
Abstract
Gender-based violence (GBV) is one of the greatest social issues affecting South Africa, and universities are no exception. This article reports preliminary results of a pilot study conducted at the University of South Africa (Unisa). The study aimed to ascertain perceptions of GBV among university staff. A range of frequency-seeking questions aimed at exploring awareness, experiences, and reflections about solutions to GBV were posed to selected staff members by means of an online survey. The results of the survey are presented here in graphic form and subjected to descriptive analysis, which is compared with existing literature on the topic. The key findings in this pilot study concern the perceptions of GBV among university staff, their awareness of the types of GBV and its prevalence, and the participants’ feelings about safety regarding GBV and commitment to participate in possible solutions. We conclude that we cannot expect trends reported in literature to be replicated in any research study.
Introduction
It is well-known that gender-based violence (GBV) is a scourge in South Africa. A 2015 report by the Tshwaranang Legal Advocacy Centre (2015) in Gauteng notes that, in relation to GBV, “justice is an aspiration, but not a reality for the women of South Africa.” (n.p.). Hargreaves, Vetten, Schneider, Malepe, and Fuller published an article in 2006 titled “‘Marriage is Like Sitting on Red Coals’: A Case Study of Domestic Violence in Four Villages of the Moretele District, Tshwane Metropole” in which the authors explore questions that are relevant to GBV in South Africa. Their article offers useful starting points for our work, including the troubling intersection between traditional culture and gender roles, as well as why men abuse their wives, and what can be done about it. The article opens with the statement that “Men’s violence and ill-treatment of their intimate female partners is widespread in South Africa” (Hargreaves et al., 2006, n.p.). All scholarly analyses of GBV agree that it is a multidimensional problem, and that isolating the root causes is well-nigh impossible, making prevention equally difficult to achieve. While part of the root cause lies in restrictive patriarchal norms for women in South Africa, gendered inequalities in relation to education and employment also contribute to the prevalence of GBV (Jewkes, 2002; Mahlori, 2016). These inequalities make women economically and socially subordinate to men. For example, women withstand the worst impact of poverty in the country: Statistics South Africa reports that, between 2008 and 2015, unemployment rates were consistently higher for women than for men and that women’s earnings are consistently lower than men’s (Merten, 2017). This means that women are poorer than men and are likely to be economically dependent on men, further reducing their agency and ability to resist GBV, which often combines physical cruelty with financial deprivation.
Economic disempowerment goes hand in hand with the prevalence of GBV. Put another way, poor women are more at risk for GBV than wealthy ones. Rachel Jewkes’s (2002) article “Intimate Partner Violence: Causes and Prevention” highlights this invidious link by saying that “there are few social and demographic characteristics that define risk groups for intimate partner violence. Poverty is the exception and increases risk through effects on conflict, women’s power, and male identity” (p. 1423). Possibly as a result, there is a paucity of data available on the prevalence of GBV among the educated strata of South African society. The educated strata form the target population for this study. If the link between GBV and poverty is absolute, then better resourced women should be less susceptible. By investigating the prevalence of GBV among the staff and student community of South Africa’s largest university (Unisa), we propose to explore a population that may be ignored in some analyses of GBV: those who are better educated and possibly better resourced than those who are often the subjects of studies of GBV. In fact, there is limited research on GBV among the tertiary education community, despite the university context in South Africa having received attention when four members of the academic staff were dismissed from the University of the Witwatersrand in 2011 and 2013. That university was subjected to an extensive investigation by its own Centre for Applied Legal Studies (CALS), in partnership with Norton Rose Fulbright, with a view to establishing the extent of GBV among students and staff. The findings of the investigation revealed, as was to be expected, that GBV was and is much more widespread in the university community than was previously suspected (CALS, University of the Witwatersrand, 2013, n.p.). A similar study was undertaken at UCKAR (the university currently known as Rhodes) in the wake of a student protest under the Twitter handle #EndRapeCulture. UCKAR appointed a Sexual Violence Task Team (SVTT) under the auspices of its own Centre for Critical Studies in Sexualities and Reproduction. The SVTT wrote a 174-page report on the problem, titled “‘We will not be silenced’: A Three-Pronged Justice Approach to Sexual Offences and Rape Culture at Rhodes University/UCKAR” (SVTT, 2016). The report is unique in the context of studies of GBV in a university context in that it focuses extensively on responses to the problem, outlining three possible routes to providing justice for the victims and perpetrators of GBV.
