
Abstract
Around the globe, the implementation of artificial intelligence (AI) has gained momentum across all settings. Likewise, AI implementation in healthcare settings has transformed processes and working efficiency; however, its impact on doctors’ psychological wellbeing (DPWB) remains insufficiently examined and understood in the extant literature. Accordingly, this study examines the influence of AI implementation on DPWB through technological awareness (TA) as a mediating factor, drawing on the social cognitive theory (SCT) perspective. Furthermore, a sample of 415 doctors was employed as key respondents within private sector hospitals to collect quantitative data. For data analysis, PLS-SEM was employed. According to the results, AI implementation significantly enhances DPWB while TA mediates this relationship. Hence, this study enriches the AI and wellbeing literature related to the healthcare setting by providing valuable insights to healthcare practitioners about how AI implementation improves DPWB in the presence of TA. This study also offers policy implications and direction for future researchers on AI implementation and DPWB.
Plain Language Summary
This study investigated the impact of AI implementation on doctors’ psychological wellbeing in the presence of technological awareness as a mediator. Based on the collected data from 415 doctors working in private hospitals. Findings indicate that AI implementation significantly impacts doctors’ psychological well-being. Furthermore, technological awareness mediates the link between artificial intelligence implementation and doctors’ psychological wellbeing. Additionally, this study provides insight into social cognitive theory from the cognitive, environmental, and behavioral perspectives and offers policy implications for healthcare practitioners.
Keywords
Introduction
Artificial Intelligence (AI) has garnered considerable attention in the era of emerging technologies from various stakeholders, including public and private sector organizations, investors, researchers, and the public. This attention has sparked global interest, specifically in healthcare settings, due to the rapid integration of AI leading to improved processes and procedures. For instance, during and after the COVID-19 crisis, studies conducted in healthcare settings revealed that 64.8% of doctors had accepted AI as an effective tool, resulting in improved wellbeing and satisfaction levels as compared to those doctors with less acceptability toward AI (Dongre et al., 2024; Hussain et al., 2024).
Accordingly, studies have been undertaken, and scholars have reported their findings about the impact of AI implementation on organizational and employee-related outcomes. For instance, existing studies indicate that AI implementation contributes to improving data handling and management, decision making, and service delivery (Bajwa et al., 2021; Davenport & Kalakota, 2019). Hence, these improvements are linked with reduced burnout along with enhanced emotional and psychological wellbeing due to efficient allocation of organizational resources (Curry, 2024; Gupta et al., 2023; Naveed, 2023; Stovall, 2023).
Additionally, it has been linked to increased organizational performance and creativity (Mikalef & Gupta, 2021; Olan et al., 2022), as well as enhanced employee performance and behavior, as set forth by Ramachandran et al. (2022) and Robert et al. (2021). However, despite the positive outcomes, the results remain fragmented and inconclusive on how AI implementation affects doctors’ psychological wellbeing (DPWB). Thus, this gap highlights the need for further investigation and deliberation across diverse cultural and organizational settings (Anitha & Shanthi, 2020; Rana & Singh, 2023).
Developing countries like Pakistan have begun to adopt AI technology despite facing several challenges that influence both organizational operations and the wellbeing of the healthcare professionals (Channa, 2023). One of the major challenges in this regard is developing and fostering readiness, as well as building confidence among doctors to adopt and utilize AI technologies effectively. A lack of technological awareness (TA) can influence the link between AI implementation and DPWB (CapeStart, 2024; Khan et al., 2023; Vonage, 2022) either positively or negatively due to insufficient knowledge and the presence of a relevant skill set (Barbazzeni et al., 2021; Chowdhury et al., 2023; Erin, 2024).
Besides, aligning with the abovementioned perspective, the provision of TA can enhance understanding, experience, and engagement of the users with the implemented AI systems and processes (Alsadoun et al., 2023; Barbazzeni et al., 2021; Flavián et al., 2022; Powe et al., 1996). As a result, improved TA can contribute to better emotional, social, and PWB of healthcare professionals (Gupta et al., 2023; Hill et al., 2024; Kulkov et al., 2023). This is possible by increased preparedness and awareness about the implemented technology (Ahmed et al., 2022). However, limited significance has been given to examining the intersection of AI and DPWB in the presence of TA as a mediating factor within the context of Pakistani healthcare settings.
