
Abstract
After the implementation of DRG (Diagnosis Related Groups) reform in China, more hospitals are concerned with the soaring cost of healthcare services and the operation efficiency. It is an issue to identify whether the Traditional Chinese Medicine (TCM) hospitals are still competent. This article aims to evaluate the Technical Efficiency (TE) of TCM hospitals in mainland China, excluding the influence of external environmental values and statistical noise. The three-stage data envelopment analysis (DEA) method was used to assess the efficiency of TCM hospitals in China, taking into account inputs including the number of TCM hospitals, licensed doctors, and beds; outputs including outpatient and emergency visits, discharged patients, and bed occupancy rate. The results showed an average TE value of 0.776, and the second-stage Stochastic Frontier Analysis (SFA) regression model indicated a significant effect of selected environmental variables on input slack. After removing these variables and statistical noise, the mean TE efficiency increased to 0.850. To further improve the efficiency of TCM hospitals, hospital managers need to optimize resource allocation based on local level development, labor dependency ratio, population density, and other factors, while the government needs to provide support by implementing supportive policies and increasing financial subsidies.
Plain Language Summary
After the implementation of DRG (Diagnosis Related Groups) reform in China, more hospitals are concerned with the increasing cost of healthcare services and the operation efficiency. It is an issue to identify whether the Traditional Chinese Medicine (TCM) hospitals are still competent. This study aims to evaluate the Technical Efficiency (TE) of Traditional Chinese Medicine (TCM) hospitals in mainland China, excluding the influence of external environmental values and statistical noise. The three-stage data envelopment analysis (DEA) method was used to access the efficiency of TCM hospitals in 31 provinces in China, taking into account inputs such as the number of TCM hospitals, licensed doctors, and beds and outputs including outpatient and emergency visits, discharged patients, and bed occupancy rate. The results showed an average TE value of 0.776, and the second-stage Stochastic Frontier Analysis (SFA) regression model indicated a significant effect of selected environmental variables on input slack. After removing these variables and statistical noise, the average TE efficiency increased to 0.850. To further improve the efficiency of TCM hospitals, hospital managers need to optimize resource allocation based on local level development, labor dependency ratio, population density, and other factors, while the government needs to provide support by implementing supportive policies and increasing financial subsidies.
Keywords
Background
Current Situation About Traditional Chinese Medicine Hospitals
Hospitals, as significant component of the social public service system, have a primary public welfare nature. This is mainly reflected in the responsibility of hospitals to offer basic medical services to the ordinary people, including preventive healthcare, disease diagnosis, treatment, and rehabilitation.
As a kind of healing developed in China more than 2000 years ago, Traditional Chinese Medicine (TCM) has made remarkable contributions to the prosperity of the Chinese nation (Bian et al., 2015). TCM hospitals play an important role in health system. Since 1949, the government has already made the unity of Chinese and Western medicine as one health work and established the proper status and role of TCM. In 1978, Chinese government gave strong support in terms of human, financial and material resources, which strongly promoted the development of TCM. With the continuous healthcare reform, the State Council constructed a perfect policy system for TCM in 2009 to provide a good policy support and legal guarantee for TCM. And also in the past few years, China has carried out the new hygiene system reform. The government has attached great importance to the TCM and to support TCM hospital services. In “Outline of the Strategic Plan on the Development of Traditional Chinese Medicine (2016–2030),” by 2030, all Chinese citizens will have access to TCM services. In March 2022, a new 5-year plan of TCM development has been launched, which shows that the development of TCM is in the period of capacity enhancement and health service expansion.
At the same time, TCM is the main reform content in the healthcare systems. As the reform of the healthcare system is being advanced, TCM has fully utilized its remarkable advantages of clinical efficacy, unique preventive, flexible treatment modalities and relatively low costs, magnifying the beneficial effects of the medical reform and enhancing the connotation of the fundamental healthcare systems with distinct characteristics. TCM has provided a higher proportion of services in comparison to the resources it is entitled to, with a comparatively modest cost. From 2015 to 2021, the medical care services rose from 11.81% to 14.19% in TCM institutions. In 2021, out-patient expenses per visit and in-patient expenses per capita at public TCM hospitals were, respectively, 11.5% and 24% lower than those at general public hospitals.
But new challenges and issues continue to rise in the development of TCM hospitals. That is, public hospitals are facing challenges such as limited financial subsidies, rising labor costs, and pressure to update equipment. Although the number of TCM hospitals is increasing year by year, their medical service efficiency are inefficient, and the development across regions is inequality. Therefore, the research on how to improve the medical service efficiency in TCM hospitals has become “the focus of government and hospital managers” (Hu et al., 2012).
