
Abstract
Nurses are loyal to their patients and coworkers. They often put the needs of others before their own and sometimes even before the needs of their families. This concern for others can cause conflicts that manifest as stress. Of the more than 2 million nurses in the United States, more than 62% work in hospitals. Hospitals are known to be both rewarding and stressful places to work. Like most workers, nurses face the challenge of balancing demands and achievements of work with those in their private lives. Hospital leaders can facilitate improved work–life balance (WLB) for hospital nurses by using tools already in place. Equally important, nurses can use their knowledge and resources to nurse the nurse within, which can greatly improve their experience of WLB, independent of the demands of their work environment.
Work–life balance (WLB) is a contemporary acronym for achieving balance between work and lifestyle ambitions. Although WLB is not well defined, the implication is that the two experiences (work and home life) should be in a state of equilibrium for nurses to be happy and healthy. Nurses often describe experiencing a lack of balance between their work and life outside of work. Yet if a sense of balance between work and lifestyle demands could be achieved, fewer nurses would report stress and more would be living healthier lives at home and in the workplace.
More than 2.5 million nurses practice in the United States. Of those, more than 62% are employed by hospitals (American Association of Colleges of Nursing [AACN], 2011). Hospitals deliver acute health care to patients and are known to be both rewarding and stressful work environments. The American Nurses Association (ANA, 2014) reports that the three most frequent concerns of hospital nurses are related to staffing, mandatory overtime, and workplace safety (ANA, 2014).
Most nurses are happier when experiencing feelings of achievement and satisfaction from their work rather than trying to acquire an arbitrary sense of work–life balance (Vredenburgh & Trinkaus, 1983). One of the goals in this article is to recognize that nurses experience more satisfaction at home and work by using tools to manage their stress.
Stress can manifest as physical complaints and emotional anxiety (Luca, Bellia, Bellia, Luca, & Calandra, 2014). Satisfactory integration of role achievement and enjoyment results in a positive emotional state experienced as WLB (Davis, Lind, & Sorensen, 2013; Winefield, Boyd, & Winefield, 2014). However, the two areas of work and life are neither equally balanced nor fixed. In other words, WLB fluctuates within an acceptable zone based on a range of circumstances and individual expectations.
Hospital Work Environment
Most hospitals provide care to sick patients regardless of their ability to pay. Yet as nurses are aware, hospitals must generate revenue to stay in business. Although the Affordable Care Act has provided coverage for previously uninsured patients, the law has also changed the way hospitals are reimbursed for care. For example, hospital reimbursement is now evaluated based on a number of metrics including patient’s length of stay, industry guidelines for admissions criteria, hospital readmission, hospital-acquired illnesses, and patient satisfaction ratings.
The Occupational Safety and Health Administration (OSHA; 2014) describes hospitals as
some of the most stressful places to work with potential hazards that include life-threatening injuries and illnesses complicated by overwork, understaffing, tight schedules, paperwork, intricate or malfunctioning equipment, complex hierarchies of authority and skills, dependent and demanding patients, and patient deaths.
No national standard for nurse–patient ratios (i.e., the number of patients a nurse is assigned during a shift) has been established. Currently, California is the only state with mandated nurse–patient ratios, though other states are working toward similar staffing goals (Schultz, 2013).
Likewise, nurses’ shift length is not regulated. Most hospital nurses work shifts of either 8.5 or 12.5 hr and many nurses are required to work overtime (Rogers, Hwang, Scott, Aiken, & Dinges, 2004). Nursing literature has documented that high nurse–patient ratios and nurse fatigue are risk factors for patient accidents and injuries (McClelland, Switzer, & Pilcher, 2013; Stimpfel & Aiken, 2013; Stimpfel, Sloane, & Aiken, 2012). However, the impact of nurse–patient ratios on WLB for hospital nurses is unknown.
