
Abstract
The influence of social media on individuals’ attitudes toward cosmetic surgery has received significant attention. However, how different patterns of social media engagement influence users’ cosmetic surgery desire and the underlying emotional and cognitive mechanisms remains underexplored. Drawing on a Chinese sample, this study addresses a notable gap in non-Western contexts where social media engagement and cosmetic surgery desire may differ significantly from Western populations. To address this gap, this study employed an online cross-sectional survey (N = 1,059) to examine how active and passive social media use relates to cosmetic surgery desire, mediated by social appearance anxiety (an emotional pathway) and perceived barriers and benefits of cosmetic surgery (cognitive pathways). Based on the stimulus-organism-response model, this study revealed distinct pathways through which active and passive social media use influence cosmetic surgery desire in the Chinese context. Active social media use was found to trigger cosmetic surgery desire through dual pathways by increasing social appearance anxiety and shaping cognitive beliefs about its benefits and barriers. In contrast, passive social media use primarily influenced cosmetic surgery desire through the emotional pathway of increased social appearance anxiety. These findings highlight the cultural and contextual importance of distinguishing between active and passive social media use in body image research, suggesting social appearance anxiety as a central emotional mechanism linking social media use to cosmetic surgery desire. Practically, this study offers culturally informed, evidence-based insights for developing interventions to reduce appearance-related pressures and enhance digital well-being.
Keywords
Introduction
Cosmetic surgery has rendered the ideals of youth and beauty technologically achievable, establishing a societal imperative for aesthetic enhancement and fostering a cultural environment where the body is viewed as perpetually improvable (Davis, 2003; Morgan, 1991). Recent data from the International Society of Aesthetic Plastic Surgeons (ISAPS, 2024) indicate a 40% surge in global cosmetic surgery over the last 4 years. While the United States remains leading in the number of surgical and non-surgical enhancements, Asian countries, including Japan, China, and India, are major and rapidly growing markets (ISAPS, 2024). Notably, China’s cosmetic surgery market has outpaced the global average in growth (Deloitte, 2024), raising questions about the drivers of this demand.
Media, particularly social media, have been identified as important drivers of this trend (Sharp et al., 2014; Wen et al., 2017; Wu et al., 2022). However, research examining the link between social media use (SMU) and cosmetic surgery desire has often treated SMU as a monolithic concept, typically measured by overall screen time. This approach overlooks the critical distinction between active and passive engagement. Although a growing body of literature distinguishes between active and passive SMU, it has primarily focused on general psychological outcomes like well-being or depression (Godard & Holtzman, 2024), leaving its influence on cosmetic surgery desire underexplored. Furthermore, the underlying emotional and cognitive mechanisms through which active and passive SMU might influence cosmetic surgery desire remain poorly understood. To address these research gaps, this study employs the stimulus-organism-response (SOR) model (Mehrabian & Russell, 1974) and the Health Belief Model (HBM) (Rosenstock, 1974) to investigate how active and passive SMU affect individuals’ cosmetic surgery desire in China, and examine whether and how social appearance anxiety and perceived barriers and benefits of cosmetic surgery, as emotional and cognitive pathways, link active and passive SMU to cosmetic surgery desire.
The contribution of this study is further strengthened by its specific focus. Existing research has predominantly focused on young, female populations in Western contexts (e.g., Forbes et al., 2012; Hendrickse et al., 2017; Perloff, 2014; Sharp et al., 2014), which limits the generalizability of findings and highlights the need for greater cultural diversity. The current study addresses this gap by surveying a national sample of adults in China, a context that differs significantly from Western countries in its socioeconomic status, patterns of SMU, and cultural attitudes toward cosmetic surgery. China offers a compelling research context by combining rapid digital adoption, extensive social media penetration, and exponential growth in its cosmetic surgery market. Unlike in Western countries, where cosmetic surgery is more established and normalized, China’s booming cosmetic surgery market reflects dynamic and rapidly evolving beauty standards shaped by digital transformation and cultural shifts. Therefore, understanding how active and passive SMU influence individuals’ cosmetic surgery desire in China carries significant theoretical and practical implications for other non-Western societies, where different social media engagement and cultural values surrounding appearance may create unique vulnerabilities to appearance-related pressures.
Literature Review
Stimulus-Organism-Response Model
The stimulus-organism-response (SOR) model posits that external environmental stimuli can provoke individuals’ emotional and cognitive responses (organism), which subsequently lead to behavioral outcomes (responses; Mehrabian & Russell, 1974). The SOR model is highly applicable to this study for several reasons. First, social media functions as an environmental stimulus that significantly affects body image concerns and the desire for cosmetic surgery (Perloff, 2014). Second, the SOR model has been applied in social media contexts to examine behavioral intentions (Luqman et al., 2017). Third, the SOR model emphasizes the mediating role of cognitive and emotional arousal between stimulus and response. More specifically, the “organism” dimension of the SOR model includes subdimensions such as pleasure, arousal, and dominance (Mehrabian & Russell, 1974), capturing the affective and cognitive processes triggered by environmental stimuli (Bakker et al., 2014). Thus, the SOR model provides an appropriate theoretical model for examining how active and passive SMU (stimulus) influence cosmetic surgery desire (response) through emotional and cognitive pathways (organism).
