
Abstract
Domestic abuse (DA) is often overlooked in primary care, despite primary care’s pivotal role. While screening improves early detection, it is not standard in primary care. This cross-sectional study aimed to assess the potential integration of a brief DA screening tool into primary care and explore the association between abuse history and WAST-Short score, controlling for demographics in Northwest London. An e-Survey with 29 items, translated into 18 languages, was sent to eligible NHS patients (aged 18 years and older) identified by general practices between 3 March and 7 October 2022 via SMS. It included questions about DA experiences, with the WAST-Short screening questionnaire used to assess tension in relationships and difficulty resolving arguments. Regression analysis examined the relationship between WAST-Short score and abuse history. Seventeen general practices participated, with 6,967 patients clicking the survey link and 4,253 (61%) completing it. Nearly half reported DA experiences, while 6.1% declined disclosure. After adjusting for age, gender and ethnicity, the multivariable logistic regression models revealed that higher WAST-Short score were associated with higher odds of disclosing history of abuse and higher odds of refraining from disclosing abuse history. This study underscores the potential of DA screening in primary care, particularly for those hesitant to disclose abuse. The WAST-Short tool offers a non-intrusive means of early identification. However, successful implementation requires adequate training and resources for primary care practitioners.
Introduction
Domestic abuse (DA) is a pervasive public health issue with serious, lasting impacts on health and well-being (Addis & Snowdon, 2023; Sivarajasingam et al., 2022; World Health Organization [WHO], 2021). Defined as abusive, coercive, or controlling behaviour between adults who are or have been intimate partners or family members (Domestic Abuse Act 2021, c. 17), DA affects individuals worldwide, leading to chronic physical conditions and mental health disorders such as depression, anxiety, and suicidality (Devries et al., 2013; Kirk & Bezzant, 2020; Oram et al., 2014). Survivors often suffer from multiple comorbidities and, as a result, visit primary care and emergency settings at higher rates than individuals without a history of abuse (Kirk & Bezzant, 2020).
DA disproportionately affects women and children, with pregnancy posing unique risks, including maternal and fetal complications (Aliasghari et al., 2024; Manandhar et al., 2024; Sabri et al., 2024). Women with mental health disorders are especially vulnerable, facing increased risks of suicide, substance abuse, and family disruptions (Salahi et al., 2018; WHO, 2021). Female survivors experience higher rates of perinatal depression and anxiety, with elevated occurrences of depression, PTSD, and somatisation linked to DA (Maharaj et al., 2010; WHO, 2021).
Childhood exposure to DA is associated with an increased risk of experiencing or perpetrating violence in adulthood (Rariden et al., 2021; WHO, 2021). Additionally, psychiatric conditions such as depression, generalised anxiety, and panic disorder correlate with an increased risk of violent behaviour, emphasising the importance of healthcare professionals (HCPs) addressing DA in routine assessments (Oram et al., 2014). Despite its prevalence, DA remains significantly underreported within healthcare systems. In the UK, approximately 1 in 5 adults reports experiencing abuse since age 16 (Elkin, 2022), though this likely underestimates the true scale of the problem (Office for National Statistics, 2023).
HCPs, particularly in primary care, play a critical role in the early detection and intervention of DA (Royal College of Nursing, 2020; WHO, 2021). General practitioners often encounter patients with chronic pain, gynaecological issues, or mental health concerns that may signal abuse. However, due to barriers such as lack of training or fear of offending, direct questioning about DA is uncommon. Studies suggest that survivors are often open to being asked about DA but rarely disclose it without direct prompting, due to embarrassment or fear (Kirk & Bezzant, 2020; Robinson & Spilsbury, 2008).
Cultural norms can significantly impact DA disclosure. In some cultures, abuse may be normalised, or family privacy highly valued, deterring individuals from reporting abuse (Habib et al., 2024; Manandhar et al., 2024). Additionally, stigma, judgment, financial concerns, and fear of social isolation further discourage disclosure, especially in primary care settings (Naveed et al., 2022; Sivarajasingam et al., 2022). The criminal justice system’s approach can also affect disclosure rates; bureaucratic or culturally insensitive processes may deter survivors from seeking help (Martitah et al., 2024).
Clinicians face challenges when discussing DA, such as limited training, concerns about privacy and confidentiality, and the lack of effective interventions (Kirk & Bezzant, 2020; Qasem et al., 2013). Research suggests that training, integrated referral pathways, and system-level support can improve detection and referral rates (Feder et al., 2011; Keynejad et al., 2022; Sohal et al., 2020; WHO, 2021). However, despite training, many clinicians remain hesitant to address DA, and a global meta-analysis revealed that 42% of female clinicians were themselves survivors of DA, highlighting potential biases and sensitivities among HCPs (Dheensa et al., 2022).
