
Abstract
Nurses are essential in coordinating palliative care among healthcare teams, yet nursing education still lacks explicit focus on this area. This study aims to explore nursing students’ competencies including palliative care knowledge (PCKN), attitudes toward death and end-of-life care (ADEoLC), perceived self-efficacy in EOL care (PSEC), ethical understanding in palliative care (EUPC), and fear and stress related to providing EOL care (FSEC), as well as the relationships among these variables. A cross-sectional descriptive correlational design was employed to examine the relationships among those variables. The sample consisted of 355 fourth-year undergraduate nursing students. Data were collected using six questionnaires: Personal Information Questionnaire (PIQ), PCKN Questionnaire, ADEoLC Questionnaire, PSEC Questionnaire, EUPC Questionnaire, and FSEC Scale. The study found that nearly half of the students (51%) exhibited low PCKN, with a mean score of 19.59/32. The average score for ADEoLC was 94.75/125, with 64.2% demonstrating a positive attitude. The mean score for PSEC was 69.90/100, while the mean score for EUPC was 3.30/5. Fear and stress related to providing end-of-life care scored 3.78 and 5.11 out of 10, respectively. PCKN was positively correlated with ADEoLC and EUPC but not with PSEC. ADEoLC was positively correlated with both PSEC and EUPC. PSEC was positively correlated with EUPC. Fear was correlated with stress related to end-of-life care, but neither was associated with other variables. The results provide the basic information for appropriate planning to enhance nursing student competencies to provide quality palliative and end-of-life care.
Plain language summary
Nurses play an essential role in palliative care, yet nursing education doesn’t give this area enough attention. To explore this issue, a study was conducted with 355 fourth-year nursing students to examine their competencies, including knowledge, attitudes, self-efficacy, ethical understanding, and fear and stress related to providing end-of-life care. The findings revealed that nearly half of the students had limited palliative care knowledge. Despite this, most had a positive attitude toward providing end-of-life care. While the students felt moderately self-efficacy and ethically prepared to handle such situations, they also experienced noticeable fear and stress. The study found that greater knowledge was associated with more positive attitudes and stronger ethical understanding, although it did not necessarily increase self-efficacy. Similarly, students with positive attitudes were more likely to feel confident and ethically grounded in their approach. On the other hand, fear and stress were closely connected to each other but were not linked to the other factors studied. These findings underline the need to enhance nursing education to better equip students for the challenges of palliative and end-of-life care.
Background
Palliative care, as redefined by the International Association for Hospice and Palliative Care, is the active, holistic care of individuals across all ages with serious health-related suffering due to severe illness and especially of those near the end of life. It aims to improve the quality of life of patients, their families, and their caregivers (Radbruch et al., 2020). In 2014, the World Health Assembly adopted resolution WHA67.19, underscoring the ethical imperative of integrating palliative care into all levels of health systems, with particular emphasis on primary care (WHA, 2014). The global health burden has increasingly shifted from communicable diseases to non-communicable diseases (NCDs), which are often chronic and incurable. Despite this shift, access to palliative care remains limited, with only 39% of countries reporting its general availability (WHO, 2019). Notably, individuals aged 70 and older comprise 40% of the global population in need of palliative care (Connor, 2020).
A 2020 national survey in Thai tertiary hospitals reported that 18.7% of inpatients (N = 1,079) required palliative care, yet only 17.3% received it (Pairojkul et al., 2021). Thailand, one of the world’s fastest-aging nations, has approximately 13 million older adults among its 66 million population (Department of Older Persons, 2024). In response, the National Health Commission introduced the “Health Promotion for Good Death” strategic plan (2014–2016), aiming to enhance end-of-life care through legal reforms, public education, and improved access to holistic services spanning physical, psychological, social, and spiritual needs (Milintangkul, 2015).The plan also prioritized health information systems, workforce training, and interdisciplinary collaboration. Although various palliative care models have since emerged, system-level improvements are still needed, particularly in service integration, opioid availability, referral systems, and outcome monitoring. Continued education and training for healthcare professionals remain critical to ensuring nationwide access to high-quality palliative care (Chaiviboontham & Pokpalagon, 2021).
