
Abstract
Background: Health care professionals (HCPs) historically exhibit high rates of stress, burnout, and low rates of service utilization from Employee Assistance Programs (EAPs) and Professional Health Programs (PHPs). New and magnified stressors that accompanied COVID-19 exacerbated HCPs’ risk of burnout. Purpose: During the pandemic, this study examined Ohio HCP’s utilization of EAPs and PHPs, knowledge of available services, barriers to accessing services, and likelihood of future service utilization. Conditions needing to change to increase likelihood of future utilization were also explored. Methods: A one-time survey was administered in July and August of 2021 to HCPs from 13 licensing boards in Ohio. This study used a subset of data to examine the extent of convergence between quantitative results—analyzed using frequency calculations—and results from thematic analysis of corresponding open-ended survey items. Qualitative results supported and elaborated the quantitative findings. Results: Fewer than 25% of respondents (N = 12,807) utilized EAPs or PHPs to address mental health concerns. Obstacles impeding service utilization included issues around awareness, time commitment, and confidentiality—a concern encompassing issues of stigma and fear of employment repercussions. Noting multiple obstacles to accessing EAPs and PHPs, HCPs in Ohio reported low rates of support service utilization and low likeliness to use services in the future despite their experiences of extreme stress and burnout. Conclusions: Addressing the time commitment and confidentiality concerns could increase the likelihood of accessing services. Employers of HCPs should explore additional support mechanisms such as comprehensive wellness programs and innovative, brief intervention strategies to combat burnout, especially during viral outbreaks and other high-stress events.
Keywords
In 2020, the COVID-19 pandemic exacerbated pre-existing, high rates of stress and burnout among health care professionals (HCPs) (Stodolska et al., 2023) who are also known to have low rates of help-seeking to manage stress and mental health challenges (Wijeratne et al., 2021). Given the added stressors caused by the pandemic, accessing external supports to temper burnout and facilitate stress management was as important as ever to maintain an effective and healthy workforce. Specialty resources such as Employee Assistance Programs (EAPs) and Professional Health Programs (PHPs) are designed to assist HCPs in managing stress and promoting well-being. The Ohio Professionals’ Health Program (OhioPHP) is a nonprofit organization dedicated to the health and well-being of HCPs in Ohio, providing confidential services in a supportive and compassionate environment (OhioPHP, 2023). OhioPHP functions as an advocate and resource for HCPs affected by mental, emotional, and behavioral illness, substance use disorders, or other illnesses. To better understand the impact of COVID-19 on HCPs’ well-being and experiences with stress and mental health help-seeking during the pandemic, OhioPHP—with funding from the Federation of State Medical Boards—administered a state-wide survey of HCPs from 13 Ohio Licensing Boards. In this paper, we describe a subset of results from a large study designed to understand HCPs’ pandemic-related stressors and the impact of the pandemic on their well-being and mental health. Specifically, we describe respondents’ utilization of EAPs or PHPs and their knowledge, opinions, and experiences with these programs to manage pandemic-related stressors.
Literature/Background
Before the onset of the pandemic, over half of physicians in the United States had exhibited some signs of job burnout—characterized by feelings of depersonalization, emotional exhaustion, and reduced self-efficacy (Maslach & Leiter, 2017)—with rates even higher across some medical specialties (Shanafelt & Noseworthy, 2017). For example, a pre-pandemic study showed that nearly 70% of emergency medicine physicians reported experiences of burnout compared to 30% of those working in preventive medicine, occupational medicine, or environmental medicine (Shanafelt et al., 2012). During the pandemic, 75% of HCPs involved with clinical care for COVID-19 patients experienced psychiatric symptoms of PTSD, anxiety, substance use, depression, insomnia, and/or suicide (Lai et al., 2020; Xiao et al., 2020). Specific HCP characteristics like being female, young, early career status, lacking specialized training, and lacking institutional support increased the prevalence of mental health concerns and burnout during viral outbreaks, such as the COVID-19 pandemic (Serrano-Ripoll et al., 2020). Negative health outcomes were likely exacerbated by specific pandemic stressors, such as insufficient access to personal protective equipment and fear of contracting and/or spreading COVID-19. HCPs also reported experiencing stress due to increased work demands and longer hours at work (McCloskey et al., 2023). In addition to work-related stress, HCPs lacked sufficient time with loved ones, felt disconnected from their children, and felt their families/friends did not understand their work stress (McCloskey et al., 2023).
These high rates of burnout and stress are problematic because the consequences are serious—maintaining mental health is crucial to HCPs’ overall well-being and affects work efficacy, quality of medical care, and patient safety (Ruotsalainen et al., 2014). Studies have linked burnout in the health care profession with reduced patient satisfaction (Moss et al., 2016), reduced provider empathy (Haramati et al., 2017), increased medical errors (Hall et al., 2016), patient safety concerns (Chuang et al., 2016), decreased productivity, absenteeism, employee turnover, and increased employee health care costs (Dewa et al., 2014; Moss et al., 2016).
Employee Assistance Programs (EAPs)
Employee Assistance Programs and other workplace wellness initiatives were established to assist organizations in addressing productivity issues and to assist employees in identifying and resolving personal concerns that affect job performance—for example, issues related to health, family, marriage, finances, substance misuse, legal concerns, stress (Employee Assistance Professionals Association, n.d.). Although the structure and operations of EAPs may vary, their purpose is to deliver services to promote productive and healthy workforces and workplaces. They provide strategic support to organizational leaders’ efforts to enhance the work environment, improve employee performance, and support struggling employees; they also provide individual assistance to employees and their family members who may be experiencing personal difficulties.
