure 2). All pregnant women who consumed alcohol had an AUDIT score of 1–7, indicating that none of them were hazardous, harmful, or alcohol-dependent drunker.
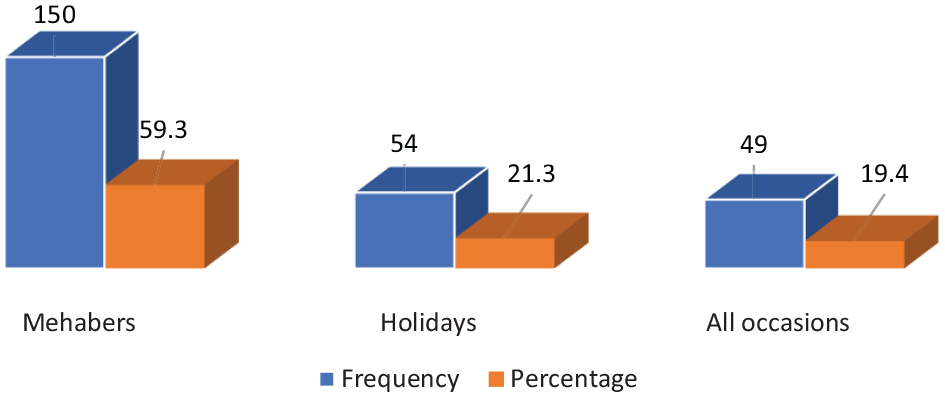
Shows the time when pregnant women consumed alcohol in Gozamin district, Amhara, Ethiopia, 2020.
Determinants of alcohol consumption
In the bivariable logistic regression analysis, marital status, wealth index, residence, pre-pregnancy alcohol consumption, type of pregnancy, and social support were associated with alcohol consumption during pregnancy. However, in the multivariable logistic regression, only wealth index, pre-pregnancy alcohol consumption, type of pregnancy, and social support were significantly associated with alcohol consumption among pregnant women. Based on the multivariable logistic regression results, compared to the poorest economic group, the odds of alcohol consumption among pregnant women were greater in richest, rich, middle, and poor wealth index as 3.21 (95% CI = 1.68–6.14), 2.96 (95% CI = 1.55–5.64), 5.15 (95% CI = 2.72–9.75) and 7.39 (95% CI = 3.84–14.23), respectively. Also, the odds of consuming alcohol during current pregnancy was 3.67 times (95% CI = 2.36–5.71) greater in women who consumed alcohol during their pre-pregnancy period. Pregnant women who had poor social support were 3.08 times (95% CI: 1.60–5.94) more likely to consume alcohol compared to pregnant women who had strong social support. In addition, pregnant women whose pregnancy was unplanned were 1.66 times (95% CI: 1.04–2.66) more likely to consume alcohol than those whose pregnancy was planned (Table 4).
Determinants of alcohol consumption among pregnant women in Gozamin district, Amhara, Ethiopia, 2020.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
1.00 = reference category.
Significant at p-value < 0.05.
Significant at p-value < 0.001.
Discussion
This study showed that the prevalence of alcohol consumption among pregnant women was 45.6%. This finding supports the reports of previous studies conducted in Ghana Accra (48%) 35 and Ukraine (43.6%). 36 The possible reasons for the similar reported prevalence may be similar socio-economic status of the participants and also the use of similar study design. Similar to the reports of the study in Ghana Accra, the majority of our participants indicated the main reason for antenatal alcohol consumption was attending social events. 35 However, greater prevalence of alcohol consumption during pregnancy has been reported in other countries, such as Australia (64.3%), 37 Europe (including Poland, Russia, and France) (70%), 38 Britain (53%), 39 and Ireland (82%). 40 The cross continents social norms, regulations, and the data collection techniques might have contributed to this observed difference. For example, in a multinational study in Europe, 38 the data were collected anonymously online so the possible social desirability bias could be avoided. In addition, better economic status and smoking habits were found to be attributes of general alcohol consumption in the Europe. 41 The difference in the tool of measurement and sample size may have also contributed to the difference prevalence rates. The multinational study in Europe did not use standardized tools, 38 whereas the study in Ireland considered a larger sample size (18,000 pregnant women). 40 The socio-economic status difference might also be the possible justification for the difference.
On the other hand, the prevalence of alcohol consumption among pregnant women in this study was greater than other studies conducted in Ethiopia (30.2%), 42 the Netherlands (22%), 32 Sweden (6%), 31 Korea (16.4%), 43 Brazil (15.2%), 44 and the United States (30.3%). 30 The possible reason for the lower prevalence in Sweden might be the different study populations, in which only pregnant women with a gestational age more than 18 weeks were included. 31 Also, unlike our study, previous studies were conducted at the facility or country levels.