Literature Review
With the increasing prevalence of over treatment, traditional operating models in hospitals are no longer able to satisfy the hygiene demand of the masses. Under such circumstances, the government proposes the DRG payment reform to cope with the systematic cost pressure, and resource shortage. And therefore, the hospital has to grasp the internal and external operation. After that, it could improve service quality, optimize the resource allocation, then to be more competent. In the context, the hospital administration concentrates on the comprehensive operation efficiency.
Current scholars’ research on TCM hospital has focus on two aspects: health resource allocation and efficiency assessment. In terms of “health resources,”Lu and Zeng (2018) used “Moran’s index and the local Moran’s index to comprehensively analyze the spatial distribution and density of beds in TCM hospitals.”Dai et al. (2022) studied “the equity of resource allocation of TCM hospitals among regions by using the Gini coefficient and agglomeration degree”. Furthermore, some studies have used “different models to evaluate the efficiency of TCM hospitals”. Li et al. (2022) applied “DEA-BCC model to measure efficiency and compared the TE of efficient and inefficient hospitals in Gansu province through the use of the Mann-Whitney test.”Yue et al. (2021) used “super-efficiency DEA model and Malmquist to measure changes in the efficiency and productivity of Hubei traditional Chinese medicine hospitals.”Bai et al. (2022) also used “super-efficiency DEA model to measure the efficiency of rural TCM hospitals and found that efficiency was relatively low in rural areas, with significant room for improvement.” It is predicted that public hospitals would be in a critical period of strategic transformation. That is, public policy will force hospitals to shift from extensive operation to lean management, and solve the problem of uneven resources through intelligent and graded diagnosis and treatment.
By reviewing previous literature, there are fewer research on the overall efficiency of TCM hospitals. Much of these research has been limited to specific regions or rural areas, without considering the efficiency in urban hospitals. Moreover, the method does not deliberate the interference of the external environment on the measurement results, leading to poor accuracy. At present, the three-stage DEA model is “widely adopted to evaluate hospital efficiency” (Chen et al., 2020; Hajiagha et al., 2022; Lu et al., 2020; Su et al., 2022; Yang & Zeng, 2014). Therefore, through the above results, this article adopts three-stage DEA model to calculate the TCM hospitals efficiency across mainland China in 2021, and provides suggestions for policymakers to facilitate the rapid development of TCM hospitals. It is not only a deep exploration of improving the efficiency of existing resources, but also a solemn recognition of the continuous optimization of medical service quality.
Methods
Theoretical Model
Hospitals service is a primary public welfare. With the aging population and advances in medical technology, China’s medical expenses have been rising year by year, putting enormous pressure on the medical insurance fund. Hospital operation involves multidimensional inputs such as medical staff, medical equipment, and drugs, while generating diverse outputs, for example, patient satisfaction.
Against the backdrop of current healthcare issues, the reform of DRG (Disease Diagnosis Related Group) payment methods is becoming a key means to improve hospital operational efficiency and medical service quality. As the deepening of healthcare system reform, the medical concept has shifted from “disease centred” to “patient-centred.” The competition among hospitals has also shifted from traditional scale and equipment comparison to soft power competition. How to build and enhance the soft power of hospitals and enhance their competitiveness, becomes an important issue for the high-quality development of public hospitals.
The Data Envelopment Analysis (DEA) model is suitable for evaluating hospital operational efficiency, mainly for the following reasons. The DEA model can comprehensively consider these complex relationships and avoid the one sidedness of traditional methods caused by single indicator evaluation. DEA is a non parametric method. It does not require specific production functions or dimensional conversions to be set in advance, and can directly process raw data. This reduces model setting bias and makes the evaluation results more objective. The DEA model automatically assigns weights to inputs and outputs, adapting to the dynamic adjusts in input-output relationship of the medical industry over time, technological progress, and other factors. For example, the weight of medical equipment investment in different departments may be adjusted due to technological iterations.