Utilization of EAPs in the United States has produced positive outcomes. Some studies indicate that participation in EAPs can reduce stress, improve mental health symptoms, and restore higher work functioning and productivity (Attridge & Dickens, 2021, 2022). A large study of federal government employees reported statistically significant improvements in work and social relations, emotional problems, physical problems, absenteeism and lateness, and overall global assessment of functioning (Selvik et al., 2004). Similar findings across more recent studies also support evidence of EAP utilization effectiveness on clinical and workplace outcomes (Attridge & Dickens, 2022). Given these positive outcomes, it is perhaps unsurprising that EAPs can contribute to financial savings for health care organizations (Csiernik et al., 2021). Attridge and Dickens (2022) estimated a return on investment of $4.26 to $1 for an EAP where cost savings amounted to over $2,000 per case—avoided depression treatment costs were estimated to save $611 per case and avoided loss of productivity costs were estimated to be $1,433 per case.
Counterintuitive patterns have shown that EAP utilization tends to be lower during times of extreme stress or crisis. For example, demand for EAP individual counseling services decreased in the aftermath of the terrorist attack on September 11, 2001 (Azzone et al., 2009). COVID-19 was no exception; EAP utilization was 35% lower in the beginning months of the pandemic compared to the same time period the year prior (Couser et al., 2021). One study of public health workers reported that the top reasons against utilization were lack of knowledge about their EAP benefits, difficulty accessing benefits, and belief that EAP services would not be useful (Moore et al., 2023). Other commonly cited reasons for low EAP utilization include confidentiality concerns, stigma, and fear of job repercussions (McRee, 2017; Moore et al., 2023). Alternatively, the unique nature of significant stressors presented during times of extreme crisis could also be a contributing factor to lower utilization rates (Azzone et al., 2009).
Physician/Professional Health Programs (PHPs)
Physician and Professional Health Programs are also employee-focused programs designed to promote well-being in the workplace. PHPs were initially established to support physicians specifically, but programs now serve a broader clientele and are more commonly referred to as Professional Health Programs. Distinct from EAPs, “PHPs are state programs whose primary dual missions include: (1) Supporting physicians diagnosed with a potentially-impairing condition (i.e., substance use disorder [SUD], severe psychiatric disorder, cognitive disorder, or other medical condition) and (2) protecting patient safety by providing monitoring services” (Merlo et al., 2022, p. 116).
Physician and Professional Health Programs provide active care management, monitoring, and supervision for HCPs who have signed formal contracts for PHP participation, which usually begins with intervention followed by evaluation and intensive residential and/or outpatient treatment (Merlo et al., 2022). Participants adhere to certain requirements, which commonly include a monitoring plan (typically 5 years for PHP participants with a moderate to severe SUD), random drug screenings, participation in facilitated support group meetings, and quarterly evaluations (Merlo et al., 2022). Usually, PHP utilization is confidential and voluntary and serves as an alternative to disciplinary measures from state licensing boards (Merlo et al., 2022).
Compared to general population treatment outcomes the, outcomes associated with PHP participation historically have been favorable (Merlo et al., 2022). In a study of 902 PHP participants, 80.7% completed the 5-year monitoring agreements and 78.7% continued working with no license restrictions (McLellan et al., 2008). A more recent study reported an 89% monitoring agreement completion rate with no return-to-use during the monitoring period (Merlo et al., 2022), and 79% reported no alcohol use since the completion of the agreement. Satisfaction with PHP participation is high—76% of physicians perceived that they would have been unsuccessful without formal SUD treatment through the PHP; 77% would refer colleagues to the state PHP without reservation.
Given the added stressors caused by the pandemic, accessing external support to temper burnout and facilitate stress management during the COVID-19 pandemic was as important as ever to maintain an effective and healthy workforce. However, the degree to which Ohio HCPs accessed workplace support during the pandemic was unknown. Similarly, Ohio HCPs’ perceptions, experiences, and opinions about these supports had not been formally explored. Therefore, the purpose of this study was to (a) better understand the extent to which Ohio HCPs accessed workplace supports (i.e., EAPs or PHPs) to manage pandemic-related stress, (b) determine Ohio HCPs’ knowledge, opinions, and experiences of EAPs and PHPs during the COVID-19 pandemic, and (c) among those who were unlikely to access services, examine perceptions about what would need to change to increase their likelihood of accessing services. This study aimed to answer the following research questions: (1) What percentage of Ohio HCPs utilized workplace supports (i.e., EAPs or PHPs) during the pandemic; (2) What were Ohio HCP's knowledge, opinions, and experiences regarding EAPs and PHPs during the pandemic; (3) What do Ohio HCPs who are very unlikely in the future to use workplace support services describe EAPs and PHPs as needing to change before they would consider using these services?
Methods
In this study, we used a cross-sectional, retrospective pretest-posttest design (Little et al., 2020). In the one-time, online survey, participants were asked to respond to questions two times, with each time referring to a different time period—first referring to the period of time prior to exposure to a condition (i.e., the COVID-19 pandemic) and second referring to the period following exposure.
The study adhered to standards for conducting ethical research, and the 13 Ohio licensing boards in Ohio reviewed and approved the research protocol. OhioPHP submitted a public records request with each of the 13 licensing boards in Ohio to obtain the email addresses of licensed HCPs. OhioPHP sent batched emails to HCPs with information about the survey and a link to access the survey. After clicking on the link, respondents were required to review the study information and provide their informed consent before advancing to the survey. Participation was voluntary, there were no incentives offered to participants, and participants could withdraw at any time without repercussion. Participant responses were both anonymous and confidential, and the research team did not have access to the participants’ email addresses or any other identifying information that could link responses to any one individual.
