
Abstract
A second dose of measles (MCV2) was established to immunize children who did not respond protectively to the first dose. However, outbreaks continue to occur despite the availability of safe and effective vaccinations. The objective of this study was to identify determinants of defaulting from completion of the second dose of measles among 18 to 24 month-old children in Gindeberet district, West Shoa, Oromia, from January 6 to March 5, 2022. A community-based, unmatched case-control study was conducted among 654 children (218 cases and 436 controls). A systematic sampling technique was used to select the study participants. Data were collected using a pretested and structured questionnaire. An adjusted odds ratio with a 95% CI and a p-value of <.05 was used to identify the determinants of defaulting from MCV2. Absence of reminder (PNC; AOR = 4.28, 95% CI: 2.34–7.82), Antenatal Care (ANC) contact ≥2 2 (AOR = 5.15, 95% CI: 2.86–9.25), long waiting time (AOR = 2.27, 95% CI: 1.18–4.36), no awareness (AOR = 7.95, 95% CI: 4.21–15.02), not receiving Penta3 (AOR = 4.08, 95% CI: 1.88–8.82), and not receiving ≥2 doses of vitamin “A” (AOR = 4.18, 95% CI: 2.15–8.10) were found to be determinants of defaulting from MCV2. Absence of reminder, ANC ≤2, long waiting time, no awareness, not receiving penta3, and not receiving ≥2 doses of vitamin “A” were determinants of defaulting from MCV2. Hence, mothers should be aware of the importance of a second dose of measles.
Introduction
Immunization is the process of making a person immune or resistant to an infectious disease, which is usually accomplished by the administration of a vaccine. Vaccines activate the body’s immune system, which protects the individual from potential infection or disease (World Health Organization, 2013). Measles is an extremely infectious and serious illness. It also leads to serious health problems such as pneumonia, diarrhea, brain damage, deafness, and blindness. The disease spreads quickly from infected to uninfected people. For many years, due to the low measles vaccination coverage, many countries, including Ethiopia, couldn’t achieve measles elimination (KMOH, 2012; World Health Organization, 2020).
The term “defaulters” states fail to return for a vaccination appointment at least 2 weeks after the scheduled date (KMOH, 2012). The measles vaccine is recommended on a regular basis at the age of 9 months for measles-containing vaccines first and 15 to 18 months for a second dose. One month is the minimum interval between MCV1 and MCV2 vaccines. The best age for measles vaccination is established by taking into account the age-dependent rise in measles vaccine seroconversion rates and the average age of infection. Antibody responses to MCV grow with age up to roughly 15 months due to lowering levels of inhibiting maternal antibodies and decreasing immune system immaturity (World Health Organization, 2020).
Measles vaccine second dose (MCV2) is an opportunity for those whose children failed to develop a protective immune response to the first dose and allows vaccination of children who have not received the first dose of measles vaccination (World Health Organization, 2018).
Even though the World Health Organization (WHO) report indicates the global dose increase is a 42% MCV2 dose increase to 71% in 2019. Annually, more than 37 million children around the world lose their second dose of the measles vaccine (World Health Organization, 2020). Ethiopia launched the measles vaccine second dose vaccination into a regular scheduled immunization program in the year 2019 (World Health Organization, 2018).
Despite the availability of a safe and effective vaccination, measles remains a global public health issue and outbreaks continue to occur, and progress toward regional elimination goals has slowed; so strengthening routine MCV2 administration has a great role (World Health Organization, 2020).
Generally, the measles strategic framework guidelines indicate that of all unvaccinated children, 90% of them are susceptible to measles. So, to ensure the goal of a measles-free world in 2030, the issue of MCV2 introduction needs the contribution of all, like caregivers, health personnel, government, and partners (World Health Organization, 2020).
There has been limited research on the determinants of defaulting from second-dose measles in the study area. Therefore, this study aimed to identify determinants defaulting from completion of the second dose of measles among 18 to 24-month-old children in Gindeberet district, West Shoa.
Methods
Study Area and Period
This study was conducted in the Gindeberet district in West Showa Zone, Oromia Regional State, Ethiopia, from January 6 to March 5, 2022.
Study Design
A community-based unmatched case-control study design was used.
Population
Source population
All mothers/caretakers with children aged 18 to 24 months living in the Gindeberet district started their first dose of the Measles vaccine.