This study complements the SOR model with the Health Belief Model (HBM), which explains how perceived barriers and benefits influence health-related decisions. Together, these frameworks allow us to examine how active versus passive SMU (stimulus) shapes cosmetic surgery desire (response) through cognitive and emotional pathways (organism).
Social Media and Cosmetic Surgery
Social media is powerful in setting beauty standards, amplifying body image pressures, and promoting the medicalization of appearance in our society (Bonell et al., 2021). Previous research has shown that exposure to appearance-focused content on social media enhanced consideration of cosmetic surgery (Walker et al., 2021). In addition, SMU can influence individuals’ perceptions of cosmetic surgery and self-image (Hawes et al., 2020). Sherlock and Wagstaff (2018) found that SMU can increase users’ exposure to idealized body images, which is positively related to appearance anxiety and body dissatisfaction. Lee et al. (2014) revealed that using social media to get body image information was negatively associated with body satisfaction, self-esteem, and psychological well-being. Moreover, individuals with lower body satisfaction and self-esteem were significantly more likely to consider and accept cosmetic surgery (Hermans et al., 2022; Swami et al., 2009; Walker et al., 2021). Taken together, these studies suggest that greater SMU is associated with increased cosmetic surgery desire.
However, it is necessary to recognize that SMU is not a single activity but a composite of many nested activities within what appears to be a single activity (Gerson et al., 2017). Past research has distinguished between active and passive SMU, demonstrating that different patterns of social media engagement yield important implications for psychological well-being (Verduyn et al., 2017). This distinction is equally pertinent when examining body image concerns and desire for cosmetic surgery. For example, some researchers found that both active and passive SMU can increase the salience of appearance and normalize the acceptance of cosmetic surgery (Bell et al., 2024; Hermans et al., 2022). Whereas others found that passive SMU increased men’s interests in cosmetic surgery while active SMU failed to show any significant influence (Truasheim & Bonell, 2024). In light of these conflicting results, it is necessary to clarify whether active versus passive SMU influence the desire for cosmetic surgery differently, exploring the underlying mechanisms that may explain such differences. Therefore, this study adopted the proposed distinction between active and passive SMU (Gerson et al., 2017) and applied it to appearance-related SMU. More specifically, active SMU is characterized by an active behavior pattern that includes creating content or communicating with others, whereas passive SMU is described as passively consuming appearance-related content such as browsing profiles, updates, and newsfeeds, or lurking on social media. Based on the SOR model, active and passive SMU are considered as stimuli in this study.
Perceived Barriers and Benefits as Cognitive Mediators
The association between appearance-related SMU and cognitive beliefs, such as perceived barriers and benefits of cosmetic surgery, has been well-established (Hermans et al., 2022; Seekis & Barker, 2022; Sharp et al., 2014; Wen et al., 2017). The Health Belief Model (HBM) posits that perceived barriers are either objective or subjective factors that may prevent individuals from engaging in certain health behaviors, whereas perceived benefits refer to the anticipated positive outcomes of such behaviors (Jones et al., 2015; Rosenstock, 1974). For cosmetic surgery, perceived barriers include costs, inconvenience, risk, and pain associated with both surgical and non-surgical procedures; perceived benefits include physical attractiveness, self-assurance, and potential advantages in marriage and job markets (Darisi et al., 2005).
Theoretically, perceived barriers and benefits of cosmetic surgery that result from active and passive SMU can be related to the “dominance-submissiveness” sub-dimension of the “organism” dimension in the SOR model (Mehrabian & Russell, 1974). This sub-dimension describes individuals’ sense of control or lack of control over cosmetic surgery, as well as the extent to which they perceive restrictions when considering such procedures. These factors are effectively characterized by perceived barriers and benefits of cosmetic surgery. Other HBM constructs, such as perceived susceptibility and perceived severity, are not examined in this study, due to the fact that they are less effective than perceived barriers and perceived benefits in predicting health behaviors (Carpenter, 2010).
Previous studies revealed that social media is a convenient channel for individuals to access and learn about cosmetic surgery information, enabling them to be better informed about its potential barriers and benefits (Walker et al., 2021). Meanwhile, filled with idealized and digitally enhanced body images, misleading advertisements, and over-crowded misinformation, social media tends to overstate the benefits while understating the barriers to cosmetic surgery (Hermans et al., 2022; Oregi et al., 2022). Therefore, we hypothesize that both active and passive SMU negatively influence perceived barriers to cosmetic surgery while positively influencing perceived benefits. In addition, previous studies revealed that attitudes toward cosmetic surgery were positively influenced by perceived benefits and negatively influenced by perceived barriers (Wu et al., 2022). Therefore, we hypothesize that perceived barriers are negatively associated with cosmetic surgery desire, while perceived benefits are positively related to it.