The Domestic Abuse Act 2021 (Home Office, 2021) and WHO guidelines emphasise the health sector’s responsibility to support DA survivors. In the UK, NICE guidelines (National Institute for Health and Care Excellence, 2016) recommend DA enquiries only when clinical indicators are present, rather than using routine screening with validated tools. This reliance on clinical judgment can lead to missed opportunities to identify and support DA survivors. In contrast, the U.S. Preventive Services Task Force takes a more proactive approach, advocating for routine screening in primary and prenatal care settings (Feder, 2016).
Research shows that proactive DA screening improves detection rates, especially among individuals who may be hesitant to disclose abuse in societies where social norms discourage open discussion of DA (Hegarty et al., 2021; Manandhar et al., 2024; O’Doherty et al., 2015). Effective screening among pregnant and postpartum women is especially crucial, as it addresses the health of both mother and child (Hegarty et al., 2021; O’Reilly & Peters, 2018). Screening has become even more essential as remote consultations – common after the COVID-19 pandemic – limit clinicians’ ability to observe non-verbal cues. Emerging digital and AI-based technologies present novel opportunities for DA identification in this increasingly complex landscape (Novitzky et al., 2023).
Primary care screening tools like HITS, HARK, and WAST provide structured approaches to DA assessment (Basile et al., 2007; O’Doherty et al., 2014). Broad, general questions are typically ineffective, whereas concise screening tools have proven more effective in identifying DA (Shinjo et al., 2021; Thombs et al., 2007).The HITS tool (Hurt-Insult-Threaten-Scream) assesses psychological and physical abuse but does not address sexual abuse (Sherin et al., 1998). The HARK tool (Humiliation, Afraid, Rape, Kick) consists of four questions that evaluate emotional, sexual, and physical abuse (Sohal et al., 2007). The WAST (Woman Abuse Screening Tool) assesses multiple forms of abuse including physical, psychological, and sexual abuse (Brown et al., 1996), and its shorter two-item version, the WAST-Short, focuses specifically on relationship tension and conflict resolution (Brown et al., 2000). The brevity and adaptability of the WAST-Short make it especially suitable for high-volume clinical settings, and international studies show its reliability across diverse populations (Fogarty & Brown, 2002; Iskandar et al., 2015). A recent study confirmed that the WAST-Short is an effective, easy-to-use DA screening tool, outperforming an adapted clinical interview in reliability and suitability for busy primary care environments (Matavel et al., 2023). When combined with clinical judgment, this tool can help facilitate early DA identification and timely intervention, enabling clinicians to support patients effectively without adding significant time burdens.
Despite the availability of screening tools, many clinicians still hesitate to use them due to time constraints, discomfort, and a lack of training and protocol clarity (Collins et al., 2023; Hegarty et al., 2021; Miller et al., 2021). There is no universal standard for DA screening across healthcare settings, and clinicians often lack suitable tools, hindering consistent use. Some tools are too lengthy or not validated for all populations. Simplifying resources and providing regular DA screening training for HCPs is essential to support patient disclosure and care (O’Reilly & Peters, 2018). A recent review stressed the need for simple screening tools for maternal mental health in primary care (Gyimah et al., 2024). Additionally, a Clinical Decision Support tool improved DA screening by boosting physician confidence and care quality (Rossi et al., 2024). Clinicians recommended improving its conciseness and flexibility. A meta-analysis found that computer-assisted self-administered screenings led to higher DA disclosure rates than face-to-face or written screenings (Hussain et al., 2015). Digital tools like self-administered questionnaires offer a privacy-preserving option that encourages disclosure (Lenert et al., 2024).
Our study selected the WAST-Short tool for its indirect approach, making it particularly suitable for culturally sensitive environments. By focusing on relationship dynamics rather than asking direct questions about abuse, it minimises stigma and encourages disclosure, addressing key barriers at the individual and relational levels of the Social Ecological Model (SEM). SEM provides a valuable framework for understanding the multiple factors that influence DA disclosure, highlighting how individual experiences, interpersonal relationships, community support, and societal attitudes shape survivors’ willingness and ability to disclose abuse. Based on this framework, we hypothesise that NHS patients in UK primary care with a history of abuse will score higher on the WAST-Short, even after adjusting for demographic factors. This would reflect the impact of past trauma on disclosure at the individual level, as well as the role of healthcare environments (community level) in facilitating identification. Additionally, we propose that WAST-Short will be especially effective in identifying DA among individuals with prior abuse histories, as it reduces direct confrontation and aligns with the need for sensitive screening approaches in healthcare settings.
The use of WAST-Short in UK primary care has not been previously examined. To address this gap, we conducted a cross-sectional study among NHS patients in Northwest London (NWL) to explore the relationship between abuse history and WAST-Short scores. By evaluating its effectiveness within a primary care setting – an essential community-level factor in SEM – our study provides insights into how structured screening can improve DA identification and intervention, ultimately supporting a broader societal shift toward better DA recognition and response.