Study Population
Sampling Unit
Individual mother/caregiver of children aged 18 to 24 months.
Inclusion and Exclusion Criteria
Inclusion criteria
Mothers or caregivers who lived in Gindeberet district for at least 6 months with singleton children aged between 18 and 24 months were eligible for the study and were not confused with describing information about the children that were included
Cases: All mothers/caregivers of children aged 18 to 24 months who started the first dose and defaulted from the second dose of measles.
Exclusion criteria: Mothers/Caregivers who were seriously ill.
Sample Size Determination and Sampling Technique
Sample
size determination
The sample size was determined by using EPI info version 7.2.2.6 with the following assumptions: 95% confidence level, 80% power, Design effect 1.5, and a case to control ratio of 1:2. Based on the PENTA3 variable, the odds’ ratio of 3.45, and the percent of controls exposed, 3.92%, were taken from the previous study done on uptake of the second dose of measles (Makokha, 2016). This gave us 132 cases and 264 controls, which gave 396 sample sizes. Then, by considering the 1.5 design effect, the sample size was 594. By adding a 10% non-response rate, the final sample size was n = 654 (218 cases and 436 controls; Table 1).
Socio-Demographic Characteristics of the Study Participants in Gindeberet District, West Shoa, Oromia (n = 651), 2022.

Sampling Procedure
The Gindeberet district was purposely selected because it is one of the marginalized districts in West Shoa and there was interruption in provision of health care, including immunization, because of security problems for 3 years prior to the data collection period. Gindeberet district was stratified into urban and rural kebeles (lower administrative units); from 31 rural kebeles, 10 were chosen by a lottery method and one urban (the only sub-district in the study area) was included in the study. To identify the cases and controls, the baseline survey was conducted 2 weeks before data collection to identify the list of children who completed the second dose of measles according to the schedule (controls) and those who took only the first dose of measles (cases) by trained data collectors.
The total sample size was proportionally allocated to each sub-district based on population size. Using the sample frame of cases and controls from the baseline survey, 218 cases and 436 controls were selected by systematic random sampling technique (Figure 1).
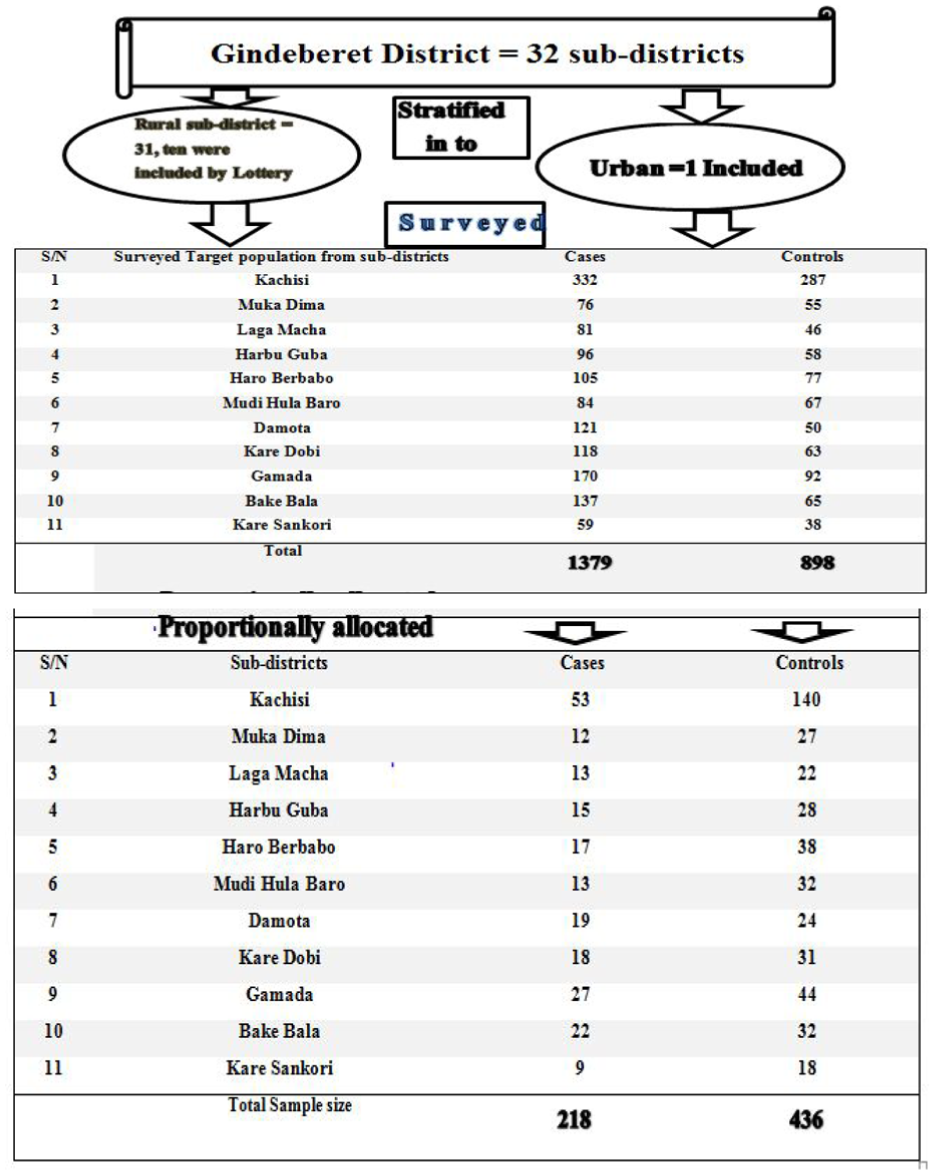
Schematic presentation of the sampling procedure for determinants of defaulting from completion of MCV2 study participants in Gindeberet district, West Shoa, Oromia (n = 654), 2022.
Variables
Dependent Variable
Defaulting from the second dose of Measles Vaccination
Independent Variables
Socio-demographic Related Factors:
• Educational status of Mothers/Care-giver • Place of residence • Caregivers age • Marital status • Family size • Caregivers occupation • Age of child • Birth order • Sex of child
