
Abstract
Background:
Although many adults with diabetes are productive members of the workforce, loss of work productivity has been associated with diabetes. The purpose of this study was to explore the interrelationship between work-related factors and current work ability in adults with type 1 diabetes (T1D) and type 2 diabetes (T2D).
Methods:
This study used a convergent mixed-method design. We assessed the relationship between work-related factors and work ability using bivariate statistics and logistic regression. Work ability was measured using the Work Ability Index and Karasek’s Job Content Questionnaire (JCQ) was employed to measure job demands. Qualitative interviews (n = 30) explored the relationship between diabetes and work.
Findings:
The sample (n =101) was mostly female (65%) and White (74%). Most worked full-time (65%), had T2D (87%), an elevated glycated hemoglobin A1c ≥ 7% (56%), and were overweight (22%) or obese (68%). Only 33% of subjects self-reported their work ability as excellent. Four of the JCQ subscales (skill discretion, psychological demands, supervisor support, and coworker support), and work–life balance were significantly associated with work ability (all p < .05). In adjusted models, better coworker support (OR = 1.4; 95% CI = [1.04, 1.9]) and better work–life balance (OR = 1.3; 95% CI = [1.1, 1.5]) were associated with excellent work ability. Many stated their diabetes impacted them at work and spoke of the effects of stress. Few engaged in workplace wellness programs.
Conclusion/Application to Practice:
Social support and work–life balance were associated with excellent work ability. Engaging workers with diabetes in workplace educational programs may take strategic efforts by occupational health staff.
Background
Over 30 million Americans, or 9.4% of the population, have a diagnosis of diabetes, with type 2 diabetes (T2D) accounting for 90% to 95% of cases (Centers for Disease Control and Prevention [CDC], 2019). The estimated cost of diagnosed diabetes in 2012 was US$245 billion, including US$176 billion in direct medical costs and US$69 billion in reduced productivity (American Diabetes Association [ADA], 2013). Although many adults with diabetes are productive members of the workforce, loss of work productivity has been associated with the presence of diabetes (Krstovic-Spremo et al., 2014). Diabetes self-management (DSM) is a lifelong process and includes healthy nutritional habits, being physically active, taking medication, and monitoring blood glucose, with the goal of preventing both acute and chronic complications (Haas et al., 2014). Despite a decline in the prevalence of cardiovascular disease overall, it is still the leading cause of death in individuals with diabetes (Duca et al., 2013) and is also associated with workplace absenteeism and short-term disability (Song et al., 2015).
Managing diabetes in the workplace may present challenges. A high workload (restricting the duration of frequency of breaks), poor job control (unscheduled events) and unspoken social norms (discomfort in regard to checking blood glucose or injecting insulin) may be barriers to effective diabetes self-management during the workday (Loerbroks et al., 2018). Adults with diabetes must decide whether or not to disclose their diagnosis to their employer. Those who believe it is an employer’s responsibility to provide flexible working conditions and those who feel respect from their superiors are more likely to disclose they have diabetes, while nondisclosure was associated with greater absenteeism due to illness (Olesen et al., 2017).
A qualitative study on perspectives of both employees (n = 23) and health professionals (n = 22) regarding what adults with diabetes needed in the workplace to support job retention, reported that several themes emerged (Detaille et al., 2006). For example, the employees wanted their colleagues to know they had diabetes and how to react if they became ill; to have support and understanding from both colleagues and management; to have a stable workload with a good balance between their diabetes and their work; and to have health care professionals who could help them avoid or handle complications. According to data collected from the health professionals in this same study, employees with diabetes needed a work environment that supported diabetes self-management; no workplace discrimination as a result of their diagnosis; health care professionals who took workplace demands into account when planning treatment and counseling patients; and family support that encouraged a normal lifestyle (Detaille et al., 2006). Although many adults with diabetes do not need special accommodations in the workplace, an in-depth assessment of their needs (e.g., maintaining glycemic control or other diabetes complications) may facilitate a safe work environment where the person with diabetes may work at optimal levels (Iavicoli et al., 2019).
Many factors influence the ability of an employee to work productively. The purpose of this study was to explore the interrelationship between work-related factors (job content, work limitations, and work–life balance) and current work ability in a diverse sample of working adults with diabetes.