In addition, grounded on social cognitive theory (SCT), the integration of AI, TA, and DPWB has remained an underexplored dimension in literature. Therefore, in response to the call by prior researchers, it is necessary to see the influence of AI implementation on DPWB using SCT as a theoretical framework (Wood & Bandura, 1989). Therefore, this study offers a significant extension of SCT by incorporating cognitive, environmental, and behavioral outcomes in a technologically evolving healthcare setting.
Building on prior deliberations, our study makes subsequent contributions to current AI and well-being literature. First, the effect of AI implementation on DPWB is examined. Secondly, TA is examined as a mediating factor between AI implementation and the DPWB relationship. Third, our study advances the existing AI implementation and wellbeing literature by applying SCT as a foundational theoretical framework, including cognitive, environmental, and behavioral outcome mechanisms for healthcare psychology in a tech-driven environment within the Pakistani healthcare setting. Lastly, building on the arguments presented earlier, this study focuses on exploring the underlying mechanisms that shape these relationships among doctors working in hospitals.
Theoretical Underpinning
Social Cognitive Theory (SCT)
According to SCT, an individual faces and responds to the adversity and environmental changes by adapting and transforming their behavior (Wood & Bandura, 1989). This adaptation process is facilitated by an intact cognitive process and the presence of a social environment that enables individuals to learn and manage the implemented change, thereby exhibiting the desired behavior (Schunk & Usher, 2019). As a result, such behavioral adaptations can influence employee productivity (Wang et al., 2019) and wellbeing (Bandura, 2011). Furthermore, SCT emphasizes the role of observational learning, asserting that individuals often acquire and exhibit desired behaviors by observing the behavioral aspects of others. In the same vein, Bandura (1986) elaborated that learning about digital technologies is reliant upon social interaction, modeling, and observation.
Consequently, in the realm of digital technologies, cognitive and emotional experiences can be enhanced through creating awareness and social interaction, as well as engagement (Schneider et al., 2022). Accordingly, the notion of TA has gained prominence during the adoption of AI. TA encompasses the process of enhancing understanding and knowledge about the implementation of AI. Without awareness, PWB and emotions may be negatively influenced (Tao et al., 2024). However, limited studies exist related to the intersection of AI, TA, and doctors’ PWB from the perspective of SCT (Tao et al., 2024).
Drawing on Bandura’s (2001) SCT framework, TA can be conceptualized as a cognitive (personal) factor that enables doctors to understand, interpret, and respond to technological changes effectively. Likewise, cognitive orientation is critical for timely awareness and adaptation to environmental (technological) development and changes (Middleton et al., 2019; Wu et al., 2021). Besides, being aware of emerging technologies within healthcare settings requires cognitive capacity among doctors, which in turn enhances working efficiency and wellbeing (Huo et al., 2025). However, AI implementation is only feasible when both TA and adaptation are achieved, thereby fulfilling both organizational and psychological needs of professionals.
Furthermore, AI implementation in this study is viewed as an environmental factor, another imperative facet of SCT. AI implementation in today’s organizations is a crucial need to transform the organizational processes and practices, rather than having conventional methods (Bandura, 2001). According to Bandura’s SCT, an individuals who possess a substantial belief and abilities in their capability to employ and execute technology is more likely to perceive AI implementation as an opportunity for growth, leading to improved wellbeing rather than viewing it as a source of stress and anxiety (Naiseh et al., 2025).
Traditionally, SCT has been applied to behavioral change and learning; this study expands its application by framing DPWB as a behavioral outcome influenced by cognitive (personal) and environmental factors. Behavioral outcomes such as PWB may be either positively or negatively shaped by AI implementation (Anitha & Shanthi, 2020). Moreover, TA serves as a mechanisms that aid in AI adaptation, leading to reduced stress and enhancing PWB (Bandura, 2011; Chin & Mansori, 2018; Hui et al., 2024; Lent & Brown, 2008). Thus, SCT emphasizes the significance of behavioral change through observation and reciprocal determinism. TA can foster positive perceptions and confidence among users about AI tools and technologies, ultimately supporting the psychological wellbeing (PWB; Alanezi, 2024).
