
Abstract
The integration of Artificial Intelligence (AI) into healthcare holds transformative potential for developing countries, yet its application remains underexplored in many such contexts. This study addresses the research gap by examining the current state, challenges, and ethical considerations of AI adoption in Tanzania’s healthcare system. Combining a systematic literature review with semi-structured interviews involving 32 key stakeholders, including healthcare practitioners, policymakers, and technologists, the study provides a comprehensive, context-sensitive analysis. The findings reveal that AI is increasingly applied to diagnostics, predictive analytics, mental health support, and health education. However, widespread adoption is constrained by infrastructural deficits, organisational readiness gaps, limited workforce capacity, and low digital literacy, particularly in rural areas. Ethical concerns such as data privacy, algorithmic bias, and lack of transparency also emerged as critical barriers. Policy fragmentation and the absence of AI-specific implementation guidance further complicate integration efforts. Despite these challenges, stakeholders expressed optimism about AI’s potential to improve diagnostic accuracy, reduce provider burden, and expand access, especially through mobile-based tools. This study’s unique contribution lies in its integration of the Technology-Organisation-Environment (TOE) and Ethical AI frameworks to assess AI adoption holistically, linking global evidence to local realities. The study recommends decentralised policy development, inclusive design processes, and sustained investment in digital infrastructure and training. These actions are essential for fostering ethical, inclusive, and sustainable AI-driven healthcare transformation in Tanzania and similar low-resource settings.
Plain language summary
This study looks at how artificial intelligence (AI) is being used to improve healthcare in Tanzania. AI includes computer systems that can help doctors diagnose diseases, predict outbreaks, or support medical decision-making. In many countries, AI is already helping to improve patient care, reduce costs, and make health services more efficient. But in Tanzania and other developing countries, the use of AI is still new and faces many challenges. The study combines a review of published research with interviews from doctors, policymakers, and technology experts in Tanzania. It finds that while AI tools can support healthcare, especially in rural areas, there are problems like poor internet, limited electricity, lack of trained staff, and concerns about patient privacy and fairness in AI decisions. The research also explores how government policies and local infrastructure affect the ability to use AI in hospitals and clinics. One key concern is that many AI tools are designed for high-income countries and may not work well in Tanzania’s settings. The study suggests ways to make AI more useful and ethical, such as involving local healthcare workers in designing tools, improving training, and creating clear rules to protect patient data.
Keywords
Introduction
The integration of Artificial Intelligence (AI) into healthcare is reshaping service delivery globally (Alowais et al., 2023; Bajwa et al., 2021). In developed countries such as the United States, AI has been successfully applied to tasks such as diagnostic imaging, clinical decision support, patient monitoring, and administrative automation (Bajwa et al., 2021; Elhaddad & Hamam, 2024; Khalifa & Albadawy, 2024). These innovations have significantly enhanced diagnostic accuracy, supported treatment planning, and led to reductions in operational costs across health systems. AI-powered diagnostic algorithms have demonstrated performance matching or exceeding human experts. For example, deep learning models used in radiology for pneumonia or stroke detection enhance accuracy and improve efficiency (Hanna et al., 2025; Khalifa & Albadawy, 2024; Maleki Varnosfaderani & Forouzanfar, 2024). Furthermore, clinical decision support systems leveraging machine learning have improved treatment outcomes and reduced missed diagnoses by providing timely, data-driven guidance during patient care (Karuppan Perumal et al., 2025; Mitra & Rehman, 2024; Pinto-Coelho, 2023). AI-driven administrative automation, including natural language processing (NLP) for clinical documentation and automated billing systems, has streamlined hospital workflows, and reduced operational overheads (Karuppan Perumal et al., 2025; Pingili, 2025).
In contrast, the adoption of AI in healthcare across developing countries is still emerging. While the potential for AI to address systemic healthcare challenges in developing countries is well acknowledged, such as in disease surveillance, remote diagnostics, and workforce support (Elhaddad & Hamam, 2024; Tshimula et al., 2024; Zuhair et al., 2024), its implementation remains uneven. Pilot projects across countries like India, Kenya, and Ghana have demonstrated the promise of AI-powered mobile tools, chatbots, and predictive analytics in improving access and quality of care (Segun-Omosehin et al., 2025; Tshimula et al., 2024). However, these efforts often face significant barriers, including poor infrastructure, limited digital capacity, and ethical concerns related to data privacy and algorithmic fairness.
In Tanzania, the adoption of AI in healthcare is still nascent, despite increasing recognition of its potential. While foundational digital health systems such as electronic health records (EHRs), mobile health (mHealth), and telemedicine have been rolled out, AI-specific implementations remain limited and fragmented. The Tanzania Digital Health Strategy (2019–2024) and the AI policy framework for the health sector both acknowledge the transformative role of AI, yet challenges persist, including underdeveloped data systems, lack of interoperability, and insufficient regulatory frameworks (Holl et al., 2024; Ministry of Health, 2022; MoHCDGE, 2019). These issues are particularly acute in rural areas, where connectivity gaps, workforce shortages, and infrastructure limitations hinder effective technology use. Although recent strategies emphasise inclusive digital governance and investments in ICT infrastructure, the absence of clear AI integration pathways and weak capacity at subnational levels continue to constrain progress (MoH, 2017).
Despite this context, few empirical studies have systematically explored how AI is currently being used in Tanzania’s healthcare system or examined the challenges that healthcare stakeholders encounter. While international literature outlines general barriers to AI in developing countries, there is a lack of locally grounded evidence that captures the lived experiences of healthcare practitioners, policymakers, and technologists in Tanzania. Ethical considerations such as data protection, fairness in AI outcomes, and trust are especially underexplored. These gaps are critical, as ignoring them risks further entrenching health inequalities through technologies that are not designed with local needs and contexts in mind.
This study, therefore, aims to provide a comprehensive understanding of the current state of AI use in Tanzania’s healthcare sector, the barriers impeding its wider adoption, and the ethical and policy issues that must be addressed for responsible implementation. By drawing on a systematic literature review and semi-structured interviews with key stakeholders, the study offers practical insights for policymakers, healthcare leaders, and technology developers. Unlike previous work that has often focussed on technical feasibility, this study centres on the realities of integrating AI in low-resource settings, including rural perspectives that are frequently overlooked.
The main objective of this study is to investigate how AI technologies are being applied in Tanzania’s healthcare system and to identify the challenges and ethical considerations that influence their adoption and use. In doing so, the study aims to propose strategies for the inclusive, sustainable, and context-sensitive integration of AI across Tanzania’s health sector. Table 1 lists the research questions guiding this study.
Research Questions.

Source. Authors’ work.
Literature Review
Theoretical Framework
The adoption of AI in healthcare requires a theoretical lens that captures both operational complexity and ethical responsibility. This study integrates the Technology-Organisation-Environment (TOE) framework and the Ethical AI framework to guide analysis of enablers, barriers, and implications of AI use in Tanzania’s healthcare system.
The TOE framework is well-suited for developing countries’ contexts, as it considers not only the technological attributes of innovation but also the organisational readiness and external environment (Tornatzky & Fleischer, 1990).
These dimensions help assess factors such as AI tool compatibility, infrastructure and workforce capacity, and policy or societal influences, core elements examined through this study’s interviews and literature review.
Complementing this, the Ethical AI framework focuses on fairness, transparency, accountability, and privacy, key concerns in Tanzania, where data protection is evolving, and algorithmic bias risks are real (Floridi & Cowls, 2019). This framework ensures ethical imperatives are not peripheral but central to understanding and designing AI for equitable healthcare.
Alternative models like the Technology Acceptance Model (TAM) and Unified Theory of Acceptance and Use of Technology (UTAUT) were considered but lacked the contextual depth needed. TOE offers broader applicability to institutional and policy-level dynamics, while the Ethical AI framework anchors the study in principles critical to responsible AI use in low-resource health systems.