DEA model is a nonparametric approach (Charnes et al., 1978). The DEA model enables the determination of the effective Decision-Making Unit (DMUs) by estimating the input and output indicators of the effective production frontier, and it also point out the reasons why the DMU is ineffective, and how to improve the direction through the projection method. In DEA analysis, DMU refers to a set of multiple intervals with the same characteristics, such as enterprises with the same input and output (Zhu & Song, 2022). Considering that environmental factors can affect the efficiency of hospitals in each province, this study uses the three-stage DEA model (Fried et al., 2002) to effectively reduce the influence of environmental variables and random disturbances on the data. The following is a detailed description of the three-stage DEA process:
Stage 1: The Traditional DEA Model
The DEA model encompass both the CCR and BCC models. The technical efficiency of the CCR model may vary in the presence of non-optimal scale operations of the DMUs. However, the BCC model can incorporate it into the measurement. This model is variable returns to scale (VRS), dividing the overall technical efficiency of CCR model into pure technical efficiency and scale efficiency. The healthcare services supply is not linear. And thus, the VRS technical efficiency assumption may be more appropriate (Osei et al., 2005). The BCC model can be divided into input-oriented and output-oriented. As hospitals generally have stronger control over the inputs (Piubello Orsini et al., 2021), this article employs input-oriented BCC model. The formula is expressed as:

Where j=1, 2, …, n and j denotes the sequence number of the DMU, X denotes input variables and Y denotes output variables. If θ = 1 and S+ = S− = 0, the DMU is considered efficient. If θ less than 1, it is inefficiency.
Stage 2: SFA Model
The first stage DEA model was used to measure the efficiency values without removing management inefficiencies, environmental influences and random effects. To get more accurate efficiency, we considered the environmental variables as the explanatory variables and the slacks of inputs obtained from first stage as dependent variables (Zhou et al., 2024). Then build the following SFA regression model.

Where Sni denotes the n-th inputs slacks of the i-th DMU. Zi represents an environmental variable, βn is the coefficient of the environmental variable, vni + µni is composed error term, vni is statistical noise and µni reflects managerial inefficiency.
The formula for separating statistical noise and management inefficiency is below (Dengyue, 2012):

Where
The random errors are:

SFA regression could eliminate the influence of environmental variable and random factors, so as to maintain all DMUs to the same external environment. The adjusted inputs formula is below.
Where
Stage 3: Adjusted DEA Model
Based on the input-oriented BCC model, the adjusted input variables are used to measure each DMU efficiency again. At this time, the efficiency has eliminated the influence of environmental variables and random factors, which is relatively realistic.
Data and Variables
The competitiveness of hospitals can indeed be divided into two categories: hard power and soft power. The hard power mainly includes tangible resources such as medical equipment and medical infrastructure. For example: High end medical equipment; Advanced diagnostic and treatment technologies (minimally invasive treatment, remote medical support). The soft power covers intangible elements such as management, operation culture, etc. For example: Performance Management System, Multidisciplinary Collaboration Mechanism.
Hard power is the foundation, while soft power is the core driving force. However, the specific classification needs to be analyzed in conjunction with different dimensions. There are differences in the focus of soft power construction among hospitals at different levels (such as primary, specialized, and comprehensive). For example, primary hospitals place more emphasis on “nursing + equipment upgrading,” while specialized hospitals focus on “technological iteration + talent echelon pool.”
The DRG reform in China is being promoted in stages. In 2018, the National Healthcare Security Administration was established. The first batch of pilot projects were launched in 2019. The country released version 1.0 of the technical specifications and grouping system in 2020. Considering the issue of data availability, this study took the TCM hospitals in mainland China in 2021 as the research subjects. As result of differing statistical systems, data from Taiwan, Hong Kong and Macau are not on the list. The data is sourced from the “China Health Statistics Yearbook 2021” and “China City Statistical Yearbook 2021,” published by National Health Commission of China, which is credible and accurate.
How to select objective and valid variables is a key step in DEA. The fundamental principle is that the data needs to be comparable and available. And the total number of evaluation variables should be less than half of the number of DMUs. Review of previous research have found that “a high number of beds is one of the major causes of hospital inefficiency as it increases overhead costs” (Rebba & Rizzi, 2001). Aloh et al. (2020) found that bed occupancy rate can be an important indicator for evaluating hospital efficiency. So we use “the number of beds,”“the number of licensed doctors and the number of TCM hospitals” as input variables. “The number of outpatient and emergency visits, the number of discharged patients and bed occupancy rate” are used to be the output variables. Otherwise, The three-stage DEA needs to “meet the requirements of separability assumption for environmental variables” (Simar & Wilson, 2005), so it is necessary to select environmental indicators that have an impact on hospital operation efficiency but are not subject to subjective control and modification. Through literatures (; Afonso et al., 2025; Feng et al., 2023; Flokou et al., 2017; Kiadaliri et al., 2013; Lai et al., 2017; Tsakas & Katharaki, 2021; Zheng et al., 2018) and data availability, this study finally selects urban population density, gross regional production, dependency ratio, case fatality rate and government subsidy as the environmental variable. The above variables are defined in Table 1.