Guided by SCT, this study proposes that doctors with a higher level of efficacy, achieved through the cognitive factor of TA, are better positioned to adapt to AI implementation (an environmental factor) and thereby enhance PWB (behavioral) outcome. However, the empirical evidence regarding the intersection of AI, TA, and DPWB is missing in the literature, which needs to be assessed through the lens of SCT. Henceforth, this study focuses on extending the theoretical as well as practical relevance of SCT by applying it to a tech-driven healthcare environment, specifically focusing on doctors within Pakistani hospitals.
Literature Review
Artificial Intelligence (AI)
The concept of AI has been explained in several ways in the literature, offering various conceptualizations. For instance, a few researchers view it as a capability (Chowdhury et al., 2023), while others consider it as digital agency (Ågerfalk, 2020), a manifestation of technological change (Shi et al., 2020), and a systematic interdisciplinary category that is being applied across diverse sectors and settings (Palanca-Castan et al., 2021; Pan & Froese, 2023). Still, the explanation related to AI remains elusive in the literature. Besides, the AI implementation has gained prominence in the organizational context (Wirtz et al., 2019). AI notion is broken down into two foundational components for better understanding. The term “artificial” refers to an idea created by humans, reflecting the imitation of natural phenomena (Walter, 2008). In contrast, intelligence refers to the capacity to learn, interact, retrieve, and adapt information from experiences to deal with uncertainty (Legg & Hutter, 2007).
Hence, AI is a form of non-human intelligence designed to execute duties and fulfill responsibilities using technology (Owsianka, 2023) but lacking cognitive functions. However, AI is a crucial environmental factor within the workplace, enabling employees to complete tasks more efficiently and effectively (Paluch & Wittkop, 2023). Grounded in the two core concepts, Table 1 presents a summary of AI elaboration conceptualized by various authors across the literature.
AI Elaborations.

Psychological Wellbeing
In literature, the concept of wellbeing has been explained in a broader context. Few researchers linked wellbeing as an individual valued experience to perform work-related responsibilities effectively (Huang et al., 2016; Locke, 1987). On the other hand, researchers view it as a person’s subjective assessment of happiness, satisfaction, and the ability to accomplish the task (Diener, 2009). Others view it from hedonic (cognitive and affective) and eudaimonic (happiness and potential) perspectives (Ballesteros-Leiva et al., 2017). Moreover, researchers have conceptualized wellbeing through complementary approaches, including subjective experiences, physical and mental well-being, and relationships, as a key dimension to understand and explain overall wellbeing (Pagán-Castaño et al., 2020).
Accordingly, subjective experience refers to a sense of fulfillment and pleasure; physical and mental wellbeing refers to physiological and psychological health, and social wellbeing refers to the relationship with others (Li et al., 2024). Furthermore, few scholars have conceptualized wellbeing from a diverse set of perspectives, including social, physical, and psychological aspects (Grant et al., 2007). Therefore, PWB refers to the utilization of mental (psychological) resources and the capability to cope with changes in a more optimistic manner (Obrenovic et al., 2020). It involves the human capacity to have a purpose in life (Diener et al., 2009). Accordingly, PWB is explained in this study as a process of achieving satisfaction and value in accomplishing work and life tasks. Building on SCT, DPWB can be treated as a behavioral outcome influenced by cognitive (personal) and environmental factors (Anitha & Shanthi, 2020).
Hypothesis Development
Artificial Intelligence Implementation and Psychological Well-Being
Referring to AI implementation, technological advancements have significantly influenced working patterns, life activities, and wellbeing from psychological and social perspectives (Feijóo et al., 2020). Moreover, in the era of cutthroat competition in AI and digitalization, the PWB has gained attention among practitioners and researchers, especially within the healthcare setting (Alowais et al., 2023; Elsawy, 2024). To sustain wellbeing, upskilling alongside reskilling is an essential training aspect to equip and develop individuals with the relevant skills in order to manage AI implementation (Cramarenco et al., 2023). An overview of the existing studies is presented in Table 2 related to AI implementation and wellbeing within healthcare settings.
AI Implementation and Wellbeing.
