
Abstract
With the increasing integration of computational and information science in healthcare, the digital health field has leveraged gamification as a strategy to enhance user engagement and behavior change. However, existing studies still lack a comprehensive mapping of digital health gamification. This study presents a bibliometric analysis of 1,967 Scopus-indexed publications on digital health gamification from 2005 to 2025, 618 core documents were analyzed using BiblioMagika®, Biblioshiny, VOSviewer, and OpenRefine. The dataset includes 3,240 contributing authors, with journal articles (50.65%) and conference papers (37.54%) dominating the field. English-language publications account for 98.71%. A rapid rise in publications post-2016 reflects the field’s growing interest. Interdisciplinary collaboration is evident, with contributions from medicine (58.9%), computer science (43.9%), and engineering (29.3%). The United States leads with 144 publications (h-index 27, 2,435 citations), followed by the UK (50 publications, h-index 15) and Australia (47 publications, h-index 16). The University of Twente ranks first among the top 20 institutions. Four prolific authors are based in Australia. Co-occurrence analysis of 1,763 author keywords identified seven major clusters, including behavior change, mental health, chronic disease, mobile health apps, and AI-driven personalization. Topic modeling revealed three dominant themes, and the most prominent theme was digital health gamification applications. This study highlights gamification’s role in shaping health behaviors and the need for refined models to address sustainability and gamification fatigue. It also underscores the increasing use of adaptive, AI-driven personalization in digital health, emphasizing ethical governance and inclusive design.
Plain Language Summary
Digital tools like mobile apps and online programs are increasingly using game-like features—such as points, rewards, and challenges—to help people stay healthy. This approach, known as “gamification,” is designed to make health activities more engaging and to encourage positive behavior change. This study reviews 20 years of global research on how gamification has been used in digital health. By analyzing 1,967 scientific publications from 2005 to 2025, we identified key trends, leading countries and institutions, and major research themes. Most studies were published after 2016, showing that interest in this topic has grown rapidly. The research comes from a mix of disciplines, especially medicine, computer science, and engineering. The United States contributed the most studies, followed by the United Kingdom and Australia. We found that popular research topics include how gamification supports mental health, manages chronic illnesses, and improves mobile health apps. Many studies also explore how artificial intelligence (AI) is used to personalize digital health tools for different users. This review highlights the benefits of gamification in promoting healthy behaviors, but also points to challenges, such as keeping users engaged over time and ensuring ethical use of AI. The study provides useful insights for researchers, developers, and healthcare providers aiming to design effective and inclusive digital health solutions. By mapping the development of this field, our research helps guide future efforts to use gamification in a way that is both impactful and responsible.
Keywords
Introduction
The global health landscape is increasingly shaped by complex, interrelated challenges, including the rising prevalence of chronic diseases, widespread sedentary lifestyles, and a growing burden of mental disorders (Goyal & Rakhra, 2024; Münzel et al., 2023). Non-communicable conditions such as diabetes, cardiovascular disease, and obesity account for more than 70% of annual deaths worldwide—about 41 million—placing unsustainable pressure on health systems (Garg, 2025; Malik & Ahmad, 2025). Although physical inactivity is a well-established, modifiable risk factor for chronic disease, it remains pervasive and has been described as a “global pandemic” (Henson et al., 2023). Roughly one-third of adults worldwide do not meet recommended activity levels, and average daily sedentary time exceeds 7 to 8 hr (J. H. Park et al., 2020). The problem is particularly acute—and rising—among adolescents and young adults (Mandili et al., 2022). In addition, mental health disorders, including depression and anxiety, have not declined since 1990 and now constitute a major share of the global disease burden (GBD 2019 Mental Disorders Collaborators, 2022). These challenges threaten individual well-being, undermine economic productivity, and impede social development, underscoring the need for more efficient, pragmatic, and feedback-responsive public health interventions (Mandili et al., 2022).
Yet traditional public health programs, while essential, are often constrained by high costs, limited scalability, and difficulties sustaining user engagement (Herlitz et al., 2020; L. Sun et al., 2024; Weber et al., 2024). Cost pressures span design, rollout, and maintenance, covering infrastructure, workforce training, technical support, and continuous monitoring, which are especially challenging in resource-constrained settings (Weber et al., 2024). Scalability is frequently lost when moving from controlled pilots to broader implementation due to limited human, technical, and organizational resources, complex delivery models, and poor local fit (L. Sun et al., 2024). Sustained engagement also declines over time as budgets tighten, staff turnover increases, and ongoing training and incentives wane, making long-term maintenance difficult (Herlitz et al., 2020).
Against this backdrop, digital health technologies, including mobile apps, wearables, and telemedicine, have rapidly become important tools for health management and prevention (Hong, 2024). Despite their popularity and rapid progress, however, many digital health interventions face the same challenge as traditional programs: producing durable behavior change (Pelly et al., 2023). Initial gains often erode as long-term adherence and engagement decline, a concern for practitioners and researchers alike (Duffy et al., 2022).
Combining digital health with gamification has therefore emerged as a distinctive and promising approach to today’s health challenges (Lukka & Palva, 2023). Gamification refers to the use of game design elements in non-game contexts—especially health—to motivate users through feedback, competition, and rewards. Common elements include points and badges, progress feedback, leaderboards, goal setting, and social interaction (Berglund et al., 2022). When integrated into digital health, gamification can turn routine behaviors—such as physical activity, medication adherence, or self-care in mental health—into interactive, personalized, and potentially more sustainable experiences, often via points, badges, leaderboards, and rewards (J. Kim et al., 2025). Unlike many traditional models, gamified digital solutions can be scalable, accessible, and adaptable, making them well-suited to address urgent public health needs at relatively low cost (L. Sun et al., 2024). Recent studies highlight applications across chronic disease management, mental health support, fitness, diet management, and health professional training (Garrison et al., 2021; Lukka & Palva, 2023). Advances in computing and information science—particularly AI and big-data analytics—further enhance gamification through personalized recommendations, adaptive feedback, and interactive user experiences (Gao, 2024; Pérez-Juárez et al., 2022). As a result, digital health gamification is increasingly viewed not as a marginal innovation but as a strategic pathway to sustained behavior change and reduced system burden in the 21st century (Ukabuiro & Agomah, 2025).
Despite this promise, the literature remains conceptually fragmented and methodologically heterogeneous, with limited standardization in evaluation tools and study protocols (Schmidt-Kraepelin et al., 2020). Contributions span computer science, psychology, public health, and education, yielding divergent definitions, boundaries, and core elements of “gamification” in health (J. Kim et al., 2025; Tolks et al., 2024). Studies vary widely in how they define gamification, articulate theoretical foundations, and assess health outcomes (Berglund et al., 2022). Much of the knowledge base is still composed of experiential reports and prototypes, with limited theory-driven synthesis and sector-specific best practices (J. Kim et al., 2025). These inconsistencies make it difficult to appraise the overall contribution of digital health gamification to research and practice.
Addressing this gap requires a systematic, comprehensive view of the field. Bibliometric analysis provides a rigorous approach to map the knowledge structure, thematic evolution, and collaboration networks of a domain (Donthu et al., 2021). By examining publication trends, leading contributors, and emerging topics, bibliometrics helps identify knowledge clusters, track scientific influence, and highlight areas needing further inquiry (Passas, 2024). This approach is especially valuable for digital health gamification: by analyzing cross-disciplinary contributions and applying keyword and thematic clustering, bibliometrics can trace emerging directions in digital health and gamification and spotlight under-researched areas (Hegerty & Weresa, 2025).
It also offers systematic guidance for future studies, encouraging interdisciplinary innovation and refinement of theoretical frameworks (Yıldız et al., 2024). While these reviews provide useful starting points, their narrow scopes make it difficult to understand how digital health games, serious games, and gamification have evolved together as a broader research domain (Al-Azkiya & Rahmah, 2024; Algin, 2024; Y. Wang et al., 2022; Zohari et al., 2023). Because prior studies often examine only one strand of the field or focus on limited time periods, they cannot capture long-term thematic development, shifts in collaboration structures, or the increasingly prominent cross-disciplinary integration observed in recent digital health research (Algin, 2024; Yıldız et al., 2024; Zohari et al., 2023). As a result, a more comprehensive and integrated bibliometric assessment is needed to reveal how these related areas collectively shape the trajectory of digital health gamification.
Specifically, this study addresses the following research questions:
Addressing these questions provides significant theoretical insights into the interdisciplinary integration of digital health, gamification, behavioral theories, and computational technologies. Practically, this research offers actionable recommendations for healthcare providers, app developers, and policymakers.
Literature Review
The Fusion of Digital Health and Gamification
Gamification, emerging in the mid-2000s, refers to integrating game-like elements into non-game contexts to enhance user engagement and motivation (Jun & Lucas, 2024). In digital health, gamification supports health education, chronic disease self-management, mental health treatments, and preventive healthcare through enriched user experiences and enhanced motivation (Davaris et al., 2021; Litvin et al., 2020). Effective gamification elements in digital health include personalized interfaces, real-time progress feedback, social collaboration, and narrative-driven design (Berglund et al., 2022; J. Kim et al., 2025; Vermeir et al., 2020). Combined with randomized rewards and loss-aversion strategies, these elements effectively sustain user engagement and health behaviors (Tang et al., 2023).
Integrating computing and information science with digital health gamification represents a transformative interdisciplinary synergy, greatly improving the effectiveness and sustainability of digital health interventions (Yin, 2024). Advanced computing technologies, including AI, machine learning, big data analytics, and human-computer interaction (HCI) design principles, significantly enhance digital health platforms through personalized user experiences, adaptive interactions, and dynamic behavioral interventions tailored to individual needs (Tolks et al., 2024). AI-driven personalization is central to this integration, as machine learning algorithms analyze extensive user-generated data (e.g., behavioral patterns, learning indicators, and contextual preferences) to deliver customized gamification strategies (Narayanan & Kumaravel, 2024). Adaptive recommendation systems dynamically adjust task difficulty and content, ensuring optimal challenges to maintain sustained engagement and motivation (Gupta et al., 2024). Machine learning-driven predictive analytics further enhance intervention effectiveness by proactively identifying potential user disengagement or behavioral lapses (Farhan et al., 2023).
