
Abstract
Background
Tinnitus (ie, ear or head noises not caused by external sounds) is common among the general population and is the most prevalent service-connected disability in the United States’ Department of Veterans Affairs system. While numerous clinical interventions have been created to systematically address the range of issues caused by tinnitus, only a few tinnitus interventions have focused on both teaching and assessing coping strategies. The present pilot study involved a randomized clinical trial comparing 3 brief group interventions to a usual-care (UC) group (ie, a wait-list control group): the first intervention based on acceptance and commitment therapy (ACT), a second based on cognitive-behavioral therapy (CBT), and a third based on coping effectiveness training (CET). Each intervention group also received tinnitus-related audiological education.
Participants
Forty individuals met the eligibility requirements and were randomized into 1 of the 4 groups (ACT, CBT, CET, or UC). An intent-to-treat analysis was used in this study.
Measures
The Brief COPE scale was used to assess coping. Coping was assessed at 3 time points (pre-intervention, post-intervention, and at 4-week follow-up). The outcomes were 3 coping factors (engagement coping, disengagement coping, and social support coping).
Results
When examining differences among the groups on mean coping scores over time, significant group differences were found on social support coping, with the CET group scores significantly higher than the UC group.
Discussion
While all 3 brief interventions teach stress-reduction techniques, ACT and CBT focus primarily on managing one’s unwanted thoughts and emotions. CET teaches participants both a range of coping strategies (eg, stress-management approaches) to more effectively manage stressors that cannot be changed, as well as coping strategies (eg, such as problem-solving) that can be used to eliminate stressors that can be changed. CET also teaches communication skills for telling others about one’s tinnitus-related issues. CET instructs individuals on how to select coping strategies that are appropriate for different kinds of stressors and how to seek social support, which is a skill not explicitly taught by ACT or CBT. Results of this study were derived from a small sample size, and thus, future research should focus on replicating the results among a larger sample. In addition, future research could focus on adapting the CET intervention to a different delivery format.
Keywords
Introduction
Tinnitus is the most prevalent service-connected disability in the United States’ Veterans Affairs (VA) system. 1 Tinnitus also is a common chronic condition among the general population: Approximately 30 million people in the United States have chronic tinnitus, and of that 30 million, it is estimated that 7.2% describe their tinnitus as a big or a very big problem. 2 Prevalence estimates by other researchers vary from 2.4% to 30% of the population.3–5
There is no current cure for primary tinnitus. Individuals with tinnitus often are told by clinicians that “little or nothing can be done to help them.” 6 Many individuals may experience negative emotions, such as anxiety and depression, because of their tinnitus, 2 especially if healthcare professionals have not provided them with any options for managing tinnitus-related stress. Yet, management strategies for tinnitus exist that can help increase individuals’ coping with stress triggered by their tinnitus. The purpose of the present pilot study was to compare 3 brief group interventions that were designed to increase coping with tinnitus. Each intervention was based on 1 of the 3 existing interventions: acceptance and commitment therapy (ACT), cognitive-behavioral therapy (CBT), and coping effectiveness training (CET). These specific interventions were chosen for study because (1) CBT has the strongest evidence base for tinnitus management6,7; (2) ACT, as an alternative to CBT, has been shown to be efficacious for tinnitus management in 2 randomized controlled trials8,9; and (3) CET appears particularly well-suited to address coping with tinnitus as an unchangeable stressor.10,11
Coping With Tinnitus
Coping strategies are typically defined as cognitive, affective, and behavioral attempts to master new events, such as the onset of a chronic health condition or disability, for which an individual does not necessarily have automatic, adaptive responses.12–14 Coping strategies have been categorized in numerous ways, and Lazarus and Folkman’s 13 model proposed 2 broad, theory-based categories: (a) problem-solving coping, which targets changing the source of the stress, and (b) emotion-focused coping, which targets managing emotional reactions to the stress. Other categorizations of coping strategies have been proposed.15–17
A critical element in Lazarus and Folkman’s 13 theory is whether people appraise each stressor as changeable or unchangeable (eg, having tinnitus is an unchangeable stressor because it cannot be cured or eliminated). Adaptive coping occurs when there is a “fit” between changeability of stressor and the coping strategy employed. Non-adaptive coping occurs when there is a lack of fit between changeability of stressor and the coping strategy employed, such as when a person repeatedly responds to an unchangeable stressful situation with problem-focused coping or relies on emotion-focused coping when confronted with a changeable stressor that could be resolved with problem-focused coping. 18 Clinical research supports this theory, showing that when there is a poor fit between employed coping strategies and situational demands, people experience more psychological symptoms than when there is a good fit. 19 Further, a meta-analysis that focused on coping flexibility found that a better fit between the coping strategy and the situation was moderately associated with psychological adjustment across 90 empirical studies. 20
Research on coping styles and tinnitus has indicated that when compared to individuals with hearing loss, individuals with tinnitus use more avoidant coping styles. 21 Further research indicates that individuals with tinnitus who use non-adaptive (ie, “maladaptive”) coping styles experience either higher levels of anxiety, depression, and tinnitus-related distress than those who used more effective coping styles22,23 or higher levels of anxiety and depression. 24 In a mixed methods study, a group categorized as using a passive coping style for problematic situations had significantly higher levels of distress, anxiety, and depression than the groups categorized as habituating or using active coping styles. 25 Given the evidence that many individuals with tinnitus experience distress related to the use of non-adaptive coping strategies, efforts to evaluate the efficacy of new and existing coping interventions for tinnitus would appear worthwhile.