Maternal (Caregiver) characteristics related factors
• Awareness of the schedule of immunization • Perception of the benefit of immunization • Immunization History of BCG, Penta3, and Vitamin “A”
Healthcare-related factors:
• ANC follow up • Place of delivery • PNC follow up • A reminder given during postnatal care on MCV
Health system-related factors
• Time to travel to the vaccination site • HEW Visits • Vaccination waiting time • Number of vaccination days per week
Operational Definition
Awareness of the schedule of the second dose of measles: Caregivers were asked four questions. After computing the sum, those who scored above or equal to mean were considered as having awareness and those who scored below mean were considered as not having awareness (Yenit et al., 2018).
Perception six of the benefits of six measles vaccine: Perception-related six questions were asked using a Likert scale from strongly agree to strongly disagree, which has five options. After computing, the mean score for each construct was dichotomized into positive and negative perceptions by using the mean score (Yenit et al., 2018).
Data Collection Tools and Techniques
Data was collected using a structured interview-administered questionnaire from mothers or caregivers who had children aged 18 to 24 months using a questionnaire. The questionnaire had six parts, namely: socio-demographic, maternal health care, health facility, awareness of MCV2, perceptions toward the benefit of MCV2 and parallels given immunizations related according to the objective of the study. Thirty-one questions were prepared in English after revising different literature and translated into Afan Oromo and translated back into English by a language expert to ensure consistency. Six trained data collectors and two senior B.Sc. nurses were supervisors recruited for the study.
Data Quality Control and Management
Data quality assurance was done in three steps, before, during, and after the data collection period. First, before the data collection period, two-day training was given for data collectors and supervisors based on the six parts of the questionnaire, interview-administered data collection methods followed, ethical concerns, and the purpose of the study using addition to using COVID-19 (Coronavirus disease nineteen) prevention methods such as hand washing, use sanitization, wearing a mask, and physical distance was considered. The training was given by the investigator; the questionnaire prepared in English was translated into the Afan Oromo language and back to English to keep the consistency of the questions. In addition, the Afan Oromo version questionnaire was pre-tested on 5% (On caregivers of 11 cases and 22 controls) of the sample size before actual data collection at Gindeberet district from a non-selected sub-district. The necessary modification was done modifications on some items of the questionnaire based on a finding of the pretest done for the actual data collection. Close, timely supervision was made to maintain the quality of collected data.