Definition of Input, Output and Environmental Variables

To eliminate the influence of numerical values among various environmental variables and reduce the differences between them, so as to obtain more accurate analysis results, all environmental variables are normalized, and the processing formula is below.

Where
Results
The descriptive statistics for the input, output and environmental variables are shown in Table 2. The substantial standard deviations observed in “the number of beds and doctors” indicate that a marked discrepancy in the distribution of medical resources. And there is also a large fluctuation in outputs and environmental variables across different regions. For example, the number of discharged patients varies from 57,889 to 2,452,177 and the gross regional product varies between 334.30 and 110,760.94.
Descriptive Statistics of the Inputs, Outputs, and Environmental Variables.

Abbreviation: SD, standard deviation.
Three-Stage Analysis
Stage 1: applying the DEA-BCC model to evaluate the efficiency/
The DEA analysis results of the first stage are presented in Table 3. According to Mohammad’s view (Mohammad et al., 2014), we regard TE values of 0 to 0.8 as inefficient, 0.8 to 1.0 as less effective and 1.0 as efficient. In Table 3, 48% of provinces have TE values above 0.8, and the average TE of TCM hospitals of 31 provinces are 0.776. The efficiency of Shanghai, Hainan province and Tibet are 1.0 while the TE of Shanxi, Liaoning, Jilin, Heilongjiang province, and Inner Mongolia is relatively low, around 0.5. It indicates that the TE of TCM hospitals in mainland China varies greatly among provinces.
DEA Efficiency Evaluation Results of TCM Hospitals in 2021.

In terms of PTE, it represents managerial efficiency (Yusefzadeh et al., 2013), and Chen defined it as the additional consumption of the input resources for a specified output due to the operational management (Chan & Karim, 2011). In the DEA model, “Pure Technical Efficiency equal = 1” indicates that the DMU has reached the optimal state of resource utilization under the current technological level. So as shown in Table 3, PTE values of 11 provinces is 1.0 which indicates that the input and output resource efficiency of TCM hospitals in these provinces are relatively balanced, and the factor limiting its development under the current investment level is the scale of the hospital. Besides, 7 provinces are inefficient, which means TCM hospitals in such provinces have redundant input or insufficient output. The average PTE of these provinces is 0.864. And 13 (42%) provinces are below it, indicating that there is still much space for improving existing resource inputs and outputs of Traditional Chinese Medicine hospital.
According to SE and RTS, it finds that the mean SE score is 0.905. 24(77%) provinces reach a diminishing RTS. They should be improved by reducing the size of hospitals and improving the efficiency of resource utilization. 1(3%) provinces have increasing RTS and their efficiency can be improved by expanding the scale of hospital input.
Stage 2: Analysis of Environmental Variables and Adjustment of Input Variables Based on SFA Regression
At this stage, we perform SFA regression analysis with the slacks of the inputs as independent variables and the environmental variables as explanatory variables. When the regression coefficient is positive, the increase of environmental variables would result in the increase of the corresponding input slack values. Then, the more the original input deviates from the input target value, making the hospital less efficient. Conversely, when the regression coefficient is negative, increasing environmental variables would reduce the input variable slack values improve the Operational efficiency of hospitals.The results are below in Table 4.
Stochastic Frontier Estimation Results.

, **, *** denote statistical levels significance at 10%, 5%, and 1%, respectively.
Table 4 shows that the LR text of the one-sided error is under 5% level, which is statistically significant. And the γ values for all input slack variables are 1, which indicates that the external environment and management noise dominates the input slack variables rather than random error. So it’s necessary to separate managerial inefficiency and statistical noise. The effects of five environment variables are shown below.
The coefficients of the urban population density are negative for the all input slack variables which suggests that the higher the population density of a region, the less wasted healthcare resources are invested. And thus it is a main environmental factor.
For gross regional product, it has a significant positive correlation with each input slack variable, indicating that with the increase of gross regional product, hospitals may expand blindly, resulting in the waste of beds and doctors and. This is also reflected in some areas of the country where the economy is well developed, but resources are not rationally allocated, leading to lower efficiency of hospital.
For the dependency ratio, the regression coefficients of this environmental variable is negative for “the number of licensed doctors,” but positive for “the number of beds,” which indicates that the rise of dependency ratio means that China has entered an aging society. The retired elderly will increase healthcare utilization (Zhang et al., 2018). Through doctors will be recruited a lot, there will be more inpatients, which will run on medical resources crashed and making hospitals less efficient.