Empirical Review
AI Applications in Healthcare
Globally, AI has become integral to advancing healthcare, particularly in diagnostics, predictive analytics, and operational optimisation (Johnson et al., 2021). In developed countries, AI is widely used for early disease detection, imaging diagnostics, and clinical decision support, leveraging high-quality datasets and robust digital infrastructures (Alowais et al., 2023). These tools have shown effectiveness in identifying cancers, cardiovascular anomalies, and neurological disorders (Beauchemin et al., 2019; Bösel et al., 2025; Huang et al., 2020; Jiang et al., 2017; Ordine et al., 2025; Samaras et al., 2023; Tiwari et al., 2025). In contrast, applications in developing countries, including Tanzania, focus more on bridging access gaps and addressing workforce shortages. In such settings, AI-enabled tools like mobile diagnostics and telemedicine platforms have been used to detect diseases such as tuberculosis, malaria, and cervical cancer (Chibi et al., 2023; IHI, 2019; Mariki et al., 2021; Mshani et al., 2024; Oronti et al., 2024). These solutions have proven valuable in rural environments where healthcare access is limited, offering time-efficient alternatives for screening and diagnosis (Guo & Li, 2018).
However, the uptake of AI in developing countries remains uneven and experimental. While some pilot programmes show promise, they are often urban-centric and donor-driven, lacking institutional continuity. Tanzania’s AI adoption, for instance, remains in early stages, with sporadic initiatives rather than integrated national frameworks indicating a critical need for context-specific evidence and scalable applications customised to the country’s healthcare infrastructure and population needs.
Barriers to AI Adoption in Developing Countries
Despite its potential, integrating AI into healthcare systems in developing countries faces numerous barriers. In developed countries, AI benefits from a confluence of technical expertise, policy support, and infrastructure (Fahad, 2024; Junaid et al., 2022). In contrast, developing countries grapple with unreliable electricity, low internet penetration, and a shortage of skilled personnel (Archer et al., 2021; Bostan et al., 2024; Touray et al., 2013; Yu et al., 2024). AI systems developed in developed countries often assume the presence of digital health records and computational resources conditions largely absent in many developing countries’ contexts (Mannuru et al., 2025; Naidoo et al., 2022; Owoyemi et al., 2020). As a result, such systems perform poorly when transferred to environments with fragmented data and constrained hardware (Hosny & Aerts, 2019).
Ethical and Implementation Considerations
The ethical deployment of AI in healthcare requires careful attention to data privacy, algorithmic fairness, and transparency concerns that are particularly critical in developing countries with evolving regulatory landscapes (Mennella et al., 2024; Pham, 2025). While developed countries have implemented legal frameworks to manage AI risks, many developing countries lack data protection laws and institutional oversight (Palaniappan et al., 2024; Rodrigues, 2020). This regulatory vacuum increases the risk of data misuse, discriminatory outcomes, and loss of trust in digital systems.
The Ethical AI framework underscores the need for fairness, accountability, inclusiveness, and transparency (Floridi, 2023; Floridi & Cowls, 2019). In practice, this translates to designing systems that incorporate local data, explainable models, and safeguards against bias. However, literature reveals that ethical considerations are often addressed superficially in developing countries, with few studies offering actionable solutions (Abhulimen & Ejike, 2024). Approaches such as privacy-by-design, community consent models, and inclusive algorithm training remain underutilised but are essential for building trust and legitimacy (Wahl et al., 2018).
Strategies for Inclusive and Sustainable AI Integration
To overcome these challenges, researchers emphasise the need for locally grounded, stakeholder-driven strategies. In developing countries, inclusive implementation frameworks combining phased deployment, user training, and infrastructure investments have been shown to improve adoption and long-term sustainability (Carnahan et al., 2023; Danso et al., 2024). Capacity-building for healthcare professionals is particularly important, as it fosters ownership and reduces reliance on external technical support (Brownson et al., 2018; DeCorby-Watson et al., 2018; Mansour et al., 2021). Programmes contextualised to clinical contexts can improve user acceptance and ensure that AI systems are integrated into existing workflows.
Policy and governance reforms also play a vital role. Evidence from countries with successful AI pilots suggests that alignment with national digital health strategies and investment in scalable, interoperable technologies are crucial (Lin & Zhu, 2025; Taeihagh, 2021; Ulnicane et al., 2021). The developing countries’ emerging digital health landscape presents a foundation for this, but more focussed policy frameworks are needed to mainstream AI applications. Investments in low-bandwidth, culturally relevant AI tools as well as frameworks for evaluating their performance are essential for ensuring inclusive and context-sensitive innovation (Wolff et al., 2021).
Literature Gap
Despite growing global interest in the use of AI in healthcare, there is a notable gap in the literature focussing on its application in developing countries. Most existing studies are based on high-income settings, where infrastructure, data availability, and digital literacy levels differ significantly. As a result, there is limited understanding of how AI performs in resource-constrained environments with unique challenges such as poor connectivity, limited workforce capacity, and weak regulatory systems. Moreover, few studies have examined the ethical implications of AI deployment in these settings or evaluated practical strategies for sustainable and inclusive adoption. This gap highlights the need for context-specific research that addresses both the operational and ethical dimensions of AI integration in healthcare systems.
Conceptual Framework
This study adopts an integrated conceptual framework combining the TOE and Ethical AI frameworks to analyse AI adoption in Tanzania’s healthcare system. The TOE framework examines technological factors, organisational readiness, and environmental influences. Complementing this, the Ethical AI framework highlights fairness, accountability, transparency, and privacy, which are essential for addressing data security and bias concerns in low-resource settings.
These frameworks guided the research questions: questions on barriers and enablers align with the TOE dimensions, while ethical concerns are mapped to principles from the Ethical AI framework. This integration ensures a coherent structure linking the conceptual model to the study’s operational and ethical focus. Figure 1 illustrates the interaction between the TOE dimensions and ethical considerations shaping AI adoption in Tanzania’s healthcare system.
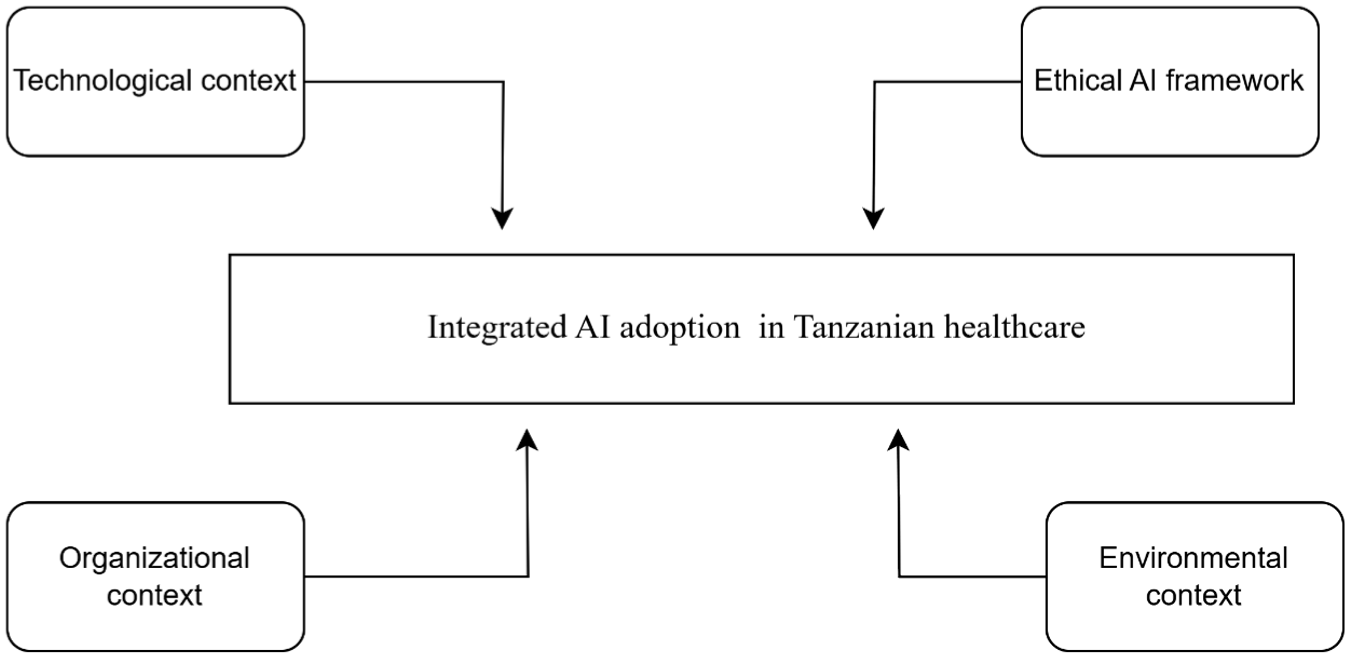
Integrated TOE and ethical AI framework for AI adoption in Tanzanian Healthcare.