Psychoeducational Interventions
Acceptance and commitment therapy
ACT is an approach that has recently been studied as an alternative intervention for tinnitus. ACT promotes the development of psychological flexibility.26–28 ACT seeks to help individuals learn how to reduce the resistance to, and avoidance of, distressing thoughts and emotions by adopting mindfulness. The approach teaches how to accept patterns of reactions (both thoughts and emotions) while encouraging people to increase committed action based on individual values.
Two studies have examined ACT in the context of tinnitus. Westin et al. 9 compared ACT to another treatment, tinnitus retraining therapy (TRT), 29 and to a wait-list control (WLC) group. Findings indicated that the ACT group exhibited significantly lower tinnitus impact scores than the control group at 10 weeks, and the ACT group had lower tinnitus-related distress than the TRT group at 18 months post-treatment. Hesser et al. 8 conducted a study using 2 self-help internet treatments based on ACT and CBT. Both ACT and CBT groups exhibited significant decreases in tinnitus distress when compared to a control group at 8 weeks.
Cognitive-behavioral therapy
CBT is one of the most commonly used psychological interventions for tinnitus. It seeks to reduce mental distress by altering cognitive distortions, automatic thoughts, and core beliefs and uses behavioral techniques to reduce physiological arousal (eg, relaxation). 30 Several meta-analyses on the efficacy of CBT interventions for tinnitus have reported discrepant findings. The first examined 8 CBT interventions for tinnitus and found that CBT was not likely to decrease tinnitus severity (ie, loudness) but was likely to decrease depression and increase quality of life. 7 A second meta-analysis of 15 studies of CBT reported that CBT interventions showed significant improvement on tinnitus-related distress, as well as a significant improvement on anxiety and depression. 31 A third meta-analysis examined 11 CBT randomized clinical trials (RCTs), dividing 8 studies into 3 comparable groups based on research design, and concluded that CBT showed significant improvement on tinnitus intrusiveness or severity, but there is little evidence that it helped reduce depression or anxiety. 32 Possible explanations for these disparate findings include the differing definitions of CBT and criteria employed by the research teams for including studies in the analyses. Nevertheless, CBT is recommended by the American Academy of Otolaryngology/Head and Neck Surgery for clinical management for bothersome tinnitus. 6
The 3-session CBT intervention used in the present research was the protocol from a program called progressive tinnitus management (PTM). 33 PTM was recently reported to be effective based on a 2-site RCT that found that PTM significantly decreased tinnitus distress compared to a wait-list group at a 6-month follow-up. 34
Coping effectiveness training
CET 10 is a psychosocial intervention that provides training in a range of coping strategies. CET includes teaching a framework for appraising stressors, identifying their changeable and unchangeable aspects, learning new coping skills, and selecting appropriate coping strategies to implement to reduce their health-related stress (eg, problem-focused strategies for changeable situations and emotion-focused strategies for unchangeable situations).10,11
CET was originally created by Chesney and her coworkers10,11 to assist individuals diagnosed with HIV/AIDS, which similarly to tinnitus, has both changeable and unchangeable stressors. CET teaches that while some aspects of individuals’ lives and health challenges are unchangeable (eg, tinnitus), other aspects of their lives and health challenges are changeable (eg, finding a more understanding physician, changing one’s sound environment), and people can be taught to apply the appropriate coping strategy to the type of stressor they are confronting.