Data Collection
From July to August 2021, the survey was administered to HCPs from 13 Ohio Licensing Boards on the online platform Typeform® and consisted of 56 multiple-choice selection items. There were five open-ended questions in which the participants were invited to type a response in their own words. In the current study, we focused on the four multiple-choice survey items about HCPs use of supportive services for mental health concerns, barriers to accessing supportive services, knowledge of mental health assistance programs (i.e., EAPs and PHPs), and the likelihood of using these services in the future. We also focused on two of the open-ended questions, which were follow-up items made available only to the respondents who indicated they would be “very unlikely” to participate in an EAP and/or PHP. The item stated, “Please indicate what might be improved or needed in order for you to access this program.” For additional details about the study’s research methods and procedures, please see McCloskey et al. (2023).
Data Analysis
Descriptive statistics with IBM’s software SPSS (Version 27) were used to analyze quantitative data. The open-ended items with respondents written responses were analyzed using qualitative team-based thematic analyses (Guest & MacQueen, 2008). Participants’ open-ended responses were extracted from Typeform® into Microsoft Excel for analysis. The EAP question data (n = 2,214) and PHP question data (n = 923) were coded in two iterations by two coders who applied descriptive codes to responses. After generating an exhaustive list of codes (i.e., no new codes were emerging), a third review of the responses was conducted. Where appropriate, related codes were collapsed and organized under main themes. The final themes were chosen by code salience, group discussion, and consensus. Peer debriefing—consultation with an impartial colleague—was used to strengthen credibility of the findings at two points throughout the analysis process and again when choosing the final themes (Nowell et al., 2017). Some responses were unclear or indicated uncertainty (i.e., not sure, I don’t know); and some respondents stated that they did not access an EAP (n = 414) or PHP (n = 268) because they were not experiencing stress or mental health concerns requiring additional support or they were receiving private services elsewhere. Consequently, responses were excluded from analysis if they were too vague, indicated uncertainty, or indicated no service needs.