Methodology
This study employed a qualitative multi-method design that integrated a systematic literature review with semi-structured interviews to explore the adoption, challenges, and ethical considerations of AI in Tanzania’s healthcare system. This dual approach enabled triangulation of insights from published research with the lived experiences of local stakeholders, ensuring a holistic understanding of the sociotechnical and ethical dimensions of AI integration in a resource-constrained setting.
Research Design
The study adopted a descriptive and exploratory design to provide an in-depth understanding of AI applications, challenges, and strategies in Tanzania’s healthcare context. This approach is especially relevant when the goal is to uncover patterns, generate insights, and explore under-researched areas without testing hypotheses (Creswell, 2014; Creswell & Clark, 2017; Creswell & Creswell, 2018; Yin, 2018). TOE and Ethical AI frameworks guided the analysis, enabling the integration of operational and ethical dimensions. This approach allowed the study to examine AI’s transformative potential while addressing systemic barriers and ethical concerns.
Data Collection
Two primary data sources were employed to investigate AI integration in Tanzania’s healthcare system: a systematic review of relevant literature and semi-structured interviews with key stakeholders. This dual-method strategy allowed triangulation of insights, combining theoretical evidence with real-world stakeholder experiences to ensure a comprehensive understanding of the technological, organisational, and ethical factors shaping AI adoption. A comparable approach was taken by Carnahan et al. (2023) in their cross-country study of electronic immunisation registry deployment in Tanzania, Vietnam, and Zambia, which similarly combined literature synthesis and qualitative interviews to cover implementation challenges and enablers.
Systematic Literature Review
A systematic literature review was conducted in alignment with PRISMA 2020 guidelines to identify and synthesise studies on AI applications in healthcare within low-resource settings, particularly Tanzania. The subsections below outline the search strategy, eligibility criteria, selection process, and data extraction methods used in the review.
Information Sources and Search Strategy
A systematic review of peer-reviewed and grey literature was conducted to explore AI applications in healthcare, particularly within low-resource settings such as Tanzania. The initial search covered publications from January 2010 to March 2024 to capture both foundational and recent studies. The databases searched included PubMed, IEEE Xplore, and Scopus, selected for their comprehensive coverage of biomedical, technical, and interdisciplinary research. The last search in this initial phase was conducted on March 20, 2024. Table 2 presents the search strings and Boolean operators used during this phase.
Search Strings Used in a Systematic Review.

Source. Authors’ work.
To enhance coverage and include emerging trends, an additional search was conducted in July 2025. This updated search expanded the scope to include Google Scholar and incorporated more specific AI-related terms such as machine learning, deep learning, decision trees, intelligent systems, and large language models. These refinements aimed to address limitations of the initial search by capturing studies using specialised terminology. The improved search strategy is shown in Table 3.
Updated Search String Used in July 2025.

Source. Authors’ work.
Eligibility Criteria
Studies were included in the review if they focussed on the application of artificial intelligence in healthcare systems and demonstrated relevance to resource-constrained settings, particularly developing countries. Eligible studies addressed systemic healthcare challenges, ethical considerations, or context-specific innovations related to AI integration. Initially, only studies published in English between 2010 and 2024 were considered. However, during the updated search conducted in July 2025, the inclusion window was extended to cover studies published up to June 2025 to incorporate the most recent evidence.
Both peer-reviewed journal articles and grey literature, such as government reports, policy briefs, and technical documents, were included to capture a comprehensive range of perspectives. With the expansion of search sources to include Google Scholar, additional screening was conducted to capture relevant academic theses, preprints, and institutional reports not indexed in traditional databases.
Studies were excluded if they focussed exclusively on high-income country contexts, lacked direct application to healthcare systems, or addressed AI use in non-healthcare domains. Furthermore, studies that presented insufficient methodological detail or did not offer empirical or conceptual insights applicable to developing countries were excluded. The updated screening process in July 2025 also involved reassessing borderline studies using the expanded search terms to ensure consistent application of these criteria.
Selection Process
All retrieved records were screened using a structured two-stage process. In the first stage, titles and abstracts were independently reviewed by two researchers to assess relevance based on the predefined inclusion criteria. Records that met the initial criteria were then subjected to full-text review in the second stage to confirm eligibility. Discrepancies between reviewers at any stage were resolved through discussion until consensus was reached. Duplicate records were identified and removed prior to screening to avoid redundancy and preserve the accuracy of the dataset. During the July 2025 update, the same selection procedure was applied to newly retrieved studies, ensuring consistency across both search phases.
Data Collection and Extraction Process
Data were extracted from the final set of included studies using a standardised data extraction form. Two reviewers independently extracted data to ensure accuracy. The extracted elements are outlined in Table 4.
Data Extracted from Included Studies.

Source. Authors’ work.
Data Items
The primary data items extracted from the included studies focussed on outcomes related to the effectiveness of AI in diagnostics, improvements in patient outcomes, healthcare system efficiency, and access to care. Additional variables included the types of AI tools utilised, the contextual setting (urban or rural), population demographics, and any reported ethical concerns. No automation tools were employed during data extraction, and no assumptions were made for missing or incomplete data.
Risk of Bias and Certainty Assessment
Given the qualitative and narrative nature of the included studies, formal risk of bias tools were not applied. However, each study’s methodological rigour and relevance to Tanzanian contexts were qualitatively assessed. The certainty of evidence was evaluated narratively, with attention to study design, context relevance, and reporting transparency.
Semi-Structured Interviews
Semi-structured interviews were conducted with a purposive sample of stakeholders, including healthcare practitioners, policymakers, and technologists actively engaged in AI-related healthcare initiatives in Tanzania. Participants were selected based on their expertise or direct involvement in the implementation, design, or regulation of AI technologies in healthcare. The sample ensured broad representation from urban and rural settings as well as from both government and technology sectors, capturing a diverse range of perspectives relevant to the Tanzanian context.
The interview guide was developed to align closely with the study’s research questions and the conceptual underpinnings of the TOE and Ethical AI frameworks, ensuring comprehensive coverage of technical, institutional, ethical, and regulatory dimensions (Appendix 1). Each interview lasted between 45 and 60 min and was conducted in either Swahili or English, depending on the participant’s preference. For Swahili interviews, professional translators facilitated interpretation, and bilingual experts verified all transcriptions to ensure accuracy and trustworthiness of translated responses.
Each interview was audio-recorded with the informed consent of participants, then transcribed verbatim and anonymised to protect confidentiality. Thematic saturation was used to guide the conclusion of data collection, and interviews were conducted until no new themes emerged, ensuring comprehensive coverage and depth across the identified topics.
Sampling and Study Population
The study targeted healthcare facilities and stakeholders with diverse expertise and experiences in AI and healthcare delivery. Participants included clinicians, administrators, government policymakers, and technologists. A purposive sampling approach was employed to select individuals directly involved in or knowledgeable of AI-related healthcare innovations. Participants were drawn from both urban and rural settings to ensure a comprehensive representation of Tanzania’s healthcare landscape. Initially, 25 individuals were interviewed. Following reviewer feedback and to strengthen rural representation, seven additional participants from remote healthcare facilities were interviewed via phone, resulting in a final sample of 32 participants. This approach enabled the inclusion of geographically dispersed voices and enhanced the contextual diversity of the findings.
Data Analysis
Thematic analysis was used to systematically analyse qualitative data collected from both the semi-structured interviews and the systematic literature review. This approach was chosen for its flexibility and capacity to provide a rich, detailed understanding of participants’ experiences and the contextual factors influencing AI adoption in healthcare. The analysis followed the six-phase process outlined by Braun and Clarke (2006), which allowed for a transparent and rigorous exploration of the data with the study’s objectives.
In the first phase (familiarisation), the researchers immersed themselves in the data by repeatedly reading interview transcripts and reviewing extracted literature notes to gain a comprehensive understanding of the content. In phase 2 (generating initial codes), key features of the data were systematically identified and coded using NVivo software, guided by the study’s theoretical lens (TOE and Ethical AI frameworks). Codes were applied both inductively from the data and deductively from predefined theoretical categories.
In phase 3 (searching for themes), codes were reviewed and grouped into potential themes that captured patterns across participants and literature sources. During phase 4 (reviewing themes), these candidate themes were refined by checking their coherence with the coded data and the entire dataset, ensuring internal consistency within themes and clear distinctions between them.
Phase 5 (defining and naming themes) involved clearly articulating the scope and essence of each theme, aligning them with the study’s conceptual dimensions: technological, organisational, environmental, and ethical. Lastly, in phase 6 (producing the report), the final themes were synthesised and interpreted with the research questions and broader literature, forming the basis of the findings presented in this study.