According to the World Health Organization, competencies are the knowledge, skills, and behaviors necessary for effective role performance (WHO, 2015). Given that nursing students typically have limited experience in palliative care, self-efficacy is included in this study as a key focus, serving as a robust proxy for behavior by reflecting an individual’s perceived ability to perform specific tasks effectively (Bandura, 1986). Attitudes, reflecting an individual’s values, beliefs, and feelings toward a particular subject or action, are significant influencers of skill development and the propensity to behave in certain ways (Cowan et al., 2005). A comprehensive assessment of palliative care competence should encompass knowledge, skills, and observable clinical behaviors. In Thailand, nursing competencies in palliative care are defined across nine domains: (1) patient and family care, (2) pain and symptom management, (3) end-of-life care, (4) grief and bereavement support, (5) communication and counseling, (6) spirituality, religion, and culture, (7) ethical and legal issues, (8) interdisciplinary collaboration, and (9) teaching and knowledge dissemination (TNMC, 2015). Despite the significance of these competencies, Thailand lacks a dedicated undergraduate framework for palliative care. The current Bachelor of Nursing Science curriculum includes limited content—averaging only 4 hr of theoretical instruction and incidental clinical exposure (Tipseankhum, 2020). This insufficient and inconsistent training may contribute to varying levels of preparedness and confidence among nursing graduates. Moreover, assessing clinical behaviors poses methodological challenges, particularly among students with minimal real-world experience in end-of-life care. Therefore, this study, while acknowledging the importance of all three components of competence, strategically focuses on knowledge, attitudes, and self-efficacy as measurable constructs. As defined by Bandura’s Social Cognitive Theory (Bandura, 1986), self-efficacy is a robust proxy for behavior that reflects a person’s perceived ability to perform specific behaviors effectively.
The theoretical framework underpinning this study draws upon Social Cognitive Theory (SCT), particularly the concept of self-efficacy (Bandura, 1986). The theory posits that an individual’s behavior is influenced by the dynamic interaction of personal factors (including knowledge and attitudes), behavioral factors, and environmental factors. Within this framework, self-efficacy refers to an individual’s belief in their capacity to execute behaviors necessary to produce specific performance attainments (Bandura, 1986). In the context of this study, we propose that nursing students’ knowledge of palliative care principles and practices, particularly concerning end-of-life care, forms a foundational personal factor. This knowledge can then influence their attitudes toward providing such care. Furthermore, according to social cognitive theory, these cognitive and affective factors contribute significantly to the development of self-efficacy, which is the students’ belief in their ability to competently perform end-of-life care tasks. Higher levels of knowledge and more positive attitudes are theorized to foster greater self-efficacy, leading to actual behaviors and the quality of care they are likely to provide.
Within the SCT, fear and stress are understood as products of dynamic interactions among personal, behavioral, and environmental factors, rather than solely internal traits or external triggers (Bandura, 1986). Personal elements such as beliefs, self-efficacy, and emotional states like anxiety interact with behavioral responses, such as coping strategies or avoidance, and environmental influences, including social support and chronic stressors, to shape how individuals perceive and respond to threats. This triadic reciprocity illustrates the ongoing interplay between cognition, behavior, and context in shaping emotional experiences (Bandura, 1986). Self-efficacy and fear represent a negative relationship, particularly when individuals feel unprepared to manage challenging situations, potentially leading to avoidance and even phobic responses. Conversely, high self-efficacy fosters a sense of control and confidence, thereby reducing fear and promoting adaptive coping (Lipp et al., 2023). Stress and self-efficacy are interrelated; low self-efficacy may elevate stress levels, while high stress can undermine self-efficacy. Research indicates a negative correlation between perceived stress and general self-efficacy among college students (Liu et al., 2024).