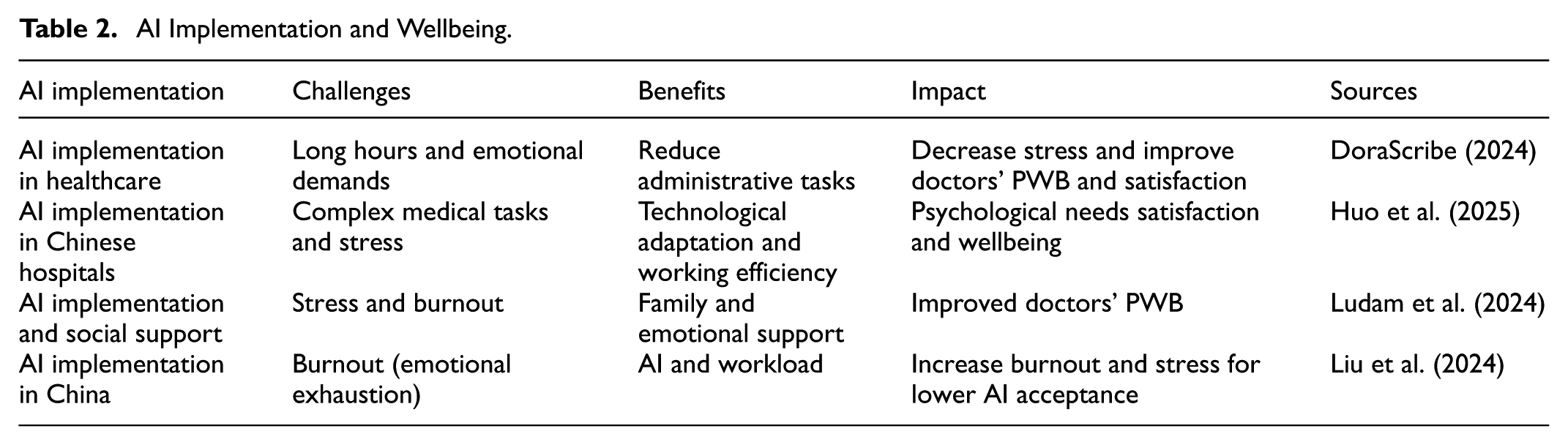
Drawing on SCT, AI implementation is viewed as an environmental factor that has begun to transform organizational processes (Bandura, 2001). This means that the transformation of organizational processes can positively shape individuals’ perceptions. Hence, individuals are likely to perceive AI implementation as an opportunity that can contribute to their wellbeing (Naiseh et al., 2025). Thus, AI implementation in this study is explained as a way of utilizing AI tools in hospitals to deliver services effectively. Based on the abovementioned Table 2, mixed findings exist about AI implementation and DPWB. In addition to this, several studies have found that AI has a negative influence on wellbeing (Gull, Ashfaq, & Aslam, 2023; Zhao et al., 2024). Conversely, AI can be a potential factor that brings a positive change in PWB (Proactive, 2023). In contrast, Giuntella et al. (2023) found that AI does not influence PWB. Consequently, the link between AI and PWB, particularly among doctors, remains inconclusive and warrants further exploration, as recommended by Rana and Singh (2023). Therefore, the subsequent hypothesis was put forth.
Technological Awareness as a Mediator
The notion of TA refers to a process in order to acquire the knowledge and skill set to manage and implement technology in an effective manner (Santana & Díaz-Fernández, 2023). On the other side, TA encompasses a self-assessed competency to understand the knowledge and skills level required for AI implementation (Scantamburlo et al., 2025). These abilities can be enhanced by employing techniques, including upskilling and reskilling, with a focus on developing the competency, which in turn creates awareness and builds confidence about the utilization of AI tools (e.g., robots and algorithms), leading to improved working efficiency and PWB (Brougham & Haar, 2018).
Furthermore, awareness enables an individual to manage change by acquiring knowledge about the effectiveness of AI implementation. This, in turn, mitigates the negative perception among key users (Pillai & Sivathanu, 2020), as well as enhances fairness and transparency (Pant et al., 2024), contributes to generating positive societal outcomes (Forsyth et al., 2021), along with improving service delivery (Brougham & Haar, 2018; Yudiatmaja et al., 2021) and wellbeing (Oosthuizen, 2019). However, a lack of awareness can negatively influence working behavior (Ahmad et al., 2024) and also impede the process of AI implementation (Pant et al., 2024).