Methods
This was a convergent mixed-methods study in which quantitative and qualitative data were collected concurrently in a convenience sample of 101 working adults with type 1 diabetes (T1D) and T2D. To achieve the aims of the study, the quantitative data were prioritized and the qualitative data were used to augment the quantitative findings (Creswell, 2014).
The Organization of Work conceptual framework guided this study (CDC, 2002). This framework included the inter-related and multi-level factors of the organization of work: external context (the changing worker demographic affected by increased prevalence of diabetes), organization context (organizational structure that facilitated or impeded diabetes self-management; ability to balance life and work), and work context (physical and psychological demands placed on the worker; the culture of the work environment). This framework allowed us to explore the relationships between work-related factors (job content, work limitations, and work–life balance), and work ability.
Study Sample
Approximately 2,624 individuals were invited to participate in our study through two methods: through a local academic medical center and ResearchMatch, a national online recruitment tool that matches adults interested in research with researchers throughout the United States (ResearchMatch, n.d.). Participants were eligible for participation if they were (a) currently employed either full- or part-time, (b) aged > 18 years, (c) diagnosed with T1D or T2D for at least 1 year, (d) able to read and understand English, and (e) able to access an email address to participate in the online surveys. They were excluded if they were (a) unable or unwilling to provide informed consent or (b) did not complete the study instruments.
Study flyers were distributed in the medical center and the principal investigator (PI) met with nursing personnel to describe the study. Over 10 months (November 2017–August 2018), 2,624 invitations were sent to potential participants through ResearchMatch, and those who were interested could agree to be further contacted about the study. The PI then confirmed inclusion and exclusion criteria with the potential participant. If all criteria were met, and the participant was still interested in the study, the PI would proceed with the consent process.
A subsample of adults from the total sample were asked to participate in the qualitative interviews which allowed for adequate data saturation. Maximum variation sampling (Creswell, 2014) was used to ensure that cases for the qualitative analysis provided the maximum heterogeneity on specific attributes (e.g., sex and occupation) that affect the variables of interest. Appropriate Institutional Review Board approval was obtained from New York University Langone Health for this study.
Data Collection
Telephone consent was obtained prior to sending the link to the surveys. Surveys were then administered online using Research Electronic Data Capture (REDCap) (Harris et al., 2009). The qualitative interviews were conducted by telephone, with subjects calling into a Webex audio conference number after they completed the quantitative data collection.
Work-Related Measures
The Job Content Questionnaire (JCQ) (Karasek et al., 1998) evaluated the psychological aspects of work and included five subscales (possible item range 1–4; higher scores are better): skill discretion (six items) (e.g., “My job requires that I learn new things”), decision authority (three items) (e.g., “My job allows me to make a lot of decisions on my own”), psychological demands (five items) (e.g., “My job requires working very fast”), coworker support (three items) (e.g., “People I work with are friendly”), and supervisor support (three items) (e.g., “My supervisor is concerned about the welfare of those under him”), with established reliability (previous α = .73). Responses were on a Likert-type scale ranging from 1 = “strongly disagree” to 4 = “strongly agree.” Scores were summarized for each individual scale. Cronbach’s alpha for our study was adequate (α = 0.81).
Work Limitations Questionnaire (Lerner et al., 2001) measured the degree to which health problems interfered with specific aspects of job performance and the productivity impact of these work limitations (e.g., “How much does your physical health or emotional problems make it difficult for you to handle the workload”) with adequate previous internal reliability (α = .90). Responses were on a Likert-type scale ranging from 0 = “does not apply to my job,” 1 = “all of the time,” to 5 = “none of the time.” The Questionnaire was scored on a continuous scale. The possible range was 14 to 35 with higher scores indicating greater difficulty completing work. Cronbach’s alpha for our study was adequate (α = .82).
Work–life balance was measured by Brett and Stroh’s balance scale (Brett & Stroh, 2003), a survey with established reliability (α = .79) that assessed the perception of the effect of work on physical and psychological well-being and ability to balance duties at work and home (e.g., “Feeling tension about balancing all your responsibilities”). Responses were on a Likert-type scale ranging from 1 = “never” to 5 = “very often.” The scores were summarized with a possible range of 5 to 25 with higher scores indicating poorer work–life balance. Cronbach’s alpha for our study was adequate (α = .86).