Materials and Methods
Study Design
An open, anonymised 29-item electronic survey (e-Survey) was administered via the Qualtrics™ platform to a broad population in the NWL community, targeting individuals aged 18 and over, residing in the UK. The research team included a female general practitioner, a clinical academic, a mixed methods researcher, and a statistician. The survey questionnaire was developed through a rigorous, systematic process grounded in theoretical and empirical literature (Black et al., 2010; Brown et al., 2000; Elkin, 2022; Pingley, 2017). The Social Ecological Model (SEM) guided the selection of survey items, ensuring that factors influencing DA disclosure were examined at multiple levels, including individual experiences, interpersonal relationships, healthcare accessibility (community level), and broader societal attitudes toward DA screening. By structuring the questionnaire in alignment with SEM, the study aimed to explore how these interconnected factors shaped disclosure patterns and the effectiveness of WAST-Short in primary care settings.
The team conducted an exhaustive review of existing research and questionnaires on similar topics, selecting and refining items from previously validated sources to align with the study’s objectives. To ensure scientific rigor and validity, several established tool development methods were employed, including Content Validity Ratio for item relevance, face validity to assess clarity and appropriateness, and reliability testing to confirm consistency. After piloting the questionnaire with a small sample, feedback from institutional colleagues and patient representatives informed further revisions. This ensured that the items accurately reflected the study’s aims. Questionnaire items were organised to reflect the study’s key research dimensions, with adjustments guided by input from institutional colleagues and pilot testing. This collaborative approach ensured that each item accurately captured the core aspects of the study’s objectives. All members of the research team contributed to the development of the study protocol, including study design, methodology, and data analysis. No sample size calculation was performed, as this was an exploratory study, but the piloted and validated questionnaire provided a structured tool for gathering meaningful data.
General practices across NWL (Brent, Central London, Ealing, Hammersmith & Fulham, Harrow, Hillingdon, Hounslow, and the West London Clinical Commissioning Groups) served as patient identification centres. The Clinical Research Network contacted these practices to express interest in the study. We hoped to engage as many NHS patients on GP lists as practically possible, not only to deepen our understanding of this complex subject but also to raise awareness about DA and the available support services. Participation was voluntary, and practices were given the choice to exhibit study posters in their reception and waiting areas to enhance awareness. Once practices expressed interest, study materials were dispatched. Practices could withdraw from the study at any time without providing a rationale. The GP practice team identified eligible patients (aged 18+) who had consented to SMS contact and sent the e-Survey link via bulk SMS. Informed consent was implied upon submission of the completed questionnaire. Based on the recommendation from the ethics committee, the practices were instructed to initially send the SMS containing study information and the e-Survey link to all eligible female patients. Subsequently, 1 month later, the same message would be sent to all eligible male patients. No follow-up messages were to be sent beyond this initial communication.
Exclusion criteria included individuals unable to provide informed consent due to conditions such as dementia or autism and those without access to the necessary technology (e.g. smartphone or computer with internet). The final decision on exclusions was made by the GP partner, considering the sensitivity and intricacy of the subject matter.
The survey included the Participant Information Sheet (PIS) detailing the study aims, ethical considerations, data handling procedures, and contact information for DA support services. It was made available on Qualtrics™ (Version XM) licenced via the Imperial College between 3 March and 7 October 2022. Participation was voluntary, and there were no financial incentives. Participants were informed that their responses could help advance knowledge about DA and contribute towards developing policies to tackle DA. They were encouraged to reach out to the study team for further details about the study’s findings or its publication. The survey ensured confidentiality and anonymity, with data stored securely in an institutional database, which could only be accessed by the research team. Duplicate case entries could not be identified by the study team as IP addresses were not obtained.
Electronic Survey
The 29-item survey was presented on a single page in Qualtrics and automatically captured responses (Supplemental File 1). The tool was translated into 18 languages (English, Arabic, Bengali, Chinese (simplified), Chinese (traditional), French, German, Hindi, Italian, Persian, Polish, Portuguese, Sinhalese, Somali, Spanish, Tamil, Turkish, and Urdu). Participants were informed that language translations were available via a dropdown menu. Qualtrics’s websites have first-party cookies, allowing third parties to place cookies on devices. The e-Survey was accessible by anyone with a link via a personal computer or smartphone and included questions of tick or Likert-scale responses. The questions explored personal experiences and understanding of DA, responses to the two WAST-short screening questionnaire, and the public’s view on routine screening in raising awareness, identifying and supporting those experiencing abuse in primary care.