Social Appearance Anxiety as Emotional Mediator
Social appearance anxiety is defined as a persistent fear of social scrutiny and negative judgment based on one’s physical appearance such as body shape and facial characteristics (Hart et al., 2008). It is related to body image dissatisfaction and personality traits that magnify one’s concerns about appearance (Hart et al., 2008; Levinson & Rodebaugh, 2011). In this study, social appearance anxiety is conceptualized as an emotional mediator to fit in the “organism” dimension of the SOR model (Mehrabian & Russell, 1974). SMU can trigger social appearance anxiety as a form of emotional arousal (Papapanou et al., 2023). First, social media fosters social appearance anxiety by curating idealistic self-images and internalizing it into the management of one’s appearance. For instance, active SMU, such as editing and sharing selfies with impression management in mind, is linked to increased body image concerns and social appearance anxiety (Boursier et al., 2020). Second, passive SMU can create a social comparison environment that raises appearance concerns and possibly exacerbates emotional problems, including social appearance anxiety (Hawes et al., 2020; Meier & Johnson, 2022). Third, both general and appearance-related SMU have been identified as important triggers for social appearance anxiety (Mills et al., 2018; Shensa et al., 2018). Notably, both active and passive SMU have emerged as strong predictors of social appearance anxiety (Pan et al., 2023). Moreover, cosmetic surgery is considered a relatively direct and effective means of gaining social recognition, thereby mitigating social appearance anxiety (Wu et al., 2022). As emotional arousal emerges from the evaluation of social media content and appearance-related cues, social appearance anxiety can evoke appearance management behavior and cosmetic surgery intent (Kim & Chung, 2016). Given this, we hypothesize that both active and passive SMU are positively associated with social appearance anxiety, which in turn predicts the desire for cosmetic surgery.
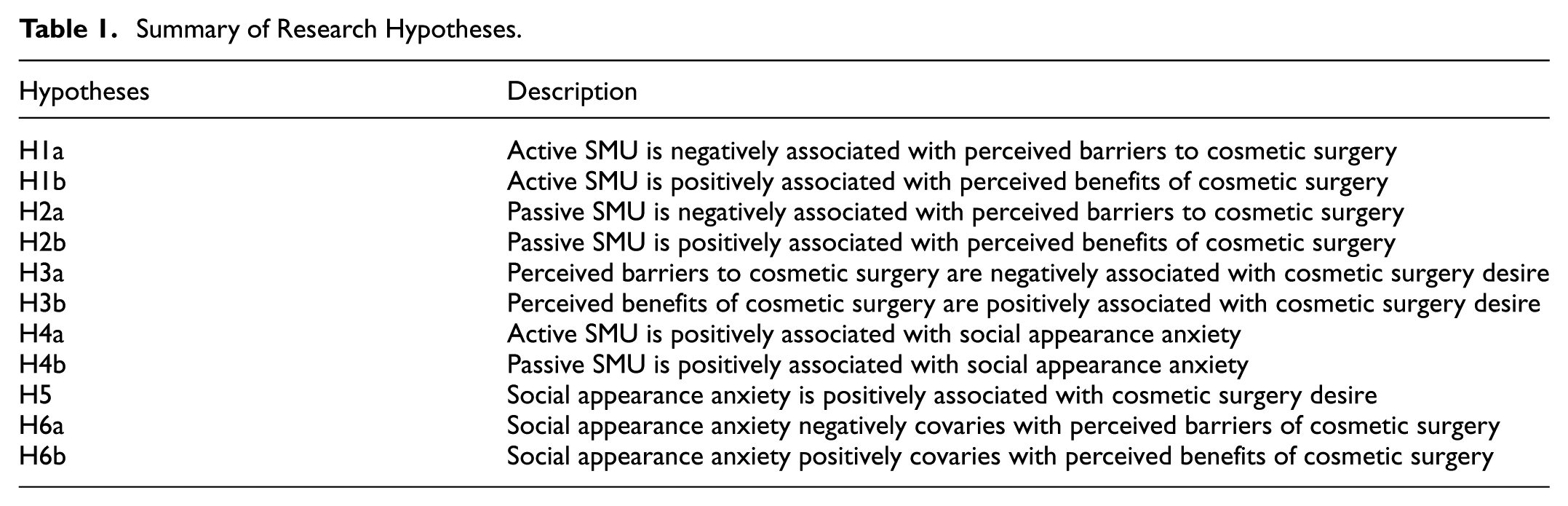
Last but not least, the SOR model treats the cognitive and emotional factors in the “organism” dimension as covariance caused by the external “stimulus.” Particularly, relevant research suggested that emotion operates as a learning and feedback process driving reflection and appraisal that, in turn, leads to behaviors/intentions (Brosch, 2021). Moreover, according to the affect heuristic model, individuals form their cognitive beliefs and judgments regarding the perceived barriers and benefits of cosmetic surgery through an overall affective evaluation of available information (Finucane et al., 2000). Therefore, it is plausible to hypothesize that social appearance anxiety is associated with perceived barriers and benefits of cosmetic surgery. The full set of research hypotheses is presented in Table 1.
Summary of Research Hypotheses.