Ultimately, the fusion of computing and information science with digital health gamification leverages technological advancements to overcome traditional challenges such as user disengagement and behavioral inertia, fundamentally reshaping how digital environments support sustained health behaviors (Jha & Jha, 2025). Therefore, exploring research collaborations, emerging trends, and breakthrough advancements in digital health gamification has become increasingly important and necessary, such as collaboration among clinical experts, data scientists, ethicists, and patient representatives (Arora et al., 2024).
Additionally, it should be noted in the study context. In the broader landscape of game-based health interventions, related terms such as digital health games, serious games, and gamification are often used in overlapping ways across the literature. However, these constructs represent distinct conceptual approaches. Digital health games generally refer to game-based applications developed for health promotion, education, or therapeutic support, often leveraging interactive environments to influence behavior change (Lukka & Palva, 2023). Serious games constitute full game environments designed for non-entertainment purposes, integrating structured gameplay, narratives, and measurable learning or clinical outcomes, particularly in medical or health education contexts (Yıldız et al., 2024; Zohari et al., 2023). Gamification, by contrast, involves incorporating selected game elements—such as points, badges, leaderboards, or challenges—into non-game systems without developing a complete game environment, and is widely applied in digital health platforms to enhance motivation and adherence (Berglund et al., 2022; Jun & Lucas, 2024; Vermeir et al., 2020).
Although conceptually distinct, these constructs frequently converge within digital health research because authors often use them interchangeably in titles, abstracts, and keywords. This overlap reflects shared mechanisms related to motivation, engagement, and behavior change, as well as common application areas such as chronic disease management, mental health support, and lifestyle interventions (Y. Li et al., 2019; Y. Wang et al., 2022). As a result, bibliometric analyses naturally aggregate these constructs due to keyword co-occurrence patterns and the thematic proximity of their research domains (Al-Azkiya & Rahmah, 2024). For this reason, the present study acknowledges their conceptual differences while analyzing them collectively when they appear within the same bibliometric clusters.
Bibliometric Analytical Methods
Bibliometric analysis offers an objective and replicable approach to examining rapidly evolving interdisciplinary domains by extracting patterns from publication metadata rather than relying solely on narrative synthesis (Chen et al., 2023). For fields such as digital health gamification, whose contributions span medicine, computer science, engineering, psychology, and public health, this macro-level perspective is crucial for uncovering how knowledge accumulates, themes evolve, and collaborations emerge across disciplines and regions (Méndez Isla et al., 2024).
Conceptually, bibliometric analysis rests on the premise that the relationships embedded in metadata—such as co-authorship ties, keyword co-occurrence, citation links, and geographic distribution of research—reflect the social and intellectual structure of a field (J. Li et al., 2024). From this premise emerge two complementary layers of inquiry. Performance analysis quantifies the productivity and influence of authors, institutions, countries, and sources, thereby identifying leading contributors, channels of knowledge dissemination, and temporal growth patterns (Farooq, 2024). Science mapping reconstructs relational structures by modeling collaboration networks and thematic proximity, revealing cohesive communities, bridging actors, dominant topics, and emerging frontiers (Hegerty & Weresa, 2025).
This study applies performance analysis to trace the expansion of the field from 2005 to 2025, assess citation impact, and examine the distribution of research outputs across document and source types. These indicators capture the maturity of digital health gamification and provide context for subsequent findings, such as the concentration of influence and the pace of thematic diffusion (Doroiman, 2022). Co-authorship analysis then maps collaboration structures at the level of individual scholars, organizations, and countries, highlighting the extent of interdisciplinarity, the existence of regional “centers,” and the gaps between clusters (Bornmann, 2016; Doroiman, 2022). Such gaps signal missed opportunities for knowledge exchange, which are particularly consequential in translational domains such as chronic disease management and mental health (Babu Panackal et al., 2025).
Author keyword co-occurrence analysis further reconstructs the cognitive structure of the field (Passas, 2024). By modeling how concepts co-occur within documents, this analysis identifies stable research clusters—for example, behavior change, mobile health applications, rehabilitation and aging, mental health, and serious games—as well as technological enablers (Doroiman, 2022). Temporal overlays indicate which themes are consolidating and which are expanding, providing a principled way to distinguish enduring cores from emerging directions. Building on the co-word network, factorial analysis reduces high-dimensional thematic relationships into fewer latent dimensions (Liu & Prajapati, 2022). This step clarifies how applied intervention work, theory-driven studies of behavior and motivation, and technology-oriented innovations integrate into broader conceptual spaces, thereby linking practice domains with the theoretical and computational frameworks that support them (M. Wang & Chai, 2018).
Such a multi-layered design in bibliometrics aligns with the objectives of this study. Performance indicators address the questions of “who leads and how fast the field is growing”; collaboration mapping explores “how knowledge circulates and where fragmentation occurs”; and co-word and factorial analyses reveal “what constitutes the field and where it is heading.” Together, these techniques outline a clear social and intellectual architecture of digital health gamification, provide evidence-based baselines for comparing subfields and regions (Liu & Prajapati, 2022), and offer actionable guidance for future research.
Existing Bibliometric Studies on Digital Health and Gamification
Existing bibliometric reviews of digital health gamification remain limited, with constraints such as narrow database selections, restricted methodologies, fragmented thematic analyses, and inadequate temporal coverage. Previous reviews primarily relied on databases such as Web of Science (Algin, 2024; Y. Wang et al., 2022; Yıldız et al., 2024; Zohari et al., 2023), potentially excluding interdisciplinary literature from broader databases like Scopus. Additionally, earlier reviews often concentrated on narrow subfields such as digital nursing or medical education, lacking comprehensive analyses of gamification within the broader digital health context. Prior analyses also frequently overlooked structured thematic classifications (Al-Azkiya & Rahmah, 2024). Furthermore, limited analysis periods (Yıldız et al., 2024) hinder comprehensive tracking of long-term trends and interdisciplinary developments. To overcome these limitations, this study adopts advanced bibliometric approaches covering a 20-year timeframe, employing performance analysis, co-authorship analysis, co-occurrence analysis, and factor analysis based on data from the Scopus database. This study aims to deliver a comprehensive and multidimensional scholarly overview of the digital health gamification field. Table 1 compares previous bibliometric studies with the current review in addressing these limitations.
Comparison of this Study with Existing Bibliometric Research on Digital Health Gamification.
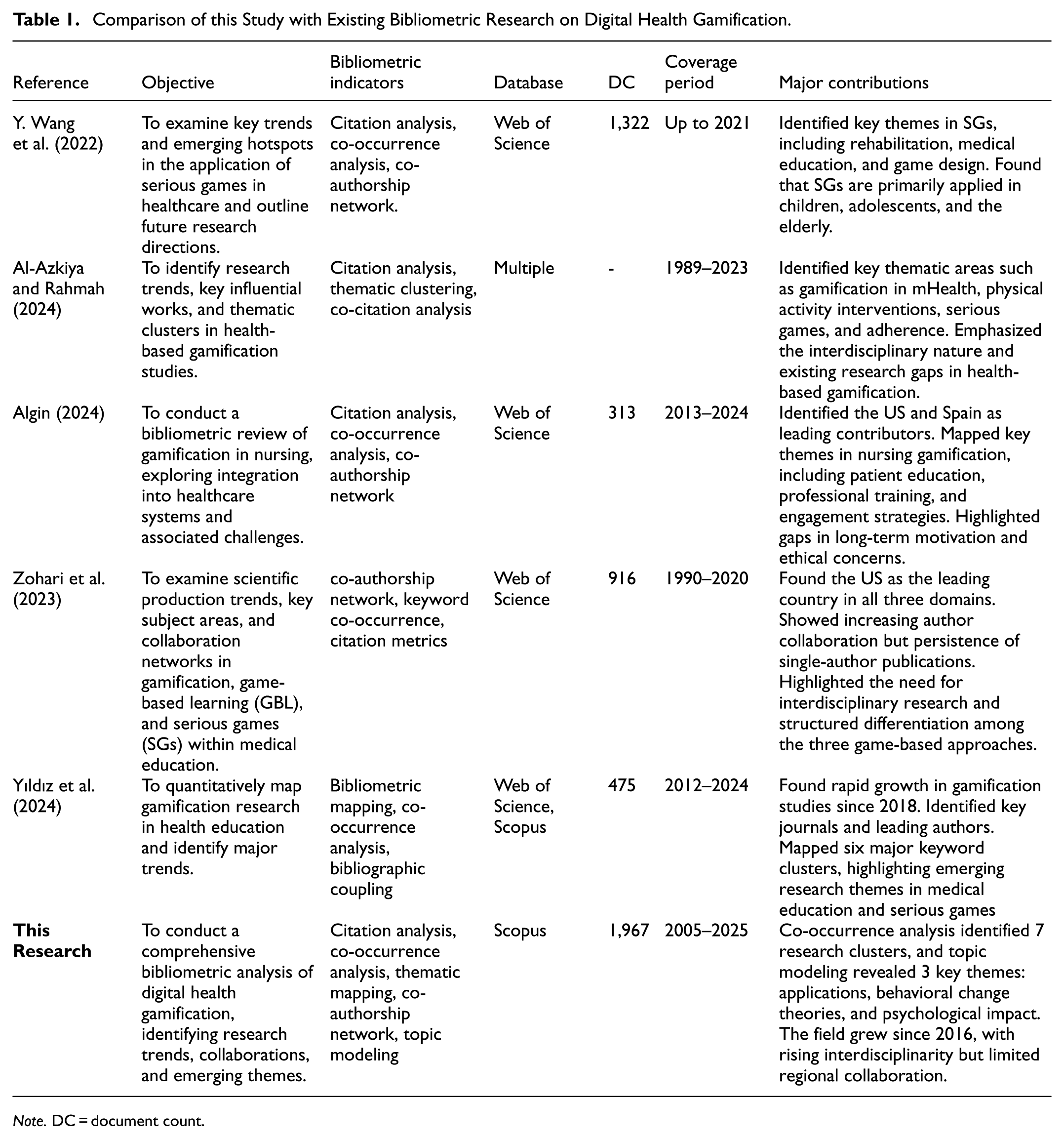
Note. DC = document count.
By bridging these gaps, this study presents a comprehensive bibliometric analysis of digital health and gamification research, enhancing theoretical insights, offering practical guidance for digital health practitioners, and serving as a methodological reference for future computational bibliometric studies.