The Work Ability Index measured work ability conceptualized as ability to work at the present time, in the near future and with respect to work demands, health, and mental resources, with adequate test–retest reliability (de Zwart et al., 2002). Responses were on a Likert-type scale ranging from 0 = “cannot work at all” to 10 = “work is at best.” Items were summarized for a continuous score. The Cronbach’s alpha for our study was adequate (α = .92). A single item “How many points would you give your current ability to work?” was used for the bivariate and multivariate analyses (Ahlstrom et al., 2010). Clinical and sociodemographic characteristics were collected by an investigator-designed survey. All data were collected by self-report.
Finally, an investigator-designed questionnaire was used to collect self-reported sociodemographic and clinical data, including percent glycated hemoglobin (hemoglobin A1c %) and diabetes duration. The American Diabetes Association recommends a goal hemoglobin A1c of < 7% for nonpregnant adults (ADA, 2020).
Qualitative Measures
An interview guide was developed based on the Organization of Work conceptual framework, which allowed us to explore inter-related work factors such as the organizational structure, work–life balance, and workplace environment. The guide consisted of a series of open-ended questions (e.g., “tell me about living with diabetes” and “tell me about your job”) followed by more direct probes (“how does diabetes affect your ability to work?” and “do you feel supported at work in managing your diabetes?”) to focus the interview, while allowing the participant to speak freely. All interviews were recorded and transcribed verbatim.
Data Analysis
Descriptive statistics were calculated for all variables using SAS 9.4. The single-item question on current work ability was first categorized into poor (0–5), moderate (6–7), good (8–9), and excellent (10) and then dichotomized into 0–9 (poor–good) versus 10 (excellent). Bivariate analyses were conducted between work-related factors (variables all on a continuous scale) and work ability with analysis of variance (ANOVA). Work-related factors that were significant (p < .05) with work ability in the bivariate analysis were then entered into logistic regression model to identify factors independently associated with high work ability (10 or “excellent”). We also included diabetes duration and hemoglobin A1c % in the model. These two factors are known to be strongly associated with diabetes complications (Kosiborod et al., 2018; Teliti et al., 2018) and thus may impact work ability. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated and presented for all significant variables. Cronbach’s alpha was calculated for all surveys.
The analysis of the qualitative data was conducted using content analysis, an inductive analytic method using Atlas.ti (ATLAS.ti, n.d.). Preliminary analysis included a line-by-line review that yielded clusters of data that were labeled into brief headings. Headings included, for example, workplace environment, effect of workplace on diabetes, and support systems. Codes derived from this data were linked to interview questions and resulted in coding categories which at the early stage of analysis remained fairly general, descriptive in nature, and consistent with the study aims. As new codes emerged through the analysis process, revision to coding categories were made as indicated. Then coding categories were summarized across cases and subsequently cross-classified to yield a rich descriptive analysis. Finally, emerging themes both within and across coding categories were identified and review of the fit with descriptive data verified. Methodological rigor was maintained through an audit trail, and periodic peer debriefing was conducted through discussions at each stage of the coding and data analysis process with one of the authors (V.V.D.), who was an expert in mixed-method research design. Qualitative and quantitative data were integrated into the final analysis phase. First, using triangulation methods, qualitative evidence of work-related factors was compared with survey scores to establish patterns of concordance. Then, themes derived from the qualitative analysis were explored within cases then across cases to augment the quantitative findings (Ayres et al., 2003).
Results
A total of 197 individuals volunteered to be contacted for our study and 101 participants (51%) were enrolled with a mean age of 54.1 ± 10.5 years (Table 1). The sample was mostly female (65%), White (74%), and non-Hispanic (93%). The majority were employed full-time (65%), had T2D (87%), with a mean diabetes duration of 12.4 ± 9.5 years, and most were obese (68%) or overweight (22%). In addition, half (n = 56) reported a hemoglobin A1c ≥ 7%. Several reported complications from diabetes: neuropathy (38%), retinopathy (15%), heart disease (18%), and kidney disease (10%). The mean ± standard deviation of the JCQ subscales included the following: skill discretion (3.1 ± 0.45), decision authority (3.2 ± 0.64), psychological demand (2.7 ± 0.42), coworker support (3.0 ± 0.6), and supervisor support (2.9 ± 0.87). The mean ± standard deviation for work limitations questionnaire was 23.3 ± 6.5. The mean ± standard deviation for work–life balance was 11.72 ± 4.4. When asked to rate their current ability to work, 10% rated their ability poor, 16% moderate, 42% good, and 33% excellent (Table 2).