As acknowledged by OSHA, hospital nurses are members of a complex health care team who provide care to sick and dying patients and their families. These nurses must maintain a strict work flow to closely monitor patients for cardiac or respiratory arrest, or more subtle changes in patients’ level of consciousness, blood chemistry, or risk behaviors (e.g., getting out of bed without assistance). As complex as the patient clinical environment may be, the health care team can be even more complex. In addition to managers who monitor regulatory standards that affect reimbursement for care, the health care team includes a wide range of health care specialists. Depending on specific patient health conditions, providers contribute to their care in unique ways.
Although nurses are the largest group of hospital workers, staff nurses who provide direct patient care have little control over their work environment. Successful solutions to improved WLB involve both the hospital and the individual nurse. In fact, most hospital leaders have resources to assist nurses in improving WLB. For example, OSHA recommends leadership access tools available through human resources and employee education departments (Table 1) to support nurses as they improve WLB.
OSHA: Methods of Reducing Hospital Worker Stress (OSHA, 2014)
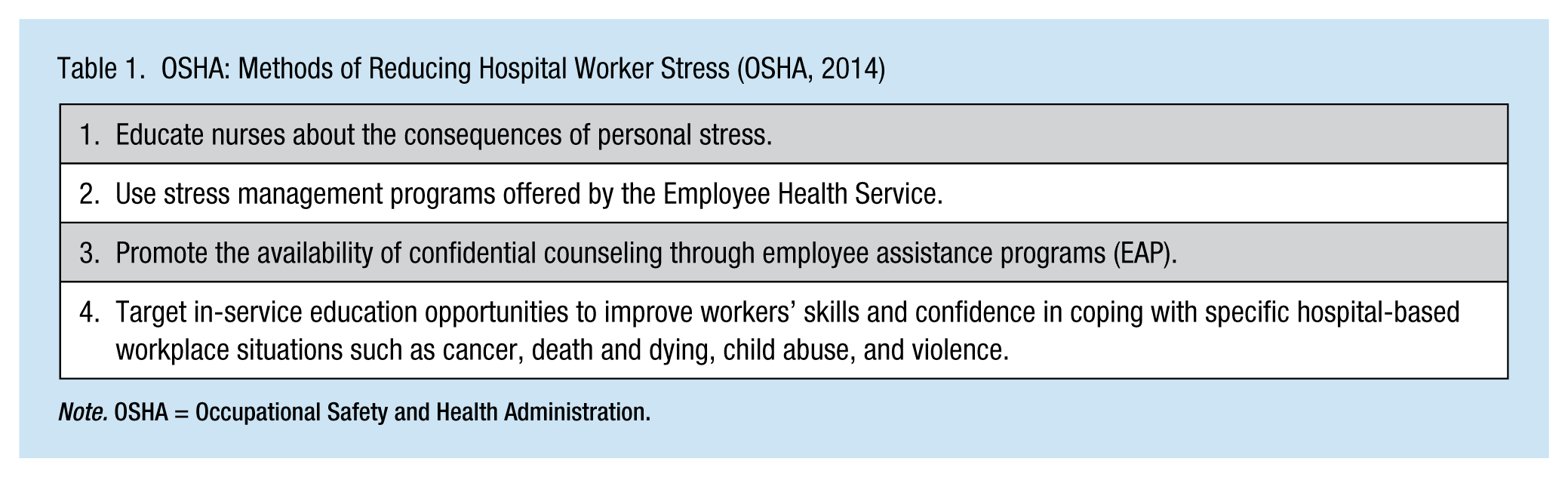
Note. OSHA = Occupational Safety and Health Administration.
Nurses Take Action for Satisfying Life
Nurses choose their profession for a variety of reasons. In a study that explored injured nurses’ motivations to work, many reported that becoming a nurse represented both a meaningful way to be of service to others and at the same time provided a role identity that connected them to family members or admired members of the community (Mullen, Gillen, Kools, & Blanc, 2013).