Methods
Selection of Database
In bibliometric research, Scopus and Web of Science (WoS) are the two most commonly used databases. This study relies exclusively on Elsevier’s Scopus for several reasons. First, Scopus indexes a larger number of journals and offers broader disciplinary coverage than WoS, especially in engineering, computer science, and the social sciences, and includes all MEDLINE journals (Baas et al., 2020; Nwagwu, 2024). Evidence shows that Scopus covers more active scholarly journals (about 20,000) versus roughly more than 13,000 in WoS (Pranckutė, 2021), while WoS traditionally emphasizes the natural and engineering sciences (including agricultural sciences). Given the core domains of the present topic, Scopus enables richer and more expansive coverage, thereby adding value to the field (Malanski et al., 2021).
Second, Scopus provides a larger volume of records and citations; both the total number of retrievable documents and citation counts typically exceed those in WoS, supplying a more comprehensive empirical basis for bibliometric analysis (AlRyalat et al., 2019; Baas et al., 2020; Pranckutė, 2021).
Third, in several disciplines (e.g., pharmacy, engineering, applied sciences), Scopus retrieves medium-impact journals and conference proceedings not indexed by WoS, and its ingestion and update cycles are generally faster. As a result, Scopus tends to reflect the research frontier more promptly (Gorraiz & Schloegl, 2008; Pranckutė, 2021)—an important advantage for an emerging topic such as the one examined here.
Fourth, compared with other major databases, Scopus offers richer metadata and built-in analytics. Detailed fields for authors, affiliations, and funding facilitate multi-dimensional analyses (e.g., collaboration networks and institutional mapping), which are essential for large-scale, cross-disciplinary bibliometrics (AlRyalat et al., 2019; Baas et al., 2020). Because different databases use different formats, some scholars recommend selecting a single, fit-for-purpose source to reduce merging steps and potential human error (Donthu et al., 2021). On this basis, we chose Scopus.
Fifth, Scopus provides broader language coverage. An analysis of more than 6 million documents (2018) found Scopus to be more comprehensive across most languages and subject areas, offering stronger representation of scientific activity in non-English-speaking countries (Vera-Baceta et al., 2019). For this study, such coverage helps present a more accurate picture of national participation.
Finally, prior articles and books in core outlets have demonstrated that Scopus-only datasets can yield comprehensive and reliable bibliometric results (Ahmad Izhan et al., 2024; Banerjee et al., 2025; Malanski et al., 2021; Md Khudzari et al., 2018; Sweileh, 2018). For these reasons, Scopus was selected as the primary database. Figure 1 summarizes the main techniques employed in this study (Donthu et al., 2021). In this research, Bibliometric mapping was chosen for this study because it enables the analysis of large-scale patterns, trends, and relationships within the field (Ahmad Izhan et al., 2024). Unlike content analysis, which requires evaluating individual studies (Zhang et al., 2025), bibliometric mapping provides a systematic overview of thematic development and collaboration structures (J. Li et al., 2024), making it more suitable for this research’s objectives.
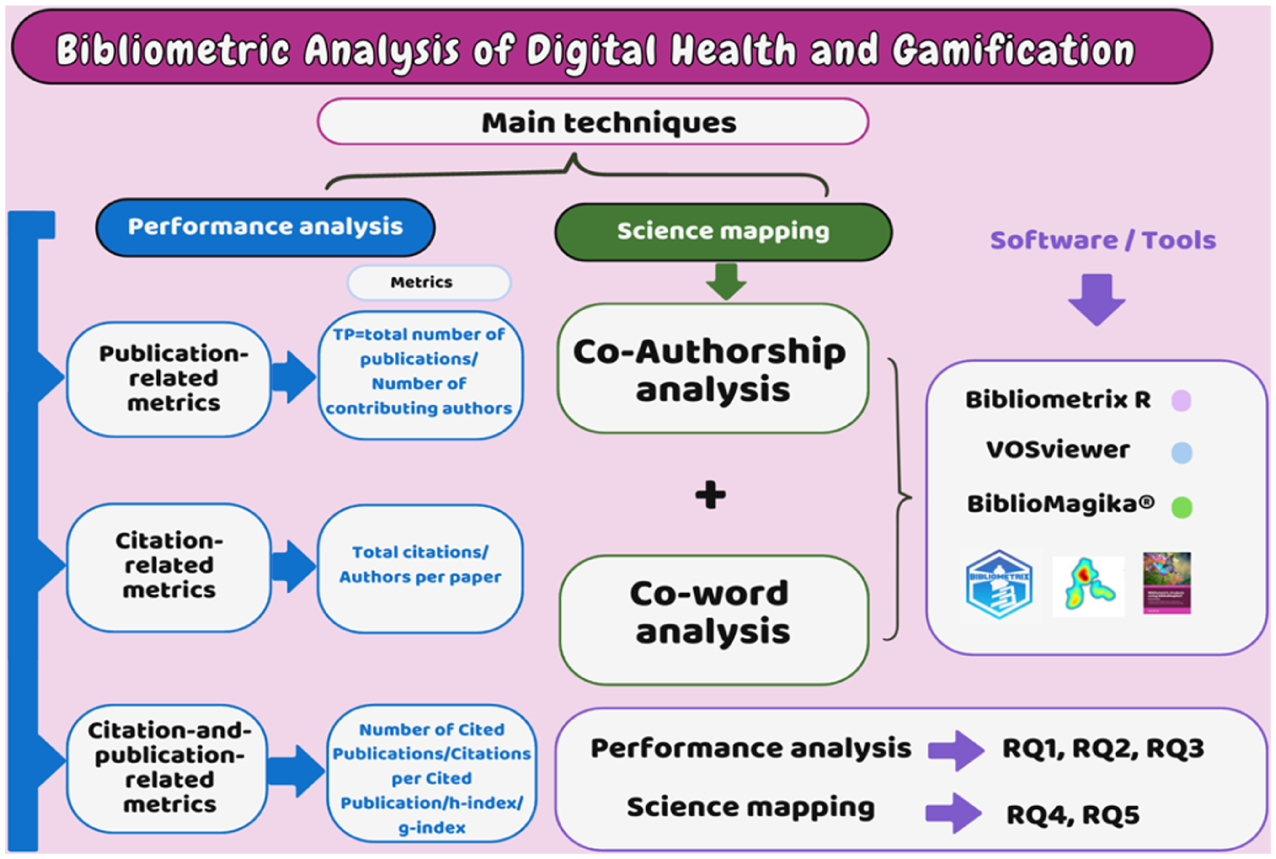
Techniques for conducting bibliometric analysis in this research.
Although Scopus offers broad coverage and strong support for cross-disciplinary bibliometric work, relying on a single database may still introduce certain limitations. Scopus indexes a large share of English-language journals, which may lead to an overrepresentation of English-language scholarship and an underrepresentation of work published in other languages. In addition, this study did not include gray literature such as theses, reports, and industry documents, which may contain relevant insights but fall outside formal academic indexing. These factors should be taken into account when interpreting the results.
Literature Search and Selection Procedure
The identification of relevant literature followed the PRISMA 2020 standards (Haddaway et al., 2022). A comprehensive search was conducted in Elsevier’s Scopus database on January 21, 2025, using the following query: TITLE-ABS-KEY ((“mobile fitness” OR “online health” OR “telehealth” OR “mobile health” OR “mhealth*” OR “ehealth*” OR “digital health” OR “health apps”) AND (“game*” OR “gamification” OR “Gamified”)).
This search strategy was designed to capture the broad terminology used to describe digital and mobile health technologies (e.g., mHealth, eHealth, telehealth, and health apps) together with game-based concepts, including both the general term “game*” and the more specific terms “gamification” and “gamified” (Lukka & Palva, 2023; Y. Wang et al., 2022). By combining these terms, the search ensured the inclusion of both general game-related interventions and explicitly gamified digital health applications.
No restrictions were applied regarding publication year, language, source type, or document type to maintain comprehensive coverage. The initial search returned 1,967 records published between 2005 and early 2025. After automatic duplicate removal within Scopus, 1,924 records proceeded to screening. Titles and abstracts were reviewed to identify studies explicitly addressing digital health in combination with gamification or game-based elements. Articles were excluded if they represented undetected duplicates or were unrelated to the study scope. A total of 1,306 records were excluded during the screening process, leaving 618 studies that met all the inclusion criteria for bibliometric analysis.
The detailed selection procedure is illustrated in Figure 2 (PRISMA flowchart).

The PRISMA 2020 flowchart for identifying relevant literature included in the study.
Data Preprocessing and Standardization
To ensure data quality, consistency, and reliability, OpenRefine was employed for data cleaning and harmonization (Verborgh & De Wilde, 2013). OpenRefine, a widely-used computational tool in information science, standardizes author names, keywords, and publication details, crucial for accurate bibliometric analysis (Mozzherin et al., 2024). During data preprocessing, duplicate records, inconsistent author names, keyword variations, and formatting issues were systematically identified and corrected, thereby enhancing data accuracy for subsequent computational analysis.
Bibliometric Analytical Techniques and Tools
VOSviewer (van Eck & Waltman, 2010) was applied to visualize author and keyword co-occurrence networks, revealing key research clusters and emerging topics. biblioMagika® (Ahmi, 2024a) facilitated citation analysis, identifying leading authors, citation counts, and publication trends to assess research impact quantitatively. Biblioshiny, part of the bibliometrix R package, was utilized for trend analysis (Lazar & Chithra, 2021). To ensure interpretability and reduce noise, the research set specific thresholds across analyses: a minimum of two publications per author, for co-authorship at the author level, at least five publications per country for co-authorship at the country level, and a minimum occurrence of 5 for author keywords in the co-word analysis (Ahmi, 2024b).