There are three primary aspects aligned with TA during AI implementation. First, AI is a machine that mimics human intelligence to carry out various operations, such as problem-solving, understanding complex mechanisms, and completing the decision-making process effectively (Shahzad et al., 2023). While TA needs to be implemented effectively before the implementation of technological (AI) solutions. Second, once awareness is created, the process of AI implementation can be streamlined, which in turn enhances operations, performance, environmental planning, and resource efficiency (Li et al., 2023; Thadeshwar et al., 2020; Waltersmann et al., 2021; Yu et al., 2021). Third, TA enhances human understanding and readiness to accept technological change. As a result, barriers can be managed effectively during AI implementation (Alam et al., 2020; Flavián et al., 2022). In contrast, a lack of awareness and inadequate knowledge about the use of AI may negatively impact PWB (Brougham & Haar, 2018; Gupta et al., 2023). Henceforth, TA can be a facilitating factor between AI implementation and DPWB. However, the limited studies on the link between TA, AI implementation, and DPWB have been reported as presented in Table 3.
Studies Related to TA, AI, and DPWB.

Consequently, individuals must exert both cognitive and physical efforts to become fully aware of technological changes. This can lessen the detrimental impact on PWB (Amichai-Hamburger, 2009; Zahoor et al., 2022). This process is further facilitated when organizations actively promote TA with emerging technologies. This contributes to enhancing PWB, attitude, and trustworthiness (Johnson et al., 2020; Nadarzynski et al., 2019). This shows that TA enables AI implementation, and henceforth, PWB can be affected (Shahzad et al., 2023; Zahoor et al., 2022).
Drawing on Bandura’s (2001) SCT, TA is viewed as a cognitive (personal) factor that enables doctors to effectively cope with technological change, resulting in reducing frustration and improving wellbeing (Huo et al., 2025). In this study, TA is delineated as a process of inculcating knowledge and developing skills among doctors for the implementation of AI. Hence, TA is positioned as a mediator between AI and DPWB. However, there are limited studies on this relationship. Therefore, based on the above deliberations, the succeeding hypothesis was projected.
Methodology
Sample and Data Collection Procedure
In our study, the quantitative research method was used to gather data from doctors employed in Pakistani private sector hospitals from April 5, 2024 to September 30, 2024, using a purposive sampling approach. The purpose of using this sampling technique was to deliberately select doctors as key respondents to capture their perception as well as experience, as they are key players linked to the AI implementation (Abid et al., 2019; Ali et al., 2023; Naveed et al., 2024).
Furthermore, 415 doctors from private sector hospitals in Karachi, Pakistan, were chosen as a sample for our study. The reason for selecting private sector hospitals is due to the AI adoption, as they operate with greater flexibility and financial autonomy as compared to public sector hospitals, in which technology adoption is a bit slower (Sajal, 2024). Therefore, private sector hospitals were chosen as an appropriate setting to study the influence of AI implementation on DPWB with TA as a mediator in a tech-driven and complex environment.
To obtain the maximum responses, the survey was disseminated to 600 respondents. Among them, 415 were received in appropriate form, resulting in a response rate of 69%, which is considered good for analysis. To achieve a high response rate and minimize response bias, multiple strategies were employed, including sending emails to potential participants and utilizing the professional medical network, followed by reminder emails over 3 weeks to ensure maximum participation. To encourage participation, a survey was designed that was compatible with both desktop and mobile devices. To ensure the participants’ willingness to participate. Furthermore, a two-step method was executed to examine the mediation effect. Firstly, data were collected on the predictor and outcome variables. After 6 weeks, data were collected on TA as a mediator from the same respondents. Time lag (T1 and T2) was used to measure the mediating effect (Cain et al., 2018).
In addition, to minimize any potential risk to the respondents, this study employed a survey. No medical interventions were used; therefore, respondents were not exposed to any physical or psychological harm. Furthermore, voluntary participation was ensured as an online method was used, and respondents had the choice to participate. Accordingly, this study offers potential benefits to society by shedding light on how AI affects doctors’ wellbeing with TA as a mediating factor. Results can help practitioners design, implement, and support systems in healthcare settings, leading to reduced stress, burnout, and mental challenges among healthcare professionals. Additionally, informed consent (IC) was obtained from the respondents by presenting the study purpose, ensuring voluntary participation, and assuring data confidentiality at the beginning of the survey. All results will be shared cumulatively to protect the rights of the respondents by following the recommendations (Spector, 2006).