Nurses’ commitment to their profession as well as the physical and emotional demands of working with sick and dying patients can place nurses at risk of failing to recognize their own physical and emotional needs. By performing the most basic patient assessment, nurses are able to identify indicators of stress. Likewise, they can provide evidence-based recommendations for lifestyle changes to reduce stress. Although nurses are well educated about when and how to intervene to meet the needs of others, many discount their own needs (Mullen et al., 2013).
Stress is a consequence of work–life imbalance (O’Keefe, Brown, & Christian, 2014). Stress is experienced physically and emotionally (e.g., musculoskeletal disorders, pain, anxiety, and sleep disorders; Koh et al., 2014). Nurses learn to work under pressure, often with limited resources, but although nurses’ work stress may be unique because of workplace demand, the stress from lifestyle demand is widely shared by all workers. For example, most hospital nurses are women. Depending on their own age, many nurses care for children or aging parents, and they also provide wages and benefits critical to their families’ basic needs.
Finding the Motivation to Change
Nurses know that patient education should empower individuals to take an active role in changing their lifestyles. The same is true for nurses who seek WLB. To help themselves cope with the emotional consequences of poor WLB, nurses must learn to nurse the nurse within. By doing so, nurses can be role models for their colleagues.
Nurses can use their own knowledge and skills to improve their WLB. Nurses need not wait for changes in hospital policy or nurse–patient ratio legislation, or leave their hospital positions to improve their WLB; nurses have individual power.
The first step to improve WLB is to recognize that the changes needed are indeed individual. Each nurse who experiences the effects of work–life imbalance has a unique story. Nurses can begin by identifying individual priority areas; taking an inventory of individual needs and stressors is the first step in improving WLB. A second step is for nurses to realize that changing behaviors is challenging, requiring support, encouragement, permission, and a belief in self-worth. For nurses, similar to others who provide direct patient care, this step might require new thinking and new behaviors.
Steps That Can Make Changes
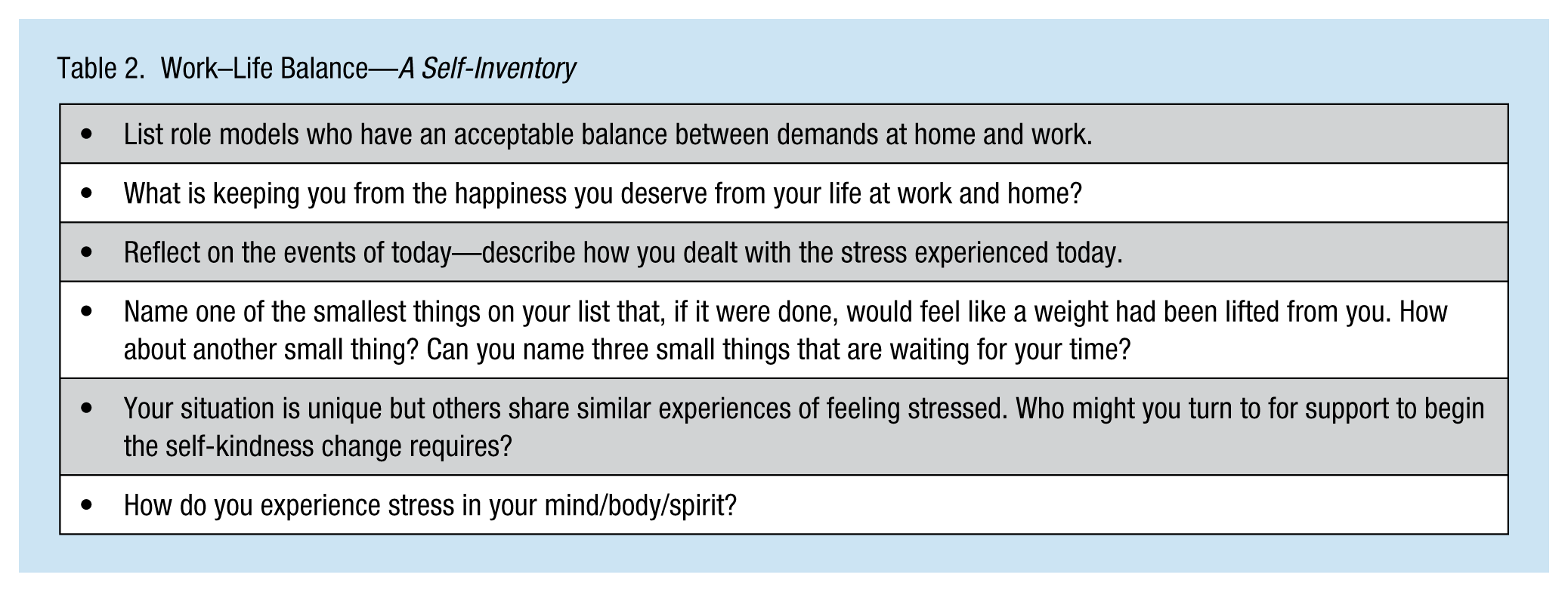
After acknowledging the need for change, nurses must find a starting place, create an individual plan, and continue to assess the need for modifications as circumstances evolve. A WLB inventory can assist individuals to focus on priority areas where rapid success is achievable, contributing to change momentum. Lifestyle changes are not easy especially if attempted without assistance; a key to success is finding individuals and processes that can support change. Coaching, a tool for self-improvement, is not new. Many health care providers employ nurses who assist patients achieve and sustain positive lifestyle changes. Now nurses must access tools they use to advocate for their clients to help themselves make healthy lifestyle changes. When work and lifestyle demands collide, nurses can take advantage of nursing the nurse within by using familiar tools and resources. Completing a WLB self-inventory (Table 2) can establish areas to set in motion for an individualized change process.