This structured process ensured the analysis was not only methodologically rigorous but also reflective of the complexity and diversity of perspectives on AI integration within Tanzania’s healthcare system.
Validity and Reliability
To ensure the reliability and validity of the study, multiple strategies were employed throughout the research process. Triangulation was used by integrating findings from both semi-structured interviews and a systematic literature review, enhancing the credibility and robustness of the results. Member checking was conducted with selected participants to confirm the accuracy and authenticity of interpreted data, thus strengthening the study’s confirmability. Additionally, inter-coder reliability checks were carried out during thematic analysis to verify consistency in coding across researchers. A clear audit trail was maintained to document analytical decisions, ensuring transparency and replicability. These combined strategies contributed to the overall trustworthiness of the findings, providing a rigorous foundation for interpreting the results.
Ethical Considerations
Informed consent was obtained from all participants, and confidentiality was maintained through anonymisation of data. Ethical principles were observed throughout, with attention to privacy, voluntary participation, and respect for participants’ views, especially regarding sensitive topics related to AI and healthcare.
Results
This study revealed several key insights into the adoption and integration of AI technologies within Tanzania’s healthcare system. The findings highlight both the transformative potential of AI and the critical challenges impeding its implementation. Consistent themes emerged across both the systematic literature review and semi-structured interviews, including technological limitations, organisational readiness, ethical considerations, and the broader need for enabling infrastructure and policy frameworks.
Literature Review Findings
Search Results
A systematic literature review was conducted using databases including PubMed, IEEE Xplore, Scopus, and Google Scholar to identify relevant studies on AI applications in healthcare, particularly within low-resource settings such as Tanzania. The search process followed the PRISMA 2020 guidelines (Page et al., 2021), which standardise the identification, screening, and inclusion of eligible studies.
The initial search, conducted between January and March 2024, yielded 120 articles. After removing duplicates and screening titles and abstracts for relevance, 15 studies were included based on eligibility criteria. Common reasons for exclusion included a lack of focus on healthcare-related AI, relevance only to high-income countries, or insufficient empirical or conceptual depth.
An additional search conducted in July 2025 expanded the scope to include Google Scholar and updated search strings incorporating specific AI-related terms such as machine learning, deep learning, intelligent systems, and large language models. Although this broader search initially returned over 98,000 results, after refining, de-duplicating, and applying the inclusion criteria, only nine additional studies were deemed eligible for inclusion.
In total, 24 studies were included in the final review. These comprised both peer-reviewed articles and grey literature that met the criteria for relevance, methodological clarity, and contextual alignment with healthcare challenges in low-resource settings. The full selection process is outlined in Figure 2, following the PRISMA flow diagram structure.
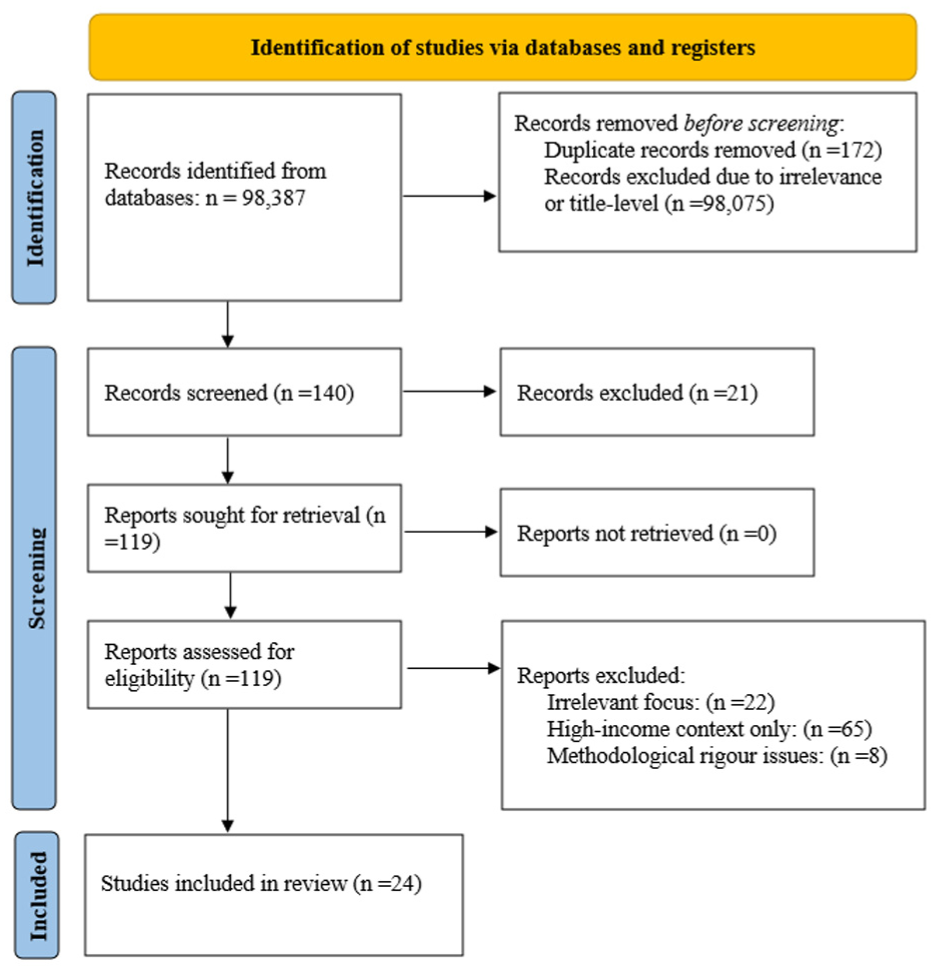
PRISMA flow diagram of article selection.
Study Characteristics
The 24 studies included in this systematic review provide a comprehensive overview of the landscape of AI applications in healthcare within low-resource settings. Thematically, these studies covered diverse AI use cases including diagnostic support, predictive analytics, telemedicine, remote patient monitoring, mental health, and electronic health records. Most studies were situated in sub-Saharan Africa, with a strong concentration in Tanzania. This geographic focus reflects the increasing prioritisation of digital health innovations in the region, particularly where health systems face chronic shortages in infrastructure, human resources, and timely diagnostics.
The majority of the studies were published between 2018 and 2025, highlighting a recent surge in interest corresponding with national digital health strategies, increased donor investments, and growing local research capacity. Approximately 10 of the studies were conducted exclusively in Tanzania, while others were distributed across the broader African continent or targeted developing countries more broadly (Figure 3). This trend underscores Tanzania’s emerging role as a testing ground for digital and AI-driven health solutions.