Results
Sample and Demographics
Of the 490,707 delivered invitation emails to licensees, there were 13,532 survey responses (2.76%) submitted representing 13 health care licensing boards in Ohio (McCloskey et al., 2023). Duplicate responses (n = 66) were removed from the complete data set. For the purposes of the current study, respondents (n = 659) who indicated they did not work at any point during the pandemic were removed from this analysis. After removing these responses which represented 4.89% of the original sample population, the total analyzed sample contained 12,807 respondents (Table 1). Among them, 31.09% were licensed with the Ohio Board of Nursing, 20.78% with the State Medical Board of Ohio, 11.06% with the State Ohio Board of Pharmacy, and 9.64% with the Ohio Counselor, Social Worker, and Marriage and Family Therapist Board. Participants had an average of 18.67 years of work experience (range 0 – 66 years). Most participants identified as female (76.69%), White (89.99%) and between the ages of 35 and 64 years old (Table 2).
Licensing Boards and Work Experience (N = 12,807)
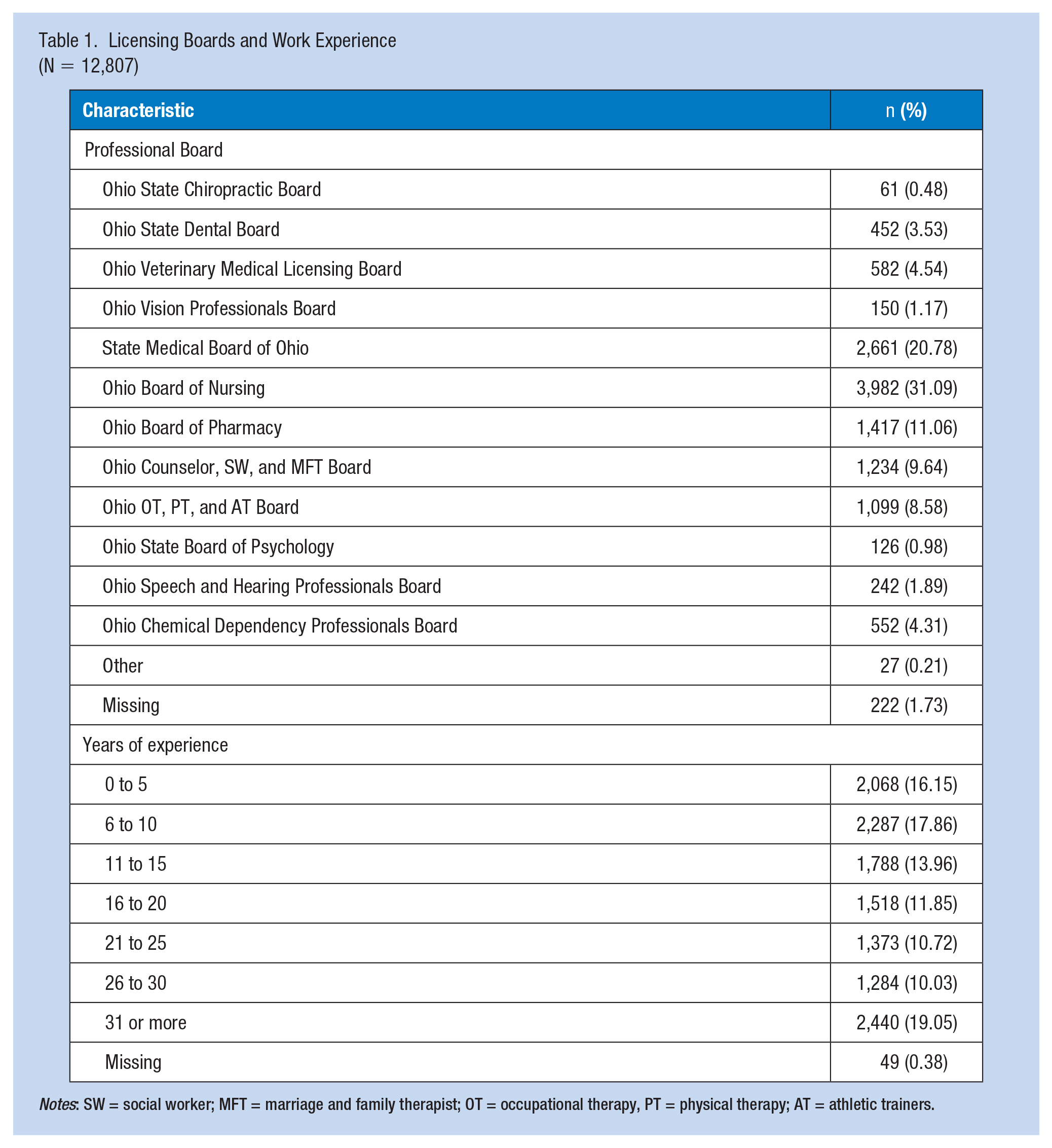
Notes: SW = social worker; MFT = marriage and family therapist; OT = occupational therapy, PT = physical therapy; AT = athletic trainers.
Demographic Characteristics (N = 12,807)
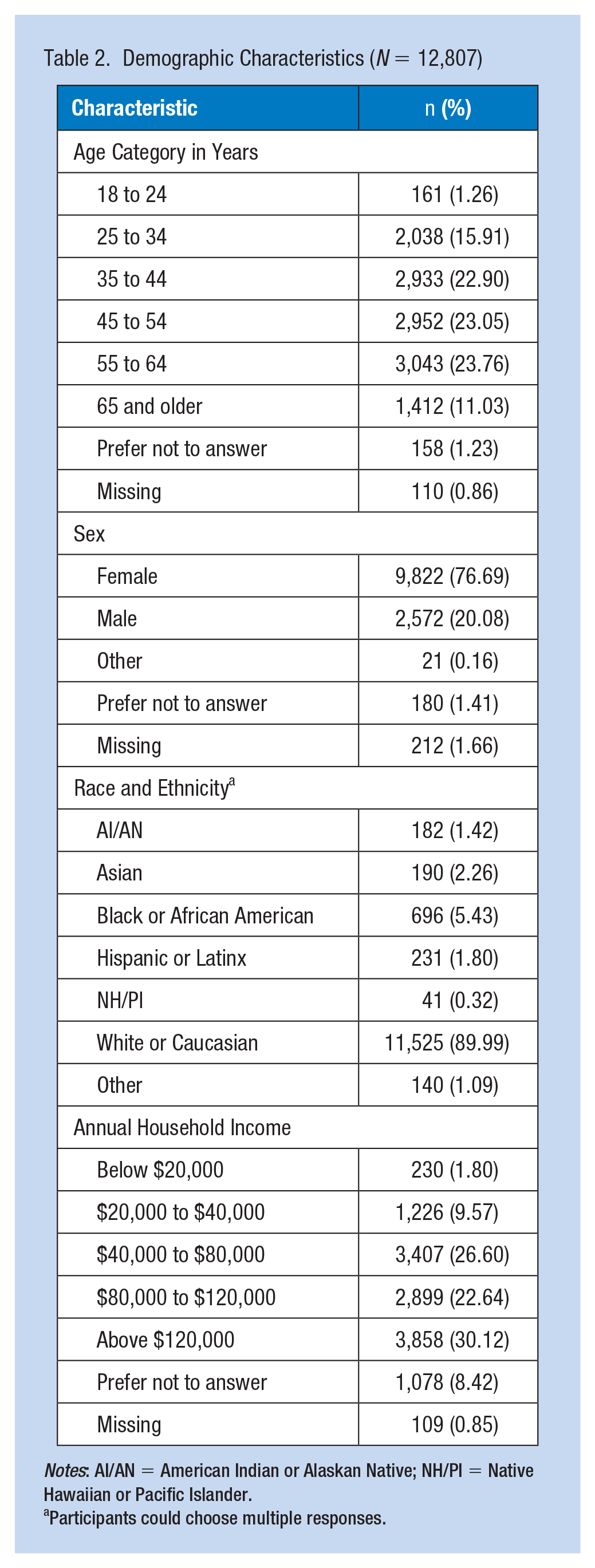
Notes: AI/AN = American Indian or Alaskan Native; NH/PI = Native Hawaiian or Pacific Islander.
Participants could choose multiple responses.
Service Access
Most participants (80.52%) reported not being screened, assessed, or monitored at work for pandemic-related stress concerns. Fewer than 1 in 4 (24.22%) HCPs sought mental health support. Among those who did seek support, the highest percentages of satisfaction were noted with support received from friends and family (65.18%), coworkers (48.88%), and therapists (47.12%). Participants were most dissatisfied with the support received “in general, at work” (48.61%) and from their supervisor (44.64%). Other categories of support included EAPs, support groups, faith communities and other.