Evidence has shown that CET is effective in facilitating adaptive coping strategies among individuals with several types of impairments or disabilities.11,35–37 An RCT comparing CET to both an HIV-information group and a WLC indicated that individuals in the CET group exhibited significant increases in coping, as well as decreases in perceived stress and burnout compared to both HIV-information and WLC groups. 35 They also reported decreases in anxiety and improvements in positive states of mind compared to the WLC group. Further, in another study investigating the effects of CET on coping among individuals with HIV/AIDS, individuals who received CET maintained improvements in positive states of mind and personal growth, compared to individuals who received usual care with periodic support telephone calls at 6- and 12-month follow-up. 38
Given the need for brief interventions to help Veterans better cope with their tinnitus, the research question of this pilot study was as follows: Are there any differences on self-reported coping among 3 brief stress-management intervention groups, ACT, CBT, or CET, over time, in individuals with tinnitus, compared with a usual-care (UC) group?
Methods
Study Design
The present pilot RCT was designed to compare the effectiveness of abbreviated forms of ACT, CBT, and CET using a 5-session structure of the PTM program. 33 The PTM model contained 3 psychoeducational sessions and 2 audiological education sessions. In the present pilot study, the 3-session CBT component was compared to 2 other brief 3-session interventions based on ACT and CET and a UC group, which was a WLC group.
Recruitment and Screening
This pilot study was approved by the VA Portland Health Care System (VAPORHCS) Institutional Review Board. Both Veterans and civilians were recruited using a variety of recruitment methods (eg, flyers were posted at approved sites within the VAPORHCS, and internet and newspaper advertisements were also posted) to reach both Veterans and civilians with tinnitus in the Portland metropolitan area. 2 focus groups of Veterans with tinnitus were conducted prior to this study that provided feedback regarding the material to be covered in the brief interventions and participant workbooks. Out of the 87 letters mailed, 31 responses were received, and 8 individuals participated in 1 of the 2 in-person focus groups. Following the completion of the focus groups, recruitment and screening for the pilot RCT continued over the course of approximately 6 months until the recruitment goals were met.
Inclusion criteria were the following: (1) report experiencing tinnitus; (2) a score of at least 21 on the Tinnitus Functional Index (TFI)39,40; (3) 2 errors or less on a 6-item cognitive screening instrument 41 ; (4) English-speaking; (5) willing and able to give written informed consent; and (6) use hearing aids if needed. If the audiological assessment indicated that an individual needed the use of hearing aids, then they were required to obtain them prior to participating in the study because the study involved group interventions with discussions. Exclusion criteria were (1) not meeting inclusion criteria 1–6; (2) having previously participated in the PTM program or 1 of the 2 focus groups held at the beginning of this pilot study; and (3) having any other factor that would preclude full participation in the study.
Participants
The number of potential participants requesting information about the pilot study was 195 (see Figure 1 for the recruitment flowchart). Of the potential participants who were screened, 78.5% were Veterans and 21.5% were civilians. Of the randomized participants, 80% (n = 32) were male and 20% (n = 8) were female. The mean age of the sample was 57.81 (SD = 16.41). The ethnicity of this sample consisted of 92.3% White, 2.5% African American, 2.5% Hispanic, and 2.5% Other. The marital status was 40% married, 30% single, 22.5% divorced, 5% widowed, and 2.5% separated. The mean educational level was 15.05 (SD = 2.01). The employment status was 45.9% retired, 16.2% employed full-time, 16.2% not employed, 10.8% employed part-time, 8.1% students, and 2.7% volunteers. Sixty-five percent of the participants reported experiencing their tinnitus as constant, while 35% reported experiencing tinnitus intermittently.
Recruitment Flow Chart.
Randomization and Allocation
A power analysis using G*Power 42 for repeated measures indicated that at an alpha of .05, a power of.95, an effect size of 0.2, and a sample size of 32 were needed. An effect size of 0.2, which is considered a small effect, was used in view of the fact that the psychoeducational groups relied on somewhat similar intervention strategies; thus, large differences were not expected among the groups.