The WAST-Short is a validated, non-threatening, gender-neutral screening tool that has demonstrated high accuracy, detecting 100% of non-abused women and 91.7% of abused women across both English- and non-English-speaking populations (Brown et al., 2000).The WAST-Short questionnaire assessed the degree of tension in the respondent’s relationship of concern (Question 1), and their perceived difficulty in working out arguments within a relationship (Question 2) (Brown et al., 2000). We chose this tool to analyse its suitability in our society. WAST-Short over the full WAST minimises the number of questions in the survey instrument and reduces participant fatigue in completing the survey. The WAST-Short score was calculated by the addition of the points allocated to the answers to the two questions: (i) Tension in relationship (no tension = 1, some tension = 2, a lot of tension = 3) and (ii) difficulty in working out arguments (no difficulty = 1, some difficulty = 2, great difficulty = 3). For example, a respondent answering “a lot of tension” to the relationship question and “some difficulty” to the working out arguments question would get a score of 5. Additionally, participants were asked about their comfort in answering these questions. Participants also answered a direct question about their personal experiences with DA (“Have you experienced domestic abuse?” with options Yes, No, and Would rather not say). They were then asked to select their relationship with the abuser. To educate participants, questions prior to this in the survey outlined signs of DA in adults and children. Participants were also asked if they would recommend that primary care providers use a short screening tool to raise awareness and identify those experiencing DA.. Furthermore, participants’ opinions were tested by asking them to select their extent of agreement (Agree/Neither agree nor disagree/Disagree). Questions included whether they perceived primary care as the best setting to help identify and refer survivors of DA, if there are sufficient support services available for survivors of abuse, and if healthcare providers should have adequate training to identify and support survivors of DA.
Demographic information such as gender, age, ethnicity, employment status, level of education, and marital status were collected, and participants had the opportunity to review and edit their responses before submission. The survey’s usability was tested with a small group prior to release. Data were anonymised and stored securely; responses were excluded only if the survey was largely incomplete.
Statistical Analysis
We used frequencies and percentages to describe participant characteristics. Given that the WAST-Short is a validated screening tool for DA, its psychometric properties have already been rigorously tested in prior research. Therefore, we did not perform additional psychometric analyses such as factor analysis or reliability testing. Instead, our focus was on evaluating the WAST-Short’s predictive capability in identifying DA history, particularly among individuals reluctant to disclose (e.g. those selecting “would rather not say” [WRNS]).
To achieve this, we employed both univariable and multivariable logistic regression models, as logistic regression is the most appropriate method for analysing binary outcomes and assessing predictive discrimination. The outcome variable was categorised as “Yes” versus “No” and “WRNS” versus “No.” This approach allowed us to quantify the association between WAST-Short scores and DA history, estimating adjusted odds ratios (ORs) and 95% confidence intervals (CIs) while controlling for demographic factors (age, gender, ethnicity, education, employment, and marital status). By accounting for uncertainty in WRNS responses, this analysis provided clinically meaningful insights into how the WAST-Short functions as a screening tool in real-world settings. This methodological approach aligns with our study’s aim of assessing the tool’s ability to distinguish individuals at risk of DA, rather than reassessing its internal validity. Statistical significance was set at p-value <.05, and analyses were conducted using SPSS version 27.0.
Ethics
This study received approval from the NHS Research Ethics Committee (IRAS ID 302611). The quality of the survey was assessed using the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) (Eysenbach, 2004) (Supplemental File 2). Our adherence to ethical guidelines influenced certain methodological choices, rendering some CHERRIES checklist elements inapplicable. Incentives were avoided to ensure voluntary participation, and our survey’s educational goals required a fixed question sequence, precluding randomisation. Prioritising participant privacy, we did not track unique site visitors or conduct log file analysis and or implement completeness checks for all items. Our methodology aimed to maximise accessibility and inclusiveness without registration, and all responses were included without time-based exclusions and foregoing statistical corrections. These choices, detailed in our manuscript and reflected in the updated CHERRIES checklist, were made to align with ethical standards and research objectives (Supplemental File 2).
Results
Demographic Profile of Respondents
Seventeen general practices across NWL participated in our study with 75,094 NHS patients identified as eligible to receive the e-Survey link via SMS. In total 6,967 patients clicked on the e-Survey link (response rate of 9.3%), of which 4,253 (61.0%) consented and completed the questionnaire (Supplemental File 3). Exclusions included individuals who did not provide consent (n = 4) and those who clicked on the survey link, consented, but did not answer any questions 38.9% (2,710/6,967). Of most participants, 73.2% were female, more than half, 52.4% of white ethnicity, and their median age was 39 years, with an interquartile range of 18 to 99 years. Over half, 50.6% were partnered (32.8% married and 17.8% in a domestic relationship), and 35.7% were single. Furthermore, more than two-thirds (67.6%) have acquired higher education or had a university degree, and 65.7% were in full-time employment. Survey findings can be found in the Supplemental File 4.
History of DA
Nearly half (49.0%) of the respondents confirmed having experienced DA (95% CI: [46.7%, 50.0%]), while 6.1% did not want to disclose it [5.4%, 6.8%]. Respondents who reported abuse claimed it was from their current spouse or partner (45.8%), their ex-partner (35.5%) or parent (28.9%).