Knowledge About Mental Health Assistance Programs
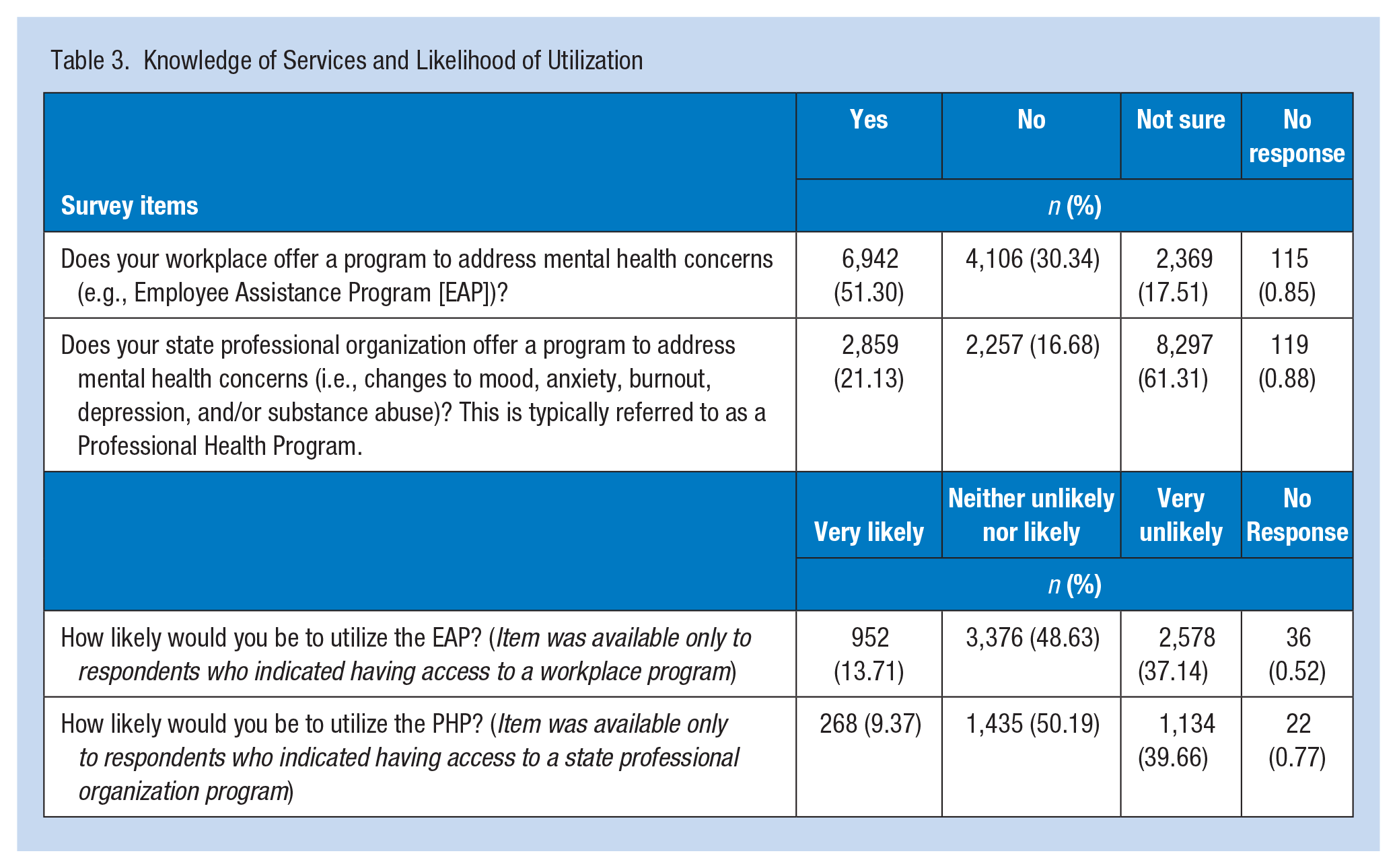
More than half (51.30%) of respondents indicated that their workplace offered a mental health assistance program, such as an EAP, while 30.34% indicated their workplace did not (Table 3). A portion of respondents (17.51%) were unsure if their workplace offered mental health-related programs. Most respondents (61.31%) were unsure if their state professional organization offered a PHP. Only 21.13% answered affirmatively that their state professional organization offered a PHP, while 16.68% said no such program existed.
Knowledge of Services and Likelihood of Utilization
Likeliness to Participate
Nearly half of the participants indicated they would be neither unlikely nor likely to participate in an EAP (48.63%) or a PHP (50.19%). Among those with access to an employee mental health program, there were fewer respondents (13.71% and 9.37%, respectively) who said they would be very likely to participate in an EAP or a PHP; more respondents were very unlikely (37.14% and 40%, respectively) to participate in an EAP or PHP.