Results
Performance Analysis
To address
Citation Metrics
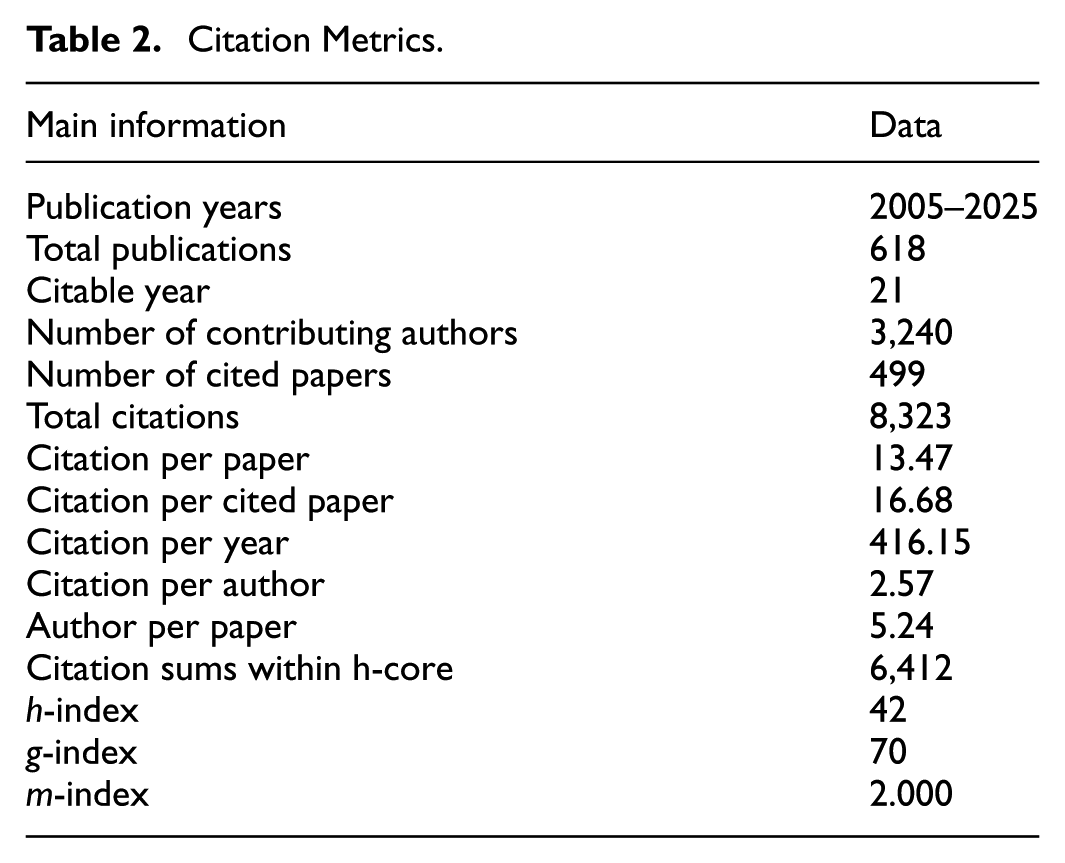
Regarding citation metrics (Table 2), the dataset (2005–2025) reflects two decades of growing scholarly interest in digital health gamification. With 8,323 citations, an h-index of 42, and a g-index of 70, the field demonstrates strong academic impact. The m-index (2.000) indicates sustained influence over time. An average of 13.47 citations per paper and 16.68 per cited paper suggests a moderate to high citation rate. The 3,240 contributing authors and 5.24 authors per paper highlight a collaborative research landscape. Additionally, 416.15 citations per year underscore the field’s increasing relevance.
Citation Metrics.
Document Type Analysis
The document type analysis in Table 3 reveals that journal articles (50.65%) and conference papers (37.54%) dominate the field, reflecting a balance between peer-reviewed scholarship and emerging research presented at conferences. The presence of 55 review papers (8.90%) suggests an ongoing effort to synthesize existing knowledge. Other document types, including book chapters (1.29%), editorials (0.81%), and letters (0.32%), contribute minimally, indicating that digital health gamification research is primarily disseminated through formal academic channels. The single short survey (0.16%) underscores the field’s limited engagement with brief empirical overviews.
Document Type.

Source Type Analysis
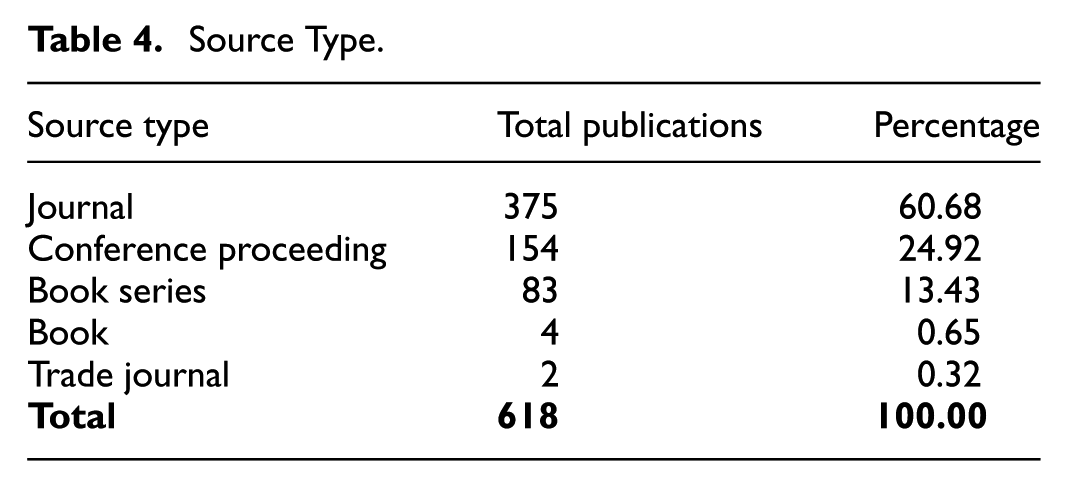
Table 4 shows journals (60.68%) as the primary publication venue for digital health gamification research, emphasizing peer-reviewed dissemination. Conferences (24.92%) also play a key role in showcasing emerging findings, while book series (13.43%) provide thematic depth. Books (0.65%) and trade journals (0.32%) are minimally represented, underscoring the academic rather than industry-driven nature of the field.
Source Type.
Language Analysis
The language distribution in Table 5 reveals that English (98.71%) overwhelmingly dominates publications on digital health gamification, reinforcing its status as the primary academic language in this domain. The minimal presence of German (0.65%), Spanish (0.32%), Italian (0.16%), and Portuguese (0.16%) suggests limited contributions from non-English sources.
Languages.

Subject Area Analysis
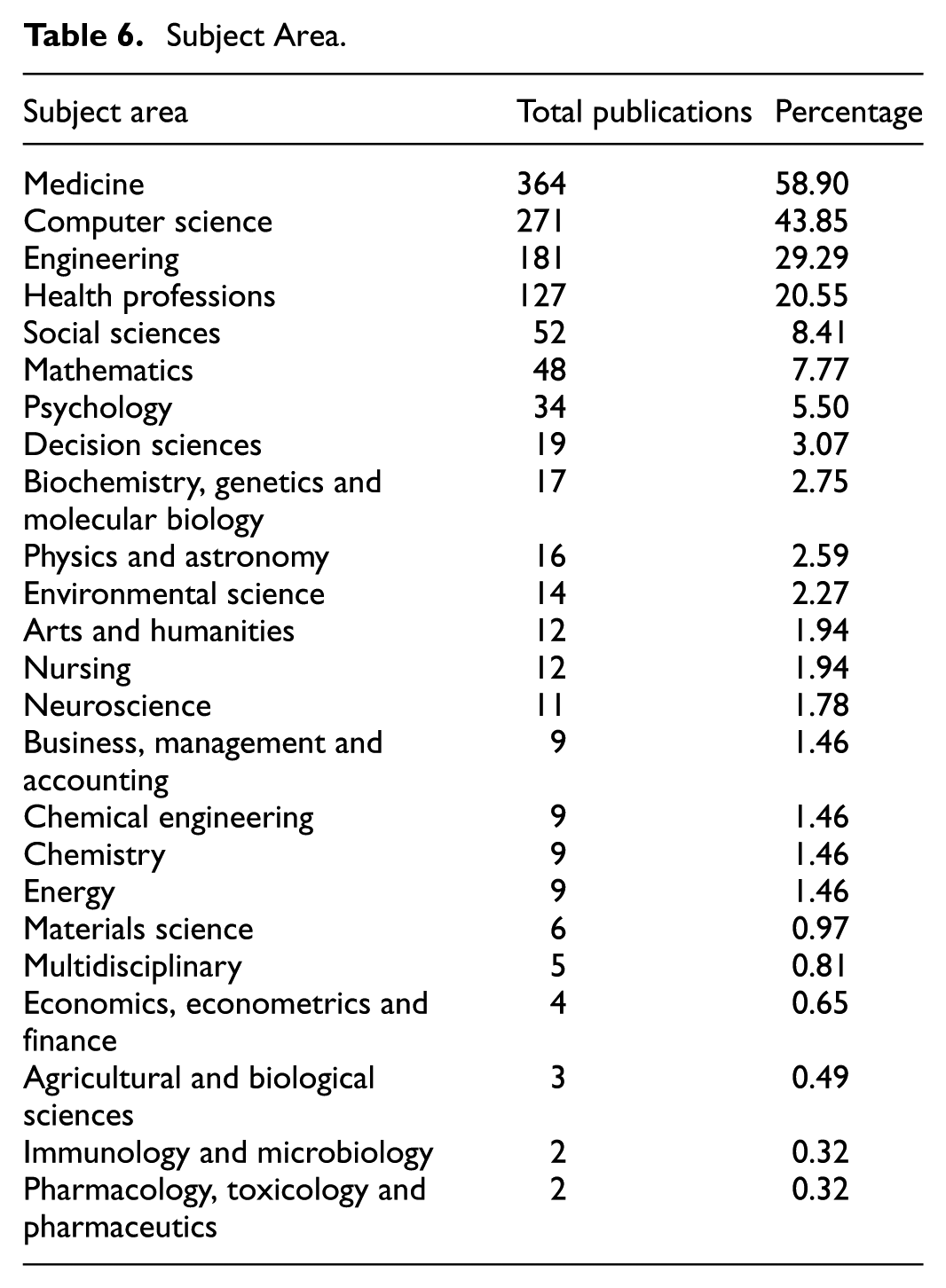
Table 6 illustrates the interdisciplinary nature of digital health gamification research, led by medicine (58.90%), computer science (43.85%), and engineering (29.29%), highlighting healthcare applications and technological developments. Significant contributions from health professions (20.55%) suggest practical clinical and public health implications, while social sciences (8.41%), psychology (5.50%), and decision sciences (3.07%) underscore behavioral and cognitive interests. Mathematics (7.77%), biochemistry (2.75%), and physics (2.59%) reflect computational and bioinformatics involvement, whereas limited business (1.46%) and economics (0.65%) representation indicates minimal exploration of market-related aspects.