GBV Globally and in South Africa
The World Health Organization (WHO), drawing on expertise from South Africa’s Medical Research Council, published a wide-ranging report on the global prevalence and patterns of violence against women both by intimate partners and by nonpartners, which appeared in 2013. According to this report, “35% of women worldwide have experienced either physical and/or sexual intimate partner violence or non-partner sexual violence” (WHO, 2013, p. 2). Chillingly, the report goes on to state that “Most of this violence is intimate partner violence” (WHO, 2013, p. 2). In a similar vein, the Joint United Nations Programme on HIV and AIDS (UNAIDS, 2014) writes in Unite With Women: Unite Against Violence and HIV that women who have experienced intimate partner violence (IPV) are 55% more likely to contract HIV than women who have not been exposed to such treatment by their spouses. WHO (2013) and UNAIDS (2014) provide the global context for studies of GBV. Many similar studies have been undertaken in the South African context, lending support to the popular view of South Africa as “the rape capital of the world” (Gordon & Collins, 2013; Human Rights Watch, 2010). The South African Police Services publish crime statistics on an annual basis. For these purposes, crimes “against the person” are classified as “contact crimes.” One of the subcategories is “sexual offenses”—an umbrella term for rape, IPV, and domestic violence, or GBV in short. The total of reported sexual offenses in 2011 was 66,196; 64,419 in 2012; 66,197 in 2013; 62,267 in 2014; and 53,617 in 2015. These numbers paint a gloomy picture of GBV in South Africa, especially when compared with the figures for murder and attempted murder, which are between 16,000 and 17,000 per year (Crime Stats SA, 2015). However, as Dunkle et al. noted as early as 2004, the rates of reported GBV are likely to be much lower than the actual rates due to a climate of victim shaming, which may make many victims feel reluctant to share their experiences with the police, or even with family members. In 2014, Genderlinks conducted research among 5,600 adults across four provinces and reported that 51% of women in Gauteng had experienced GBV, while 78% of men in the same province reported having perpetrated violence against women. It is well-nigh impossible to specify the exact extent of GBV in South Africa with any accuracy because of the problem of underreporting and a lack of current research into the problem.
One of the features that make it difficult to eliminate GBV is its multisectoral nature. If we explore only the health aspects of the problem, it is easy to see that GBV has pathological implications for the psyche and health of both perpetrators and victims. Gelaye, Arnold, Williams, Goshu, and Berhane (2009) note that “women who are subjected to sexual and/or physical abuse have increased levels of anxiety . . . depression . . . low self-esteem, feelings of hopelessness and symptoms of posttraumatic stress” (p. 2). The psychological and health damages that result from exposure to GBV can be translated into economic costs for the individuals concerned as well as for their societies. Morrison, Ellsberg, and Bott (2007) cite the U.S. Centers for Disease Control and Prevention as mentioning two different types of costs: “direct costs, which are expenditures related to GBV, including health care services, judicial services, and social services, and indirect costs, which are the value of lost productivity from paid and unpaid work” (p. 30). In addition, Morrison et al. (2007) mention a metric known as Disability-Adjusted Life Years (DALYs). They record that more DALYs are lost to women as a result of GBV than as a result of cancer or motor vehicle accidents, and that the effect spills over onto the children of those who have suffered GBV as well (Morrison et al., 2007). University staff who experience GBV are likely to suffer further costs, in the form of studies that are not completed as a result of the trauma experienced by victims.
GBV in Educational Communities
It is necessary to acknowledge that the problem of GBV spreads across the educational context, from schools to universities. Several studies have been conducted into GBV at South African schools. Jewkes, Levin, Mbananga, and Bradshaw conducted a study of rape among female learners in 2002 and found that more than 25% are at risk of being raped, either at or near their schools. In 2014, the United Nations Educational, Scientific and Cultural Organization (UNESCO) commissioned a multicountry study of school-related gender-based violence (SRGBV; Leach, Dunne, & Salvi, 2014). This study offers up-to-date statistics regarding South Africa, including one estimate that 30% of South African schoolgirls are raped in or around school (Prinsloo, 2006, cited in Leach et al., 2014). Data regarding GBV in university communities are, however, less plentiful. Shefer, Clowes, and Vergnani conducted a study of transactional sex at a South African university in 2012, which reported that it is fairly common for female students to engage in sexual relationships with older men or “sugar daddies” to help them pay for photocopies, study fees, or simply to raise their social status. The fact that this is felt to be necessary is, in itself, an index of women’s inferior economic position relative to men. Similarly, Gordon and Collins (2013) conducted in-depth interviews with 12 women students at another South African university to analyze the extent of GBV at the institution. They drew similar conclusions to Shefer, Clowes, and Vergnan (2012) in that both studies found that gender inequalities among university students and staff give rise to a damaging culture of GBV being normalized. Finally, in 2013, the University of the Witwatersrand’s CALS published a report on sexual harassment at that institution (CALS, University of Witwatersrand, 2013). The report found that there was a grave lack of structures at the university that could deal with cases of GBV. It also reported that students who experience GBV may find their well-being and their studies suffering in one of several ways: “i. A decrease in their grades; ii. Failing courses; iii. Changing degrees; iv. Abandoning activities they enjoy; v. Changing universities; or vi. Dropping out of University” (CALS, University of Witwatersrand, 2013, p. 42). One of the most damning findings of the CALS, University of Witwatersrand (2013) study is that “there are no statistics or records kept by the University regarding the consequences of sexual harassment incidents on the complainant” (p. 42). This study has the advantage of surveying the experiences of staff as well as students, and concludes that staff are as much at risk as students are, and are as effectively gagged by the “culture of silence” around reporting GBV to the university authorities (CALS, University of the Witwatersrand, 2013, p. 44). In addition, the CALS, University of the Witwatersrand (2013) report makes pertinent and extensive recommendations about interventions at the university aimed at reducing the rate of sexual harassment. These include steps such as formulating a clear and accessible policy on sexual harassment; a precise definition of sexual harassment that would be communicated to all staff and students; and regulatory mechanisms regarding sexual and romantic relationships between staff and undergraduate or postgraduate students.