A theoretical model was proposed based on the SOR model (see Figure 1).
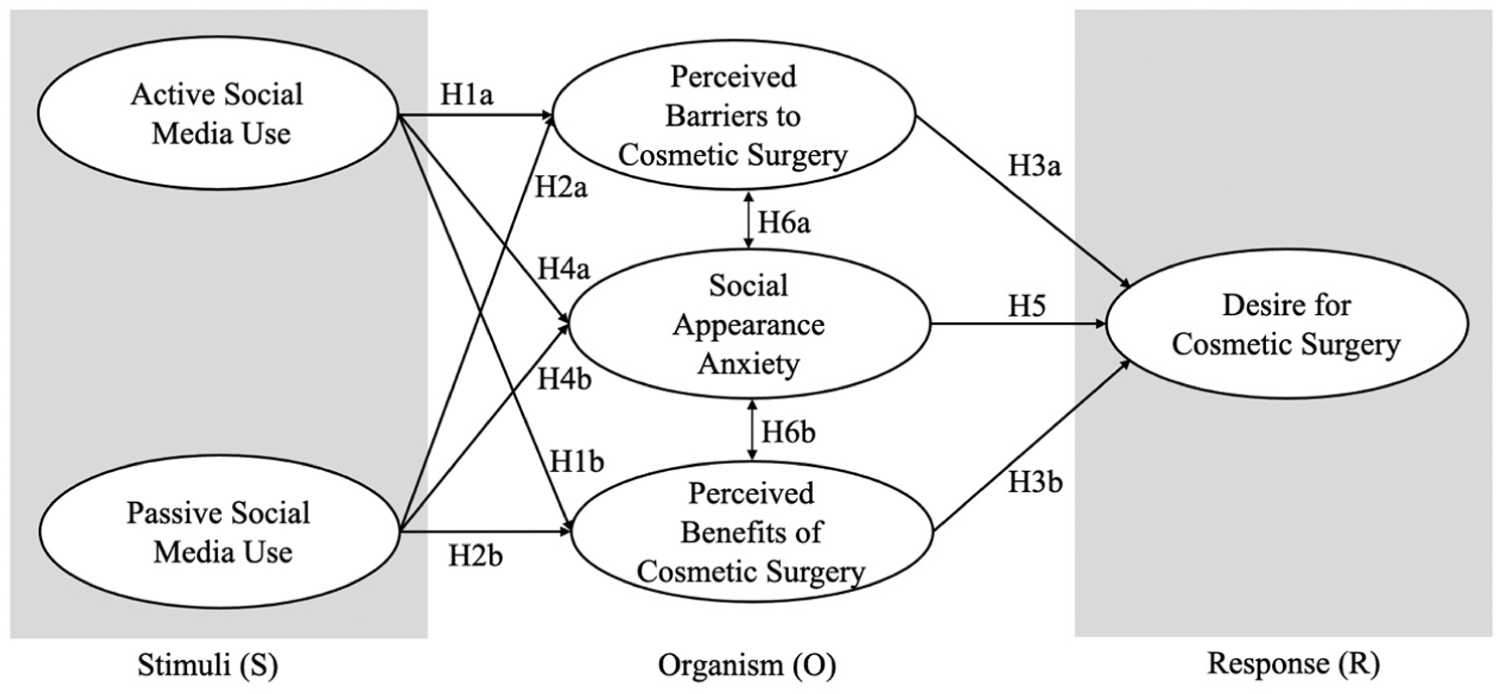
A theoretical model for the influence of active and passive SMU on cosmetic surgery desire through cognitive and emotional pathways.
Method
Data Collection
An online cross-sectional survey was conducted in May 2024. A forward-backward translation procedure was employed to adapt the original English questionnaire into Chinese. Two bilingual experts performed the forward translation, which was then back-translated by an independent translator to ensure accuracy. Discrepancies were resolved through consensus discussion. This approach aligns with established guidelines for cross-cultural instrument adaptation (Beaton et al., 2000).
Participants were recruited through convenience sampling via Wenjuanxing, one of China’s largest online survey platforms. This platform allowed us to target individuals aged 18 or older. All participants were briefed on the voluntary and confidential nature of the survey through an informed consent process. A total of 1,300 completed responses were collected. After data cleaning (i.e., deleting responses with missing answers or straight-line responses, filtering out duplicate responses from the same IP address, and excluding responses that failed attention checks), the final sample size was 1,059.
The final sample was 76.7% female (N = 812) and 23.3% male (N = 247), with a mean age of 29.7 years (SD = 9.9, min = 18, max = 42). A majority of the sample were college-educated (70.44%, N = 746) and married (61.2%, N = 648). The average BMI was 21.43 (SD = 4.10). Notably, the gender and age composition of our sample mirrors that of the core cosmetic surgery consumers base in China, which is predominantly young and female (Deloitte, 2024). This alignment enhances the relevance of our findings for this key demographic, though it limits generalizability to male, older adults (>45 years), and less educated groups. Additionally, our employment of online sampling, though supported by trends in research participant preference (Dumbari Ndiinee & Gever, 2025), inherently limits generalizability due to digital access bias. Future research should adopt diverse sampling strategies to enhance representativeness across broader populations.