Subject Area.
The Publication Trends of Digital Health Gamification
To address
Table 7 illustrates publication trends in digital health gamification research, showing low output (under 20 papers per year) from 2005 to 2015, followed by rapid growth from 2016, peaking in 2024 (98 publications). Early studies (2014–2015) received high citations (46.25 citations per paper in 2015), while recent works (2023–2024) show lower citation counts, likely due to recency. Overall, the surge since 2016 suggests growing interdisciplinary maturity in the field.
Publication by Year.

Source. Generated by the authors using biblioMagika® (Ahmi, 2024a).
Note. Year-level h-, g-, and m-indices are computed separately for each publication year by the bibliometric software. Global h-, g-, and m-indices for the full 2005 to 2025 dataset are reported in Table 2. TP = total number of publications; NCA = number of contributing authors; NCP = number of cited publications; TC = total citations; C/P = average citations per publication; C/CP = average citations per cited publication; h = h-index; g = g-index; m = m-index.
Figure 3 presents the annual distribution of publications and total citations, highlighting the field’s growth trend. From 2005 to 2015, research output remained relatively low, with fewer than 20 publications per year. However, from 2016 onward, there was a marked increase, peaking in 2024 with 98 publications, indicating a surge in scholarly interest. Notably, 2016 saw the highest citation count (1,350), suggesting that foundational works from this period have had a significant impact. While 2020–2022 sustained high publication output, citations began to decline, reflecting the time required for newer studies to gain recognition.

Annual distribution of publications and citations.
Figure 4 shows an exponential increase in cumulative publications on digital health gamification, with a strong quadratic regression fit (R2 = 0.9934). Publication growth was initially slow (2005–2015) but sharply accelerated after 2016, reflecting rising scholarly engagement and the field’s growing interdisciplinary significance.
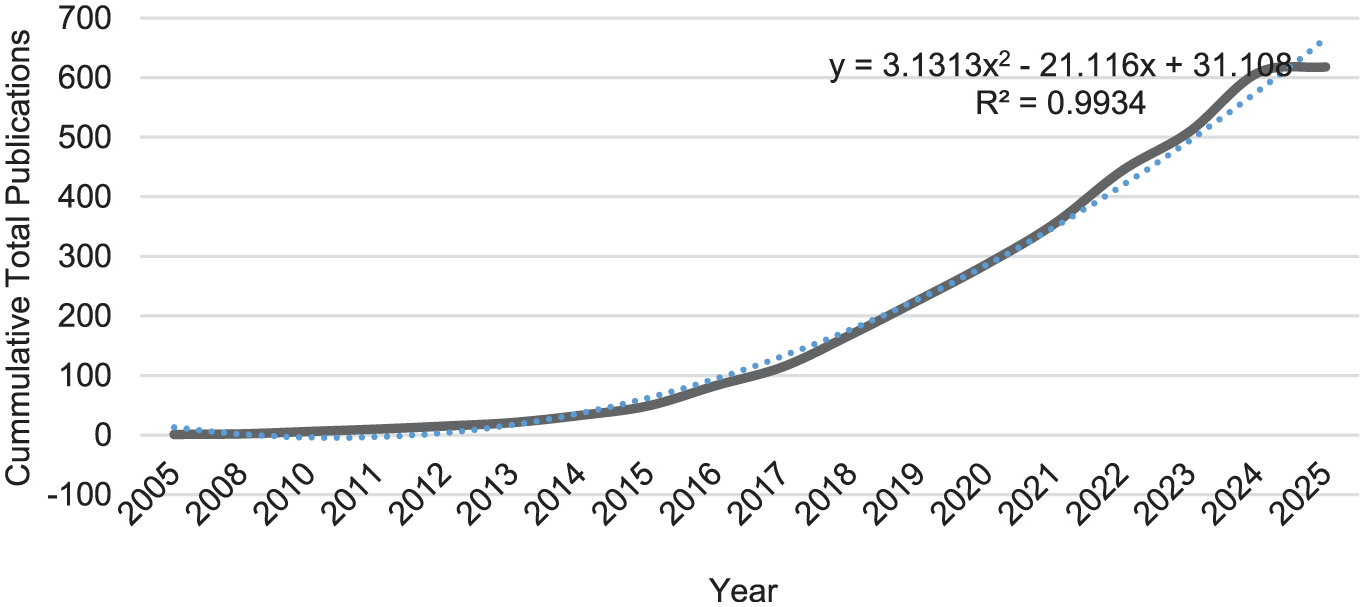
Publication growth.
The Key Players in Digital Health Gamification Research
To address
As shown in Table 8, the most productive authors in digital health gamification research are led by Aigner, Baranyi, and Grechenig from the Technical University of Vienna, Austria, each contributing six publications, making them the most prolific scholars in the field. Other notable contributors include Hlavacs (University of Vienna, Austria), Kowatsch (University of St. Gallen, Switzerland), and Barnes (SWPS University, Poland), each with five publications, indicating a strong European presence in research output. Despite having fewer publications, Cheng (The University of Sydney, Australia) and Vella (Queensland University of Technology, Australia) exhibit the highest citation impact, with 194 and 175 total citations, respectively, and an average citation per publication of 48.50 and 43.75, highlighting their influential contributions. Similarly, Johnson (Queensland University of Technology, Australia) and Christmann (Technische Universität Kaiserslautern, Germany) also demonstrate high citation density, suggesting significant recognition of their work. Overall, the author network reflects a concentration of research efforts in Europe and Australia, with some key contributors in North America.
Leading 20 Most Productive Authors.

Note. TP = total number of publications; NCA = number of contributing authors; NCP = number of cited publications; TC = total citations; C/P = average citations per publication; C/CP = average citations per cited publication; h = h-index; g = g-index; m = m-index.
Analysis of top institutions in digital health gamification research (Table 9) reveals a globally interconnected network, led by the University of Twente (Netherlands) with 12 publications and 127 citations. High-impact institutions include the University of California (201 citations, C/P 20.10) and Harvard Medical School (180 citations, C/P 22.50). The University of Auckland (C/P 37.00) and Duke University (C/P 27.67) exhibit exceptional citation density. Institutions like the University of Sydney and Imperial College London further highlight international influence. U.S. universities, including Emory, Northeastern, and USC, alongside European counterparts (e.g., Radboud, Eindhoven, UCL), underscore strong interdisciplinary leadership.
Top 20 Leading Institutions with at Least 5 Publications.
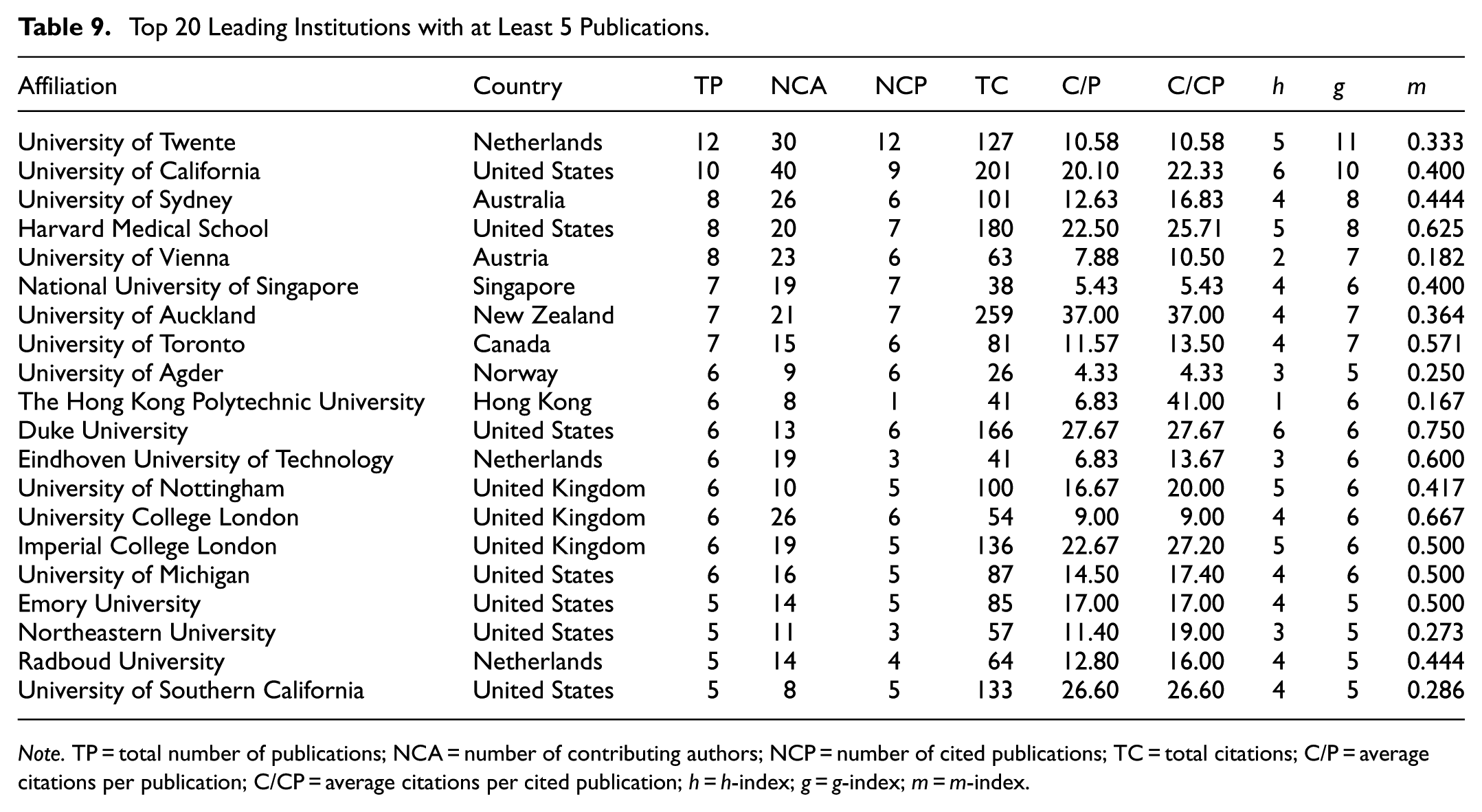
Note. TP = total number of publications; NCA = number of contributing authors; NCP = number of cited publications; TC = total citations; C/P = average citations per publication; C/CP = average citations per cited publication; h = h-index; g = g-index; m = m-index.