Obstacles to Seeking Assistance
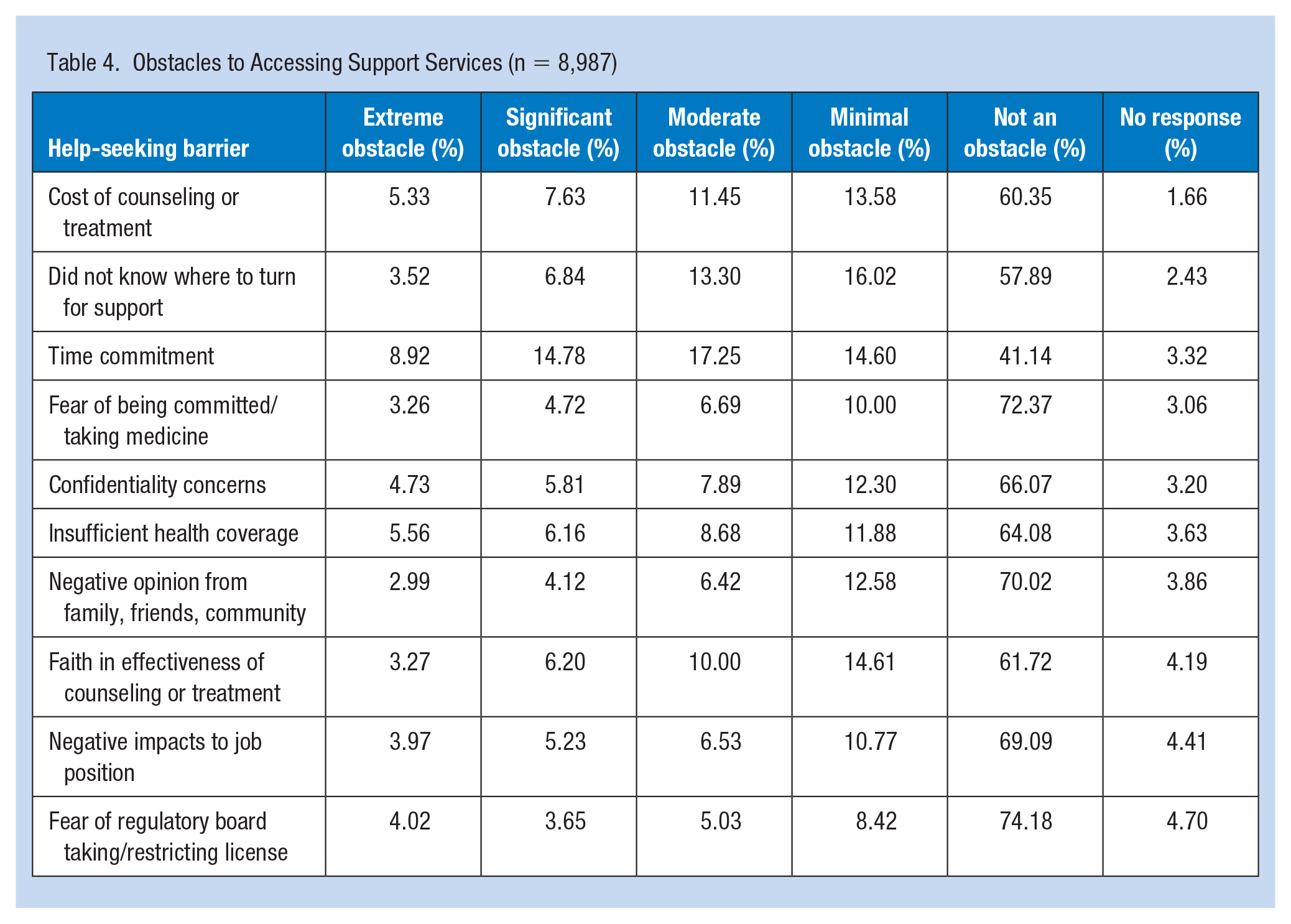
The barrier most frequently identified by respondents (56%) was time commitment; respondents identified it as a moderate obstacle (17.25%), a significant obstacle (14.78%), minimal obstacle (14.60%), or extreme obstacle (8.92%). Not knowing where to turn for support was the second largest obstacle that respondents (40%) identified (Table 4). The remaining help-seeking obstacles included the cost of counseling or treatment (38%), faith in the effectiveness of services (34%), insufficient health care coverage (32%), confidentiality concerns (31%), concern about negative impact on job position (27%), negative opinion from others (26%), fear of being committed/taking medicine (25%), fear of regulatory board taking/restricting license (21%).
Obstacles to Accessing Support Services (n = 8,987)
Qualitative Findings—Obstacles to Seeking Assistance
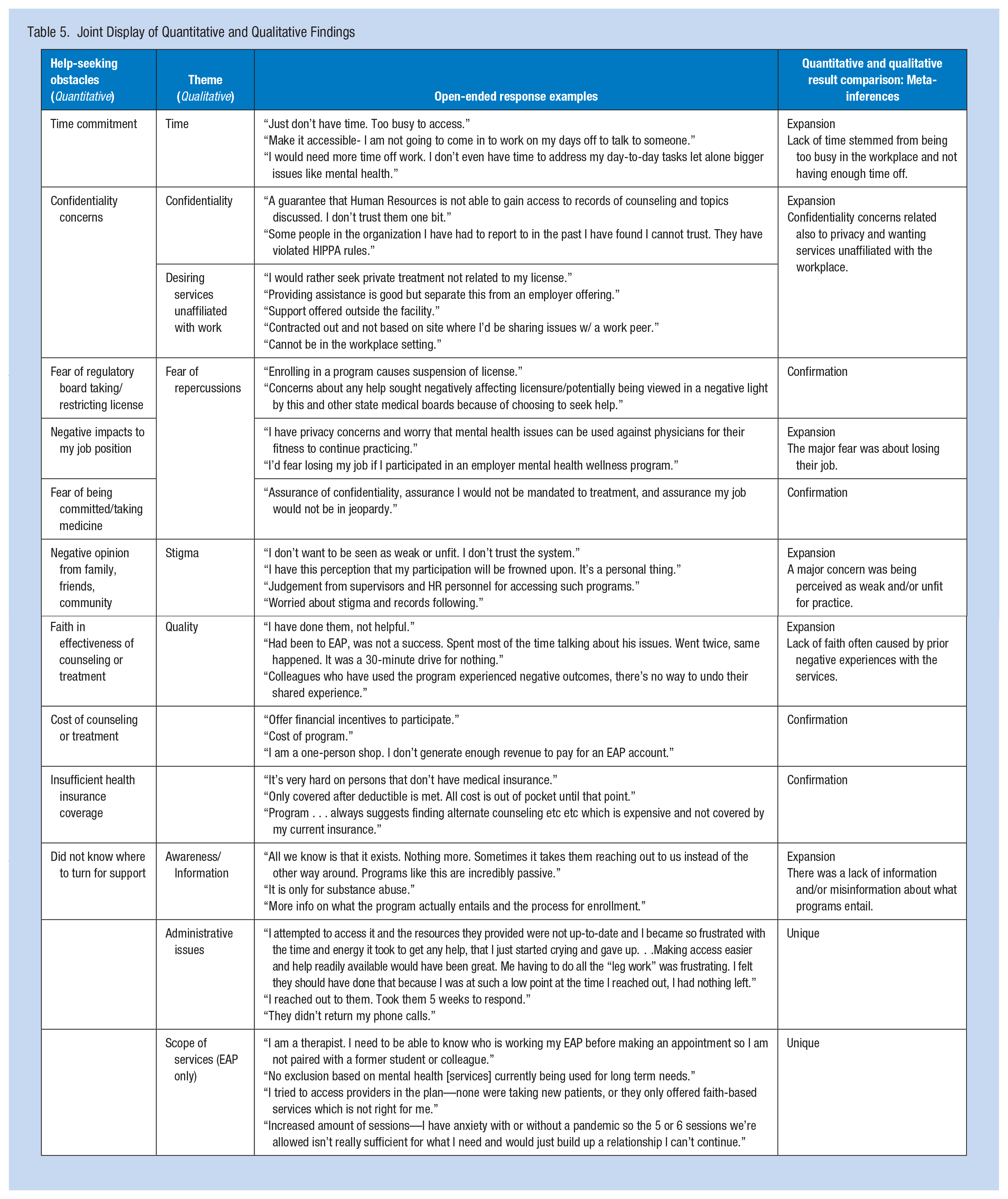
Overall, the two primary reasons for being very unlikely to access an EAP or PHP were barriers to accessing services and concerns about confidentiality. Issues around accessibility included time, affordability, awareness/knowledge, and quality of care. Additional concerns about accessing EAPs specifically were location, scope of services, and administrative issues. Confidentiality concerns related to the workplace affiliation of available services, stigma, and fear of repercussions. We describe these themes in more detail and provide example responses supporting each theme in Table 5. Where applicable, verbatim quotes were edited for clarity and grammar without changing their content or meaning.
Joint Display of Quantitative and Qualitative Findings
Barriers to Accessing Services
Overwhelmingly, respondents explained that accessibility issues needed to be addressed before they would participate in an EAP or PHP. Some accessibility concerns were general (e.g., “easier access,” “a local office with on-site help, not a 1-800 number”), while other responses described specific impediments to service accessibility: time, affordability, awareness/information, quality, scope of services, and administrative issues.
Time
For some, EAP/PHP service hours and/or models were incompatible with work or home schedules. These respondents—many with night shifts and/or atypical schedules—expressed a need for paid time off and staff coverage, which could enable their participation.
Affordability
Financial constraints were a concern. The cost of services would need to decrease, or financial incentives would need to be offered to facilitate service utilization.
Awareness/Information