In the African continent, in general, Gelaye et al. (2009) conducted a study of Ethiopian women college students in 2008 to probe the relationship between exposure to GBV and depression. Their findings, as might have been surmised, were that there was a significant increase in the rate of depression (ranging from mild to severe depression) among students who had had any exposure to GBV. Although their study is context-specific, it seems intuitively obvious that exposure to GBV among students and staff in South Africa will have a similar result on the victims, producing negative psychological effects such as depression, anxiety, lack of self-esteem, and posttraumatic stress symptoms. Another study at Ogun State of South West Nigeria examined the prevalence of GBV, specifically sexual harassment, in three universities. The study discovered that female students experienced sexual harassment on campus and a number of staff perpetrated sexual harassment (Omonijo, Uche, Nwadiafor, & Rotimi, 2013). The study reported that 85% of staff who perpetrated sexual harassment either were dismissed or suspended (Omonijo et al., 2013). Hence, GBV in the African continent has pertinent consequences for the academic sector.
Unisa provides the university context for the present article, which discusses one phase of a 3-year university-wide research project. The project aims to bring mixed methods to bear on the task of assessing attitudes to, knowledge and experience of GBV among Unisa staff and students. Some of the methods that will be used to research the matter are as follows: online surveys and questionnaires, in-depth interviews, and focus group discussions. The university occupies a different social and educational space from a residential university in that its mode of delivery is Open and Distance Learning. The lack of physical proximity of students to campus and thus to their lecturers creates a unique dynamic, and one which, one might assume, would mitigate against GBV. Nevertheless, the research is based on the hypothesis that GBV does occur with regularity among staff and students at Unisa. We base this assumption on the rare cases of GBV that are reported to university structures (such as Student Affairs and Employee Health and Wellness) and on the fact that GBV is, typically, severely underreported, which leads us to surmise that there are many more cases than have been reported in recent years.
Method
As mentioned in the previous section, this article describes one stage in a 3-year research project whose aim is to establish the prevalence and nature of GBV in the context of Unisa. The project’s data gathering instruments include an online survey for staff and students, in-depth individual interviews, and focus group discussions. In the initial stages of the project, an online survey was devised using Google Forms and distributed to a small population of Unisa staff members, who had volunteered to participate in the pilot study. The aim of the survey was to establish knowledge, attitudes, and experiences of GBV among Unisa staff. The online survey method of gathering data was chosen for convenience and in light of the large size of the population to be sampled, given that Unisa employs approximately 5,000 staff and serves more than 400,000 students in seven learning regions country-wide, as well as serving international students. As Wright (2005) and others mention, online surveys provide both advantages and disadvantages for the researchers. The advantages including the ability to reach populations that would otherwise be difficult to contact, especially when they are geographically remote from the researchers, cost-effectiveness, and saving time which the researchers can spend on other tasks. At the same time, there are disadvantages to this method of gathering data, especially the fact that the sampling process is random and does not allow researchers to gather demographic data about the participants (Wright, 2005). In this article, the responses to an online survey distributed to a small sample of staff (eight) in November 2017 are analyzed. A small sample was used to enable the researchers to gauge the usefulness of the survey by in-depth analysis of the responses. The participants were selected using snowball sampling. A Likert-type scale was used for the survey so that participants could respond by indicating the frequency of various GBV-related encounters and discussions.
Analytic Strategy
The data analysis was performed manually. In light of the small sample size, we analyzed the data by exploring deep meaning, rather than establishing trends. We will now present descriptive analyses of participants’ responses to each question in the survey. The results are presented in the form of graphs, followed by a descriptive analysis and then a comparison to the existing literature. Each question measured frequency of behavior, discussion, and experiences. Participants could select from five responses, ranging from never occurred to frequently, as on the scale shown in Figure 1.

Analytic strategy example.
The results are first presented in a graph, which is automatically created by Microsoft excel based on the frequency of responses. The graphs represent the results in terms of the number of participants who chose each response on the frequency scale. The results in the following section will provide the graphic representation together with analysis.
Results
The first question asked participants, “How often have you heard the term gender-based violence”? (Figure 2).