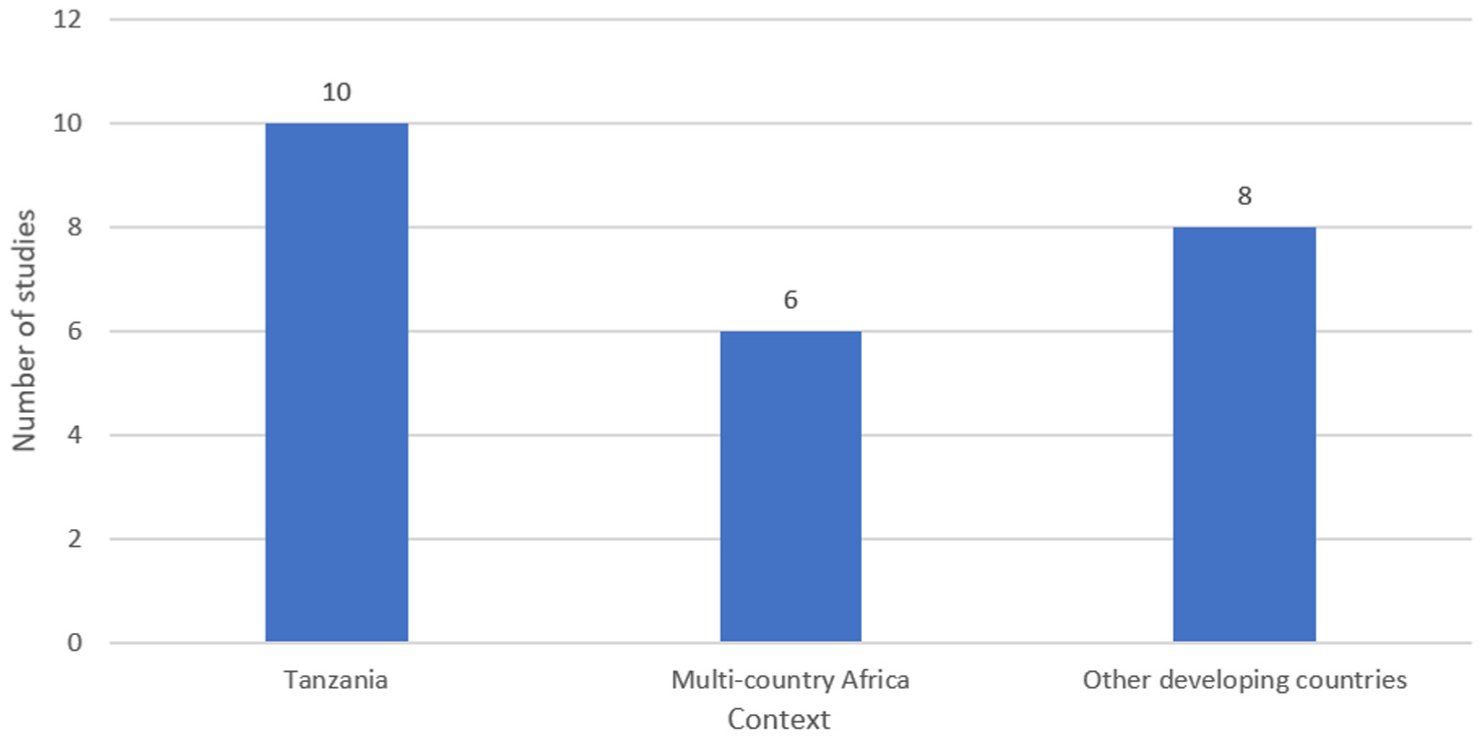
Geographic distribution of reviewed studies.
In terms of methodological approaches, qualitative case studies were the most common, accounting for 37.5% (nine studies) of the sample. These studies typically explored healthcare workers’ perceptions, organisational readiness, and ethical concerns, offering depth and contextual understanding in settings where AI adoption is still nascent. Mixed-methods designs comprised 25% of the studies, combining interviews, document analysis, and sometimes limited quantitative data to assess implementation processes. A smaller number of studies (4) used observational or pilot trial designs to assess early-stage AI tools in practice. Systematic and narrative reviews (3) helped consolidate existing knowledge, while two government or institutional reports provided grey literature insights on policy and implementation environments. The overall distribution of study designs is shown in Figure 4.

Distribution of study designs.
The dominance of qualitative and mixed-methods studies reflects the current maturity of AI in developing countries’ healthcare systems. With many technologies still in pilot or proof-of-concept phases, researchers have focussed on capturing experiential, ethical, and feasibility perspectives rather than evaluating large-scale impact aligning with broader global health research trends in developing countries, where qualitative research plays a crucial role in illuminating social, organisational, and infrastructural barriers to technology adoption before quantitative scaling becomes viable.
Together, these study characteristics highlight a rapidly evolving field where research is beginning to inform policy and practice. The growing volume of Tanzanian studies, especially those targeting ethical implementation and rural health equity, suggests fertile ground for longitudinal, and impact-oriented research shortly. Table 5 summarises the characteristics of the reviewed studies.
Study Characteristics from the Literature Review.

Source. Authors’ synthesis.
Key Findings from the Literature Review
The analysis of 24 studies revealed five central themes relating to how AI is currently applied, challenged, and positioned within healthcare systems in low-resource settings. These themes are discussed below, with specific examples drawn from the reviewed literature and comparisons across different countries and healthcare systems.
AI in Diagnostics and Disease Prediction
AI technologies are increasingly deployed to support disease diagnosis and forecasting in developing countries. Leo et al. (2019) developed a machine learning model for cholera prediction in Tanzania, achieving a balanced accuracy of 0.767 ± 0.09. Similarly, Guo and Li (2018) reported that rural clinics in China using AI for tuberculosis diagnosis saw improved turnaround times and reduced diagnostic errors, even in settings with limited clinical expertise. These applications demonstrate AI’s value in extending diagnostic capacity in underserved areas, particularly where laboratory infrastructure is minimal.
Infrastructure and Integration Constraints
A recurrent theme across the studies was the inadequacy of digital infrastructure. Multiple Tanzanian and African studies (Kondo et al., 2025; Mbunge & Batani, 2023) highlighted persistent barriers such as intermittent electricity, poor internet connectivity, and fragmented health information systems. These infrastructural deficits were noted to impede even the most promising AI tools, leading to underutilisation or abandonment post-pilot. As one policymaker described it, “We have AI tools… but without infrastructure, they are like cars without roads” (Kondo et al., 2025).
Workforce Capacity and Training Needs
The readiness of healthcare workers to use AI emerged as a critical success factor. Several studies, including Mwogosi, Mambile et al. (2025) and Kitole and Shukla (2024), reported low levels of digital literacy and minimal AI-specific training. The findings from the study by Mwogosi, Mambile et al. (2025) indicate that only 28% of clinicians felt confident operating AI-supported systems without supervision. Comparative studies from countries like Rwanda and South Africa (Kondo et al., 2025) found higher digital competence among health workers, attributed to national investment in health IT training. These contrasts underscore the importance of long-term, context-specific capacity-building in AI integration.
Ethical Challenges and Trust Deficits
Concerns around bias, fairness, data privacy, and lack of explainability were central to the ethical discourse in reviewed studies. Kumbo et al. (2024) and Schmude et al. (2022) found that AI models trained on non-African datasets risked generating inappropriate outputs, eroding clinical trust. Weak regulatory oversight and unclear consent processes were also noted as gaps in AI deployments (Owoyemi et al., 2020). One Tanzanian official remarked, “We cannot trust systems that do not understand our people,” reflecting broader scepticism among users in the absence of transparent and inclusive design.
Fragmented Implementation and Limited Scale-Up
Despite the promise of AI in pilot settings, most implementations lacked continuity and institutional integration. Cleland et al. (2024) reported that AI-assisted diabetic retinopathy screening in Tanzania was clinically effective but stalled due to unclear ownership and limited integration with national systems. Similar findings were echoed by Onsongo and Kagotho (2024), who noted that donor-driven pilots often failed to transition into long-term strategy due to the absence of funding alignment and government coordination. This fragmentation limits the scalability of AI innovations and reinforces dependency on external support.
These thematic findings are further consolidated in Table 6, which presents a structured synthesis of the reviewed studies across core domains, including AI applications, benefits, barriers, and ethical concerns. The table demonstrates strong convergence across studies in sub-Saharan Africa, particularly Tanzania, regarding the utility of AI in diagnostics and decision-support, the infrastructural and literacy-related obstacles to implementation, and the persistent ethical risks related to bias, data security, and trust. It also highlights the breadth of applications ranging from mental health to disease prediction captured in the literature (Ansah et al., 2024; Guo & Li, 2018; Kondo et al., 2025; Mbunge & Batani, 2023; Mwogosi, 2025a, 2025b; Mwogosi, Mambile et al., 2025; Mwogosi, Simba et al., 2025; Shidende & Mwogosi, 2025).
Principal Literature Results.

Source. Authors’ work.
Semi-Structured Interview Results
Participant Demographics
A total of 32 participants were interviewed through semi-structured sessions, including in-person and phone-based interviews. The sample consisted of healthcare practitioners, policymakers, and technologists, purposefully selected to capture diverse insights from both urban and rural healthcare environments. The added participants from rural areas were included to address previous limitations in geographic representation and ensure more balanced perspectives on AI adoption challenges in Tanzania’s healthcare system. Table 7 provides a demographic breakdown by professional group, gender, and setting.
Participant Demographics.

Source. Authors’ work.