For the case fatality rate, the coefficients of it are positive for all input slack variables, indicating that a high case fatality rate means an increase in deaths, thus prolonging total length of hospital stay, leading to a shortage of hospital beds and doctors, which negatively promotes the operation efficiency of health and medical institutions.
For the government subsidy, the coefficients of it are negative for all input slack variables, indicating that government subsidy affects on the three input redundancies. When government subsidy increases, it would result in input redundancies in TCM hospital, beds and licensed doctors.
Stage 3: Analysis of Adjusted Inputs Based on the BCC Model
The adjusted value of input variables are adopted to measure the overall efficiency by BCC model again. At this stage, the overall efficiency has removed the interference of exterior environmental values and statistical noise, so it is relatively accurate. The results are in Table 5.
The Results of DEA Efficiency After Adjustment.
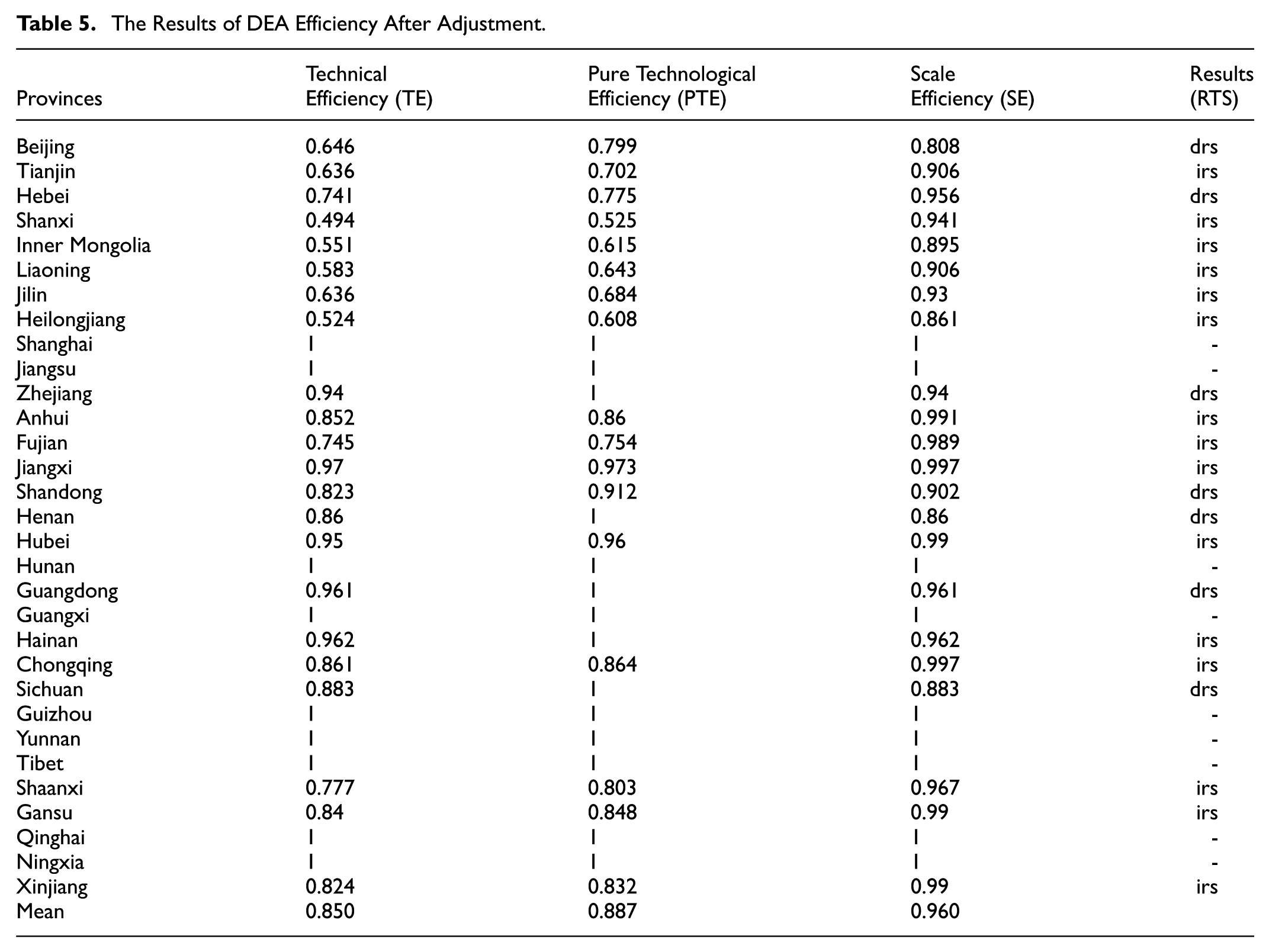
In Table 5, the TE of TCM hospital efficiency of 31 provinces in mainland China changes from 0.776 in stage 1 to 0.850 in stage 3, the PTE changes from 0.864 to 0.887, and the SE changes from 0.905 to 0.960. This indicates the PTE and the SE of the TCM hospital is underestimated in the first stage because of the influence of environmental factors. Besides, The TE value of some Chinese provinces remained almost unchanged, which further shows that TCM health and medical institutions in China should shift their emphasis from scale expansion to hospital management.