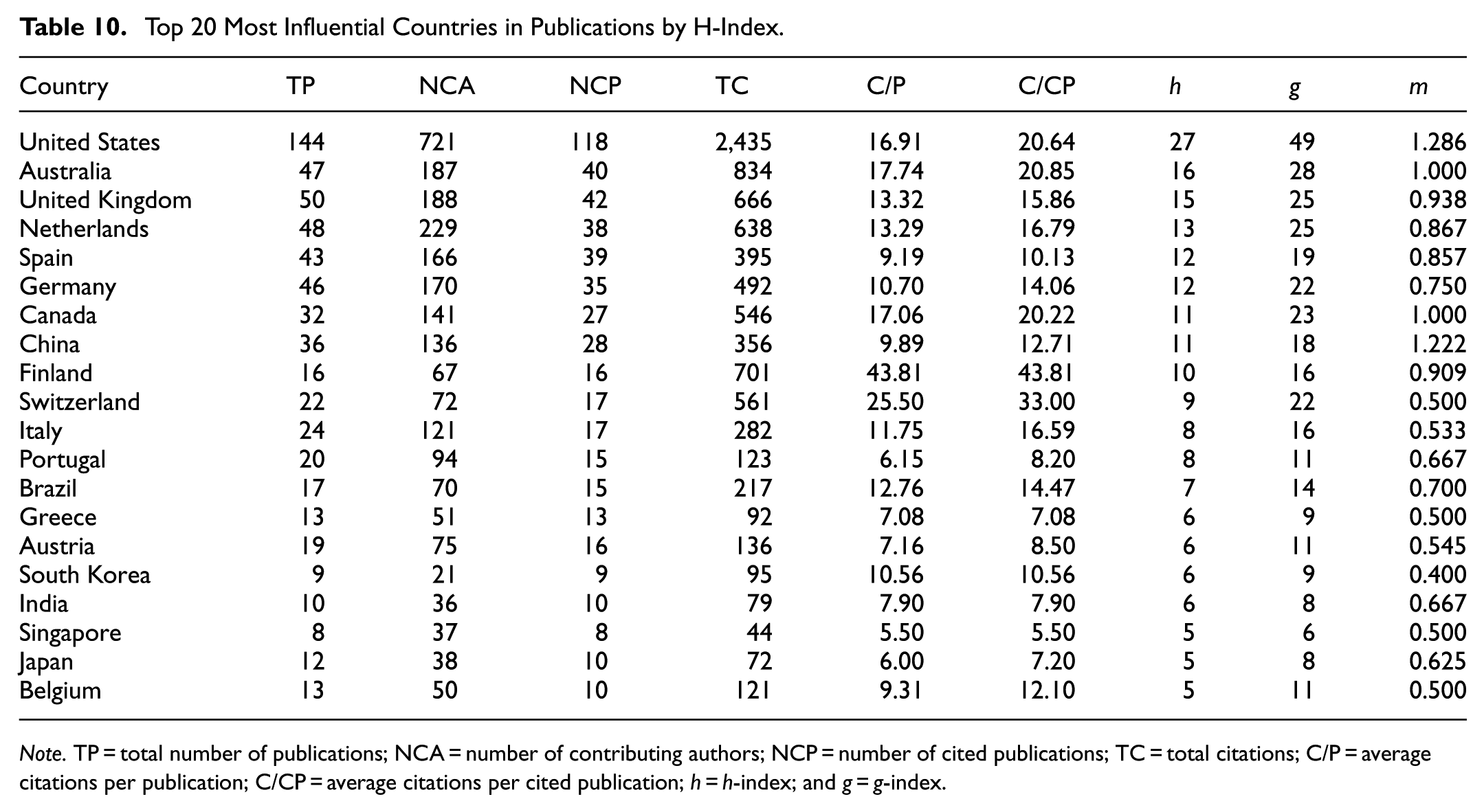
Analysis of top contributing countries (Table 10) shows the United States leading digital health gamification research, with 144 publications, highest h-index (27), and total citations (2,435). Australia (47 publications, h-index 16, C/P 17.74), the United Kingdom (50 publications, h-index 15, C/P 13.32), the Netherlands, and Canada also significantly contribute. Finland, despite fewer publications (16), has the highest citations per publication (43.81), indicating substantial academic influence, along with Switzerland (C/P 25.50) and Germany (C/P 10.70). Emerging contributors include China and Spain, while Italy, Portugal, and Brazil have moderate engagement. Overall, the U.S., Australia, and the U.K. dominate, with European and Asian countries steadily increasing their research presence.
Top 20 Most Influential Countries in Publications by H-Index.
Note. TP = total number of publications; NCA = number of contributing authors; NCP = number of cited publications; TC = total citations; C/P = average citations per publication; C/CP = average citations per cited publication; h = h-index; and g = g-index.
Global scientific output on digital health gamification indexed in Scopus highlights the United States as the leading contributor (144 publications), followed by Australia (47), China (36), Canada (32), and the United Kingdom (20). Research activity is also notable across Europe, Asia, and South America (Figure 5).

Worldwide scientific production indexed by Scopus on digital health gamification.
Science Mapping
The Patterns of Co-Authorship
To address
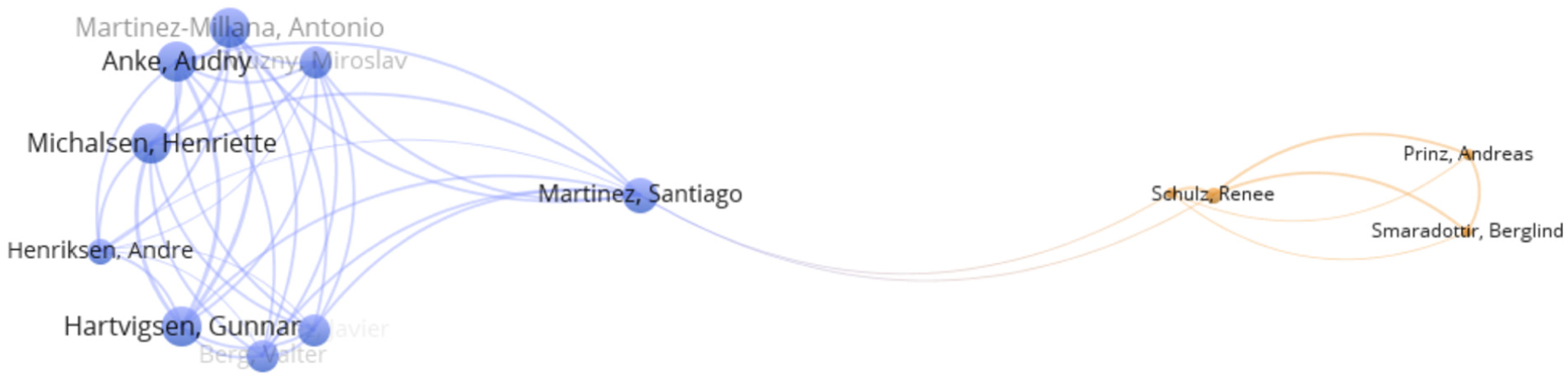
Co-authorship by author.
Figure 7 illustrates authorship trends across 618 digital health and gaming studies (2005–2025), revealing a consistent rise in multi-author collaborations and a decline in single-author papers since 2011, indicating a clear shift toward interdisciplinary research.

Single author versus multi authors.
The co-authorship network of institutions reveals a well-connected but fragmented collaboration structure, with multiple clusters of institutions forming distinct research hubs (Figure 8). Duke University (United States), Emory University (United States), and the University of Michigan (United States) emerge as key nodes in the network, indicating their central role in collaborative research. Duke University, in particular, has a high total citation count (166) and an average of 27.67 citations per publication, reflecting its strong influence in the field. Similarly, the University of California (United States) and Imperial College London (United Kingdom) exhibit high citation densities, suggesting that their research contributions are well-recognized.

Co-authorship by organization.
Other notable institutions, such as ETH Zurich (Switzerland), the National University of Singapore, and the University of Toronto (Canada), show moderate connectivity but contribute to global collaboration efforts. The Hong Kong Polytechnic University and Harbin Institute of Technology (China) represent the growing involvement of Asian institutions, although their network reach remains relatively limited compared to North American and European counterparts. The University of Florida (United States) and Radboud University (Netherlands) also appear as influential institutions with strong citation performance. However, the presence of isolated institutions with fewer connections suggests room for further international collaboration, particularly in linking European and Asian research networks to the more dominant North American hubs.
For the co-authorship by country analysis in VOSviewer (Figure 9), the analysis type was set to “Co-authorship,” using “Countries” as the unit and the “Full counting” method. Documents involving more than 25 countries were excluded to minimize interference. The threshold for inclusion was set at a minimum of five publications per country (Ahmi, 2024b), resulting in 34 countries meeting the criteria out of 67. The co-authorship network formed seven distinct clusters representing regional collaboration patterns. Cluster 1 (Green – North America) is dominated by the United States, functioning as the global research hub with extensive interdisciplinary collaborations, notably with Canada, Switzerland, and Australia. Cluster 2 (Red – Core Europe) includes Germany, Spain, and Finland, forming strong intra-European ties and active connections with North America. Cluster 3 (Orange – UK and Western Europe), involving the UK, Italy, Belgium, and Portugal, bridges North American and European research. Cluster 4 (Blue – Asia-Pacific Expansion), led by Australia, highlights growing research influence from Singapore, India, and Hong Kong. Cluster 5 (Yellow – Emerging European Contributors) includes France and Poland, exhibiting moderate international collaborations. Cluster 6 (Light Blue – Latin America and Peripheral Nations), represented by Brazil and Malaysia, shows emerging but limited global engagement. Lastly, Cluster 7 (Purple – Isolated and Weakly Connected Countries) encompasses smaller European nations, indicating limited international collaboration. Overall, North America and Europe remain central research hubs, while the Asia-Pacific region is rapidly increasing its global influence, suggesting a trend toward a more interconnected global research landscape in digital health gamification.