How often have you heard the term gender-based violence?
As the graph above shows, seven respondents admitted to having heard the term GBV very frequently. The question does not specify how or where they had heard the term, but the higher rate of response to “frequently” allows us to assume that awareness is being raised, whether through educational programs, family conversations, from peers, workshops, in the corridors, or other conversations in the workplace. As mentioned previously, GBV is a profound and widespread problem in South Africa, impacting on almost every aspect of life. SaferSpaces (2017) further confirms that GBV disproportionally affects girls and women and it is deeply embedded in cultures, institutions, and traditions in South Africa. The media could also have had an impact on the responses to this question, as radio and television broadcast reports of GBV on a daily basis.
The second question asked participants, “How often have you been in a conversation about gender-based violence?” (Figure 3).

How often have you been in a conversation about gender-based violence?
In response to the question, six respondents admitted that they had “often” spoken about GBV. The high rate of positive responses by the respondents to this and the previous question indicates that GBV is well-known and widely discussed. The survey did not include questions about how and where these conversations took place. As a result, we may assume that the recent high-profile cases of GBV involving rich and poor, as well as different racial and ethnic groups, have portrayed South Africa as the most notorious country when it comes to GBV. On average, one in five South African women older than 18 years has experienced physical violence, but the picture of gender-based attacks varies according to marital status and wealth. Four in ten divorced or separated women reported physical violence; the number increases to one in three women in the poorest households (Merten, 2017). This complex picture emerges from Statistics SA’s 2016 Demographic and Health Survey. It challenges not only societal attitudes of patriarchy and chauvinism but also the effectiveness of government programs and interventions.
The third question in the survey asked, “Does gender-based violence include physical assault?” (Figure 4). The aim of this question was to elicit what participants believe is included in the term “gender-based violence,” which can encompass a range of practices, such as verbal abuse, financial deprivation, physical assault, rape, and emotional abuse (Mahlori, 2016).

Does gender-based violence include physical assault?
The responses to this question indicated that a majority of respondents (six) believe that GBV does include physical abuse. Although we acknowledge that GBV against men (including physical violence) does occur in heterosexual and homosexual relationships, our focus, in line with that of the literature, is on violence against women. The reason is that violence against women is more frequent and usually more severe than violence against men.
Some possible reasons for the high rate of physical abuse in cases of GBV are offered by Population Services International (PSI), which states that “men feel a sense of ownership over their partners hence the physical abuse. Women tend to endure physical abuse from their partners because of family and societal pressure to make the marriage work as well as to avoid social stigma” (PSI, 2017, p. 1). They go on to say that unemployment seems to be playing a major role as it renders unemployed men wholly dependent on their working spouse and they see physical violence as a means to affirm their masculinity over their partners . . . [M]en have a tendency to come home drunk and start a fight with their partners and this leads to a physical assault towards their spouse . . . Another potential risk is when the woman refuses to have sex with her partner for whatever reason this leads to both physical assault and rape of the other partner. (PSI, 2017, p. 1)
The fourth question in the online survey asked, “Does gender-based violence include rape?” (Figure 5).

Does gender-based violence include rape?
The majority of respondents (six) responded by saying that GBV always includes rape, while two participants believed that it sometimes does. The minority, who believe that rape may sometimes be included in GBV, may base their response on the fact that by the nature of being married or in a cohabitation relationship with a man, a woman is obliged to give in to her husband’s or partner’s sexual demands, regardless of whether she is willing or not. SaferSpaces (2017) places the blame for the high rate of rape on patriarchy. They state that “patriarchy is a social and political system that treats men as superior to women—where women cannot protect their bodies, meet their basic needs, participate fully in society and men perpetrate violence against women with impunity” (SaferSpaces, 2017). GBV is an act of power and control, and rape is one form of exerting power and control by the male over a female. It goes almost without saying that when a woman refuses to have sex with her partner or husband for whatever reason, rape becomes a sort of punishment and a further method of exercising power, authority, and control.
The fifth question posed to respondents was, “Does gender-based violence include emotional cruelty?” (Figure 6).

Does gender-based violence include emotional cruelty?
All the respondents agreed that GBV does include emotional cruelty. The only difference in their responses was the frequency of the occurrence of emotional cruelty. While six of the respondents believed that emotional cruelty was always a part of GBV, only two respondents believed that it was frequently a component. This is a puzzling pattern of response, because, in our view, all kinds of violence, whether verbal, nonverbal, physical, or otherwise directed, are emotionally cruel toward the victim. Emotional cruelty is defined by the Integrated Regional Information Networks (IRIN; 2004) as non-sexual verbal abuse that is insulting, degrading, demeaning; compelling the victim or survivor to engage in humiliating acts whether in public or private; denying the survivor basic expenses for family survival, isolating a person from friends or family, restricting movements, deprivation of liberty or obstruction or restriction of the right of movement. (IRIN, 2004)
The Domestic Violence Act (DVA), Act No. 116 of 1998 of South Africa also recognizes emotional cruelty by referring to it as emotional abuse, which includes but not limited to jealousy, possessiveness, and invasion of privacy. The responses to this question indicate that the respondents are aware of the emotional dimension of GBV.