Regional Comparison of TCM Hospitals Efficiency
There is an efficiency difference of TCM hospitals in each province of China. Therefore, according to the traditional way of division, based on the economic development and geographical location of the continental region, the Chinese continental region is grouped into three economic regions: “the eastern region,”“the central region,” and “the western region.”Table 6 shows the efficiency values for the different regions.
The Efficiency of Eastern, Central and Western Regions.
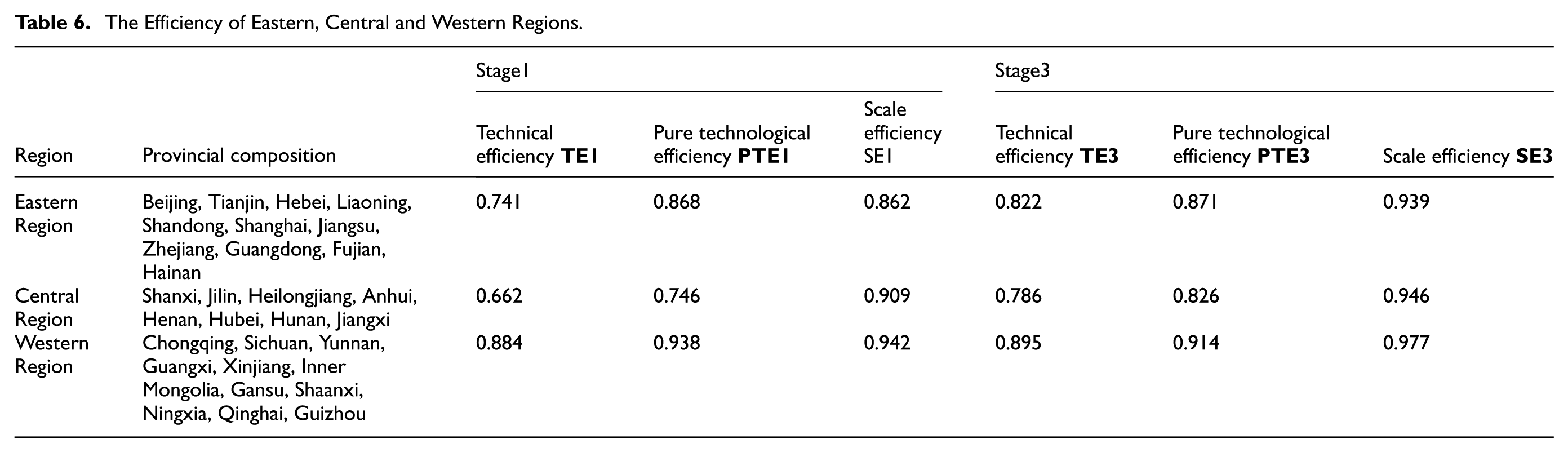
Both in the first and third stages, the western region has the highest efficiency. Eastern region and central region follow the western. It is clear that the efficiency of TCM hospitals in the eastern lags behind that of the western mainly due to the lower efficiency of Liaoning, Beijing, Tianjin, Hebei and Shandong provinces. The coastal region in Southeast China is economically developed and has many prestigious TCM universities, which provide favorable external conditions for training talented person. Moreover, the coastal region has more international contacts, and managers are able to learn advanced management skills and apply them to practice in order to improve TCM hospitals efficiency. On the other hand, Liaoning and other provinces, which belong to the northern region, have been plagued by industrial restructuring and upgrading in recent years, resulting in stagnant economic development, a serious loss of young workforce and a shortage of good medical staff in hospitals. These have led to a lower TE value in eastern as a whole than in western. Although the western region is not as economically developed as the eastern region, traditional Chinese medical theory first originated in the western region, where there is abundant knowledge and better practice techniques. Relying on the local traditional culture in the west, TCM has been developed better, leading to the highest efficiency of TCM hospitals in the western region.