A portion of respondents did not know how to access services, did not think they qualified, or required more information about service options. There was an expressed desire for employers to proactively share information about programs rather than respondents having to learn about them on their own.
Quality
Some respondents were not inclined to use services because of a concern with the efficacy or quality of programs and service providers that often stemmed from negative prior experiences or anecdotal evidence from their peers.
Scope of Services (EAP Only)
Some respondents requested modified or expanded EAP services because the existing services did not meet their needs. Some described an inability to use services due to unique circumstances (e.g., potential pre-existing relationship with an assigned therapist) or the limitation of the allotted number of sessions. Whether or not a service was faith-based also affected some respondents’ likelihood of accessing services.
Administrative Issues (EAP Only)
Administrative issues when trying to engage with the EAP itself were a barrier. These issues included scheduling difficulties, ease of getting started with the program, and poor communication and responsiveness from service providers.
Confidentiality
Overlapping issues relating to confidentiality included stigma, fear of repercussions at work, and a desire for services unaffiliated with work. Many respondents did not trust that service utilization would be confidential and expressed a desire to keep their protected health information private from licensing and state medical boards. Some respondents were concerned about stigma and how they would be perceived. They did not want their employer and colleagues to view them as impaired or unfit to practice. There was also a concern that accessing services could jeopardize career advancement (e.g., losing professional licensure or creating conflicts with state boards or human resources). Consequently, many respondents preferred to access supportive services completely unaffiliated with their employer.
Discussion
This study examined Ohio HCPs’ awareness and utilization of available support services during the height of the COVID-19 pandemic, likelihood of using services in the future, and—for those who were unlikely to use services—the factors impeding their willingness to use them. Despite exacerbated stress (e.g., McCloskey et al., 2023), fewer than 25% of HCP respondents utilized emotional services for any mental health concerns such as stress, burnout, substance abuse, depression, or unstable mood during the pandemic. Evidence has indicated that EAP and PHP services contribute to improved clinical and workplace outcomes (Attridge & Dickens, 2021), yet for participants in this study who were aware of EAP and PHP offerings, most were ambivalent about or unlikely to use these services in the future.