This pilot study was not part of a larger clinical study. The screening instruments that were used for determining eligibility (eg, TFI, a 6-item cognitive screening instrument 41 ) were not used in the data analyses because they had been used earlier to establish eligibility for participation in the study.
Once 40 individuals passed all eligibility and screening requirements, recruitment was closed. The 40 participants were randomized into 1 of the 4 groups (ACT, CBT, CET, or UC) using the following procedures. A random number generator was used, blocking by 10 per group to assure equal and balanced numbers in each group. Randomization software provided the randomization sequence. An equal number of individuals were allocated to each of the 4 groups. Allocation concealment was achieved by using the sequentially numbered, opaque, sealed envelopes method.43,44 Participants were not blinded to intervention assignments because they had to be notified about their group assignment (eg, an intervention vs UC [wait-list] group) after the randomization and allocation processes were completed.
Procedures
Content of the 3 Brief Interventions.

Abbreviations: ACT-T, acceptance and commitment therapy for tinnitus; CBT, cognitive-behavioral therapy; CET, coping effectiveness training.
This table does not include descriptions of the opening and closing procedures that are standard in psychoeducational groups (eg, group rules, confidentiality, introductions). For all 3 interventions, each session was 2 hours long, and both PowerPoints and workbooks were used.
The UC group received an intervention from the research team after the 1-month follow-up data were obtained from the participants. The 3 weekly psychoeducational sessions were taught by 2 co-leaders, who rotated through the 3 groups (2 PhDs and 1 master’s degree, all with clinical training in psychology and/or counseling). The 2 weekly sessions of the audiological group education were taught by an audiologist who had specialized training in tinnitus. The audiological sessions involved explanations on why and how to use sound enrichment techniques, information on the types of sound that individuals can use in sound enrichment, instructions on how to create a sound plan for using various types of sound targeted toward specific problem situations related to tinnitus, and explanations on how to protect one’s hearing from further damage.
Each weekly session lasted up to 2 hours. In the first session, participants received an intervention-specific self-help workbook that they could keep 45 (E. Martz, M.A. Chesney. Coping Effectiveness Training for Tinnitus [Unpublished manual]. Veterans Affairs Portland Healthcare System, Portland, Oregon; 2017; E. Martz, B. Fuller, C. Jelleberg. Acceptance & Commitment Therapy for Tinnitus (ACT-T) [Unpublished manual]. Veterans Affairs Portland Healthcare System, Portland, Oregon; 2017).
Measures
Coping: The Brief COPE scale
46
was used to assess coping. The COPE is a widely used 28-item short form of the COPE Inventory.
47
It has been used with a wide range of people with disabling conditions, including those who have sensory limitations. This instrument measures 14 coping subscales. Each item is scored using a 1–4 frequency scale (ie, 1 = “I haven’t been doing this it at all” to 4 = “I’ve been doing this a lot”), where higher scores reflect greater use of the coping strategy. Carver’s
48
website about the Brief COPE suggests that a total score should not be used, and the factor structure should be examined for each sample. Given that in the present study, the sample size was small (N = 40), it was inadvisable to run a factor analysis. Hence, a 3-factor structure was used, based on the factorial structure of the Brief COPE found among samples with a variety of chronic health conditions.49–52 The 3 factors, with the relevant subscales, were as follows: (a) Engagement coping (EC), including active coping, positive reframing, planning, acceptance, self-distraction, and use of humor (items n = 12); (b) disengagement coping (DC), including denial, behavioral disengagement, and self-blame (items n = 6); and (c) social support coping (SS), including instrumental support, emotional support, venting, and religion (items n = 8). Two items related to alcohol and drugs were not included. For this sample, the Cronbach’s alpha for the 3 factors was the following: (a) EC = .83; (b) DC = .76; and (c) SS = .80. Sociodemographic variables: Information about sociodemographic and tinnitus-related variables was collected during the intake and included the following: age, gender, ethnicity, marital status, educational level, and employment status. Basic information about tinnitus was also collected.
Data Analysis
Data on participants were collected at 3 time points: during intake (baseline, T1); at the end of the 5 sessions (T2); and 4 weeks after the end of the sessions (T3). The 4-week follow-up was chosen because the nature of the pilot study allowed for only a constricted period of time to complete the study. The UC group, which was a WLC group, was assessed at all 3 time points, approximately parallel to the assessments made for participants in the 3 intervention groups. Once the final assessment had been completed, UC group participants were offered a choice of receiving CET or CBT. No adverse events (eg, suicidal thinking) were reported during any of the group sessions.