Thematic Analysis of Interview Data
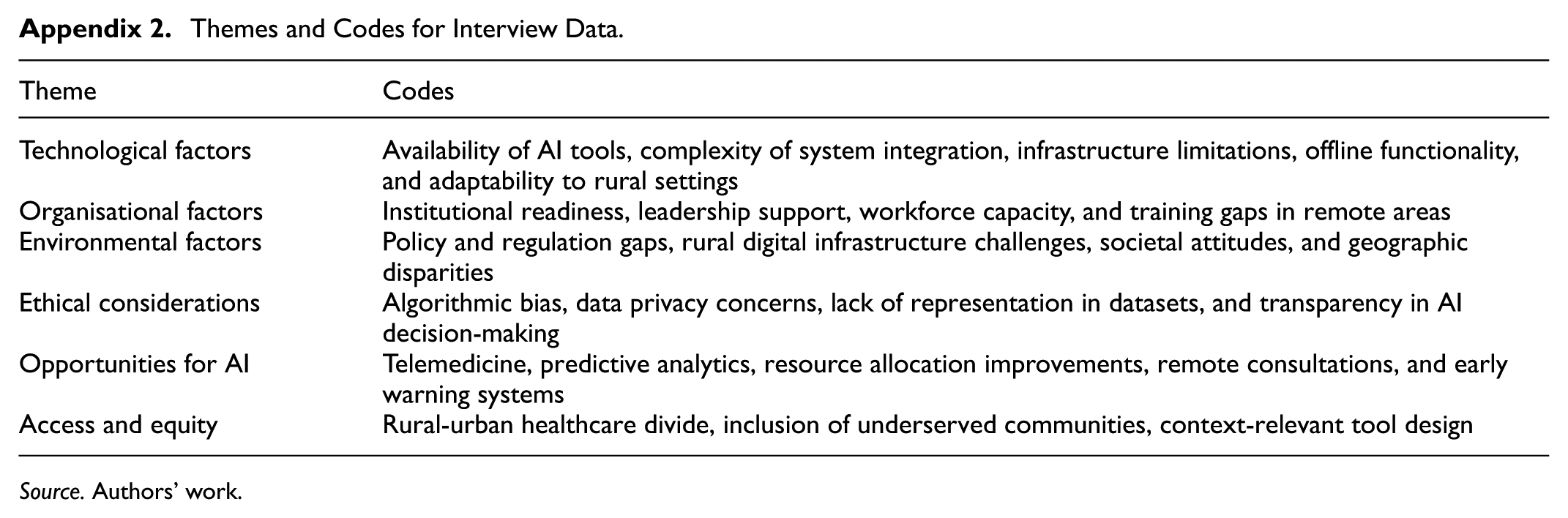
Thematic analysis identified a range of key themes emerging from the interviews, guided by the TOE and Ethical AI frameworks. The inclusion of seven additional participants from rural healthcare settings enriched the dataset by offering deeper insights into on-the-ground challenges and opportunities specific to remote areas. As a result, some themes were further detailed, and additional subthemes, particularly related to rural digital exclusion, contextual usability of AI tools, and equity in healthcare access, were identified and integrated within the existing categories. Table in Appendix 2 summarises the major themes and corresponding codes derived from the full sample of 32 interviews.
To visually represent the frequency and prominence of recurring concepts from the interview data, a word cloud diagram (Figure 5) was generated. The diagram highlights dominant terms such as “infrastructure,”“rural,”“remote,”“gaps,” and “AI,” which reflect central themes discussed by participants, particularly following the inclusion of rural perspectives. Words like “training,”“readiness,”“policy,”“disparities,” and “privacy” also appear frequently, pointing to systemic challenges and concerns around equitable AI implementation. This visualisation reinforces the emphasis placed on contextual barriers and the need for personalised, inclusive strategies in AI adoption across underserved healthcare settings.

Word cloud of key terms.
Technological Factors
Several technological factors, including infrastructure readiness, system compatibility, and digital literacy among healthcare workers, influence the adoption of AI technologies in Tanzania’s healthcare system. While urban facilities and national programmes have begun integrating digital tools, rural settings continue to face noticeable limitations that affect the scalability and equity of AI deployment.
Initiatives such as Afya-Tek in Kibaha District reflect growing momentum in Tanzania’s digital health landscape. However, AI adoption remains more advanced in urban areas, where infrastructure and technical support are relatively stronger. In contrast, some rural facilities still rely on paper-based systems or basic digital tools. A community health worker noted, “We now have digital tools in some areas, but they are not yet available in many remote facilities where they are most needed.” Another added, “In our facility, we still use normal reports. We have heard about AI systems, but we have not interacted with them yet.”
The complexity of some AI solutions also presents a challenge for integration into routine practice, particularly where users are less familiar with digital technologies. As one nurse from a regional hospital explained, “AI systems are not designed with our context in mind, and we struggle to adapt them to the realities of our healthcare settings.” A rural medical officer added, “We need tools that are easy to use and match our workflow. If they are too technical, they sit unused.”
Tools like Afya AI and Akili AI, which aim to support diagnosis and chronic disease management, are promising, but their full potential depends on training and contextual adaptation. As highlighted by a clinician, “The tools are useful, but many staff do not feel confident using them without guidance.”
Infrastructure remains an important consideration. While many regions have improved connectivity and power reliability, some rural areas still face occasional internet or electricity disruptions, which can affect the performance of AI-dependent systems. One district health officer observed, “We have internet most of the time, but there are still moments when it is slow or unstable. That can interfere with telemedicine.” Another remarked, “Power cuts do not happen daily, but when they do, they delay services that rely on digital tools.”
Organisational Factors
Organisational readiness is a critical determinant of how successfully AI technologies can be integrated into healthcare institutions in Tanzania. Key factors such as leadership commitment, staff capacity, training availability, and institutional alignment with digital health goals all shape the pace and sustainability of AI adoption.
Healthcare institutions vary widely in their readiness. Urban hospitals, particularly national and regional referral centres, are generally more advanced in their use of digital tools and have greater exposure to AI-related pilot initiatives. For example, at facilities like Muhimbili National Hospital, foundational digital infrastructure is in place, creating entry points for AI experimentation. In contrast, many district and rural clinics are still building core digital capacity and lack dedicated frameworks to support emerging technologies. A hospital administrator in Dar es Salaam commented, “In our facility, we have started using digital tools, but the transition to AI feels far off without a clear institutional roadmap.”
Leadership plays an influential role in shaping institutional readiness. Facilities with supportive and proactive leadership are more likely to invest in digital innovation, mobilise staff engagement, and advocate for training and resource allocation. A health officer from a regional facility observed, “Our leaders prioritise basic health services, which is understandable, but it means AI remains a low priority even when it could address some of our challenges.” On the other hand, in some rural facilities, leadership involvement in digital initiatives was described as inconsistent or limited. One rural nurse noted, “Sometimes we hear about digital health goals at national meetings, but they are not followed up at the facility level.” This gap suggests the need for more structured and decentralised leadership support to translate national strategies into actionable local plans.
Workforce capacity also emerged as a key organisational barrier. While healthcare workers often recognise the potential benefits of AI tools, many lack the skills and confidence to use them effectively. A clinician from Kibaha District stated, “We have seen how digital tools can improve our work, but most of us do not know how to use them effectively because training is either insufficient or non-existent.” This concern was echoed by a rural medical officer who said, “When systems are introduced, they do not come with enough hands-on training. That is why some of them go unused.”
Limited access to continuing professional development, particularly in remote areas, contributes to uneven digital readiness across the health workforce. Several rural participants expressed the need for regular, context-relevant training that aligns with their daily responsibilities. One nurse remarked, “If AI tools are to help us, they must be introduced in steps, and we need refresher training, not just a one-time session.”
Environmental Factors
Environmental factors, including government policy direction, digital infrastructure, and societal attitudes, substantially influence the integration of AI technologies in Tanzania’s healthcare system. These external conditions can either enable or hinder efforts to implement and scale digital innovation.
The Tanzanian government has demonstrated growing interest in AI through national policy instruments such as the Health Sector Strategic Plan and the Digital Health Strategy. However, while these frameworks promote digital transformation in general, they often lack AI-specific implementation guidance. As one policymaker stated, “Our policies mention digital health broadly, but there is little focus on AI-specific strategies. This gap limits coordinated efforts for implementation.” In the absence of detailed, actionable policies, many healthcare facilities are left to interpret and pursue AI integration on their own, resulting in fragmented progress.
Infrastructure readiness remains a decisive factor, especially when comparing urban and rural settings. Urban healthcare facilities are more likely to have access to stable internet, reliable power supply, and digital hardware, positioning them better for piloting and sustaining AI systems. In contrast, some rural clinics continue to face intermittent connectivity and power challenges, which restrict the functionality of even basic digital tools. A regional IT manager noted, “We have tried using telemedicine, but interruptions in power and internet make it difficult to provide reliable services.” Similarly, a rural clinician added, “We are willing to try new tools, but if the system goes down when the internet drops, it creates frustration.”