Discussions
There are Regional Differences in Hospital Operational Efficiency
As a service provider of traditional Chinese medicine, TCM hospitals have been paid more attention by the Chinese government, and evaluating their efficiency is of increasing relevance. This is due to “the government departments and hospital managers can make policy and optimize management through objective efficiency evaluation” (Niu et al., 2021). However, the traditional DEA model does not effectively control or eliminate environmental variables and statistical noise, thus failing to provide objective efficiency evaluations. To address this issue, this study utilizes the three-stage DEA method to improve the accuracy of efficiency evaluations by reducing the impact of external environmental values and statistical noise. Although the eastern region is economically developed, hospitals may face more challenges in management and operation due to factors such as abundant medical resources, fierce competition, and diverse patient needs, which may affect overall efficiency. The central region is located in the transitional zone between the east and the west, with a relatively balanced level of development and allocation of healthcare resources. However, there may also be some limiting factors, such as talent loss and insufficient funding investment, resulting in relatively low overall efficiency.
Through a comparative analysis of hospital efficiency in 31 Chinese provinces in 2021, only 9 are effective after considering environmental variables, of which 5 DMUs (67%) were located in the western part of China. Compared to the other two regions, the western region also has the highest average value of TCM hospitals efficiency. This is mainly because the theory of TCM was formed in the west, which has a wealth of knowledge and advanced practical techniques. On the other hand, the eastern coastal areas are more developed economies and are more exposed to the western medicine, while TCM is more reliant on local cultural traditions and thus faces greater difficulties in establishing a successful industry without a large market under western influence. So there are obvious differences in efficiency among provinces, and the efficiency of TCM hospitals in inland areas is higher than that in eastern coastal areas. In line with Gong et al. (2019) and He et al. (2021), the efficiency of TCM hospitals in all provinces is the same as that of general hospitals, and there is an uneven allocation of health resources between regions. Compared to the mean TE scores for all china public hospitals (0.776) (Chen et al., 2020), the TE scores of TCM hospitals in the first stage is only 0.834. It is because the PTE is low, which indicates that there is still massive waste and inefficient hospital management in TCM hospitals (Hajiagha et al., 2022). Hospitals need to attract top specialized talents to guide them and improve their management methods.
The Improvement of Hospital Operation Efficiency can be Achieved Through the Development of Technology
Research shows that after adjustment, the comprehensive efficiency and PTE of most provincial (regional, municipal) hospitals have been improved. It indicates that the operational efficiency has been improved after removing external environment and random interference. From the dynamic analysis results, there are 31 provinces (regions, cities) in China with a focus on technology, the region with the lowest index is 0.786, while the rest values are greater. This is an important reason for the high change index of total factor productivity in hospitals.
The application of modern information technology in medical management has significantly improved the management efficiency of hospitals. Through various information systems, rapid transmission and sharing of medical information, it can realize the target of optimizing medical processes, reducing human errors, and improving work efficiency. At the same time, big data is divided into the application of technologies such as analysis and artificial intelligence can also help hospitals better allocate resources, control costs, and manage quality. Hospitals adopting more advanced medical technologies, management methods, or service models can significantly improve the efficiency, thereby promoting the overall development of healthcare.
When hospitals make progress in technological development, it often prompts them to optimize and improve management, resource allocation, and other aspects. And therefore, measures such as investing in medical technology research and development, supporting hospitals in introducing and applying new technologies, and strengthening the training of medical and health talents can promote the improvement of hospital technology level and total factor productivity.
The Scale Efficiency of Hospitals Should be Significantly Considered
Besides, the scale efficiency of TCM hospitals is required to be improved. Only 6 DMUs (19.35%) in the first stage were in optimal scale, the remaining most of DMUs have decreasing RTS, indicating that these hospitals need to reduce excess input to improve their scale efficiency. After excluding environmental factors and random errors in stage 2, the SE scores of TCM hospitals in some provinces decreased, suggesting that external economic factors and population size may have made the SE of TCM hospitals overestimated.
The operational efficiency in different regions varies significantly. The problems of uncoordinated and unbalanced development are more prominent. It is necessary to continue to strengthen the allocation of health resources for TCM hospitals in the region, coordinate the progress of operational efficiency and development level, and continuously optimize the management level of TCM hospitals.
In addition, the SFA regression results indicate that all the environmental variables have an impact on input slack. Urban population density is positive for the input slack variables. Because the increase in population density will aggravate the competition among hospitals to improve their competitive advantage. An increase in the dependency ratio and case fatality rate can reduce hospital efficiency. Since China has already entered an aging society, people are seeking medical care more frequently, resulting in a shortage of beds and staff.