WAST-Short Score
We analysed the association of reported history of abuse with the WAST-Short score and the participants’ characteristics (Table 1). A significant association was found between reported history of abuse and WAST-Short score. The findings suggest that those who reported history of abuse had a significantly higher WAST-Short score compared to those who refrained from disclosing their history of abuse and those with no history of abuse (median (IQR); 5.0 (4.0, 6.0) versus 4.0 (3.0, 5.0) and 2.0 (2.0, 3.0) respectively, p-value <.001), Figure 1. The findings suggest that those who reported history of abuse had a higher WAST-Short score which means that they were more likely to report some or a lot of tension in their relationship and had greater difficulty in working out arguments with their partners. Reported history of abuse was significantly associated with all demographic characteristics (age, gender, ethnicity, education, employment, and marital status). In particular, reported history of abuse was more common among women, individuals of non-white ethnicity, those with lower education levels and those who were unemployed.
Association of History of Abuse With Participant Characteristics and WAST-Short Questions.

Note. WRNS = Would Rather Not Say.
p-Value obtained using Kruskal-Wallis test.
p-Value obtained using Chi-squared test.
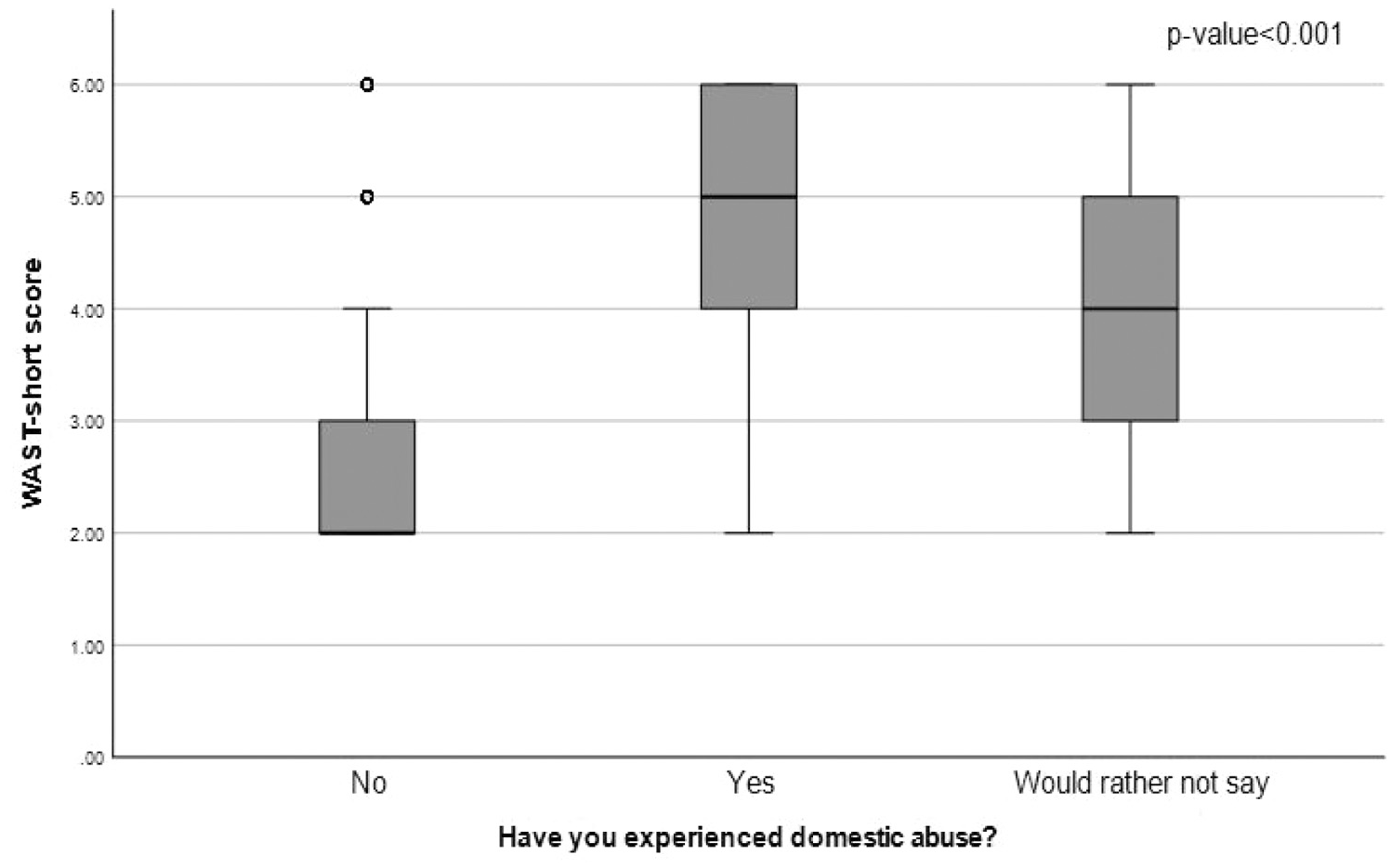
Distribution of WAST-Short score by disclosure of the DA experience.