Co-authorship by country.
The Co-occurrence Analysis
A threshold of 5 publications per country (Ahmi, 2024b) and a minimum citation count of 0 resulted in 116 out of 1,763 author keywords meeting the criteria. The co-occurrence analysis (Figure 10) of author keywords in digital health gamification research reveals seven major clusters, representing thematic areas of interest and emerging trends.
Cluster 1 (Blue - Gamification & Digital Health) forms the core research theme, with “gamification,”“ehealth,” and “serious game” as central concepts. This cluster highlights the integration of gamification into digital health interventions, with related topics like “mobile health,”“virtual reality,” and “user engagement” reinforcing its applied focus.
Cluster 2 (Orange - Behavior Change & mHealth Applications) emphasizes behavioral interventions, linking “mobile health (mHealth),”“prevention,” and “health behavior” to “smoking cessation” and “self-determination theory.” This cluster reflects the growing role of gamified mobile applications in promoting health-related behavior change.
Cluster 3 (Green - Public Health & Chronic Diseases) focuses on disease-specific applications, particularly in “diabetes,”“HIV,” and “youth self-management.” The inclusion of “digital health intervention” and “public health” suggests a strong emphasis on gamified health strategies for chronic disease management and population health initiatives.
Cluster 4 (Yellow - Aging, Cognition & Rehabilitation) centers on “aging,”“dementia,” and “stroke,” highlighting cognitive health and rehabilitation. Terms like “telerehabilitation,”“motivation,” and “healthcare” indicate the integration of gamification in elderly care and cognitive training.
Cluster 5 (Purple - Mental Health & Serious Games) explores mental health applications, connecting “depression,”“anxiety,” and “cognitive behavioral therapy” with “serious games” and “biofeedback.” This cluster underscores the therapeutic potential of gamified interventions for psychological well-being.
Cluster 6 (Light Blue - Education & Game Design) focuses on “educational game,”“game design,” and “usability,” reflecting research on gamified learning experiences. The presence of “cognitive behavioral therapy” and “engagement” suggests the use of gamification in behavioral interventions and therapy-based learning.
Cluster 7 (Pink - AI, Wearables & Emerging Technologies) includes “artificial intelligence,”“machine learning,” and “wearables,” indicating the increasing role of AI-driven gamification in health tracking and intervention personalization.

Network visualization of co-occurrence analysis.
Factorial Analysis
To identify popular topics and themes for
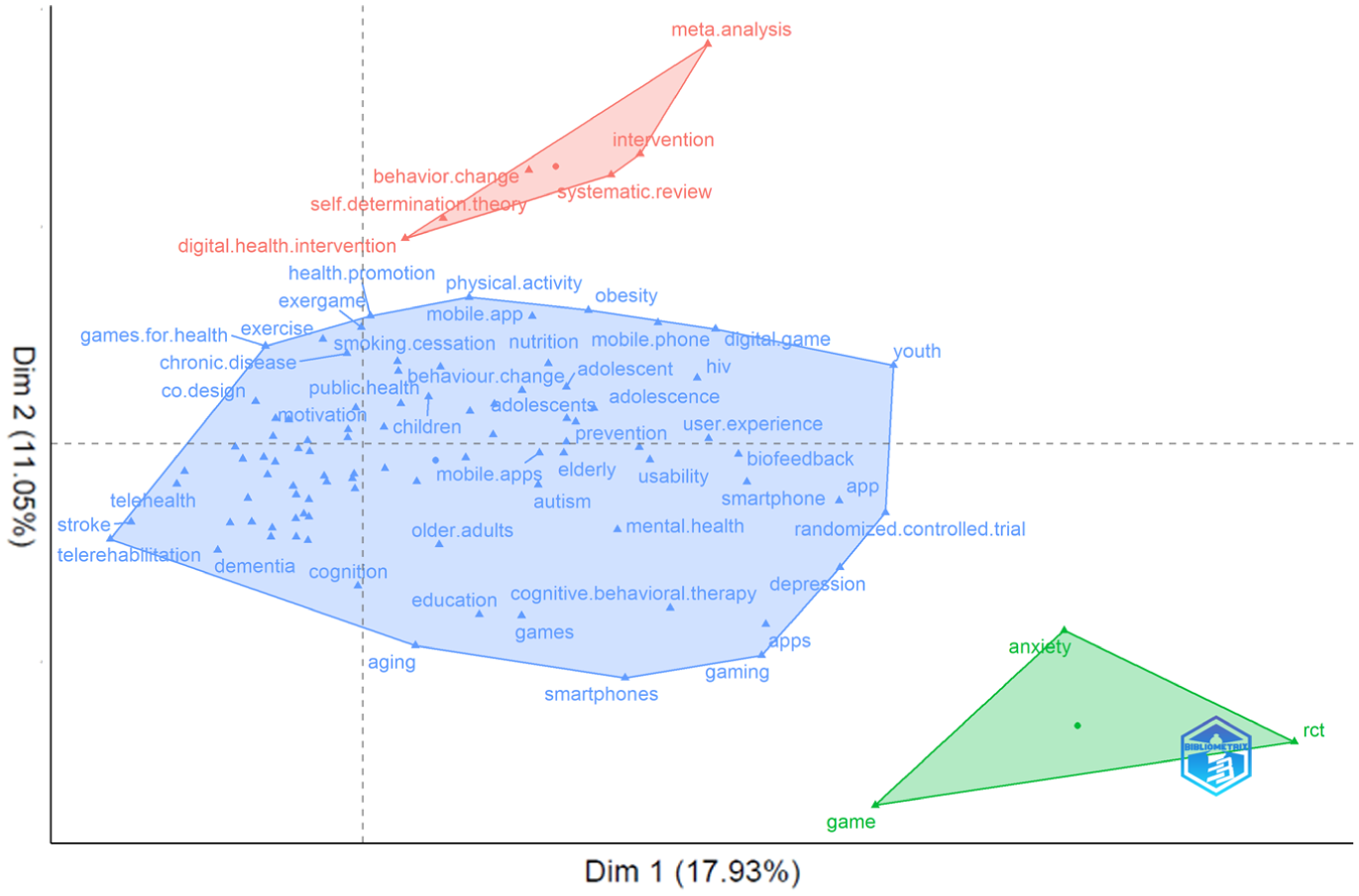
Factorial analysis using Biblioshiny (method: MCA).
The first cluster (Blue - Digital Health & Gamification Applications) focuses on applied research, integrating digital health interventions, physical activity, mobile applications, and cognitive behavioral therapy. It highlights the practical implementation of gamification in healthcare, addressing areas such as chronic disease management, rehabilitation, and mental health support. The second cluster (Red - Systematic Reviews & Behavioral Change Theories) centers on meta-analyses, systematic reviews, and behavior change theories. This reflects the theoretical foundation of gamification research, emphasizing the evaluation of intervention effectiveness and the role of self-determination theory in shaping behavioral outcomes. The third cluster (Green - Experimental Research & Psychological Impact) is characterized by randomized controlled trials (RCTs), anxiety, and gaming, indicating a strong empirical focus on psychological well-being. This suggests that gamified health interventions are frequently assessed through controlled experiments, particularly in mental health and user engagement studies.
Discussion
This study presents a bibliometric analysis of digital health gamification research, exploring its current landscape, publication trends, key contributors, collaboration networks, thematic evolution, and emerging research topics.
Based on the results of
Also, at the author level, European and Australian scholars have made significant contributions, with researchers from institutions such as the Technical University of Vienna in Austria and the University of St. Gallen in Switzerland demonstrating high publication output and impact. These findings are consistent with previous studies on digital health research (Hu et al., 2024).
Based on the results of
Based on the results of
First, this study identifies that gamification plays a crucial role in enhancing user engagement in health behaviors within the digital health domain. Specifically, “behavior change” emerges as one of the core themes, underscoring gamification’s significance as a tool for health interventions. However, while previous studies widely acknowledge that gamification can facilitate short-term behavior changes (Rosli & Omar Zaki, 2023), its long-term sustainability remains debated. Some studies highlight the phenomenon of “gamification fatigue,” where users lose motivation over time, potentially limiting its long-term effectiveness (Armaou et al., 2024; Y. Li et al., 2019). Future research should explore strategies to extend user engagement through personalized and adaptive gamification mechanisms, such as AI-driven dynamic content adjustments, to sustain user motivation and long-term health behaviors (Armaou et al., 2024).
Second, mobile health (mHealth) has become a key platform for gamified health interventions, particularly in smoking cessation, weight management, and physical activity promotion. This study finds that “mobile health” and related terms occupy a prominent position in the co-occurrence analysis, aligning with previous research (Y. Li et al., 2019). The integration of gamification within mHealth applications suggests its growing relevance in mobile-based health interventions.
Third, chronic disease management has emerged as a critical application of gamified health interventions, especially in the management of diabetes, HIV, and cardiovascular diseases. This study identifies that keywords such as “diabetes” and “public health” exhibit strong connectivity in the co-occurrence analysis, indicating a shift in research focus from mere behavior change to chronic disease management. Factorial analysis further reveals that gamified interventions can enhance patient self-management. High-quality randomized controlled trials (RCTs) remain a widely used approach to assess their long-term impact on specific health outcomes, such as blood glucose levels and blood pressure regulation. However, existing research also suggests limitations in evaluating long-term behavioral changes in patients (Song et al., 2023).
Fourth, mental health represents a well-established domain for gamified interventions, particularly in addressing anxiety, depression, and cognitive behavioral therapy (CBT), forming a distinct research area. The study finds that terms such as “depression” and “anxiety” occupy central positions in the co-occurrence analysis, consistent with existing literature (Y. Li et al., 2019). However, gamification in mental health remains a double-edged sword. While gamified psychological interventions can enhance user engagement, poorly designed interventions may lead to unintended consequences, such as gaming addiction or social isolation (Al Hussaini et al., 2024). Future research should rigorously evaluate the long-term safety of gamified mental health interventions, ensuring that while enhancing user experience, potential adverse effects are mitigated (Gilbody et al., 2023).