Previous studies have consistently shown that undergraduate nursing students often lack adequate knowledge in palliative care (Aboshaiqah, 2020; Zhou et al., 2021), despite generally positive attitudes toward death and end-of-life (EOL) care (Alwawi et al., 2022; Zhou et al., 2021). Research also indicates that students’ self-efficacy in delivering palliative care ranges from low to moderate (Kim et al., 2020; Zhou et al., 2021). Graduating students frequently report feeling unprepared to meet palliative care competencies, highlighting the need for enhanced educational efforts to build self-efficacy in this area (Henderson et al., 2016). Moreover, studies have identified significant associations between palliative care knowledge, attitudes toward EOL care, and perceived self-efficacy (Aboshaiqah, 2020; Kim et al., 2020; Zhou et al., 2021). According to Bandura’s self-efficacy theory, individuals’ perceptions of their abilities are shaped by physical and emotional cues; experiences of strength versus strain, calmness versus stress, or energy versus fatigue can significantly affect confidence and persistence (Bandura, 1997). These internal cues play a critical role in shaping self-efficacy (Lipp et al., 2023). Ethical understanding is crucial to effective palliative care practice. A systematic review with narrative synthesis among specialist palliative care practitioners identified six themes: application of ethical principles; delivering clinical care; working with families; engaging with institutional structures and values; navigating societal values and expectations; philosophy of palliative care (Schofield et al., 2021). Our study focuses on the application of ethical principles among less-experienced nursing students. Ethical challenges related to truth-telling include whether to disclose a terminal diagnosis or prognosis to patients and families, and whether withholding information is justified based on perceived harm or family wishes. The doctrine of double effect also presents dilemmas, particularly in cases involving opioid prescriptions and their unintended consequences (Schofield et al., 2021).
The limited application of SCT in explaining the interrelationships among knowledge, attitudes, and self-efficacy, particularly in undergraduate nursing education in palliative and end-of-life (EOL) care, highlights a significant theoretical gap. Key factors such as fear, stress, and ethical understanding remain insufficiently examined. Addressing this gap, the present study aims to assess the competencies of Thai nursing students namely, knowledge, attitudes, and self-efficacy related to EOL care through the lens of Social Cognitive Theory. By examining the interplay of these constructs, this research seeks to generate insights into nursing students’ preparedness to deliver compassionate and competent care to patients and families facing end-of-life situations in Thailand. The findings are expected to inform educational strategies, enhance curriculum development, and promote the cultivation of confident, knowledgeable, and empathetic future nurses in the field of palliative care
Objective
This study aims to explore nursing students’ competencies including palliative care knowledge, attitudes toward death and end-of-life care, perceived self-efficacy in EOL care, ethical understanding in palliative care, and fear and stress related to providing EOL care, as well as the relationships among these variables.
Methods
Study design: A cross-sectional descriptive correlational design was used to examine the relationship among palliative care knowledge, attitudes toward death and EOL care, perceived self-efficacy in EOL care, ethical understanding in palliative care, fear, and stress related to providing EOL care.
Sample and setting: The sample size was calculated using G*power (Faul et al., 2009) with α set at .05, 1 − β at .80, effect size at .15. The initial calculation indicated a required sample size of 346 participants, with an additional 10% added, bringing the total to 380 participants for this study. Nevertheless, the questionnaires were completely returned by only 355, which still provided an adequate sample size for the study’s requirements. This study utilized convenience sampling in settings with curricula aligned with the Thailand Nursing and Midwifery Council guidelines, including a university school of nursing and a military college of nursing. A total of 355 fourth-year undergraduate nursing students participated, with 202 enrolled at the university and 153 at the military college under the Ministry of Defense. Notably, the nursing curriculum in these settings did not include elective courses or subjects specifically focused on palliative care. Instead, limited theoretical content on end-of-life (EoL) care was integrated into broader subjects such as Fundamental Nursing and Adult and Gerontological Nursing. Consequently, students’ opportunities to practice EoL care were limited to clinical settings as they arose.
Ethical considerations: This study was approved by the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA: MURA 2017/232). The study strictly adhered to ethical guidelines outlined in the Declaration of Helsinki. All participants were provided with comprehensive information regarding the study’s objectives and procedures, and their participation was voluntary. Confidentiality of the participants was ensured, and they had the option to withdraw from the study at any point without providing a reason or facing any consequences. Written consent was obtained from all participants prior to their involvement in the study.
Data collection: The data collection process was conducted between February to March 2018. The data collection was conducted by the researcher following ethical approval. The researcher reviewed the list and number of nursing students from a university and a military nursing school. Eligible participants were selected based on predefined criteria. Data collection was scheduled during non-teaching hours, with 1 day allocated per institution after coursework completion to avoid academic disruption. The researcher met participants in a classroom, introduced the research study, and explained their rights, including the option to decline without academic consequences. Time was provided for questions, and those who agreed signed a consent form. Participants completed the questionnaire independently, reading and responding to items independently. During completion, participants were instructed to respond by starting with the questionnaire from a to f as detailed, not to seek external information or discuss the questions with peers, but to consult the researcher if they had any questions. Completion took approximately 35 to 40 min, and participants were allowed to take short breaks as needed to maintain concentration and data quality. The researcher reviewed all returned questionnaires for completeness and identified 25 with missing data. These incomplete responses were excluded from the final analysis to ensure data integrity.