Measurement
Active SMU (Frison & Eggermont, 2020; Gerson et al., 2017) was assessed by asking participants how frequently they use social media platforms (e.g., Weibo, WeChat, Xiaohongshu, Douyin, etc.) for the following purposes: (1) to post status updates or share content related to appearance concerns such as beauty, fitness/weight loss, and cosmetic surgery; (2) to interact or engage in conversations with others about appearance-related topics; (3) to like or comment on appearance-related content. Responses were measured on a 5-point Likert scale (1 = never, 5 = always; M = 2.46, SD = .98, Cronbach’s α = .84).
Passive SMU (Frison & Eggermont, 2020; Gerson et al., 2017) was assessed by asking participants how frequently they use social media platforms (e.g., Weibo, WeChat, Xiaohongshu, Douyin, etc.) for the following purposes: (1) to browse information related to appearance concerns such as beauty, fitness/weight loss, and cosmetic surgery; (2) to view others’ profiles, photos, comments, and posts related to appearance, without engaging (i.e., liking or commenting); (3) to lurk others’ activities related to appearance topics. Responses were measured on a 5-point Likert scale (1 = never to 5 = always; M = 3.03, SD = 1.13, Cronbach’s α = .83).
Social appearance anxiety was assessed using 10 items adapted from the Social Appearance Anxiety Scale (SAAS; Hart et al., 2008). Participants evaluated their anxiety in various scenarios where their appearance might be scrutinized. Items included: (1) I worry that people would not like me because of my appearance; (2) I am concerned worry that others make negative judgments about my looks when I am not there; (3) I worry that people find me unattractive because of the way I look; (4) I am concerned that people find me unappealing; (5) I worry that my appearance could be a disadvantage or an obstacle for me; (6) I am concerned that I have missed opportunities because of the way I look; (7) I feel anxious when people comment on my appearance; (8) I worry that I don’t live up to social expectations for how I should look; (9) I feel uneasy thinking that others might notice flaws in my appearance; (10) I am concerned that people think I am not good looking. Other items from the original SAAS were removed due to low factor loadings (<.50) in the confirmatory factor analysis to ensure reliability. Participants rated each item on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The ten items were averaged into a composite score with good reliability (M = 3.80, SD = .57, Cronbach’s α = .80).
Perceived barriers to cosmetic surgery, including both objective and subjective barriers, were assessed with four items adapted from prior research (Jones et al., 2015; Darisi et al., 2005), including: (1) I don’t have enough time to undergo and recover from cosmetic surgery; (2) I don’t have enough money for cosmetic surgery; (3) I believe cosmetic surgery is risky; (4) I think cosmetic surgery is painful. Participants rated each item on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The four items were averaged into a composite score with good reliability (M = 3.32, SD = .86, Cronbach’s α = .80).
Perceived benefits of cosmetic surgery were assessed using four items adapted from prior research (Darisi et al., 2005; Henderson-King & Henderson-King, 2005), including: (1) cosmetic surgery would improve my physical attractiveness; (2) cosmetic surgery would increase my self-confidence; (3) undergoing cosmetic surgery can increase one’s confidence in social situations and activities; (4) cosmetic surgery is good because it can enhance one’s competitiveness in the job market. Participants rated each item on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The four items were averaged into a composite score (M = 3.81, SD = .52, Cronbach’s α = .81).
The desire for cosmetic surgery was evaluated using four items adopted from the Acceptance of Cosmetic Surgery Scale (ACSS; Henderson-King & Henderson-King, 2005; Wen et al., 2017) on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The four items were: (1) I have thought about undergoing cosmetic surgery at some point; (2) I would consider a minor procedure to enhance my attractiveness; (3) in the absence of any negative side effects or pain, I would be willing to try cosmetic surgery; (4) I would never have any kind of cosmetic surgery (reversely coded). When referring to cosmetic surgery, both surgical and non-surgical procedures such as minimally invasive treatments were included. The four items were averaged to create a composite variable with high reliability (M = 2.35, SD = 1.01, Cronbach’s α = .82).
Demographics including age, gender, education, and BMI were also collected.
Data Analysis
The data were analyzed using SPSS 23.0 and AMOS 27.0. First, descriptive statistics were analyzed. Then, structural equation modeling (SEM) was employed, utilizing maximum likelihood estimation. Before analysis, normality of distributions was assessed via skewness and kurtosis statistics, with all key variables approximating a normal distribution. Multicollinearity diagnostics showed that all VIF values were well below the threshold of 10. Maximum likelihood estimation was employed because it is robust and efficient for large samples and provides optimal parameter estimates under multivariate normality assumptions. Then, we followed a two-step approach for SEM by conducting measurement and structural models (Anderson & Gerbing, 1988). Confirmatory factor analyses (CFA) were performed, indicating that the composite reliability (CR) for each construct surpassed the threshold of .70, the average variance extracted (AVE) for each construct was greater than .50, and the square roots of the AVE values exceeded the inter-variable correlation coefficients (see Table 2). The measurement model exhibited an acceptable fit (χ2/df = 3.26, GFI = .93, CFI = .93, TLI = .92, RMSEA = .06), with all factor loadings on corresponding latent factors above .60. A structural model was constructed based on the measurement model after controlling for age, gender, education, and BMI. The results indicated that the structural model provided a good fit to the data (χ2/df = 2.98, GFI = .92, CFI = .91, TLI = .91, RMSEA = .05).