The sixth question in the survey was, “Does gender-based violence include depriving one’s partner of financial resources?” (Figure 7).

Does gender-based violence include depriving one’s partner of financial resources?
If we consider that responses 3 to 5 (correlating to “sometimes,” “frequently,” and “always”) may all be interpreted as positive, this means that all the respondents believed that depriving one’s partner of financial resources is a form of GBV. The only difference in the responses was the frequency with which participants believed that financial deprivation occurs. This kind of abuse is recognized by the DVA as economic abuse, and it refers to the unreasonable deprivation of economic or financial resources to which the victim is entitled under law or requires out of necessity, including household necessities, mortgage bond repayments, rent money in the case of a shared residence and or the unreasonable disposal of household effects or the property in which the victim has an interest. (DVA, 1998, p. 3)
It comes as no surprise that all the participants in the study believe that financial deprivation is a form of GBV. Auditing firm Klynveld Peat Marwick Goerdeler (KPMG; 2015) estimated that GBV, and in particular violence against women, cost the South African economy at least R28.4 billion and R42.2 billion, or between 0.9% and 1.3% of gross domestic product (GDP) in the year 2012/2013. One may hypothesize that a large proportion of this figure derives from income lost to spouses whose partners are abusively depriving them of financial resources.
The seventh question in the survey was, “Does gender-based violence occur in your community?” (Figure 8).
Does gender-based violence occur in your community?
Only one of the respondents admitted to the fact that GBV takes place in their community, while five were not sure whether this was happening in their communities. In addition to being a South African social problem, GBV is a community problem. Men are reported to be the most frequent perpetrators of such violence while women, families, and children are their victims (Jewkes, 2002; Joyner, Rees, & Honikman, 2015; PSI, 2017). According to PSI (2017), The shift in roles such as women empowerment and the overturning of traditional gender roles, together with high rates of unemployment among men, are seen as causal factors of GBV in communities. Men have been institutionalized to be providers as well as taking care of the family not the other way around but the high rate of unemployment among men has resulted in men losing their status of being a breadwinner in a family set up. (p. 1)
In the 21st century, more women than ever are gainfully employed. They have become breadwinners and are heads of households and which could lead to a loss of esteem and confidence for men, which may be expressed as male violence toward women and children. Men resort to violent behavior as they feel it is their right to dominate women (SaferSpaces, 2017). These perceptions can also be seen in the responses to this question, which indicate that most respondents believe that GBV does occur in their community.
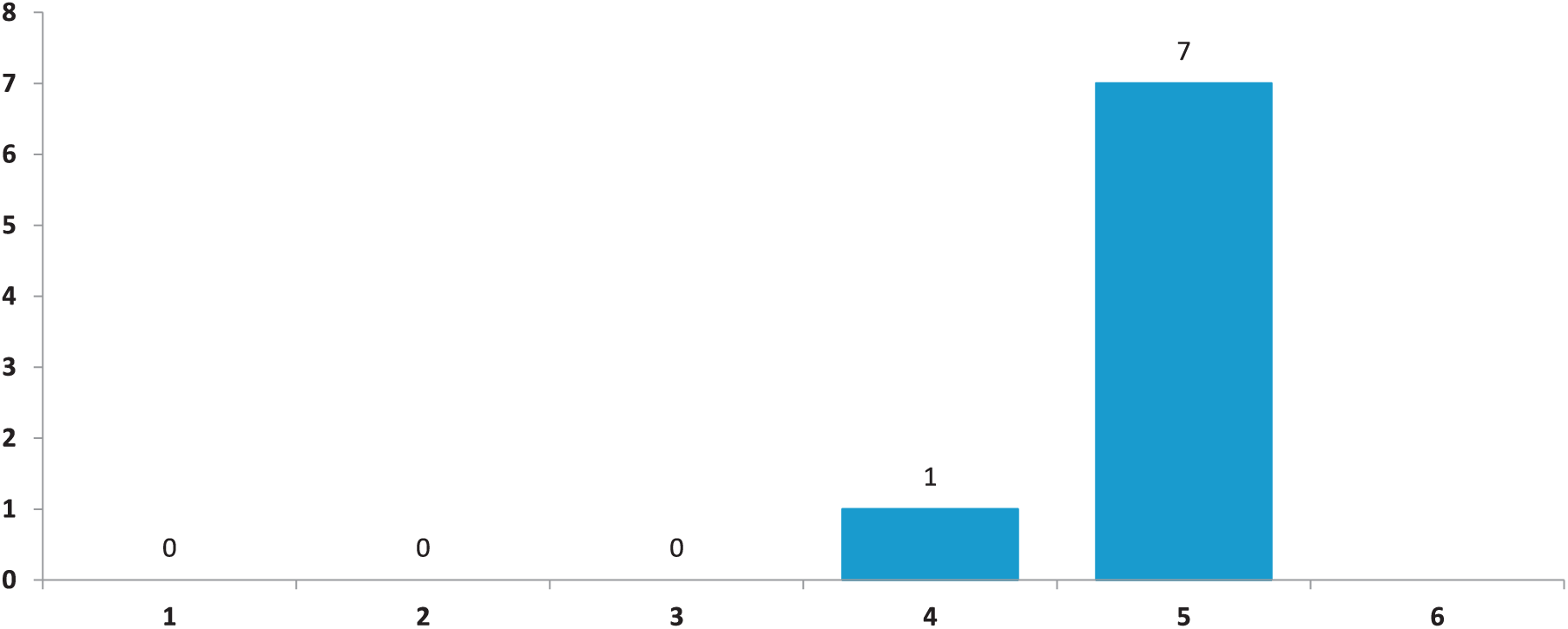
The eighth question was, “Does gender-based violence occur in the broader South African society?” (Figure 9).