Sample Characteristics of Workers With Diabetes (n = 101)
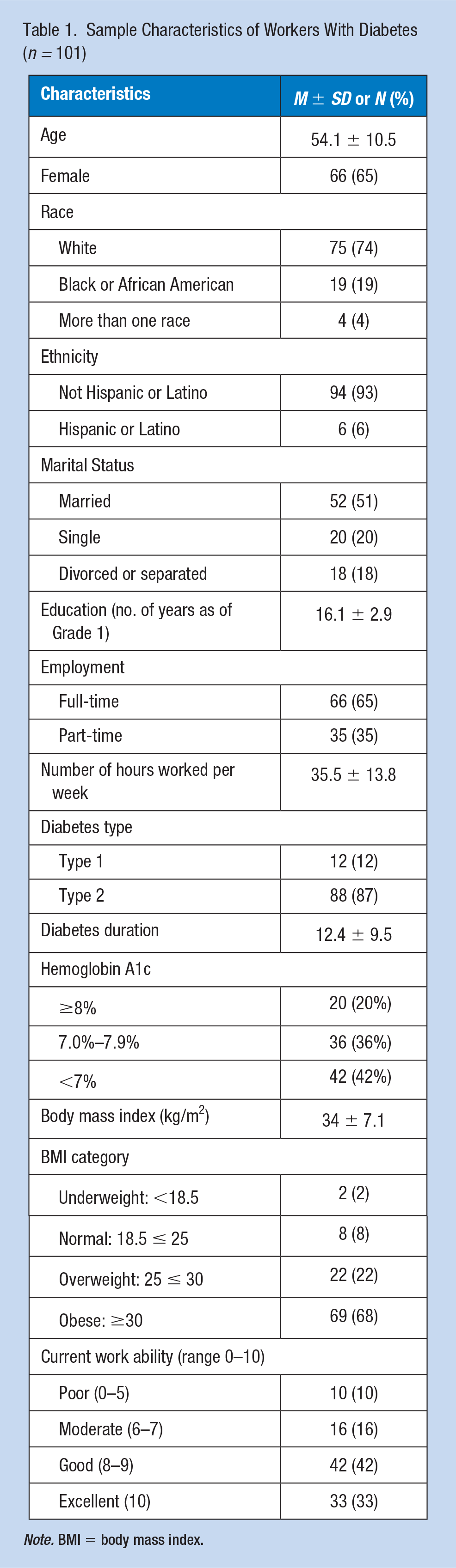
Note. BMI = body mass index.
Work-Related Factors Among Participants With Diabetes (n = 101)
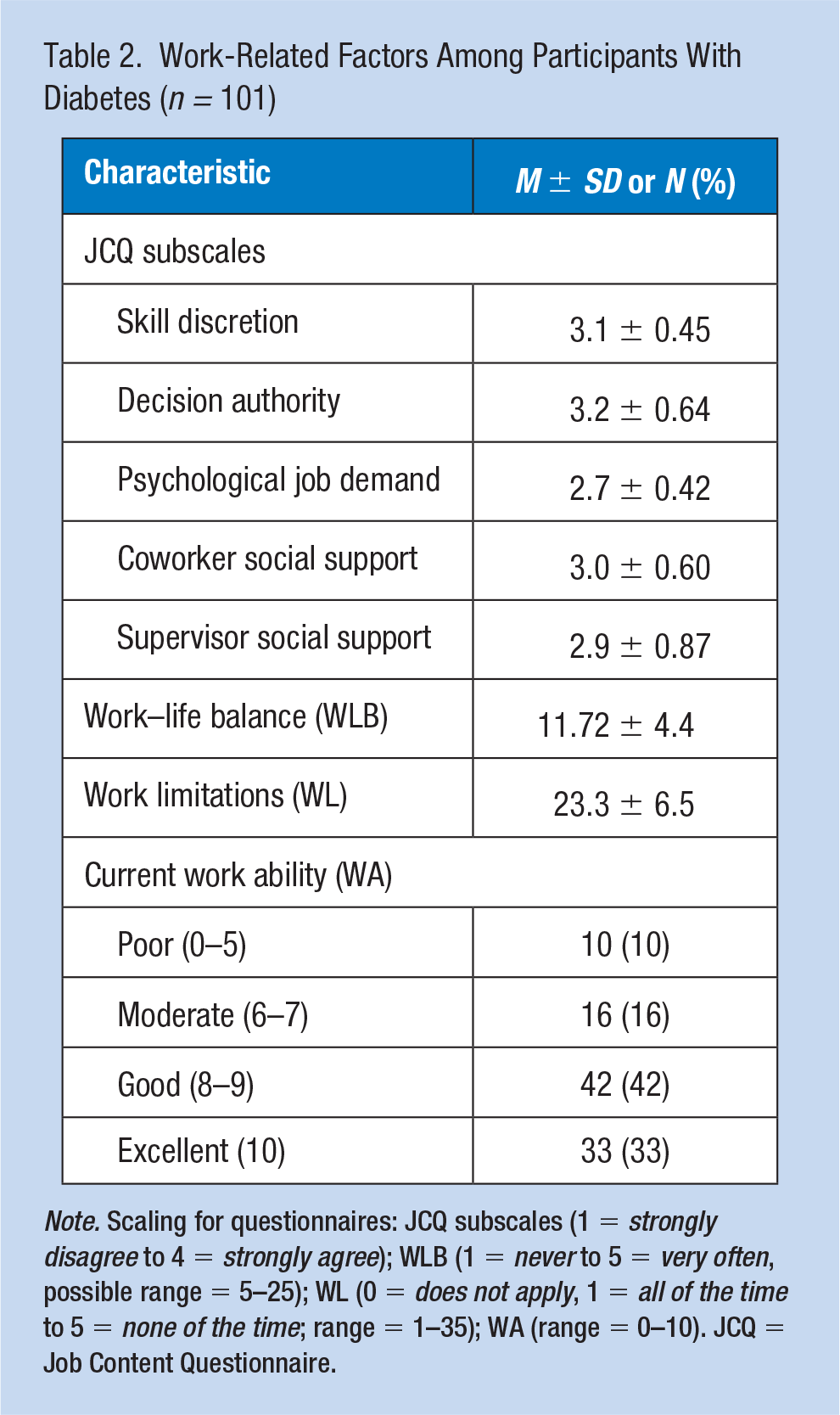
Note. Scaling for questionnaires: JCQ subscales (1 = strongly disagree to 4 = strongly agree); WLB (1 = never to 5 = very often, possible range = 5–25); WL (0 = does not apply, 1 = all of the time to 5 = none of the time; range = 1–35); WA (range = 0–10). JCQ = Job Content Questionnaire.
Work-Related Factors Associated With Work Ability
In bivariate analyses using ANOVA, five factors were significantly associated with the work ability score: four of the JCQ subscales: skill discretion (p =. 02), psychological demands (p = .006), supervisor support (p = .03), coworker support (p = .0007), and the total work–life balance scale (p < .0001). All four JCQ subscales were higher, and the total work–life balance score was lower in those reporting excellent work ability. In the final logistic regression model that included all of the above five factors, as well as hemoglobin A1c and duration of diabetes, two independent factors remained significantly associated with the outcome of excellent work ability: coworker support (OR = 1.4; 95% CI = [1.04, 1.9]) and total work–life balance (OR = 1.3; 95% CI = [1.1, 1.5]) (Table 3). As coworker support increased, the odds of working at their best improved, and as scores in work–life balance decreased (indicating better work–life balance), the odds of working at their best increased.