In our study, we assessed determinants of alcohol consumption among pregnant women in the Gozamin district. According to the multivariable logistic regression wealth index, pre-pregnancy alcohol consumption, type of pregnancy, and social support were found statically significant factors of alcohol consumption among pregnant women.
Women with the richest, rich, and middle wealth index were 3.21, 2.96, and 5.15 times more likely to consume alcohol compared to pregnant women in the poorest wealth index, respectively. This result corroborates findings from a study conducted in the United States. 30 One potential explanation could be the richest women are more likely to be able to afford and consume different types of alcohol. Also, women who consumed alcohol in the pre-pregnancy period were 3.67 times more likely to consume alcohol during their pregnancy period. This finding supports results of the studies conducted in Ethiopia10,15 and Sweden. 31 It has been suggested that women who consume alcohol during the pre-pregnancy period may not be able to stop drinking abruptly during pregnancy due to its addicting effect. 14
We also showed that pregnant women who had poor social support were 3.08 times more likely to consume alcohol during pregnancy compared to those who had strong social support. Similar results were found from earlier studies conducted in Addis Ababa, 15 Sweden, 31 and the United States. 30 Another study conducted among students demonstrated that higher social support reduced alcohol consumption. 2 It is assumed that women with poor social support may be more worried about their lives, survival, employment, and social coexistence, and they use alcohol as a coping mechanism to alleviate their anxiety. According to our findings, unplanned pregnancy was a significant risk factor for increasing antenatal alcohol consumption, which supports the reports of previous studies conducted in Ethiopia,10,16 New Zealand, 45 and the United States. 30 A meta-analysis study has already revealed that women whose pregnancies are unplanned are more likely to present risky and unhealthy behaviors before and during pregnancy and to be more careless about their pregnancy outcomes. 46
Strength and limitations of the study
This study had its limitations. Due to resource constraints, we could not consider alcohol biomarker tests. This was a great challenge in which the extent each participant consumed was not determined. Another limitation of our study was potential recall and social desirability bias by the participants. Moreover, the measurement instruments validation other than pretesting was not conducted, and the psychometric proprieties of the participants were not measured. Despite these, our study provides unique results as there is no similar study conducted at the community level in the country. Therefore, findings of our study can be used by policy makers and educators to update training programs for pregnant women and provide solutions on the problem to reduce alcohol consumption during pregnancy.
Conclusion and recommendation
In this study, almost half of the women consumed alcohol during pregnancy. The determinants of alcohol consumption among pregnant women were wealth index, pre-pregnancy alcohol consumption, type of pregnancy, and social support. Thus, the government and other stakeholders in the study area should work on awareness creation about the potential health impacts of alcohol consumption during pregnancy to the community. Researchers are also recommended to conduct alcohol consumption using biomarker tests.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221130903 – Supplemental material for Alcohol consumption and its determinants among pregnant women in Gozamin district, Amhara, Ethiopia, 2020
Supplemental material, sj-docx-1-smo-10.1177_20503121221130903 for Alcohol consumption and its determinants among pregnant women in Gozamin district, Amhara, Ethiopia, 2020 by Mulatu Mengaw Abetew, Addisu Alehegn Alemu, Haymanot Zeleke, Asteray Assmie Ayenew, Fikreselassie Getachew Aynalem, Getachew Mullu Kassa and Marjan Khajehei in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express their deepest heartfelt appreciation to the Debre Markos University for sponsoring this study. Moreover, their special thanks go to the study participants.
Author contributions
All authors were involved in the conception, design, analysis, interpretation, drafting of the manuscript, and manuscript editing. Finally, the authors read and approved the manuscript before submission.
Availability of data and materials
The data utilized in this are found from the corresponding authors upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical clearance was obtained from the Ethical Review Committee (ERC) of Debre Markos University College of Health Sciences (approval number/HSC/R/C/Ser/Co/93/11/131). The ethical clearance was submitted to the Gozamin district health office, then the office wrote an official letter of permission to health facilities. The data were collected anonymously and kept confidential.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Debre Markos University.
Informed consent
Written informed consent was mandatory after describing the objective of the study and its risk and benefits to the participants including their right not to be a part of the study as well as withdraw at any time before proceeding with data collection. Unfortunately, all the study participants were above 18 years old.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.