Despite ongoing efforts to improve national digital infrastructure, these disparities suggest the need for targeted, region-sensitive investments, particularly in remote and underserved areas. Solutions such as low-bandwidth platforms and offline-capable AI tools could bridge existing gaps, ensuring continuity of care even in lower-connectivity environments.
Societal perceptions and public trust also shape the adoption environment. Awareness of AI technologies in healthcare is still emerging, and in many cases, community members and some frontline staff express uncertainty about their reliability and implications. A healthcare worker remarked, “There is a lack of trust in AI because people do not understand it. People often ask, ‘Can the machine know better than a doctor?’” Another participant shared, “Some think AI might replace their jobs or make mistakes that no one can correct.”
Ethical Considerations
Ethical considerations are central to the successful and equitable adoption of AI in Tanzania’s healthcare system. Key concerns include data privacy, algorithmic bias, and transparency in AI decision-making, each with significant implications for trust, fairness, and long-term sustainability.
One of the most pressing issues raised by participants is the protection of patient data. Although Tanzania is making progress towards formalising data protection policies, legal and regulatory frameworks for AI-specific data governance remain limited. Healthcare workers voiced concerns about the security of sensitive patient information used by AI systems. A nurse in a regional hospital shared, “We know the systems can help, but we worry about where the patient data goes and whether it will be kept safe.” These concerns are particularly pronounced in rural settings, where understanding of data handling protocols is often limited, and regulatory oversight may be weaker. Addressing these issues requires robust, context-relevant data protection policies aligned with international standards, as well as capacity building in data stewardship.
Another ethical challenge relates to algorithmic bias, especially when AI tools are trained on datasets that do not represent the Tanzanian population. Such bias can result in reduced diagnostic accuracy or inappropriate clinical recommendations, particularly for underrepresented groups. A health informatics officer noted, “AI tools trained on foreign data do not always work well here. We need solutions that understand our local context.” These observations underscore the importance of developing and validating AI models using locally sourced, diverse datasets that reflect the demographic and epidemiological realities of Tanzanian communities.
Transparency or the lack thereof in AI decision-making processes is also a source of concern. Several participants highlighted the difficulty of trusting AI-generated outputs without understanding the rationale behind them. A doctor in Dar es Salaam commented, “If the system gives a diagnosis, we need to understand how it reached that conclusion. Otherwise, it is hard to rely on it.” This sentiment was echoed by rural clinicians who noted that unfamiliar tools without clear explanations often lead to hesitation in clinical use. Enhancing the explainability of AI systems through user-friendly interfaces, visual decision aids, or clinical reasoning explanations is essential for promoting accountability and user confidence.
More broadly, there is a need to embed ethical safeguards into both the design and deployment phases of AI implementation. It includes clear consent procedures, community engagement, and ethical review processes that reflect local cultural and healthcare contexts. As one rural health officer stated, “People need to know what AI is doing and why it matters. Otherwise, they will not accept it, even if it works well.”
Opportunities for AI Adoption in Tanzania’s Healthcare System
AI presents a range of promising opportunities for strengthening Tanzania’s healthcare system. Its potential extends beyond technological efficiency to address systemic challenges, including limited specialist availability, inefficient resource management, and delayed disease detection, especially in underserved and rural areas.
One of the most immediate opportunities lies in AI-enhanced telemedicine. In settings where healthcare professionals are scarce, especially in rural regions, AI-powered systems support remote consultations, diagnoses, and treatment recommendations. These tools help reduce the need for patients to travel long distances to access specialist care. A community health worker from a rural facility explained, “With AI supporting telemedicine, we can connect to doctors in the city for advice, which saves time and reduces the burden on the local clinic.” AI-supported teleconsultation platforms can also assist frontline workers by integrating decision-support features, improving diagnostic accuracy and promoting timely intervention.
AI’s capacity for predictive analytics offers another valuable opportunity in Tanzania’s healthcare context. By analysing large and complex datasets, AI can forecast trends in infectious diseases like malaria, tuberculosis, and cholera, as well as support long-term management of chronic conditions such as hypertension and diabetes. A health informatics officer shared, “AI tools can help us predict the spread of diseases and allocate resources more efficiently. This predictive power is invaluable, especially during outbreaks.” These capabilities enable health planners and frontline providers to take proactive measures such as pre-positioning supplies, targeting interventions, and mitigating risks before they escalate into emergencies.
AI also holds great promise in streamlining resource management within healthcare facilities. In resource-constrained environments, inefficiencies in medicine supply chains, workforce scheduling, and patient flow can significantly impact service delivery. AI tools can help monitor inventory, optimise staff allocation, and improve patient triage systems. As one healthcare manager explained, “AI can help hospitals track resources like medicines and staff time, ensuring they are used where they are most needed.” Such efficiency gains not only enhance clinical operations but also reduce waste and operational costs, making healthcare systems more responsive and sustainable.
Moreover, AI has the potential to improve data-driven decision-making at multiple levels of the health system. From national health policy to facility-level planning, the integration of AI analytics can offer timely insights into patient outcomes, service utilisation, and performance metrics, contributing to more informed, agile, and accountable healthcare delivery.
Discussion
This study offers a grounded and theory-informed exploration of the opportunities and constraints in integrating AI into Tanzania’s healthcare system. By triangulating data from a systematic literature review and semi-structured interviews with healthcare professionals, technologists, and policymakers, the study identifies recurring challenges and enablers across technological, organisational, ethical, and policy dimensions. These findings not only confirm but also extend existing scholarship on digital innovation in low-resource settings, offering context-sensitive insights attached in the TOE and Ethical AI frameworks.
Technological Constraints
Technological limitations emerged as a consistent barrier across both the literature and stakeholder narratives. The literature widely documents challenges such as inadequate digital infrastructure, limited availability of localised health data, and the absence of context-appropriate tools (Ansah et al., 2024; Mbunge & Batani, 2023; Owoyemi et al., 2020; Schmude et al., 2022). Interview participants echoed these concerns, particularly highlighting unreliable internet access, frequent power outages, and low digital literacy in rural settings, conditions that severely constrain AI deployment. These findings align with Guo and Li (2018), who argue that AI systems developed for high-bandwidth, data-rich environments often fail in developing countries due to mismatched assumptions about local infrastructure and usability.
However, few reviewed studies systematically evaluated the performance of AI tools under these constrained conditions. Most relied on qualitative observations or pilot outcomes, limiting generalisability and making it difficult to assess long-term effectiveness. There is also limited discussion in the literature about how tools like Afya AI or Akili AI, referenced by interviewees, have been adapted for local contexts or tested for resilience in offline or low-resource settings. It signals a critical gap in operational research on AI adaptation in developing countries.
Organisational Readiness
Organisational readiness, as articulated in the TOE framework, was found to be a major determinant of AI adoption. The literature highlights the importance of leadership commitment, staff training, and digital infrastructure as prerequisites for successful integration (Emani et al., 2021; Wahl et al., 2018). This study reinforces those factors but reveals sharp disparities between urban and rural institutions. While referral hospitals in urban centres exhibit relative digital maturity and have piloted some AI applications, many rural facilities lack even the basic building blocks, such as EHR systems or IT support, needed to adopt advanced technologies.
Interview data suggest that leadership gaps, unclear strategic direction, and fragmented institutional priorities exacerbate these disparities. Many rural health facilities lack internal champions or managerial bandwidth to drive AI innovation, leading to passive or sporadic engagement with digital initiatives. This finding exposes a limitation in the literature, which often assumes that organisational structures are uniformly prepared to adopt AI, without sufficiently interrogating subnational disparities or governance bottlenecks.
Ethical Concerns
Ethical concerns around AI, including data privacy, algorithmic bias, and lack of transparency, were widely cited in both the literature and field interviews. The Ethical AI framework (Floridi & Cowls, 2019) highlight these dimensions as foundational to responsible innovation. However, while theoretical discussions in the literature tend to emphasise global norms and principles (Mennella et al., 2024), this study brings forth more urgent, context-specific concerns from Tanzanian stakeholders.
Interviewees raised fears about job displacement, mistrust of machine-generated decisions, and the opacity of AI recommendations. Some also noted weak legal protections for patient data, which heightens the risk of misuse or loss of public trust. These concerns suggest that ethical AI deployment must go beyond technical design and include robust, locally informed regulatory frameworks and inclusive community engagement processes. Notably, few empirical studies reviewed examined how ethical safeguards are operationalised on the ground, indicating a major implementation research gap in developing countries’ contexts.