Multivariate Modeling of Work-Related Factors on Work Ability (n = 101)
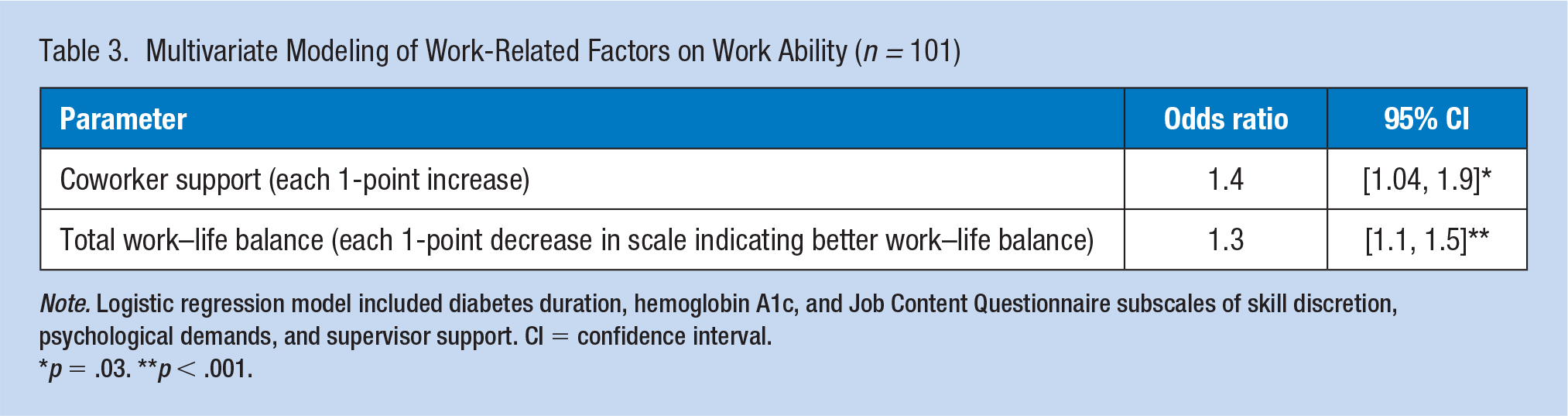
Note. Logistic regression model included diabetes duration, hemoglobin A1c, and Job Content Questionnaire subscales of skill discretion, psychological demands, and supervisor support. CI = confidence interval.
p = .03. **p < .001.
Qualitative Results
When asked whether their work interfered with diabetes self-management, half the participants stated that work had no impact on their self-management. They spoke of being on a regular schedule and being able to eat and check their blood glucose as needed. One participant, a 41-year-old male with T2D stated, “I’m able to check my blood sugar at my desk when I need to. Literally, that’s about the only diabetes-related task that I have to do at work.” Others felt diabetes tasks were impacted by their work schedule. One participant, 56 year-old, female, with T2D stated “You have to stop—many times when you’re doing a lot of work you forget to take your blood sugar. You forget to take the insulin . . .” Participants were also asked if their diabetes affected how they worked. The majority (n = 17) stated yes, their diabetes impacted them at work. Several spoke of the effects of stress. One participant (60-year-old female) with T2D stated, “I know now that I can’t take stress because then my blood sugar goes way up.” Another (53-year-old female) with T2D stated “It does occasionally because sometimes I’m in very stressful situations . . . and I don’t get to eat lunch on time and sometimes, it’s hard.” Others also spoke of dealing with the highs and lows of blood glucose. A 52-year-old female with T2D stated, “Initially, it affected me ‘cause when my sugar level was very high, I was constantly thirsty, constantly going to the bathroom.” A 40-year-old female with T2D remarked, “Well obviously, when my blood sugar is running low, I can be a little irritable.” A 38-year-old male with T1D stated, It’s one of those things that’s in the background. I have to remember to check in the morning, and then I usually eat a snack at the same time every day to make sure I don’t get lows while I’m working.
Of those who denied any impact of diabetes on their work, it was almost equally split between female and males (six and seven, respectively).
Participants were asked about social support from colleagues or supervisors, as well as workplace programs. Many spoke of not sharing details of their diabetes with colleagues. A 52-year-old female with T2D stated, “No, diabetes to me is something personal,” expressing similar sentiments to other participants: “most people don’t know unless I’ve told’ em” (57-year-old male, T2D); “I keep the workplace and private life as separate as I can” (70-year-old male, T2D); “Nobody knows I have it.” (66-year-old female, T2D). Most participants (n = 16) were not aware of any workplace wellness programs, and for those who had access to a program did not appear to be engaged in the program. One participant (61-year-old male, T2D) stated “. . . what I would call a wellness program, that they have different things each month . . . they try to encourage healthier habits”; another participant (72-year-old female, T2D) stated, “There are wellness plans here and wellness counselors that would be more than happy to assist.” A 51-year-old female with T2D expressed, “Yeah. I guess, through our insurance, yeah. I have access to a health coach.”