Moreover, data was collected from a single source. To mitigate common method bias (CMB). The following steps were taken to lessen this bias. Firstly, anonymity was ensured, and items were carefully worded to minimize social desirability bias. To assess CMB, Harman’s single-factor test was run, which shows that 46.7% of the variance was accounted for by the first factor, well below the recommended value of 50%. Hence, it specifies no issue of CMB. Alongside, VIF values support the robustness of the results against CMB, as its value is less than 5.
Scales
The following AI, TA, and PWB scales were adapted by different researchers, and data were gathered using a five-point Likert scale, ranging from “strongly disagree to strongly agree.” To assess AI implementation, the scale was taken from Shinners et al. (2021). However, only six items were used for analysis as a few items with factor loadings <.70 were excluded. Furthermore, TA was evaluated using the scale developed by Basaif et al. (2020). The scale contains 13 items. However, based on the measurement model, only five items were used for analysis as the remaining items were omitted due to low factor loadings. Lastly, PWB was assessed using a scale developed by Pradhan and Hati (2022). Nevertheless, based on the measurement model, only nine items were used for analysis as one item with low factor loadings was excluded.
Data Analysis Strategy
To assess the measurement and structural model following (Hair, Hult, Ringle, et al., 2013; Hair, Sarstedt, et al., 2017) recommendations; PLS-SEM was used. The prime reason was to employ a variance-based technique that overcomes the limitations linked with CB-SEM (Legate et al., 2023). The PLS-SEM technique is an appropriate way for model testing and predictive relevance from the observed data (Ringle et al., 2020; Sarstedt et al., 2022). It is an effective approach for primary research as well as an extension of a theoretical model (Hair et al., 2022; Wilden et al., 2013).
Findings
Respondents’ Profile and Correlation Matrix
Table 4 presents the respondents’ profile details. The sample consisted of 231 (55.7%) males and 184 (44.3%) females, along with additional information related to age and years of experience. Moreover, AI has the highest mean value of 4.08. In contrast, TA has a mean value of 3.92, and PWB has a mean value of 3.89, respectively. Furthermore, the correlation matrix indicates that there is no issue of collinearity as values fall under the value of .85, and a substantial relationship exists between variables, as the p-value was <.000 (Gujarati & Porter, 2009; Tabachnick & Fidell, 2012).
Respondent’s Profile and Correlation Matrix.

Measurement Model
The factor loadings of each variable shown in Table 5 fall under the threshold of .70 (Black et al., 2010; Joseph et al., 2010). However, a few items were excluded due to low factor loadings. Furthermore, AVE values >.50 indicate the attainment of convergence validity according to the recommendation of Hair et al. (2019). Likewise, alpha values greater than .70 indicate no reliability issues. In addition, the VIF value suggests no multicollinearity issue as all value falls under the threshold value of 5 (Hair, Black, et al., 2009; O’Brien, 2007).
Factor Loadings, Construct Reliability, and Validity.

Note. CA = Cronbach alpha; AVE = average variance extracted; CR = composite reliability.
According to Table 6, the value of R2 indicates that .658 variation in PWB is explained by AI implementation, which is substantial. In contrast, .395 variation in TA is explained by AI implementation, indicating a moderate level of explanatory power. Furthermore, the Q2 value shows the predictive relevance in the model, as the value is >0, as per the recommendation of Cohen (2013), Khan et al. (2025).
Quality Criteria (R-square and Q2).

According to Table 7, the value of f-square shows that the effect size of AI implementation on PWB is explaining a medium effect (f-square = .119), while AI implementation on TA and PWB shows a large effect, respectively (f-square = .652 and .686; Cohen, 2013; Khan et al., 2025).
Quality Criteria (f-square).

According to the results in Table 8, the SRMR value falls below the specified value, that is, <.08, indicating a good model fit. However, the NFI value below .90 indicates the model does not fit. However, not all models require an NFI to be considered valid, particularly in predictive modeling contexts, such as PLS SEM. Recent literature suggests that this index should be interpreted in PLS SEM, where the focus is on prediction rather than exact model fit (Hair et al., 2022). However, the NFI threshold is not well established, and its use is less prevalent in the composite model employed in PLS-SEM (Henseler et al., 2016). Besides, the overall model assessment, as indicated by SRMR and Q2 values, demonstrates strong predictive relevance and supports the structural model’s adequacy (Cohen, 2013; Khan et al., 2025).