Measurement Assessment and Correlation Matrix of Variables.

Notes. The italicized diagonal elements are the square root of the AVE. All the correlation coefficients are significant at the .01 level (2-tailed).
Results
Regarding the hypothesized relationship between SMU and cognitive beliefs, the results showed that active SMU was positively associated with the perceived benefits of cosmetic surgery (β = .23, p < .05) and negatively associated with perceived barriers (β = −.60, p < .001). Therefore, H1a and H1b were supported. However, no significant associations were observed between passive SMU and perceived barriers to cosmetic surgery (β = −.09, p > .05) or between passive SMU and perceived benefits of cosmetic surgery (β = .06, p > .05). Therefore, H2a and H2b were not supported. Moreover, perceived barriers were found to negatively associate with cosmetic surgery desire (β = −.15, p < .01), while perceived benefits were positively associated with cosmetic surgery desire (β = .21, p < .01). So, H3a and H3b were supported.
Social appearance anxiety showed significant positive associations with both active (β = .31, p < .001) and passive SMU (β = .31, p < .001), as well as with cosmetic surgery desire (β = .31, p < .001), thus supporting H4a, H4b, and H5. Moreover, it was found that social appearance anxiety was negatively associated with perceived barriers to cosmetic surgery (β = −.10, p < .05) and positively associated with perceived benefits of cosmetic surgery (β = .13, p < .05). Thus, H6a and H6b were supported. Among the controlled variables, gender (β = −.21, p < .001) and BMI (β = .30, p < .001) were significantly associated with cosmetic surgery desire, while age (β = .03, p > .05) and education (β = .01, p > .05) were not significantly related. The model explained 46.3% of the variance in the desire for cosmetic surgery (R2 = .463; see Figure 2).

Structural equation model of the effects of active and passive SMU on cosmetic surgery desire via cognitive and emotional pathways.
Mediational paths were assessed using bootstrapping with 5,000 samples, controlling for demographic variables. Results of bootstrapping showed significant mediation of the relationship between active SMU and cosmetic surgery desire through perceived barriers (β = .042, 95% CI [.020, .065]) and perceived benefits (β = .009, 95% CI [.001, .019]). However, the indirect paths from passive SMU to cosmetic surgery desire through perceived barriers (β = .004, 95% CI [−.002, .014]) and perceived benefits (β = .003, 95% CI [−.001, .015]) were not statistically significant. Notably, social appearance anxiety significantly mediated the relationships between active SMU and cosmetic surgery desire (β = .021, 95% CI [.008, .039]), as well as the relationship between passive SMU and cosmetic surgery desire (β = .028, 95% CI [.010, .047]).
Discussion
Drawing upon the SOR model, this study conceptualized active and passive SMU as external stimuli (S), social appearance anxiety as an emotional mediator alongside perceived barriers and benefits of cosmetic surgery as cognitive mediators within the organism dimension (O), and individuals’ desire for cosmetic surgery as the response (R). Based on this framework, this study revealed that both active and passive SMU trigger cosmetic surgery desire, but through distinct pathways. Specifically, active SMU operates through dual processes, including both emotional and cognitive pathways, while passive SMU primarily influences cosmetic surgery desire through an emotional pathway. For active users, the emotional pathway emerges when they engage in posting, sharing, and interacting with appearance-related content, which leads them to undergo higher self-presentation concerns and intensify social appearance anxiety. The cognitive pathway emerges through deliberative information processing, in which active users encounter information related to appearance and cosmetic surgery on social media and actively evaluate and mentally elaborate upon it. Such cognitive engagement reduces perceived barriers (e.g., by normalizing procedures through peer discourse) while enhancing perceived benefits of cosmetic surgery (e.g., through selective exposure to positive narratives shared by trusted peers and influencers). This dual-process mechanism reflects the distinction between automatic emotional appraisal and controlled cognitive elaboration proposed by dual-process theory (Loewenstein & Lerner, 2003).
In contrast, passive SMU primarily increases cosmetic surgery desire through the emotional pathway of elevated social appearance anxiety. One possible explanation is that passive SMU limits deeper cognitive processing by failing to provide sufficient psychological engagement. Passive users encounter appearance-related content without intentionally seeking it or interacting with others, limiting their opportunity for critical evaluation or mental elaboration. While this exposure still triggers emotional responses as social appearance anxiety remains activated, it fails to reshape cognitive beliefs about cosmetic surgery. This aligns with research on shallow versus deep information processing (Perloff, 2014), where passive consumption typically engages only surface-level encoding. Another possible explanation lies in cognitive resource allocation (Lavie, 2005). Passive users operate under perceptual load conditions where attention is diffusely distributed across multiple stimuli without focused elaboration, leaving limited cognitive resources for systematic processing of appearance-related information encountered in social media. In contrast, active users’ intentional engagement concentrates cognitive resources on appearance-related content, enabling more thorough schema formation and belief formation.