Policy and Governance
The literature and interview data also converge around the absence of coherent, AI-specific policy frameworks in Tanzania. While the Tanzania Digital Health Strategy and policy guidance on AI exist, they remain high-level and poorly integrated into local health systems (Mwogosi & Simba, 2025). Interview participants noted that implementation is often fragmented, donor-driven, and lacks alignment with national health goals. Moreover, frontline workers and facility-level managers are rarely involved in digital planning processes, further weakening institutional ownership.
This governance gap reflects a broader critique in digital health literature: many developing countries have embraced digital health strategies rhetorically but lack the technical capacity, inter-sectoral coordination, and regulatory infrastructure to implement them effectively. This top-down model risks reproducing digital divides, especially between urban and rural health systems, and limits the sustainability of otherwise promising pilot interventions.
Optimism and Opportunity
Despite these challenges, stakeholders consistently expressed optimism about the transformative potential of AI, particularly in augmenting diagnostic capacity, reducing provider workload, and improving care delivery in underserved regions. Both literature and interviews point to successful use cases in telemedicine, predictive analytics, and AI-assisted diagnostics (Kitole & Shukla, 2024; Mbunge & Batani, 2023). Mobile-first and offline-capable AI solutions were especially valued for their scalability in low-bandwidth environments.
However, this optimism is often contingent on critical enablers: strong leadership, inclusive design, ethical safeguards, and sustained capacity-building. These factors must be central to any AI implementation roadmap in Tanzania, lest AI replicate the inequities it promises to solve. Furthermore, this study calls for a shift from pilot-focussed research to longitudinal and impact evaluations that assess AI’s real-world contributions to health system resilience, equity, and efficiency.
Integrating Evidence and Theory
By combining literature and lived experiences, this study advances a more grounded understanding of how both macro-structural constraints and micro-level realities shape AI adoption. Table 8 synthesises these findings thematically, drawing clear links between global evidence and the Tanzanian experience. This integration reinforces the value of applying both the TOE and Ethical AI frameworks to inform implementation strategies that are not only technically sound but also contextually and ethically appropriate.
Synthesis of Literature and Empirical Findings on AI Adoption in Tanzanian Healthcare.

Source. Authors’ work.
Together, these insights reaffirm that AI alone cannot fix underperforming health systems. However, with targeted investments in infrastructure, governance, and human capital, AI can serve as a catalytic enabler of health system transformation provided it is approached with caution, inclusivity, and long-term commitment.
Study Implications
This study contributes important insights into the dynamics of AI adoption in low-resource healthcare settings, particularly through a context-grounded, stakeholder-informed analysis. The implications of these findings span practical application, theoretical development, societal transformation, and policy reform.
Practical Implications
This study highlights the need for AI tools that are tailored to low-resource environments, offline-capable, mobile-friendly, and easy to use by healthcare providers with varying levels of digital literacy. Technologists must engage end-users in design processes, while implementers should prioritise training, mentorship, and feedback loops to build confidence and ensure effective use of AI in routine clinical practice.
Theoretical Implications
By applying the TOE and Ethical AI frameworks, this study demonstrates the value of integrating structural and normative lenses in examining digital health adoption. It challenges technology adoption models that assume digital readiness and suggests expanding theoretical models to better account for contextual, ethical, and institutional variations in developing countries’ health systems.
Societal Implications
AI holds promise for improving healthcare access and reducing diagnostic delays, particularly in rural areas. However, concerns over job displacement and mistrust in AI highlight the need for transparent communication, ethical safeguards, and public engagement. Stakeholders must ensure AI is introduced as a supportive, not replacement, tool to sustain community and workforce trust.
Policy Implications
The findings reveal a policy-practice gap in AI integration, with top-down strategies lacking operational clarity and local involvement. Policymakers should develop AI-specific guidelines, strengthen data protection laws, and empower regional health actors to adapt national frameworks to local contexts, ensuring AI adoption is ethical, inclusive, and sustainable.
To address workforce readiness, we recommend the establishment of a national “AI-for-Healthcare Academy” to deliver practical, context-specific training for healthcare providers. Embedding such training into national policy frameworks would strengthen digital capacity and support ethical, sustainable AI integration across diverse healthcare settings.
Study Limitations
While this study offers valuable insights into AI integration in Tanzania’s healthcare system, several limitations should be acknowledged. First, the qualitative design, though rich in contextual depth, limits the generalisability of findings. Stakeholder selection, while purposive and diverse, may still reflect bias, particularly an overrepresentation of urban perspectives. Future studies should aim for broader geographic and sectoral inclusion, including patient and private-sector voices. Second, the study did not include quantitative measures of AI’s actual impact on healthcare outcomes, which limits the ability to assess effectiveness and scalability. Third, the literature review excluded non-English and some grey literature, potentially omitting regionally relevant insights. Lastly, methodological heterogeneity across included studies complicated direct comparison and synthesis. Future reviews should adopt broader inclusion criteria, integrate grey literature, and apply synthesis techniques suited for diverse study designs. Despite these constraints, the study’s triangulated approach provides a strong foundation for guiding ethical and context-sensitive AI implementation in similar settings.
Conclusion
This study offers a distinctive contribution to the AI-healthcare discourse by presenting a contextually grounded analysis of AI adoption in Tanzania, integrating both empirical evidence and theoretical perspectives. Unlike prior research that often frames AI implementation in low-resource settings primarily as a technical issue, this study brings to light the complex interplay of infrastructural, organisational, and ethical factors that influence real-world integration. By combining stakeholder insights with the TOE and Ethical AI frameworks, the study provides a comprehensive lens through which to understand the multifaceted nature of AI adoption in a healthcare system characterised by resource constraints and systemic disparities.
To support ethical, inclusive, and sustainable AI implementation, the study recommends coordinated action across key stakeholder groups. Policymakers should prioritise the development of AI-specific health strategies that move beyond high-level vision statements to include clear implementation pathways, ethical safeguards, and mechanisms for accountability. These strategies must also be decentralised to reflect local realities and should invest in digital infrastructure, data governance, and workforce readiness.
Healthcare practitioners play a central role and should be actively involved in the co-design and iterative feedback processes that shape AI tools, ensuring that they align with clinical workflows and operational demands. Equally important is the need for continuous professional development and support systems that build digital literacy and promote confidence in using AI-assisted technologies.
Technologists and AI developers must shift their focus towards designing tools that are functionally robust in low-connectivity, low-bandwidth environments. Solutions must be developed using local datasets, incorporating fairness, transparency, and explainability to build trust among both users and patients.
For researchers, there is a clear need for longitudinal and implementation-focussed studies that go beyond technical performance to examine ethical impacts, social acceptability, and system-level outcomes. Interdisciplinary research that integrates clinical, technical, and social science perspectives will be essential for capturing the full complexity of AI in health systems.
Ultimately, aligning innovation with equity and technology with trust is essential. When guided by inclusive frameworks, ethical principles, and participatory design, AI can serve as a powerful catalyst for strengthening health systems in Tanzania and similar low-resource contexts.
Footnotes
Appendix
Themes and Codes for Interview Data.
| Theme | Codes |
|---|---|
| Technological factors | Availability of AI tools, complexity of system integration, infrastructure limitations, offline functionality, and adaptability to rural settings |
| Organisational factors | Institutional readiness, leadership support, workforce capacity, and training gaps in remote areas |
| Environmental factors | Policy and regulation gaps, rural digital infrastructure challenges, societal attitudes, and geographic disparities |
| Ethical considerations | Algorithmic bias, data privacy concerns, lack of representation in datasets, and transparency in AI decision-making |
| Opportunities for AI | Telemedicine, predictive analytics, resource allocation improvements, remote consultations, and early warning systems |
| Access and equity | Rural-urban healthcare divide, inclusion of underserved communities, context-relevant tool design |
Source. Authors’ work.
Acknowledgements
The author extends sincere gratitude to the University of Dodoma for its invaluable support and resources that made this research possible.
Ethical Considerations
This study received ethical clearance from the relevant Tanzanian ethics board. All participants provided informed consent prior to participation, and confidentiality was strictly maintained throughout data collection and analysis.
Consent to Participate
All participants were informed of the purpose and scope of the research and gave verbal and/or written consent prior to the interviews. No patient data or sensitive clinical records were used.
Author Contributions
Augustino Mwogosi conceptualised the study, conducted the data collection and analysis, and prepared the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available upon reasonable request and have been anonymised to protect participant confidentiality.