For the intent-to-treat analysis, missing data were imputed by SPSS version 22.0 by replacing the missing values using linear interpolation.53,54 The alpha was set at .05 across this study. Prior to undertaking the analysis that addressed the research question, the outcome variables were examined for possible associations with sociodemographic variables and for possible differences among the 4 groups at T1 (after randomization into groups). The zero-order correlations of age and level of education with the coping outcomes were not significant. The analyses of variance (ANOVAs) of gender and tinnitus type and the coping outcomes were not significant. Further, separate ANOVAs were run on all 3 dependent variables at T1 with group assignment (ACT, CET, CBT, or WLC) as the grouping variable; none of the 3 ANOVAs were significant (P values were the following: EC, P = .32; DC, P = .47; SS, P = .41). These non-significant findings suggest that the randomization and allocation processes were sufficiently robust to minimize differences in baseline characteristics (at T1) of this sample.
The research question of this pilot study was addressed by using a multivariate analysis of variance (MANOVA) with the dependent variables as the coping factors. The MANOVA procedure was used to answer the research question, given that moderate correlations were expected among the 3 factors of the Brief COPE as dependent variables. 55 Before conducting the analysis, MANOVA assumptions were checked, including linearity, normality, multicollinearity, and equality of variance-covariance matrices. 56 The linear relationship of the dependent variables was assessed by bivariate correlations and scatterplots. The Shapiro–Wilk statistic and Q-Q plots were run to assess normality on each dependent variable across the between-group factor (group assignment). The Shapiro–Wilk statistic was not significant for any of the 3 coping factors across all 4 groups, which suggested normality. Multicollinearity was assessed by examining the correlation of the dependent variables; none exceeded the .8 limit suggested by Stevens. 57 To answer the research question about the effect of group assignment on coping scores over time, this study used a mixed design with 2-way (MANOVA), 56 a form of repeated measures MANOVA. The within-group factor represented individuals’ scores on outcome variables over 3 assessment points. The between-group factor represented the group assignment (ACT, CBT, CET, or UC groups).
Results
All 40 participants provided full sets of data at baseline at T1. At T2 (ie, at the end of 5 sessions for the intervention groups and at a parallel time for the UC group), 62.5% of the participants provided data on coping outcomes. At T3 (a 4-week follow-up for all 4 groups), 60% of the group provided data on coping outcomes. No further data were gathered on the UC group after the final assessment at time 3. The following were the percentages of completers of each intervention group: CET = 60%; ACT = 70%; and CBT = 40%.
Differences Over Time
Means and Standard Deviations of Groups on Coping Outcomes.

Data listed as mean and standard deviation.
T1: Time 1, baseline.
T2: Time 2, at the end of 5 sessions for the intervention groups and at a parallel time for the UC group.
T3: Time 3, at 4-week follow-up for all 4 groups.
Because of the significant multivariate interaction, the simple effects (ie, univariate effects) were examined. For all 3 factors, Mauchly’s test of sphericity was significant, indicating that sphericity could not be assumed. Thus, Greenhouse-Geisser correction was used in the interpretation of the univariate tests. There were no significant interactions at the univariate level between-group factor (group assignment) and within-subjects factor (time) on EC, DC, or SS using the Greenhouse-Geisser correction. Levene’s test of equality of error variances of the dependent variables across groups was significant for 4 of the 9 data points of the 3 factors (EC T3, DC T1, T2, and T3), while the other 5 data points were not significant. Thus, variances were assumed to be equal across the EC and SS measures, but not the DC measure. The effect of between-subjects (group assignment) on SS was significant, F(3, 93.71) = 3.13, P = .037, with a partial ɛ2 = .21 (see Figure 2). Pairwise comparisons of the between-group factor (group assignment) on the 3 coping factors indicated only 1 significant pairwise comparison of intervention groups compared to the UC group: between CET and the UC group on SS, mean difference = 4.21, P = .03.