Univariable and multivariable logistic regression analysis were carried out to assess the association of reported history of abuse (Yes vs. No and WRNS vs. No) with the WAST-Short score. The results of the multivariable analysis, after adjusting for age, gender, ethnicity, education, employment and marital status suggested that a higher WAST-Short score was significantly associated with higher odds of reported history of abuse and higher odds of reluctance to disclose a history of abuse (adj. OR of 2.98 (95% CI: [2.77, 3.20]) and 2.33 [2.06, 2.65] and p-value <.001, respectively (Table 2). In terms of demographic characteristics, males compared to females had significantly lower odds of history of abuse for both groups (Yes vs. No and WRNS vs. No) with adj. OR of 0.51 [0.42, 0.63] and 0.54 [0.37, 0.78] both p-values <.001 respectively.
Univariable and Multivariable Association of the History of Abuse (Yes vs. No and WRNS vs. No) With WAST-Short Score and Demographic Characteristics.

Finally, regarding the goodness of fit, both model 1 and model 2 explained a good proportion of the variability (Nagelkerke R 2 = 55.6% and 24.8% respectively). Despite the low R square for the second model, the Hosmer and Lemeshow Test for goodness of fit did not reject the null hypothesis for the model being specified correctly (Chi-square = 2.970, p = 0.94) reassuring the goodness of fit for model 2 (Table 2).
Discussion
Our study found that nearly 50% of respondents reported a history of DA. Notably, individuals who reported having experienced abuse and those who refrained from disclosing their experiences of abuse (WRNS) had significantly higher WAST-Short scores compared to those with no reported history of abuse. The WRNS category, comprising 6.1% of the sample, presented an analytical challenge, as it was unclear whether non-disclosure reflected discomfort or a simple refusal to answer. However, the elevated WAST-Short scores among WRNS respondents suggest that some may have experienced abuse despite their reluctance to disclose.
These findings can be understood through the lens of the Social Ecological Model (SEM), which highlights how individual, relational, community, and societal factors shape experiences and behaviours, such as DA disclosure. The individual level of SEM, for example, helps explain how past trauma influences individuals’ willingness or ability to disclose abuse. Our study’s results suggest that even when abuse is not openly disclosed, the trauma may still manifest in screening tools like the WAST-Short, supporting the utility of such tools in identifying individuals in need of support.
Regression analyses further reinforced these findings. A higher WAST-Short score was associated with significantly higher odds of having a history of abuse and a reluctance to disclose abuse. The first model, linking WAST-Short to a reported history of abuse (Yes vs. No), is unsurprising given that WAST-Short is a validated tool for assessing DA history. However, our second model, which explored the WRNS versus No response, revealed a significant association between higher WAST-Short scores and an unwillingness to disclose DA experiences. To our knowledge, this association has not been previously explored in a UK primary care context, and the findings underscore the relevance of SEM’s relational and community-level factors. Primary care settings serve as critical touchpoints for disclosure, where appropriate screening can facilitate early identification and intervention.
The reliability of WAST and WAST-Short as screening tools is well-documented, with high sensitivity and specificity in distinguishing between abused and non-abused individuals (Brown et al., 2000). Our findings are consistent with a French study that validated the French version of WAST as an effective and widely accepted tool for early detection and prompt referral to personalised support for those facing abuse (Guiguet-Auclair et al., 2021). Similarly, a cross-sectional study in Iran found that WAST-Short, with a cut-off score of 3, accurately identified DA in the previous year among women with mental disorders, recommending its use for screening (Salahi et al., 2018). It was also recognised as a practical tool for initial DA screening in busy settings. Additionally, an earlier Malaysian study highlighted the important role of primary care in secondary prevention for abused women and emphasised how adapting the WAST screening tool could support primary prevention for non-abused women during routine visits to primary care clinics (Lin & Othman, 2008). These findings reinforce primary care’s role in identifying DA, reflecting SEM’s community and societal levels and the influence of healthcare settings on recognition and response.
The higher odds of WRNS responses in our study suggest that individuals who refrain from disclosing abuse may share similar experiences and needs as those who directly report abuse. This finding aligns with SEM’s individual and relational levels, where both trauma and relational dynamics influence disclosure. Previous research suggests that some survivors are emotionally unready to disclose abuse, often due to ongoing psychological processing or fear of judgment (Reisenhofer & Taft, 2013). In such cases, screening tools like WAST-Short provide a non-intrusive means of identifying those at risk, particularly given the well-documented barriers to disclosure, including stigma, fear of consequences, and uncertainty about available support (Dowrick et al., 2021).
A qualitative meta-analysis further highlights the importance of woman-centred care, emphasising emotional connection, proactive support, and an approach that respects autonomy (Tarzia et al., 2020). Many survivors do not receive adequate care, often resulting in misdiagnosis or inappropriate treatment (Papas et al., 2023). The Crime Survey for England and Wales (Office for National Statistics, 2024) estimated that 4.6% of individuals aged 16 and over experienced DA in the past year, equating to approximately 2.2 million victims. Alarmingly, 6.1% of our respondents declined to disclose experiences of abuse despite the anonymity of the e-survey. These findings highlight the need for HCPs to foster supportive environments that encourage disclosure, aligning with SEM’s societal level, where cultural norms and healthcare systems influence DA recognition and intervention. Our findings suggest that using non-intrusive screening tools like WAST-Short in primary care could facilitate disclosure and help identify at-risk individuals who may otherwise go undetected.