Data Analysis
The collected data were checked, coded, and entered into Epi-info version 7.2.2 and exported to SPSS version 26 for analysis. Descriptive statistics were calculated by using cross-tabulation for independent and dependent variables. The presence of multi-col-linearity between independent variables was checked using the VIF<10 and tolerance test between 0.1 and 1 to fulfill the assumption of no multi-collinearity. The Hosmer and Lemeshow goodness of fit test was used to assess the fitness of the fit and the final model fit in the binary logistic regression model assessing the association between the dependent and independent variables.
All variables with p-value <.05 were entered into the multivariable analysis to determine the independent determinants of defaulting from the second dose of measles. The adjusted Odd ratio with a 95% confidence interval and p-value <.05 was reported to declare significant determinants of defaulting from the second dose of measles. Finally, the data was presented with texts, tables, and graphs.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 651 mothers/caregivers of children aged 18 to 24 months (217 cases and 434 controls) participants were involved in this study with a response rate of 99.5%. The mean age of respondents was 32.82 (SD ± 8.19) for cases and 30.02 (SD ± 5.44) for controls, respectively. Most caregivers, 193 (88.9%) cases and 411 (94.7%) controls were mothers. One hundred fifteen (52.8%) of cases and 232 (53.5%) of controls were female children (Table 1)
Maternal Healthcare-Related Characteristics
In this study, 102 (47.0%) in cases of mothers and 7 (1.6%) mothers of controls did not attend antenatal care services before delivery (Table 2).
Maternal Healthcare-Related Characteristics of Study Participants in Gindeberet District, West Shoa, Oromia (n = 651), 2022.

Health Facility-Related Characteristics of the Study Participants
Among study participants, 103 (47.5%) caregivers of cases and 193 (44.5%) caregivers of controls traveled more than 30 min to reach the nearest health facility. Sixty-five (30.0%) caregivers of cases and 97 (22.4%) caregivers of controls experienced delays during their vaccination appointment (Table 3).
Health Facility-Related Characteristics of the Study Participants in Gindeberet district, West Shoa, Oromia (n = 651), 2022.

Awareness-Related Characteristics of the Study Participants on MCV2
This study found 192 (88.5%) caregivers of cases and 161 (37.1%) caregivers of controls had no awareness of the second dose of measles (Table 4).
Awareness-Related Characteristics of the Study Participants in Gindeberet District, West Shoa, Ethiopia (n = 651), 2022.

Perception-Related Characteristics of the Study Participant on MCV2
This study shows 157 (72.4%) caregivers of cases and 288 (71.1%) caregivers of controls had a negative perception of the second dose of measles (Figure 2).
Shows perceptions toward benefits MCV2 of study participants in Gindeberet district, West Shoa, Oromia (n = 651), 2022.
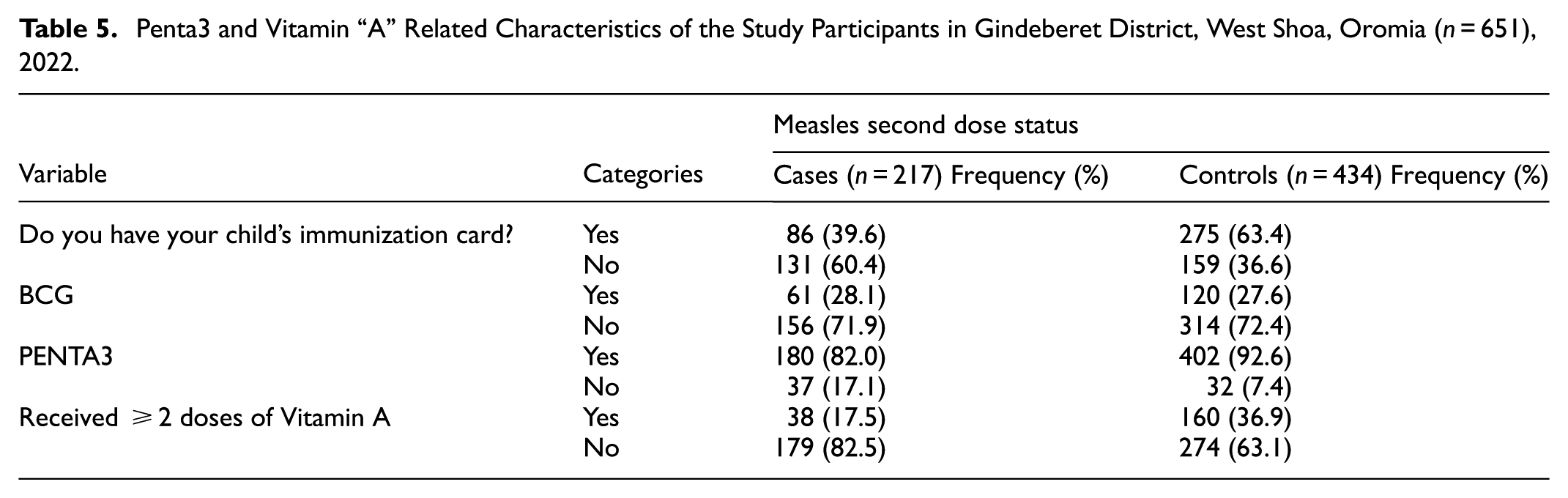
The study finding shows that 132 (60.6%) of caregivers and 160 (36.7%) caregivers of controls had no immunization card (Table 5).