Study findings indicate a need to increase awareness of available support service options. Respondents often were unaware of many aspects of EAP and PHP programs, such as whether they were offered at their workplace, and if so, what type of services were available and what service utilization would entail. To eliminate this knowledge gap, organizations should vigorously promote EAP and PHP services; extensive promotion by employers has been shown to increase the likelihood of employee enrollment (Azzone et al., 2009; Shepps & Greer, 2018). Interestingly, in workplaces where employers focused a great deal on wellness and prevention programs, EAP utilization tends to be lower, though an enhanced focus on promoting overall health and well-being could explain a reduced demand for EAP services (Azzone et al., 2009).
There was a particular knowledge gap about reporting mandates associated with support service utilization—respondents lacked clarity around confidentiality and potential consequences when accessing PHP services. This finding aligns with previous studies citing confidentiality concerns and fear of negative employment repercussions as a reason for low EAP utilization (McRee, 2017; Moore et al., 2023). However, since 2018, OhioPHP has offered the One-Bite program enabling HCPs licensed through the State Medical Board of Ohio (SMBO) and the Ohio Vision Professionals Board to seek substance use treatment without being penalized or subject to SMBO disciplinary action so long as the participant adheres to certain requirements (e.g., immediately suspend practice for a minimum of 30 days). Other licensing boards also offer non-disciplinary treatment options. Strategies to promote awareness about these options—which should be customized for each licensing board because the terms of utilization vary across the professions—should involve a plan to dispel myths and share accurate information about the scope and quality of services.
Strategies to promote service utilization should consider the reported obstacles to accessing services. One major obstacle to seeking help was burdensome workloads and the inability to commit necessary time for accessing support services. HCPs also reported a desire for support services unaffiliated with their workplace. Innovative strategies are needed to offer services that are independent of the workplace and require a minimal time commitment. Newly implemented efforts in the state of Ohio aim to address some of these concerns. For example, The Ohio State Medical Association established in 2022 an anonymous, free, 10-item questionnaire enabling HCPs to assess their well-being (2023). After completing the questionnaire—the Well-Being Checkup and Referral Engagement (CARE) Service—a licensed mental health practitioner reviews the results and provides individualized recommendations for mental and emotional support services available in multiple modalities in the HCP’s geographic area. HCPs can remain anonymous while also learning about various treatment options. Though the impact of this program is not yet known, the well-being CARE service aligns with many of the desired characteristics HCPs identified.
Limitations
These study findings should be interpreted within the context of the study's limitations. As a cross-sectional study with a self-administered survey, there was no opportunity to follow up with respondents to elicit more detail or to clarify open-ended comments that were vague, unclear, and removed from analysis by the research team. Another limitation is the relatively small response rate compared to the pool of eligible participants. Although the sample size was large, only a small portion (i.e., 2.76%) of eligible respondents completed the survey. A larger response rate may have adjusted the study findings. Also, the analyzed sample excluded 4.89% of the total sample because respondents who did not work at any time during the pandemic were necessarily removed from analyses. These respondents may have had unique perceptions about—and experiences with–accessing supportive services; however, to include their responses was outside of this study's scope. Finally, data were not disaggregated by each licensing board, so no patterns or variations across HCPs from each licensing board could be detected.
Implications for Occupational Health Practice
Given the low service utilization rates, the low intention to use EAPs and PHPs in the future, and the range of barriers participants identified, it could be argued that additional policies/programs are needed to augment the traditional models of EAPs and PHPs. How, then, might existing programs adapt—or new programs develop—to provide effective services to more HCPs in need of support? It could be possible that a more holistic and expansive wellness benefits plan/package would be beneficial to a larger portion of HCPs. More effort is also needed to raise awareness and provide clarity about EAP and PHP services and policies—particularly those related to reporting mandates and potential consequences (if any).
Future research and evaluation could further explore the perceptions of HCPs about what employers could do to manage workplace stress. Focus groups and/or interviews with HCPs could elicit a more in-depth understanding, which in turn could inform the development of new and/or augmented health and wellness supports in the workplace. In addition, future research is needed to distinguish differences in perceptions and experiences across demographic groups (race, sex, age, and years of experience). Because specific HCP characteristics (e.g., career status, sex, and age) are associated with increased prevalence of mental health concerns and burnout during viral breakouts (Serrano-Ripoll et al., 2020), understanding the variation of support service utilization, likeliness to utilize services in the future, and barriers to accessing services by demographic groups would be useful for tailoring awareness campaigns, programs, and policies.
Conclusion
Even though the peak of COVID-19 has subsided, it is critical that HCPs have access to and receive the type of support necessary to promote their health and well-being. Workers were stressed before the pandemic, and they are likely to experience continuing mental health symptoms (anxiety and depression) even after the outbreak has subsided (Serrano-Ripoll et al., 2020). With a better understanding of Ohio HCPs’ knowledge, experiences, and barriers to supportive service utilization, employers and stakeholders can develop and implement responsive strategies to reduce burnout and promote employee well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Federation of State Medical Boards Foundation
Research Ethics
This manuscript reports a human study that followed high ethical standards. No ethics committee reviewed the study protocol; however, each of the 13 licensing boards in Ohio that participated reviewed and approved the study.
Participants were identified through a public records request, were notified through email, and completed an informed consent form prior to accessing the survey. The authors/researchers do not have access to participants’ identifiable information.