Measurements
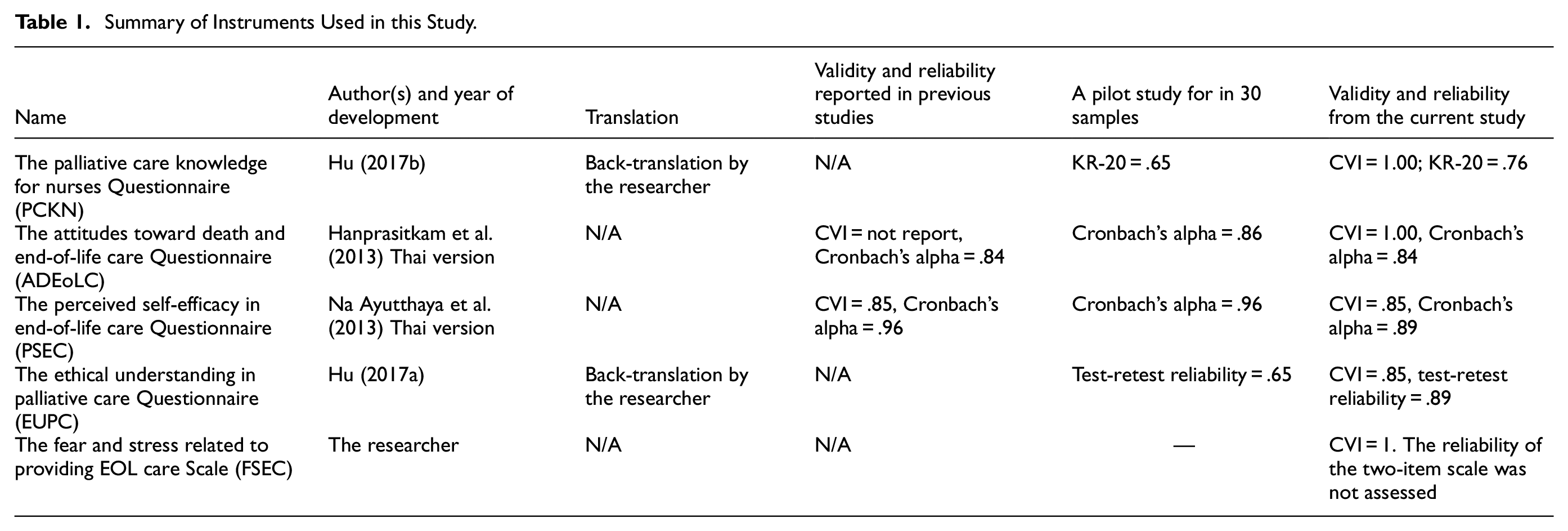
The questionnaires used in this study included (a) the Personal Information Questionnaire (PIQ), (b) the Palliative Care Knowledge for Nurses Questionnaire (PCKN), (c) the Attitudes Toward Death and End-of-Life Care Questionnaire (ADEoLC), (d) the Perceived Self-Efficacy in End-of-Life Care Questionnaire (PSEC), (e) the Ethical understanding in palliative care Questionnaire (EUPC), and (f) the Fear and Stress Related to Providing EOL Care Scale (FSEC). All questionnaires were validated by three experts and pilot tested for reliability in 30 samples which not included in the main study.
The PIQ was developed by the researcher to gather information on age, gender, religion, EoL care experience, training experience, and educational and training needs. The content validity index (CVI) was 1.00.
The PCKN was developed by Hu et al. (2017b) at the School of Nursing, National Taiwan University, to evaluate the principles and knowledge about palliative care, such as symptom management and psychological and spiritual care. This unpublished questionnaire was granted to be translated into Thai by the developer. The 32-item questionnaire was designed based on the literature, with the main reference being the PCQN (Ross et al., 1996). The scoring system used “true (1)” and “false/unknown (0).” The overall score of PCQN ranges from 0, “lowest level of knowledge,” to 32, “highest level of knowledge.” A score of over 80% correct answers or more than 26 points indicates a high knowledge level; 61% to 80% correct answers or 20 to 26 points indicates a moderate knowledge level; and 60% or fewer correct answers or fewer than 20 points indicates a low knowledge level. The content validity index (CVI) shows 1.00, while the internal consistency by Kuder–Richardson formula 20 (KR-20) was 0.76.