Penta3 and Vitamin “A” Related Characteristics of the Study Participants in Gindeberet District, West Shoa, Oromia (n = 651), 2022.
Determinants of Defaulting from the Second Dose of Measles
Bi-variable logistic regression analysis was conducted to identify candidate variables for multivariable logistic regression analysis and variables with p-values of <.25 were included in the multivariable logistic regression analysis model. After adjustments for possible effects of confounding variables, multi-variable logistic regression shows the absence of reminder of measles vaccine during postnatal care, number of antenatal care contact, keeping long facility waiting times for vaccination, educational status of maternal/caregivers, absence of awareness of the second dose of measles, being not vaccinated penta3, and not received greater or equal to two doses vitamin “A” were significantly and independently associated with defaulting from completion of the second dose of measles.
In this study, defaulting from the second dose of measles was 4.28 times (AOR = 4.28, 95% CI: 2.34, 7.82) more likely among children whose mothers didn’t get reminders of the second dose of measles during their post-natal care than those who were during their post-natal care. Additionally, regarding this study, defaulting from a second dose of measles among mothers of children who had ≤2 antenatal care contact was 5.15 times (AOR = 5.15, 95% CI: 2.86, 9.25) more likely as compared to those who had above two antenatal care contacts. Mothers/caregivers served with a long facility waiting time for vaccination is 2.27 times (AOR = 2.27, 95 % CI: 1.18, 4.36) are more likely to default from the second dose of measles as compared to those who served within a short waiting time.
Children of mothers/caregivers who didn’t follow their formal education were 5.72 times (AOR = 5.72, 95% CI: 2.80, 11.69) more likely to default from a second dose of measles compared to those who followed their formal education. Additionally, those mothers/caregivers of children who had no awareness about the second dose of measles were 7.95 times (AOR = 7.95, 95% CI: 4.21, 15.02) more likely to default from the second dose of measles than those who had awareness about the second dose of measles.
Mothers/caregivers whose children didn’t receive pentavalent3 were 4.08 times (AOR = 4.08, 95% CI: 1.88, 8.82) more likely to default from the second dose of measles as compared to those of vaccinated penta3. Similarly, mothers/caregivers whose children didn’t receive ≥2 doses of vitamin “A” were 4.18 times (AOR = 4.18, 95% CI: 2.15, 8.10) more likely to default from second doses of measles as compared to those who received greater or equal to two doses vitamin “A” (Table 6).
Bi-Variable and Multi-Variable Logistic Regression Analysis (By Using Backward Variable Selection) Showing the Association Between Independent Variables and MCV2 AMONG STUDY Participants in Gindeberet District, West Shoa, Oromia (n = 651), 2022.

Note. AOR = Adjusted Odds Ratio; CI = Confidence Interval; 1 = Reference.