Does gender-based violence occur in the broader South African society?
Seven of the participants confirmed that GBV does occur in the broader South African context. This is an indication that they are aware of GBV and its occurrence in the broader South African society, in addition to being aware of its existence within the university context. The high awareness about the occurrence of GBV does not seem to contribute to generate possible solutions to the problem, as the statistics in South Africa are still alarming. Joyner et al. (2015) confirm that South Africa is among the countries with the highest rates of GBV in the world. The participants’ awareness of GBV may be a result of awareness campaigns being implemented by well-known organizations in South Africa, such as Sonke Gender Justice and People Opposing Women Abuse (POWA), which use media to raise awareness of the scourge of GBV.
The ninth question asked, “Is it possible for a married person to rape his or her partner?” (Figure 10). This question specifically targets the participants’ understandings of sexual agency and consent within marriage.

Is it possible for a married person to rape his or her partner?
All eight participants in this pilot study agreed that it is possible for someone to rape their spouse. This question was asked in a gender-neutral way to include males and females. Participants were both males and females and they agreed that it is possible for either gender to rape their spouse. The finding here does not necessarily elaborate on the ability of women to rape men, and in any case such a discussion is outside the scope of this article. The question, rather, explores whether rape can take place within a marital context and this is borne out by all the participants. Although marital rape exists and is widespread, Bennice (2003) indicates that many cultural beliefs invalidate victims’ experiences, under the pretext that a married man has the right to sex with his wife whenever he so chooses.
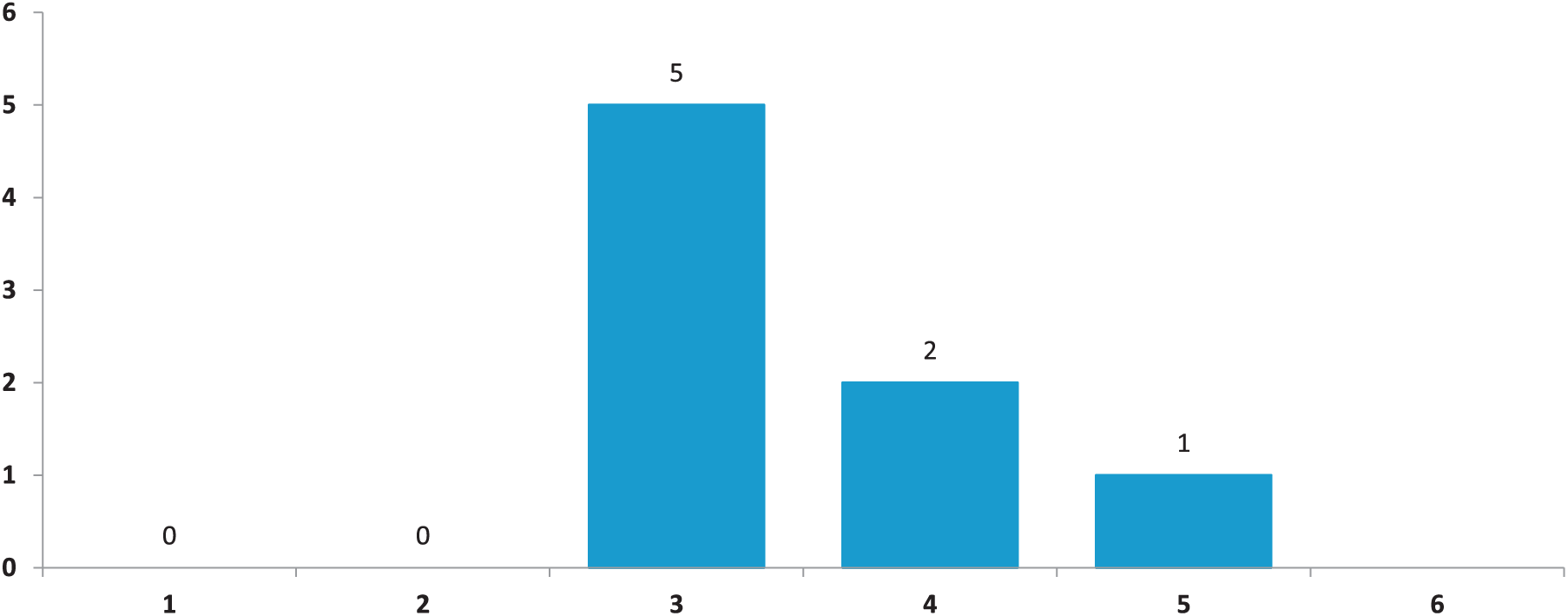
The 10th question moved the respondents toward the university context. It asked, “Have you ever felt threatened or unsafe in discussions with colleagues?” (Figure 11). The question deliberately did not specify the kind of unease that could be felt in discussions with colleagues. The reason is that often sexual harassment is nebulous and is felt more subtly than it can be definitively identified.