This study highlights social appearance anxiety as a critical emotional pathway linking both active and passive SMU to cosmetic surgery desire. Emotional contagion is a possible explanation for this phenomenon. Humans live in complex social networks and the basis of their social behavior lies in their ability to share and respond to others’ emotions (Norscia & Palagi, 2011). This ability may generate emotional contagion (Hatfield et al., 1993), a phenomenon increasingly documented in social media context (Lin & Utz, 2015; Krammer et al., 2014). While emotional contagion occurs across cultures, research demonstrates that individuals from collectivist cultures are more susceptible to in-group members’ affective states (Ilies et al., 2007). In collectivist cultures like China, individuals often prioritize group harmony and interdependence, making them actually sensitive to others’ evaluations and social approval (Markus & Kitayama, 1991). Within our research context, when Chinese social media users, who are motivated to maintain group harmony and avoid standing out negatively, encounter idealized appearance-related content online, they are more susceptible to social appearance anxiety (Kuang et al., 2019). Consequently, they may pursue cosmetic surgery as a mechanism for conformity. Furthermore, exposure to appearance-focused content on social media may also lead Chinese users to not only compare themselves to others but also internalize these comparisons as threats to their group standing and social acceptance. This internalization, in turn, can intensify their social appearance anxiety and reinforce the desire for cosmetic surgery.
This cultural perspective may also help to explain why social appearance anxiety emerged as a stronger predictor of cosmetic surgery desire than cognitive beliefs in our study. Social appearance anxiety creates urgency and pressure by making individuals feel inadequate or insecure about their appearance, prompting immediate consideration of cosmetic procedures (Cash et al., 2004). Collectivist values create culturally-specific amplification of such emotional urgency that overrides rational cost-benefit analyses. Algorithmically-curated content that concentrates on appearance-focused posts from in-group members further amplifies this culturally-rooted emotional response.
Social media platforms’ structural features interact with both emotional/cognitive processes and cultural context to amplify cosmetic surgery desire. Importantly, the distinction between active and passive SMU partly reflects different exposure to these architectural features. Social media algorithms employ content curation mechanism that disproportionately prioritizes engagement-generating content, which in appearance domains often includes beauty standards, success stories, positive testimonials, and influencer endorsement (Seekis & Barker, 2022). For active users, the algorithmic recommendations are reinforced through positive feedback loops. Their engagement with appearance-related content trains algorithms to deliver more similar content, exposing them repeatedly to cosmetic surgery narratives that downplay risks while emphasizing benefits. It potentially reflects the inherent bias in appearance-related social media content that disproportionately emphasizes benefits over risks (Besmens et al., 2021). Influencers, celebrities, and peers predominantly share narratives highlighting aesthetic improvements, enhanced confidence, and social acceptance while minimizing discussions of pain, complications, and recovery challenges (Hermans et al., 2022). Such selective representation combined with algorithmic reinforcement creates an unrealistic perception of cosmetic surgery as safer and more accessible than it actually is.
For passive users, although they encounter appearance-related content within natural feed scrolling, their lack of intentional engagement limits cognitive elaboration. This effect is compounded by the way cosmetic surgery is framed on social media—not as a taboo medical procedure but as a routine self-care option, similar to skincare or fashion consumption (Sarwer, 2019). This normalization promotes more automatic emotion-driven decision-making over systematic evaluation. As a result, while passive exposure may emotionally trigger social appearance anxiety, it fails to prompt systematic information processing required to shape cognitive beliefs about the procedure’s benefits and barriers.
Our results also demonstrated that social appearance anxiety was negatively associated with perceived barriers and positively associated with perceived benefits of cosmetic surgery. This finding underscores the interconnection between emotional and cognitive processing (Xu et al., 2023), suggesting a potential reinforcing dynamic that intensifies the desire for cosmetic surgery. It aligns with cognitive appraisal theory (Frijda & Mesquita, 2000), which proposes that emotions and cognitions are mutually influential. Specifically, when experiencing elevated social appearance anxiety induced by SMU, individuals enter a threat-detection mental state, in which they unconsciously reframe information to align with emotion-driven goals to reduce immediate threats. Cosmetic surgery, presented through social media as a viable solution to appearance deficits, becomes cognitively reconstructed as less risky and more beneficial. This emotion-colored interpretation then corresponds with the increased desire for cosmetic surgery. Crucially, the loop can operate in the opposite direction. A cognitive focus on the higher benefits and lower risks of cosmetic surgery could also amplify anxiety about one’s current appearance, further solidifying the perceived need for a solution. Therefore, our results support a model of reciprocal influence. Social appearance anxiety co-occurs within a cognitive calculus that makes surgery seem more favorable, and this cognitive pattern is, in turn, linked to a heightened desire for cosmetic surgery. This highlights a potentially self-sustaining relationship between how individuals feel about their appearance and how they think about potential solutions.