Significant at p < .05
Discussion
This study aimed to assess the determinants of second-dose measles vaccination dropout among children aged 18 to 24 months old in Gindeberet district, West Shoa, Ethiopia. The findings of this study showed that the absence of reminders of the measles vaccine during postnatal care, number of antenatal care contacts, long facility waiting times for vaccination, educational status of maternal/caregivers, absence of awareness of receiving the second dose of measles, being not vaccinated penta3, and not receiving greater or equal to two doses of vitamin “A” were found significantly and independently determinants of defaulting from completion of the second dose of measles. This study found that mothers who did not get reminders about a second dose of measles during their postnatal care were more likely to default from a second dose of measles than those who have been reminded during their post-natal care. This finding is in line with studies conducted in the USA systematic review and Laelay Adiabo, Tigray (Aregawi et al., 2017; Watterson et al., 2015). Reminders, particularly text messages, can be effective in reducing the rate of defaulting from the second dose of the measles vaccine as that reminders can improve timely receipt of the second MMR dose by increasing appointment scheduling and attendance. This, in turn, can lead to higher overall vaccination coverage and help prevent measles outbreaks. Postnatal care is the best opportunity to learn what services are required and to be reminded of all relevant appointments in the future (Watterson et al., 2015). In this study, defaulting from a second dose of measles among mothers of children who had ≤2 antenatal care contact were 5.15 times more likely as compared to those who had above two antenatal care contacts. Having fewer than two antenatal care (ANC) contacts is significantly associated with an increased likelihood of defaulting from the second dose of the measles-containing vaccine (MCV2). Specifically, studies show that mothers with fewer ANC contacts are more likely to have their children drop out of the MCV2 vaccination schedule. This finding is consistent with studies conducted in Afar, Ethiopia (Hailu et al., 2022; Kinfe et al., 2019). This can be due to mothers who had more antenatal care services having a chance to communicate with health workers to hear about the benefits of vaccinations (Kinfe et al., 2019). This study shows that mothers/caregivers’ children who received the vaccine after a long waiting time were 2.27 times more likely to default from a second dose of measles as compared to those who received it within a short time at the health facility. This finding is consistent with the study in Afar (Hailu et al., 2022). Long waiting times are most of the time considered due to negligence and fewer health care providers (Ekhaguere et al., 2021). In this study, the mothers/caregivers who didn’t follow their formal education were 5.72 times more likely to default from a second dose of measles compared to those who were formally educated. The finding is in line with the studies conducted in East China, EDHS, 2016, and Ethiopia systematic review (Nour et al., 2020; Kinfe et al., 2019). This is because mothers are more likely to be exposed to their children among families, and their education enables them to understand and easily identify necessary care for their children (Kibreab et al., 2020). However, a study conducted in Kenya reveals no statistical difference between caregivers’ education and defaulting from completion of the second dose of measles (Makokha, 2016). This might be due to socio-demographic and methodological differences. Caregivers who had no-awareness of the second dose of measles were 7.95 times more likely to default from the second dose of measles than those who had awareness. This finding is consistent with studies conducted in Kenya and East China (Hu et al., 2013; Makokha, 2016). This might be due to the fact that poor counseling at the facility and inadequate advice regarding the next appointment were found to contribute to the problem of defaulting from vaccination. Mothers/caregivers whose children were not vaccinated for the penta3 dose are 4.08 times more likely to default from the second dose of measles as we compared those of children vaccinated patanta3. This is potentially due to factors like increased access to vaccination services and improved parental awareness among those who complete the Pentavalent series. Similarly, mothers/caregivers whose children didn’t take ≥2 doses of Vitamin “A” were 4.18 times more likely to default from the second dose of measles as compared to those children who took above two doses of vitamin “A.” This finding is in line with the study conducted in Kenya (Makokha, 2016). Many times, maternal and children services are children integrated into healthcare facility settings. One service can open another opportunity to get more recommended services. But it is based on a strong health system in all aspects like awareness creation and bringing, necessary products mandated for the services (Wallace et al., 2009). The strength of this study is that cases and controls were selected from the same source population (controls were selected from the respective community that yielded the cases). There is enough an adequate number of kebeles were included. As a result, cases and controls were comparable. A qualitative study is needed to explore further determinants of children defaulting from second doses. Recall bias may occur due to the forgetfulness of the mothers/caregivers about their children’s status, which could result in misclassification cases and controls.
Conclusion and Recommendations
Conclusion
This study identified that, a reminder not given on the second dose of measles, ANC contact ≤2, long health facility waiting time, maternal/caregiver education status, absence of awareness on the second dose of measles, not received penta3, and not received greater or equal to two doses of vitamin “A” were determinants of defaulting from completion of the second dose of measles. Hence, the results highlight the need for strengthening reminder on second doses of measles, timely antenatal care, vitamin A vaccine administration and increasing awareness of the benefits of areas penta3 vaccine in areas.
Footnotes
Author Contributions
All the authors contributed significantly to the research work. All authors made contributions in design, implementation, data collection, analysis, writing to and interpretation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be shared upon request. The corresponding author will make any reasonably necessary data available.