Model Fit.

Table 9 indicates no discriminant validity issue, as the values below .90 are an acceptable degree of divergence from other latent constructs (Henseler et al., 2015, 2016).
Discriminant Validity (HTMT Ratio).

Structural Model with and Without Control Variables
According to Table 10, no significant impact was observed on the relationship among variables with control variables. Figure 1 displays the structural model with control variables.
Structural Model Estimates with Control Variables.


Structural model with control variables.
Based on the data results in Table 11, AI has a significant influence on DPWB and TA, while TA has a noteworthy impact on DPWB, as indicated by p < .05.
Structural Model Estimates Without Control Variables.

Accordingly, Table 12 shows the mediation analysis results. The total effect indicates that the implementation of AI has an influence on DPWB. Likewise, TA mediates the link between AI implementation and DPWB. Specifically, the bootstrapped indirect mediating effect is significant, as the confidence interval does not include zero, confirming the presence of TA as a mediating effect between AI implementation and the DPWB relationship by following the bootstrapping method as suggested by Hair et al. (2022). Hence, this indicates that a higher level of TA among doctors fosters a greater sense of control and competence, which contributes to reducing stress and improving wellbeing during AI implementation. Although the direct effect of AI implementation on DPWB remains significant, the presence of a significant indirect effect through TA supports partial mediation.
Mediation Model Estimates.

Discussion and Conclusion
This study offers valuable insights that contribute to the extant literature by examining the AI implementation in predicting DPWB with TA as a mediator. However, it has remained inconclusive from the doctor’s perspective within the healthcare setting. This study provides empirical evidence to fill the gap. Mixed evidence is found in the extant literature on AI and PWB (Giuntella et al., 2023; Gull, Ashfaq, & Aslam, 2023; Proactive, 2023; Zhao et al., 2024).
According to the results, no significant impact is observed on the relationship between the predictor, mediator, and outcome variables when control variables are considered. However, without control variables, AI implementation demonstrates a positive effect on DPWB. This indicates that AI implementation in private sector hospitals not only streamlined the processes but also suggests that emerging technologies like AI enhance doctors’ working efficiency, which in turn contributes to improved DPWB. In addition, findings of the study specify that private sector hospitals are adopting technology more swiftly than the public sector, which often face limitations in resources and infrastructure, which impedes service delivery and negatively affects the DPWB (Naeem et al., 2022). The results align with Proactive (2023) which asserts that AI implementation can aid in boosting wellbeing. This elaboration reinforces that effective implementation of AI tools can foster confidence among doctors, improve service delivery, and lead to enhanced DPWB.
Furthermore, this study responds to the call by researchers to examine the link between AI and DPWB (Gupta et al., 2023; Nazareno & Schiff, 2021; Shaikh et al., 2023). However, the results are not aligned with the study of Gull, Dilawar, and Sher (2023), as a positive link between AI and DPSWB is observed. This indicates doctors see AI implementation as an opportunity to deliver quality services to patients, leading to enhanced wellbeing rather than creating stress in private hospitals.
Besides, TA mediates the link between AI implementation and DPWB. This suggests that TA can help increase awareness, knowledge, and understanding among doctors regarding the application of AI technologies. In turn, doctors perceive AI as a supporting tool, resulting in reduced psychological strain and improved DPWB. Results are linked to the prior perspective presented by researchers (Shahzad et al., 2023; Zahoor et al., 2022). Contrary to this, without TA, confusion may be created, leading to stress and negatively affecting PWB (Brougham & Haar, 2018; Gupta et al., 2023).
Our study also confirms the SCT explanatory power by positioning TA as a cognitive factor mediating the relationship between AI implementation, an environmental factor, and DPWB as a behavioral outcome (Middleton et al., 2019; Wu et al., 2021). Hence, this integration represents a major contribution to the SCT framework within a tech-driven healthcare setting. It is concluded that investing in TA initiatives as part of AI implementation strategies in healthcare is beneficial. Such initiatives can foster DPWB. Furthermore, this study offers substantial insight into SCT from cognitive, environmental, and behavioral perspectives. This, thereby, enriches the AI and PWB literature, particularly from the context of private sector hospitals in a developing country like Pakistan.