Have you ever felt threatened or unsafe in discussions with colleagues?
One participant responded that they never felt threatened or unsafe, while five had seldom felt threatened or unsafe and two of the participants responded that they had sometimes felt threatened or unsafe. The majority of the participants indicated that they do or have at some point felt unsafe in discussions with colleagues. The question did not ask what type of discussions makes them feel threatened or unsafe, but referred to discussions in general. The reason for this is that a colleague may look at another in a way that makes one feel misunderstood, uncomfortable, and/or stereotyped. Shapiro (2011) reports that a stereotype threat is “a concern that one’s actions can be seen through the lens of a negative stereotype” (p. 464). Stereotype threats can take place in conversations between colleagues. Some of the most common stereotype threats are gender stereotypes. Gender stereotypes have severe consequences, especially for women in the workplace as we live in a patriarchal society that considers women as weak, indecisive, soft, and sensitive, while men are considered rational, logical, and of high social status (Mihalčováa, Pružinskýa, & Gontkovičováa, 2015).
The 11th question asked participants, “Have you ever felt unsafe or threatened in discussions with your line manager?” (Figure 12).

Have you ever felt unsafe or threatened in discussions with your line manager?
Six of the participants responded that they had never felt threatened, while one had seldom felt threatened and another one had sometimes felt threatened. This contrasts with the fact that relationships between line managers and subordinates frequently open the door for the abuse of power. Lutgen-Sandvik (2003) also indicates that “the supervisors who inflict psychological abuse on subordinates represent one of the most frequent and serious problems confronting employees in today’s workforce” (p. 471). In contradiction of this finding, none of the participants in our study responded that they had frequently felt unsafe or threatened, only that they had sometimes experienced this.
The 12th question asked participants, “Have you ever heard of people in the Unisa community, either students or staff, who have experienced GBV?” (Figure 13).
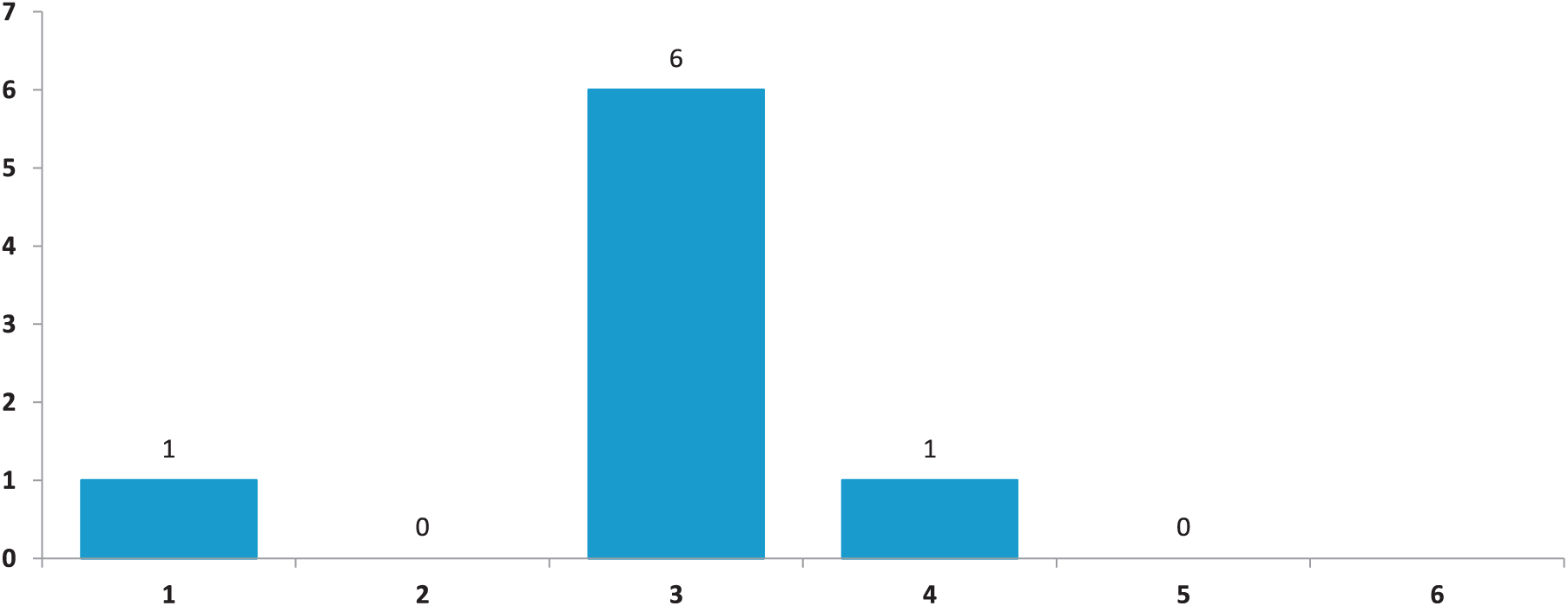
Have you ever heard of people in the Unisa community, either students or staff, who have experienced GBV?