Of those participants who rated their current ability to work as excellent, several spoke of the large degree of control or flexibility they have at work: “That’s the beauty of it. I have total control . . .” (70-year-old male, T2D); “I’ve got pretty much full control because there’s no one around to watch me . . .” (65-year-old male, T2D); “Quite a lot of control. On my own schedule . . .” (62-year-old male, T1D); “A pretty good amount. I have guidelines that I need to follow and material that I need to cover, but in terms of day to day and how I do that, it’s largely up to me” (38, male, T1D); “My job is with obvious flexibility” (38-year-old male, T1D). One subject expressed a desire to keep his personal life out of work “I keep the workplace and private life as separate as I can because I really don’t want them to co-mingle” (70-year-old male, T2D). However, only a few spoke of support at work: “They give us a lot of options how to stay healthy with different programs that we can get into and access to nurses and doctors” (65-year-old male, T2D); “several of ‘em have it, so they’re familiar” (49-year-old female, T1D). In contrast, two participants who rated their current work ability as poor spoke of the effect of their diabetes and health on their ability to work: “Sometime if I’m not feelin’ good at work, I just—sometimes I have to shut it down” (50-year-old female, T2D); another stated, “I’ve got neuropathy” (54-year-old female, T2D). When asked about the effect of her diabetes on working in the short term, she added, “because of all the ups and downs that go on, that I would be taking too much time off work in order to hold a job.”
Discussion
In this sample of working adults with diabetes, the majority rated their work ability as good to excellent, with half reporting in the qualitative interviews that work had no impact on their diabetes self-management. Coworker support and work–life balance were independently associated with reporting an excellent work ability. However, this positive outlook on work was in contrast with their diabetes and health status. The majority reported a hemoglobin A1c ≥ 7% and were overweight or obese, putting them at higher risk for cardiovascular disease.
Interventions to support workers with chronic illnesses like diabetes may improve diabetes self-management and thereby cardiovascular health. One program, Stanford’s chronic disease self-management program, focused on lifestyle and disease-related factors such as coping with symptoms. This intervention led to improvements in participants’ attitudes toward self-management, which may be the first step in improving health outcomes (Nazarov et al., 2019).
Despite our findings that increased social support was related to excellent current work ability, several participants spoke of not wanting to disclose their diabetes at work. This is unfortunate given the workplace may be a place to learn about coping with diabetes. In a survey of open-ended questions for adults (n = 328) with T1D and T2D, work as a context for learning about diabetes, either from colleagues or through routine health checks, was a theme that emerged from the data (Cleal et al., 2019). Another emerging theme regarded social support, which included emotional support but it was the practical help from colleagues that was especially helpful in dealing with diabetes at work.
Social support may differ in those with T2D as compared with T1D in general, unrelated to work. In a cross-sectional study of the social aspects of diabetes, researchers compared social relations in adults with both types of diabetes (Hempler et al., 2016). In that sample, adults with T2D had fewer social contacts with family and friends as compared with those with T1D, and this difference was stronger in women. Those with T2D also felt less able to count on the social support of others in case of severe illness. The majority of our sample had T2D, and although greater coworker support was associated with increased odds of reporting excellent work ability, some may still feel a wariness of sharing personal health details at work.
Better work–life balance was also associated with excellent work ability in our sample. This was not an area that was specifically explored in the qualitative interview so we do not have a full understanding of this relationship. Subjects who reported excellent work ability also reported a greater degree of control or flexibility and an ability to keep work and personal life separate. It is possible that those who report better work–life balance had a schedule that allowed time for health-promoting behaviors such as routine blood glucose checks, taking medication on time, preparing nutritious meals, and getting adequate physical activity. Results from an integrative review on work–life balance indicated that better work–life balance was associated with positive effects on health, life satisfaction, and job performance, while poorer work–life balance was associated with increased anxiety, depression, hypertension, cholesterol, and smoking (Sirgy & Lee, 2018). If these negative outcomes occurred in adults with diabetes, this may explain our findings of the association between better work–life balance and excellent work ability.