Differences Between Groups Over Time on Social Support Coping.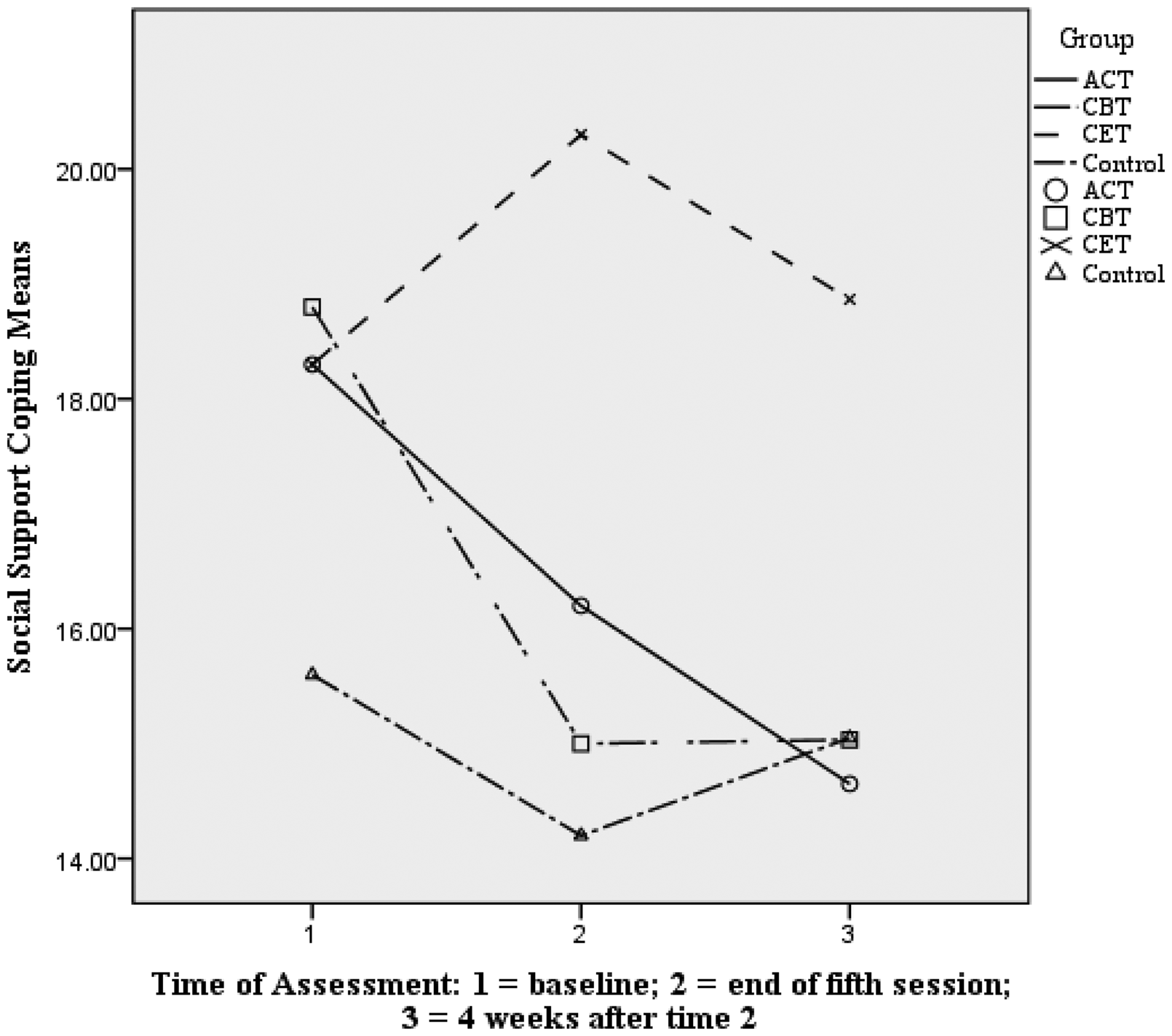
One other pairwise comparison of intervention groups contrasted with the UC group failed to reach significance: between CET and the UC group on EC, mean difference = 4.26, P = .097 (see Figure 3).
Differences Between Groups Over Time on Engagement Coping.
Discussion
The purpose of this pilot study was to examine the influence of 3 brief psychoeducational interventions, when taught along with audiological education sessions, on individuals’ coping strategies. When examining differences among the groups on mean coping scores over time, significant group differences were found only on SS, with the CET group scores significantly higher than the UC group. One explanation for those significant differences is that CET provides targeted coping education not only about problem-solving and stress-management techniques but also about how to seek appropriate social support (eg, help or advice about problems or empathic listening) from others.