The Cultivation of Traditional Chinese Medicine Professionals Could Improve the Technical Efficiency of TCM Hospitals
With the continuous promotion of TCM in recent years, the documents issued by the government have also provided a lot of policy support. Over the years, the improvement in operational efficiency of TCM hospitals has mainly been driven by their technological progress. As a concentrated manifestation of China’s traditional Chinese medicine industry, the development of TCM hospitals cannot do without the supply of talent resources. Only by continuously adding talents to TCM hospitals, and improving the service level and technical efficiency in terms of manpower, can the operational efficiency of hospitals be enhanced. The government should increase its emphasis on the cultivation and employment of traditional Chinese medicine talents, and strive to cultivate a new generation of traditional Chinese medicine talents. It should pay attention to the cultivation of practical talents in primary traditional Chinese medicine. At the same time, it should promote educational reform and continuously improve the training mode of traditional Chinese medicine talents. For example, establish a standardized training system for traditional Chinese medicine physicians and a training mechanism for general practitioners and rural doctors on traditional Chinese medicine knowledge. Apply more updated technologies to the field of traditional Chinese medicine.
Conclusions and Limitations
Conclusions
In this study, a three-stage DEA model is applied to quantitatively evaluate the efficiency of TCM hospitals in mainland China. The following conclusions are drawn.
In the first and third stage, it indicates that the efficiency of Chinese hospitals is influenced by the external environment variables and random error. Furthermore, after removing them, the TE scores for TCM hospitals have increased. In the second stage, the most environmental variables coefficients are significant at a 99% confidence interval, indicating that the selected environmental variables have an impact on the efficiency of the TCM hospital. Therefore, the consideration of external factors is imperative in order to enhance the efficiency of the hospitals.
There are significant regional differences in the efficiency. The TE value of western region surpasses that of central and eastern regions, which means there is substantial potential for the development of TCM hospitals.
Policy Recommendation
The recommendations have been proposed to theoretically guide the provinces in improving the efficiency of hospitals:
(1) The efficiency of TCM hospital is affected by internal and external factors.
For those undeveloped areas, the scale of hospital construction should be carefully considered. It is closely tied to the local economic development level, the number of residents, the labor dependency ratio and other factors. Therefore, if TCM hospitals want to achieve success in the competition with Western medicine in the medical market, they should analyze the external environment and local policies, and then formulate a development plan and optimize the allocation of factors according to the local situation of the hospital in order to maximize the utilization of factors.
(2) It is important to enhance inter-regional communication and implement differentiated hospital competition strategies.
The stark disparities of TCM hospitals efficiency across regions highlights the need for hospitals to exchange talents and technologies and to adopt differentiated methods for treating diseases based on local conditions. The eastern region can learn from the successful experiences of the western region, cultivate TCM culture, and improve the efficiency of hospitals. Meanwhile, the government in the high-efficiency western region should continue to support the development of TCM through a series of policies and subsidies.
(3) The traditional Chinese medicine hospital has unique advantages. The government should promote the sustainable development of TCM hospitals.
It is necessary to explore new paths to make good use of the TCM advantages in China for its future development. Due to the unique TCM characteristics, its income level is relatively low. Moreover, according to the national statistics of TCM in recent years, its investment level is limited. Traditional Chinese medicine has its own unique advantages in health care, and rehabilitation. It should fully leverage the characteristics of TCM, innovate development models, and promote the development of TCM hospitals. The government should promote the integration of traditional Chinese medicine guarantee models, integrate various health management and health services projects, spur innovation in the operation mode of TCM hospitals. In that case, it could meet the health service demands from the general people.
Limitations
However, due to the availability of data, it is not possible to obtain more detailed environmental variables (such as financial aids for traditional Chinese medicine hospitals), and relevant indicators such as cure rate, patient satisfaction, proportion of TCM characteristic services have not been included in the model for consideration, which may result in some deviation between the final results and the real situation. In the future, we will consider more suitable indicators from a more objective perspective, study more accurate efficiency values, analyze the factors affecting the TCM hospitals operational efficiency, and provide theoretical basis for improving their operational efficiency and promote the overall development of TCM hospitals.
Footnotes
Consent to Participate
There are no human participants in this article and informed consent is not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank National Social Science Fund of China (23&ZD037, 22BTQ063), Zhejiang department of education (Y202351863) and the suggestions from Jiqiang HU from Zhejiang Conba Pharmaceutical Co., Ltd. Yinyan HE from Zhejiang Huabett Pharmaceutical Co., Ltd.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The Data are available on request from the authors.