Finally, AI is identified as an emerging topic in gamified health interventions, primarily in personalized recommendations, predictive modeling, and dynamic content adaptation. This study finds that terms such as “artificial intelligence” and “machine learning” form an independent research cluster in factorial analysis, suggesting that AI technologies are increasingly driving innovation in gamified health interventions. However, ethical concerns related to AI-driven gamification remain insufficiently addressed, including issues of data privacy, algorithmic transparency, and potential manipulation (F. Li et al., 2022). These concerns call for more transparent AI governance and ethical frameworks to ensure fairness and interpretability in AI-driven gamification (Anyanwu et al., 2024).
Specifically, data privacy and security must be prioritized, as gamified platforms often combine sensitive health records with fine-grained behavioral logs (F. Li et al., 2022), increasing the risk of data breaches and misuse. As these platforms become more personalized through AI, ensuring robust data protection measures, such as data minimization, informed consent, and opt-out options, is crucial. Second, algorithmic transparency and explainability are needed to avoid opaque reward structures or nudges that may undermine user autonomy, particularly in mental health contexts (Anyanwu et al., 2024). Third, fairness audits should be conducted to detect performance differences across age, gender, and cultural groups; otherwise, reward schemes or difficulty adjustments may encode bias (J. Park et al., 2022). Attention should be paid to cultural factors. Research indicates that attitudes toward competition, rewards, and social interaction may vary significantly across cultures, thereby influencing the effectiveness of gamification interventions (J. Sun et al., 2025). For instance, some cultures may embrace competitive elements like leaderboards, while others may favor collaborative tasks. Consequently, the cultural sensitivity of gamification interventions is crucial for ensuring their global applicability and success. Future research should explore how gamification can be adapted to respect these cultural differences, thereby ensuring its applicability and impact across diverse regions. Also, accountability and safety should be ensured through human oversight, incident reporting, and preregistered evaluation protocols in clinical settings (Festor et al., 2025). To put these principles into practice, we recommend privacy-by-design approaches (e.g., data minimization, explicit consent, and opt-out options), transparent personalization logic, routine bias testing for key subgroups, and independent review of high-risk interventions.
Finally, economic and business implications need to be critically assessed. While gamified health interventions are often positioned as low-cost alternatives to traditional healthcare models, their long-term sustainability remains uncertain (Duffy et al., 2022). Many gamified platforms are developed by private companies, raising concerns about the commercialization of health (Weber et al., 2024). The focus on profit generation could influence the design of interventions, potentially compromising their ethical foundations. Moreover, the effectiveness of gamified interventions in low-resource settings, where access to technology and healthcare is limited, remains underexplored (Duffy et al., 2022). These factors highlight the need for more research into the economic viability of gamification in diverse healthcare contexts and its potential impact on healthcare equity.
Implications
This study offers significant theoretical, practical, and methodological implications for digital health gamification research.
The current study provides substantial theoretical implications by identifying seven distinct thematic clusters. Furthermore, through factorial analysis, these themes are systematically condensed into three core research dimensions: practical applications, behavioral theories, and psychological impact studies. These findings enrich theoretical insights by demonstrating clear linkages among gamification strategies, technology adoption, and sustained health behavior changes. Specifically, the identified cluster emphasizing behavior change and mHealth interventions highlights the theoretical integration between gamification principles and established models such as the Technology Acceptance Model (TAM), Unified Theory of Acceptance and Use of Technology (UTAUT), and Health Belief Model (HBM). Additionally, the emerging themes of AI-driven gamification and wearable technologies extend theoretical understanding in computing and information science by highlighting how personalized recommendation algorithms, adaptive feedback systems, and computational modeling techniques improve user engagement, adherence, and long-term behavior change. From an information science perspective, this underscores the importance of data-driven personalization and interactive user interfaces in shaping effective digital health interventions.
Importantly, this study reveals the increasing significance of psychological and experimental research within gamification studies. Such findings necessitate extending theoretical frameworks beyond traditional technology adoption models to incorporate intrinsic motivational theories, psychological empowerment, and emotional engagement processes. Therefore, future theoretical developments in digital health gamification should more explicitly integrate behavioral psychology and human-computer interaction theories to comprehensively explain the complex mechanisms underlying gamification’s long-term effectiveness.
Practically, the insights from this thematic analysis offer specific, actionable recommendations for health practitioners, app developers, and policy makers. First, the results indicate significant opportunities for practitioners to effectively utilize gamification elements in managing chronic diseases such as diabetes and HIV, cognitive rehabilitation for elderly populations, and mental health interventions targeting anxiety and depression. For example, healthcare providers and app developers can directly implement validated gamification strategies, including adaptive feedback loops, personalized task challenges, and interactive social features, to improve patient adherence and health outcomes in these specific areas.
Moreover, the behavioral change and mHealth cluster clearly emphasizes the efficacy of integrating gamification into preventive health interventions and public health programs. Policymakers can utilize this knowledge to promote and fund evidence-based mobile health initiatives, such as smoking cessation apps, youth health education programs, and vaccination awareness campaigns, which effectively leverage gamification to encourage long-term behavioral change and public health engagement.
The identification of AI-driven gamification approaches also provides a clear practical pathway for health app developers. Developers are encouraged to incorporate machine learning algorithms, personalized recommendation engines, and real-time adaptive interventions to create more responsive, engaging, and user-centric digital health solutions. Practitioners must simultaneously address ethical considerations around data privacy and transparency of AI-driven algorithms to ensure user trust and sustainable adoption.
Methodologically, this study significantly contributes to bibliometric research by presenting a comprehensive and replicable analytical framework utilizing advanced computational techniques. Specifically, the systematic use of VOSviewer for co-occurrence network visualization, Biblioshiny for thematic modeling, and BiblioMagika® for citation analysis, along with rigorous data cleaning through OpenRefine, ensures methodological transparency and replicability for future research. The analytical approach employed in this study provides clear guidance for future bibliometric investigations in the fields of digital health gamification.
Limitations and Recommendations for Future Research
Although this study provides a comprehensive bibliometric analysis of digital health gamification literature from 2005 to 2025, certain limitations remain and should be considered in future research.
First, this study relies solely on Elsevier’s Scopus database, which, despite its broad coverage in social sciences, computer science, and information sciences, may exclude relevant studies from sources like Web of Science, IEEE Xplore, and ACM Digital Library. Future research should integrate multiple databases for a more comprehensive view of interdisciplinary trends and emerging technical developments.
Second, the bibliometric approach utilized in this study primarily focuses on macro-level analysis, without deeply exploring the underlying mechanisms of specific gamification elements. Although key gamification features such as personalization, adaptive feedback, and social interaction were identified, their exact effects on user experiences and psychological mechanisms were not thoroughly examined. Future research could integrate experimental methods from computer science, such as A/B testing and empirical studies of personalized recommendation algorithms, to validate how specific gamification elements influence health behaviors. Moreover, examining how artificial intelligence-driven personalization impacts long-term behavioral changes could deepen the theoretical and practical contributions of future studies.
Third, although the current study addresses the potential for gamification to sustain long-term user engagement, detailed analysis regarding “gamification fatigue,” or declining user participation over time, remains limited. Future research should incorporate advanced computational methods, such as survival analysis or predictive modeling using user log data, to quantitatively evaluate user engagement trajectories. Additionally, applying deep learning and data mining techniques could support the development of real-time predictive interventions to mitigate user attrition, enhancing the long-term effectiveness of gamified health interventions. In addition, future research should adopt longitudinal designs that track user behavior over a 6 to 12-month period, employing growth-curve modeling and event-history analysis to systematically examine the long-term effects of gamification interventions and potential patterns of fatigue.
Fourth, this study did not fully explore cross-cultural and regional differences in responses to gamification. While the bibliometric analysis covered global trends, the cultural adaptability and effectiveness of gamified strategies across different regions remain insufficiently explored. Given that cultural backgrounds may significantly influence user preferences and acceptance of gamification elements, future research should integrate cross-cultural research methods drawn from information science, such as culturally sensitive user interface (UI) design principles. This approach would offer valuable insights into culturally adaptive gamification strategies, thereby increasing the global applicability and effectiveness of digital health interventions.
Finally, methodological limitations inherent to the analytical tools utilized should be recognized. Although VOSviewer, Biblioshiny, OpenRefine, and BiblioMagika® are commonly employed in information science and computer science fields. Future research could leverage advanced natural language processing techniques, including sentiment analysis, topic sentiment modeling, and semantic network analysis, to reveal deeper latent trends and themes. Integrating these methods would enhance and extend the existing bibliometric framework.
Conclusion
This bibliometric study mapped 618 Scopus-indexed publications (2005–2025) on digital health gamification, examining research trends, contributors, collaborations, and thematic evolution.
The findings have concrete implications. For healthcare providers, gamification can be applied to chronic disease self-management and rehabilitation programs to improve adherence. For developers, the integration of AI-driven personalization and adaptive feedback offers a pathway to reduce user dropout and sustain engagement. For policymakers, the prominence of mobile health and public health applications suggests opportunities to design scalable interventions such as smoking cessation apps or youth health campaigns. Limitations include reliance on Scopus, macro-level focus, and insufficient cross-cultural and longitudinal perspectives. Future studies should integrate multiple databases, employ experimental designs, and investigate cultural adaptability and long-term engagement. Overall, this study underscores gamification’s potential to strengthen healthcare delivery and sustain health behavior change, while emphasizing the need for inclusive design and ethical safeguards.
Footnotes
Acknowledgements
The author sincerely thanks Professor Ahmi from Universiti Utara Malaysia (UUM) for his bibliometric workshop guidance and Universiti Putra Malaysia (UPM) library for its valuable search support.
Ethical Considerations
This study did not involve human participants, human subjects, or identifiable personal data. Therefore, ethical approval from an institutional review board or ethics committee was not required.
Consent to Participate
Informed consent was not required for this study, as no human participants or identifiable personal data were involved.
Author Contributions
Xin Zhang was responsible for Writing – original draft, Writing – review & editing, Conceptualization, Data collection, Data analysis & presentation, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, and Investigation. Qingqing Tang contributed to Data collection, Investigation, Methodology, Validation, Resources, and Visualization. The authors reviewed and agreed to publish.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*