While all 3 interventions teach that tinnitus itself is a chronic condition that cannot be changed and all 3 interventions teach stress-management approaches (eg, relaxation), CET is the only 1 of the 3 interventions that teaches a framework on how to evaluate the kind of coping strategy to use according to the stressor. This framework includes instruction about appraising stressors, identifying the changeable and unchangeable aspects, and selecting appropriate coping strategies that fit the stressor. Research has demonstrated that the use of emotion-focused coping strategies in response to changeable stressors, as opposed to the use of more appropriate problem-focused coping, represents a “lack of fit” between the changeability of stressors and the coping response. This lack of fit has been shown to be associated with worse outcomes.18,19,58 Therefore, to the extent that tinnitus has aspects that are changeable as well as unchangeable, both ACT and CBT do not specifically teach concepts on how to address changeable stressors. Instead, ACT and CBT focus primarily on stress-management principles and dealing with one’s emotions and thought patterns, whereas CET teaches a flexible framework for selecting suitable coping strategies.
Thus, one possible reason for the significant differences on SS across the 3 interventions is that the CET framework emphasizes selecting coping strategies that fit the type of stressor. That framework includes training participants to seek appropriate assistance (eg, problem-solving for changeable stressors and emotional support for unchangeable stressors) from others. This training may be reflected in the increased scores on SS in the CET group.
Although significant differences among the 3 brief interventions were found on SS, it may be that compressing these interventions into only 3 sessions did not provide sufficient time for participants to fully incorporate the psychological principles typically taught in these 3 interventions. For example, research on 28 RCT studies (26 of which used CBT) indicated a dose-response relationship in which between 58% and 67% of individuals receiving psychotherapy showed clinical improvement (on a range of problems) within an average of 12.7 sessions. 59 In the present pilot study, all 3 interventions were structured to parallel the PTM format that contained 3 sessions of psychological education, plus 2 sessions of audiological education. Adding more sessions to all 3 interventions may allow more time for participants to better acquire coping skills, as well as to sustain them over time. However, even with using the 3-session format, CET exhibited significant differences from the UC group. Before making definitive statements about the relative effect of these brief interventions on coping outcomes, these results should be replicated. Adding a measure that assesses adaptation to disability (eg, the Reactions to Impairment and Disability Inventory; H. Livneh, R.F. Reactions to Impairment and Disability Inventory Users’ Manual [Portland State University; 2008) may provide additional information about the effect of the interventions.
Limitations
The use of self-report instruments may have influenced the results that individuals reported due to honesty and social desirability.60,61 Further, the generalizability of findings is limited because the present sample was small and homogeneous on several sociodemographic variables, although it is reflective of the geographical location of recruitment.
In this pilot study, all participants received reminder phone calls the day before each intervention session. Follow-up questions were not documented among the participants who stopped attending the intervention. Such data could have provided information about perceived usefulness of the interventions and about other reasons for attrition. While the present study involved repeated measures, the sample was small, and for that reason, these results should be replicated. Further, a longer follow-up time-period would be required for better understanding of the impact of these brief interventions on individuals’ use of coping strategies to manage tinnitus.
Conclusion
The present pilot study was the first to evaluate CET as a psychoeducational intervention for bothersome tinnitus. The results of this pilot study indicated that this brief intervention that teaches individuals about types of stress and about how to appropriately match coping strategies to types of stressors may help people deal with their tinnitus better than interventions that focus primarily on managing unwanted thoughts and emotions (ie, ACT and CBT). The results indicate that CET may be a viable approach to use when helping individuals cope with tinnitus, particularly if further studies replicate the results that were observed in this study in larger and more diverse samples over a longer period of time.
Future research using different delivery formats, such as by using an internet or a smart-phone application platform, should also be examined. 25 Alternate platforms can provide more flexibility to participants to absorb the material at their own pace and schedule, which may decrease attrition that arises from scheduling conflicts. Internet-based interventions can also provide more accessibility to individuals who have transportation issues or who live too far away to attend weekly in-person groups.
Footnotes
Acknowledgments
A thank you is due to Tara Zaugg, AuD, for teaching the audiological component of the intervention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of a grant (VA RR&D C1578-P) awarded to the first author. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.