Work–Life Balance—A Self-Inventory
A lifestyle coach can establish a process to support change. Generalist life coaches, as well as nurse life coaches who have specific insight into the complexities of health care, are available. Finding a coach is similar to finding any other counselor. Valuable sources for finding a wellness coach to facilitate WLB include employer-sponsored employee assistance programs (EAP), trusted coworker and friend referrals, or health coach training facilities. Nurses must choose a coach who engenders trust and confidence. If an individual coach is not realistic, other sources of support and encouragement may improve nurses’ responses to conflicting demands. Some nurses may prefer to keep a journal of thoughts and ideas. Others may establish a contract for change with a supportive friend or mentor. Still others combine several methods to use as their individual process changes and matures.
Implications for Occupational Health Nurses
Hospital employee health nurses support the health and wellness of nurses and other health care workers. Although occupational health nurses often focus on specific workplace rules and regulations for health and safety, acknowledging the importance of WLB to employee health is an emerging area. By becoming more aware of the consequences of occupational and personal stressors, employee health nurses can expand their role and increase their value to both workers and organizational leadership. OSHA suggests a variety of strategies to bridge employee health to other employee assistance programs that are already in place, resulting in better use of services, and improving employee health nurse and staff relations.
Summary
Improving work–life balance requires active, evidence-based strategies. The process begins with self-reflection and progresses by taking action. Hospital nurses are drawn to the environment for many of the same reasons that challenge their well-being. Yet nurses can learn individual strategies to achieve a sense of balance and well-being. This knowledge will support them as they become successful and effective at work, maintaining roles outside the hospital that bring happiness and joy. Recognizing the need for and committing to change are the starting points for creating effective WLB.
Footnotes
Acknowledgements
The author would like to thank Mikako Arakida, RN, PHN, PhD, professor, School of Nursing and Rehabilitation Science at Odawara International University of Health and Welfare, Japan and Oi Saeng Hong, RN, PhD, FAAN, professor, University of California San Francisco, California.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Kathleen Mullen, PhD, MS, RN, is Assistant Clinical Professor-volunteer at the University of California San Francisco, Community Health Systems. Dr. Mullen’s work focuses on the impact of work injury and job loss on the individual, family, and community.