Six of the participants have never heard of anyone at Unisa who has experienced GBV, while one has seldom heard of someone who has experienced GBV and another respondent has occasionally heard of someone who has experienced GBV. With the alarming statistics of GBV in the country, including the Unisa community, this is an indication that many victims of GBV do not speak about it. This may explain the large number of participants who have not heard of colleagues and students who have experienced GBV. This should not be taken as an indication that there are no victims of GBV in the Unisa community. In a study by the Institute for Security Studies (ISS) in 2011, it was found that in Gauteng alone 50% of women have experienced GBV. Hence, we interpret the responses to this question as confirming that many victims of GBV do not speak about it.
The penultimate question in the survey was, “Have you ever reported an incident of gender-based violence?” (Figure 14).

Have you ever reported an incident of gender-based violence?
Six of the respondents reported that they have never reported an incident of GBV, while two participants responded that they have seldom reported an incident. The question did not ask whether they were personally involved in the incident of GBV that they reported, or whether they were reporting on behalf of someone else. Many factors affect the reporting of GBV cases. Mahlori (2016) indicates that these factors have an impact on the official statistics relating to GBV in South Africa. We contend, therefore, that the fact that six respondents have never reported an incident of GBV does not indicate that they have neither experienced GBV nor that they do not know someone who has. Rather, this response may be influenced by the factors that regularly prevent people from reporting such cases, including shame and fear of reprisals from the perpetrator, line managers, or family.
The final question in the survey was, “Have you ever taken part in a discussion of possible solutions to gender-based violence?” (Figure 15).

Have you ever taken part in a discussion of possible solutions to gender-based violence?
Five of the respondents indicated that they had sometimes participated in such discussions, while two respondents indicated that they had frequently participated and one respondent replied that they always, or very often, participated. Carlson et al. (2017) report that discussions about GBV do contribute to ending it and that the long-term goal should be to increase activism about GBV, leadership of gender initiatives, and to increase attendance at GBV-related events. All the respondents indicated that they had participated in discussions about ending GBV, which means that they are all part of ending the scourge.
Discussion and Conclusion
The preceding analysis of the responses to the online survey compared the responses with the questions to trends in the literature. The responses resonated to a large extent with existing literature, especially in terms of the respondents’ awareness of what is meant by GBV. They showed advanced knowledge of what is meant and included in the phenomenon of GBV, including marital rape and physical assault. This was to be expected from staff at a higher education institution, who would have access to specialized knowledge and vocabulary. The responses to questions about experiences of GBV diverge from those reported in the literature, which frequently notes that GBV occurs in situations where there is a power inequality, such as in discussion between subordinates and their line managers. The majority of respondents did not report that they had felt unsafe or threatened in discussions with their line managers, in contrast to what might have been expected from other studies. Moreover, the responses regarding reporting of GBV were in line with existing statistical trends. These trends show a disappointing tendency not to report incidents of GBV, due to a variety of factors, including fear of social stigma and fear of repercussion. GBV thus becomes a silent scourge, affecting mostly women, who are frequently marginalized and made invisible through their inability to speak out about their experiences.
As this was a limited study with only eight respondents, the researchers hypothesized that it would not be possible to extrapolate significant trends from their responses. It was therefore unexpected that the responses would correlate so closely with trends reported in existing literature. Nevertheless, the researchers caution that it is not advisable to rely only on existing literature, but that the responses had pointed to trends that could be further explored by means of in-depth interviews and focus groups among respondents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research that formed the basis for this article was funded by a grant from Unisa’s Women in Research (WiR) fund.