Conclusion
Drawing upon the SOR model, this study revealed that active SMU operate through both emotional and cognitive pathways to increase cosmetic surgery desire, whereas passive SMU primarily functions through emotional mechanisms. It is a distinction with important implications for targeted intervention. Moreover, by illuminating the cultural amplification effects on social appearance anxiety’s role, as well as the interplay between emotion and cognition, this research points toward more culturally-informed approaches to promoting healthier relationships with digital media and embodied identity.
Theoretically, this study makes several key contributions. First, while prior research documents social media’s general influence on body image concerns (Tiggemann & Slater, 2014), this study advances understanding of how social media influences individuals’ desire for cosmetic surgery by distinguishing between active and passive SMU and identifying their distinct pathways to cosmetic surgery desire. Moving beyond monolithic conceptualizations of “social media use,” this study revealed the distinct emotional and cognitive pathways linking different engagement patterns to cosmetic surgery desire within the SOR framework. Furthermore, it advances dual-process theory by revealing how automatic emotional responses (social appearance anxiety) and deliberate cognitive process (perceived barriers and benefits) operate differently across engagement patterns, thereby clarifying the mechanisms through which social media shape appearance-related intentions. Second, this study examines these mechanisms within a collectivist cultural context and discusses how collectivist cultural values may help explain the emotional and cognitive pathways identified in the SOR framework. The finding that emotion-driven decision-making predominates over cognitive deliberation among Chinese users may reflect collectivist identity processes not typically documented in Western contexts, suggesting cultural boundary conditions for social media effects. Third, by examining different engagement patterns with social media, this study suggests that algorithmic curation may shape the information environment differently for active and passive users. This raises the theoretical possibility that platform features function as moderators of psychological processes rather than neutral channels, suggesting future research should investigate platform-specific mechanisms rather than treating platforms merely as context.
Practically, the findings of this study offer evidence-based suggestions for different stakeholders. For individuals, understanding that passive SMU primarily triggers emotional responses while active SMU also shapes cognitive beliefs enables more informed self-regulation of social media habits. Educational initiatives such as media literacy programs and psychological support services that alleviate social appearance anxiety and provide balanced information about cosmetic surgery could help mitigate the negative impact of social media. Considering the differences between active and passive SMU as well as their effects on cosmetic surgery desire, media literacy programs for active social media users should emphasize cognitive skills such as identifying biased information, recognizing algorithmic amplification, understanding selection effects in peer-shared narratives, as so to correct distorted beliefs about cosmetic surgery. Programs for passive users should focus on emotional regulation techniques such as anxiety management and social media use boundaries. Media literacy curricula should teach algorithmic awareness, platform economics, and cultural critique of beauty standards, particularly in Chinese context where collectivist pressures amplify appearance concerns. For social media platforms, they need to disclose how appearance-related content is algorithmically promoted and limit repetitive exposure to appearance-focused content, especially among heavy users. For example, they should rotate diverse beauty representation, flagging AI-modified or heavily filtered images, and limiting surgery advertisements to age-appropriate users. For policy makers, it is necessary to provide stricter oversight of cosmetic surgery advertisements and influencer content, particularly on social media platforms popular among adolescents. To counter the biased cognitive appraisal triggered by idealized beauty content, regulations should mandate evidence-based disclaimers about potential complications and the recovery process, restrict the overrepresentation of success stories, and limit testimonials from unverified users. Moreover, to empower individual’s cognitive appraisal and build emotional resilience, the government should integrate digital health literacy into school curricula and promote public awareness campaigns on social media. Such public education is important for deconstructing the self-care narrative and fostering critical engagement with appearance-related content.
Limitations and Future Research
This study has several limitations. First, the cross-sectional design limits our ability to determine causal relationships. Future research could employ longitudinal designs (tracking participants over time) or experimental designs (manipulating social media exposure) to better establish causal relationships among key variables. Second, the sample skewed toward young, well-educated, and predominantly female respondents, limiting generalizability. The reliance on the online survey further introduces self-selection bias, as participants with more online engagement are likely overrepresented. Future research should employ broader sampling strategies to enhance external validity. Third, self-reported measures present inherent limitations. Despite using the validated SAAS scale to measure social appearance anxiety, it should be noted that the findings may be subject to social desirability bias inherent in self-reports. Similarly, measuring active and passive SMU through behavioral analytics on apps rather than self-report data would strengthen validity. Finally, this study did not distinguish between specific platforms (e.g., WeChat, Douyin), which may activate different mechanisms given platform-specific affordances and user demographics. Future studies could conduct platform-specific analyses to determine how engagement effects vary across social media platforms.
Footnotes
Ethical Considerations
The study protocol was reviewed and approved by the Academic Ethics Committee of the College of Media and International Culture, Zhejiang University. Informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Zhejiang Provincial Philosophy and Social Science Planning Project (No.: 23NDJC002Z) and the National Social Science Fund (No.: 24FXWB010).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon request.