Although several participants spoke of having a degree of control over their workday in the qualitative interviews, the JCQ subscale of decision authority was not significantly associated with work ability. It may be these adults, perhaps because of strong coworker support, had a positive attitude toward work ability. They also may not be considering their diabetes when they think about work, as evidenced by some participants wanting to keep their diabetes status separate from their work. This may explain a similar pattern seen in a study of working adults with diabetes where work-related psychosocial stress (which included subscales of decision authority, job demands, coworker and supervisor support) was not associated with glycemic control (Annor et al., 2015). In contrast, these work-related factors have been associated with cardiovascular health in working adults (Rocco et al., 2017). In a large sample of active workers aged 35 to 74 years (though not specifically with diabetes), participants with low decision authority and low social support (as measured by the Swedish Demand Control Support Questionnaire) had poorer cardiovascular health scores. Although these two studies examining the relationship between work-related factors and physiologic outcomes appear contradictory, these factors (job content, glycemic control, and cardiovascular health) are important to consider and can be explored in future research to extend our understanding of how work impacts the health of adults with diabetes.
Finally, we found the majority of this sample of working adults with diabetes had an elevated hemoglobin A1c and were also overweight or obese. This is troubling given their high risk for cardiovascular disease mortality (Duca et al., 2013). It is possible some kept their blood glucose deliberately elevated at work to avoid hypoglycemia. This pattern was seen in a sample of working adults with T1D (n = 1,030), where almost one third reported keeping their blood glucose elevated while at work, which was then associated with poorer glycemic control (Hansen et al., 2019). For some, the work environment may be a barrier for optimal diabetes self-management, including healthy eating. This may include those who travel for work and have difficulty finding healthy foods to eat, or those who found that work-related stress impacted their glycemic control (Adu et al., 2019). How these risk factors for cardiovascular disease are managed may have consequences on work ability in the future.
This study was a cross-sectional analysis of patient reported data. Therefore, we are unable to infer a causal relationship between our independent work-related variables and our outcome of interest work ability. The majority of participants had T2D, and their responses and experiences may differ from those with T1D. Despite these limitations, this mixed-method study fostered our ability to identify factors related to excellent work ability and explore the experiences of adults as they manage their diabetes and work responsibilities.
Implications for Occupational Health Practice
Managing both diabetes and work can be a challenge for some working adults, but one that has an impact on their future health and work ability. According to the American Association of Occupational Health Nurses (“Health and Productivity: The Occupational and Environmental Health Nurse Role,” 2013), innovative programs that support workers in managing chronic diseases like diabetes are needed to help address issues like low productivity, high worker turnover, and the increasing health care and disability costs associated with worker health problems. Occupational health nurses with their unique training (“Delivery of Occupational and Environmental Health Services,” 2013) play an important role in supporting workplace wellness initiatives like the National Institute for Occupational Safety and Health’s Total Worker Health Program (CDC, 2020) that integrate occupational safety and health protection with health promotion to advance worker health and well-being.
Conclusion
In summary, we identified work-related factors that were associated with excellent work ability. Although one third reported excellent work ability, glycemic control and body mass index levels were less than optimal. These are areas of needed improvement in this sample of adults with diabetes, and workplace policies may support this endeavor. However, additional research is needed to test workplace interventions aimed at improving overall health that will engage workers with diabetes.
Applying Research to Occupational Health Practice
This cross-sectional mixed-methods study explored the association between work-related factors and work ability. Our sample of 101 working adults with diabetes (87% with T2D) completed online surveys on work-related factors. This sample was majority female, White, married, and worked full-time. One third rated their current work ability as excellent. Better coworker support and work–life balance were associated with excellent work ability. However, the majority of the sample were overweight/obese with suboptimal hemoglobin A1c. Strategies are needed to continually engage workers with diabetes in occupational health programs for diabetes education and support. Emphasizing healthy eating and exercise, in addition to checking blood glucose and taking medications, may help improve the workers’ hemoglobin A1c and body weight, thereby reducing their long-term risk of cardiovascular disease, and thus, improving long-term work ability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a New York University Research Challenge Fund award.
Author Biographies
Margaret McCarthy is an assistant professor at the Rory Meyers College of Nursing, New York University.
Allison Vorderstrasse is professor and dean at the College of Nursing, University of Massachusetts Amherst.
Joeyee Yan is undergraduate student at the Rory Meyers College of Nursing, New York University.
Angie Portillo is undergraduate student at the Rory Meyers College of Nursing, New York University.
Victoria Vaughan Dickson is an associate professor and director of the Pless Center at the Rory Meyers College of Nursing, New York University.