Theoretical and Practical Implications
In the era of emerging technologies, this study contributes to the extant literature on SCT by highlighting the role of TA as a mediator in the relationship between AI implementation and the DPWB. Our study expands the SCT framework by emphasizing the interplay between cognitive, environmental, and behavioral factors that affect learning as well as outcomes (Bandura, 2001). Specifically, AI implementation serves as an environmental stimulus that can influence a personal (cognitive) capacity, such as TA, which in turn influences behavioral outcome, that is, DPWB. Thus, this underscores the crucial role of cognitive orientation in adapting to the environmental (technological) change (Middleton et al., 2019; Wu et al., 2021).
Furthermore, this study provides novel insights regarding the integration of TA as a mediator between AI and psychological outcomes, as limited research has explored this link in the healthcare context (Bandura, 2011; Chin & Mansori, 2018; Hui et al., 2024; Lent & Brown, 2008). This gap is addressed through this study by examining the mediating role of TA within the framework of AI and DPWB in a private sector hospital in a developing country, specifically Pakistan (Tribune, 2021). Accordingly, this study responds to the recent call for exploration of the impacts of AI on various factors of the healthcare setting (Cavanagh et al., 2023).
This study provides valuable insights into the adoption of technological tools by healthcare practitioners. Healthcare managers should devise and implement employee-centric strategies aimed at fostering TA, such as by investing in targeted training programs designed to enhance doctors’ understanding, knowledge, and proficiency with AI tools. As a result, familiarity with AI is expected to reduce uncertainty, build confidence, and subsequently reduce stress, thereby enhancing DPWB.
Additionally, the inclusion of AI-related education in medical curricula may help equip healthcare professionals with the necessary skills and knowledge to adapt more effectively to technological advancements. This proactive approach can reduce resistance as well as stress, thereby fostering better doctor-patient relationships. In addition, healthcare organizations should consider implementing structured awareness campaigns, mentorship programs, and emotional support to ease the psychological transition during AI implementation (Nazareno & Schiff, 2021). Henceforth, the abovementioned initiatives are aligned with the recommendation of Parry and Battista (2019) who emphasize the importance of holistic support in improving wellbeing outcomes.
In this regard, to fully understand and realize the benefits of AI implementation, healthcare organizations must strategically align their tangible, intangible, and human resources to enhance awareness and support the adoption of technological innovation. Managers should implement mechanisms to monitor DPWB and performance following training and development interventions, enabling them to address issues more effectively and manage their stress and anxiety levels, promoting sustained wellbeing among healthcare professionals.
Limitations and Directions for Future Researchers
A few limitations exist in this study that future researchers can address. First, TA was assessed as a mediating factor between AI implementation and PWB from the doctors’ perspective. Future researchers may examine this link from a management perspective by adding mediating and moderating variables such as digital servitization, organizational culture, management support, and digital leadership.
Furthermore, this study focused only on quantitative data. Future studies may conduct mixed-methods studies to expand the scope of AI, TA, and PWB literature. Moreover, this study is limited to doctors working in private sector hospitals. Researchers may conduct studies in the public sector to compare the results, which will advance the generalizability (Naeem et al., 2022).
Accordingly, future researchers may explore the framework across various countries and cultures by examining the other dimensions of well-being, such as occupational and social wellbeing. Lastly, a cross-sectional design was employed in this study. Researchers may explore the model using a longitudinal time horizon to see the impact of AI implementation over time.
Footnotes
Ethical Considerations
The Faculty of Management Sciences, Bahria University, Pakistan, granted ethical clearance: Letter No. BUKC/DMS/2024 (110). We declare that no data related to human medical intervention, and tissues were involved in this study.
Consent to Participate
Principles of informed consent, data confidentiality, and voluntary participation were strictly followed.
Author Contributions
Munaza Bibi: Original draft, investigation, formal analysis, conceptualization, validation, methodology. Tse Guan Tan: Review & editing, original draft, supervision. Heng Yao: Analysis, review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a postdoctoral fellowship from the Universiti Malaysia Kelantan, Kelantan, Malaysia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be available on request.