Demographic factors such as age, gender, ethnicity, education, and employment status further contextualise DA experiences. Marginalised groups, particularly those with lower education and unemployment, face a higher risk of abuse (Maharaj et al., 2010). A Malaysian primary care study similarly found significant associations between DA and ethnicity, income, and education (Lin & Othman, 2008). Our study aligns with these findings, showing higher abuse rates among women, non-white individuals, those with lower education, and the unemployed. Women disproportionately experience severe physical and sexual violence (Smith et al., 2011), with an Australian study reporting that 1 in 5 women and 1 in 21 men have experienced sexual violence since age 15 (Australian Institute of Health and Welfare, 2022). Single mothers, in particular, face heightened vulnerability due to financial hardship (Summers, 2022). A Trinidadian study also found DA more common among women with lower education, though employed women reported higher abuse rates, possibly due to financial security enabling disclosure (Maharaj et al., 2010). Additionally, DA, measured by WAST-Short, was more prevalent among those of lower socioeconomic status. This emphasises the need for culturally sensitive interventions and targeted screening strategies, as ethnic, social, and economic factors shape disclosure behaviours.
In primary care settings, DA screening programs should be designed with consideration of structural and societal factors, such as healthcare system barriers and provider attitudes, as outlined by the SEM. Routine screening using tools like WAST-Short can be particularly effective for identifying individuals who may not otherwise disclose their experiences, particularly in high-demand environments such as busy clinics or virtual consultations. Standardised questioning during patient interactions can help initiate sensitive discussions, reassuring survivors that they are not alone and that support is available.
HCPs play a critical role in DA identification and intervention. Proactive enquiry about DA in routine consultations facilitates early detection, benefiting both survivors and those at risk. A World Organisation of Family Doctors (WONCA, 2020) webinar emphasised that any healthcare interaction is an opportunity to identify abuse. Similarly, qualitative research shows that survivors often prefer clinicians to ask about DA directly (Feder et al., 2006). While debate exists regarding routine screening versus targeted clinical enquiry, evidence suggests that structured DA screening increases identification rates and access to support (O’Doherty et al., 2015). Despite variations in effectiveness, most women – regardless of DA history – support routine screening in healthcare settings (Feder et al., 2006).
To enhance early identification, clinicians require ongoing training and resources to conduct screenings effectively and sensitively (Feder et al., 2011; Sohal et al., 2020). Simplified screening approaches can improve awareness, ensure patient safety, and minimise unintentional harm (Tarzia et al., 2020). Implementing structured screening protocols can strengthen DA identification efforts, enabling timely intervention and supporting primary prevention.
With increased mental health demands post-COVID-19, the role of validated screening tools like WAST-Short becomes even more crucial. Our findings highlight a gap in care for individuals reluctant to disclose abuse, reinforcing the need for targeted screening strategies. Identifying at-risk individuals through unobtrusive screening methods can also help uncover underlying health issues, ensuring that treatment addresses root causes rather than just symptoms. Further research is needed to evaluate the effectiveness of short-validated screening tools like WAST-Short in clinical settings and to optimise referral pathways. Strengthening screening and intervention strategies will ultimately enhance care for DA survivors and improve overall health outcomes.
Strengths and Limitations of the Study
To our knowledge, this study represents the first large-scale exploration of the non-threatening WAST-Short DA screening tool in the English primary care setting since the advent of the COVID-19 pandemic. A key strength of our study is the translation of the e-survey into 18 languages, ensuring participation from diverse, multi-ethnic communities residing in NWL. Such surveys provide a convenient and cost-effective means of data collection. However, our recruitment process faced inherent challenges, primarily due to the anonymous nature of the survey and its multi-step recruitment process. The resulting low response rate can be attributed to several factors: privacy concerns stemming from the sensitive nature of the topic, the voluntary and anonymous format lacking incentives, and the absence of reminders for safety reasons. Nonetheless, we achieved a commendable 61.0% participation rate among registered individuals at NWL general practices, yielding valuable insights into our study objectives. The large sample size, encompassing a wide age range and diverse demographics despite the sensitivity of the subject matter, further strengthens our findings.
A key limitation is that survey access was restricted to individuals with smartphones and internet access, potentially excluding DA survivors experiencing coercive control, thereby limiting completion rates. Additionally, not all survey questions were validated, particularly those exploring various facets of DA, which may have affected response accuracy. Some survivors may not relate to the term “domestic abuse,” leading to potential underreporting and skewing study findings. Moreover, our study relied on screening rather than confirmatory tests, further highlighting its limitations.
Our study focused on respondents’ experiences of DA without considering the impact of multiple perpetrators on survivors. Additionally, the sample may not fully represent the entire UK population, as only a quarter of respondents were male, 8.1% were aged 66 and older, and nearly half were between 26 and 45 years old. Given that a systematic review found that one in four vulnerable elders faces abuse, with a largely undetected portion, future research should aim to improve representation among older adults. Elders and their caregivers are open to reporting abuse and should be routinely questioned about it (Cooper et al., 2008). Additionally, most participants had a higher level of education, which may have influenced their willingness to participate in research and surveys, as well as their likelihood of completing such assessments. Addressing these demographic gaps in future studies would enhance generalisability.
Another noteworthy limitation is the study’s exclusive focus on NHS patients, omitting crucial insights from primary care HCPs. Including HCP perspectives would provide invaluable insights into the feasibility, implementation challenges, and clinical relevance of using screening tools like WAST-Short in primary care settings.
Furthermore, while the WAST-Short has demonstrated effectiveness in identifying individuals with a history of DA, its applicability in culturally diverse or non-Western settings may be influenced by differing societal norms around disclosure, stigma, and perceptions of abuse. Cultural differences in the interpretation of screening questions and willingness to disclose abuse – particularly in societies where discussing DA carries significant stigma – may impact the tool’s sensitivity and specificity. Additionally, variations in the conceptualisation of DA across cultures may influence the tool’s ability to capture certain forms of abuse. Future research should explore the cross-cultural validity of the WAST-Short and consider adaptations to enhance its relevance across diverse populations.
Conclusion
This study conducted among NHS patients across primary care in NWL explored the use of a short DA screening tool in primary care settings. It underscores the importance of screening in identifying survivors, particularly those who may struggle to disclose their experiences of abuse. The use of the established, non-threatening two-item WAST-Short in primary care settings could significantly aid in identifying and supporting DA survivors. Training health and social care professionals in administering this brief screening questionnaire would not only enhance awareness but also improve the identification and support of abuse survivors.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251374382 – Supplemental material for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London
Supplemental material, sj-docx-1-sgo-10.1177_21582440251374382 for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London by Vasumathy Sivarajasingam, Manisha Karki, Emmanouil Bagkeris and Austen El-Osta in SAGE Open
Supplemental Material
sj-docx-2-sgo-10.1177_21582440251374382 – Supplemental material for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London
Supplemental material, sj-docx-2-sgo-10.1177_21582440251374382 for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London by Vasumathy Sivarajasingam, Manisha Karki, Emmanouil Bagkeris and Austen El-Osta in SAGE Open
Supplemental Material
sj-docx-3-sgo-10.1177_21582440251374382 – Supplemental material for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London
Supplemental material, sj-docx-3-sgo-10.1177_21582440251374382 for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London by Vasumathy Sivarajasingam, Manisha Karki, Emmanouil Bagkeris and Austen El-Osta in SAGE Open
Supplemental Material
sj-docx-4-sgo-10.1177_21582440251374382 – Supplemental material for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London
Supplemental material, sj-docx-4-sgo-10.1177_21582440251374382 for Exploring the Use of the WAST-Short Domestic Abuse Screening Tool in Primary Care: A Cross-Sectional Study in Northwest London by Vasumathy Sivarajasingam, Manisha Karki, Emmanouil Bagkeris and Austen El-Osta in SAGE Open
Footnotes
Acknowledgements
The authors thank Ms. Iman Webber and Aos Alaa for supporting the development of the e-Survey and the research protocol.
List of Abbreviations
CHERRIES Checklist for Reporting Results of Internet E-Surveys
CSEW Crime Survey for England and Wales
COVID-19 Coronavirus Disease 2019
DA Domestic Abuse
e-Survey Electronic Survey
GP General Practitioner
HCPs Healthcare Professionals
NHS National Health Service
NWL Northwest London
PIS Patient Information Sheet
PTSD Post Traumatic Stress Disorder
SMS Short Message Service
UK United Kingdom
WAST Women Abuse Screening Tool
WAST-Short Women Abuse Screening Tool-Short
WRNS Would Rather Not Say
Ethical Considerations
The research involved human participants in accordance with relevant guidelines and regulations (such as the Declaration of Helsinki). This study received ethical approval from the NHS Research Ethics Committee (IRAS ID 302611) and Health Research Authority (HRA).
Consent to Participate
Participation in the survey was voluntary. Before answering the questionnaire, participants were asked to confirm their consent. Consent was implied through the submission of a completed questionnaire.
Consent for Publication
Participants were informed that the data collected during the study would be anonymised and used for research purposes, including publication. Consent was implied through the submission of a completed questionnaire.
Author Contributions
All authors provided substantial contributions to the conception (V.S., A.E.O.), design (V.S., A.E.O., E.B., M.K.), acquisition (M.K., A.E.O.), and interpretation (V.S., A.E.O., M.K., E.B.) of study data and approved the final version of the paper. V.S. took the lead in planning the study with support from co-authors. M.K. and, E.B. carried out the data analysis. A.E.O. is the guarantor.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. A.E.O. is supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration (ARC) Northwest London. The views expressed are those of the authors and not necessarily those of the NHS, NIHR, or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.