The ADEoLC assesses perceptions and beliefs regarding end-of-life care. It was developed by Hanprasitkum et al. (2013) in the Thai language based on a literature review and granted to be used in this study. The questionnaire consists of 25 items with responses on a 5-point Likert scale ranging from strongly disagree (1 point) to strongly agree (5 points). The questions include positive and negative aspects, with the scores for the negative items being reversed before the total score was calculated. The total score ranges from 25 to 125 points, with higher scores indicating a more positive attitude towards end-of-life care. A score of 93 to 125 points indicates a high attitude, 60 to 92 points indicates a moderate attitude, and 59 points or lower indicates a low attitude. The CVI shows 1.00, while the internal consistency shows Cronbach’s alpha of .84.
The PSEC, developed by Na Ayutthaya et al. (2013) in the Thai language based on a literature review and granted to be used in this study, is a 5-point Likert scale with 20 items designed to assess nurses’ self-efficacy in providing end-of-life care. Scores range from 1 (not confident) to 5 (extremely confident), with total scores ranging from 20 to 100, where higher scores indicate greater self-efficacy. The CVI was .85, and reliability testing yielded a Cronbach’s alpha of .89.
The EUPC was the unpublished questionnaire developed by Hu and colleagues at the School of Nursing (Hu, 2017a), National Taiwan University, and was granted to be translated into Thai. This 5-point Likert scale consists of 4 items to evaluate understanding of the major ethical issues in palliative care. The scores ranged from 1 (strongly disagree) to 5 (strongly agree). The higher scores indicate greater understanding. The CVI of this instrument was .85, while the test-retest reliability was .79.
The FSEC is a two-item scale for evaluating the feelings of fear and stress in providing EOL care created by researcher. This rating scale ranges from 0 to 10; a higher score refers to the higher fear and stress. The CVI of this instrument was 1, while the reliability of the two-item scale was not assessed.
The back-translation process was applied to translate the PCKN and EUP tools. One bilingual translator translated the questionnaire into the target language, and another independently translated it back into the source language. Native English speakers reviewed both versions to identify discrepancies, and revisions were made to ensure linguistic and conceptual accuracy before validation by three experts. All instruments were summarized in Table 1.
Summary of Instruments Used in this Study.
Data Analysis
Personal information and scores on the PCKN, ADEoLC, PSEC, EUPC, and FSEC were analyzed using frequency, percentage, mean, and standard deviation. Relationships among these variables were examined with Pearson’s Product Moment Correlation Coefficient, following the Kolmogorov-Smirnov test to assess normal distribution.
Results
A total of 355 fourth-year undergraduate nursing students completed the questionnaire. The average age was 22.3 years (SD = .64), aged 21 to 26 years. Most participants were female (95.5%) and identified as Buddhist (97.5%). Most had experience with end-of-life (EoL) care and had received information about palliative care. Further details on participant characteristics are provided in Table 2. The participants’ mean scores and levels of Palliative Care Knowledge, Attitudes toward death and end-of-life care, Perceived self-efficacy in EOL care, Ethical understanding in palliative care, and Fear and Stress related to providing EOL care are presented in Table 3. For the educational and training needs, the communication skills for terminally ill patients were in the highest demand for training follow by psychological care, spiritual care, legal and ethical issues, caring for families after a patient dies, symptom management, utilization of resources from the community, the lowest was the philosophy and principles of palliative care. As shown in all the details in the Supplemental Tables.
Participants’ Characteristics (N = 355).

The Descriptive of Participants’ Palliative Care Knowledge, Attitude Toward Death and EOL Care, Perceived Self-Efficacy in EOL Care, Ethical Understanding in Palliative Care, and Fear and Stress Related to Providing EOL Care (N = 355).

Palliative Care Knowledge
Almost half of the students have low palliative care knowledge (51.0%). The mean score was low, with 19.59 (SD = 2.90; Table 2). As shown in Figure 1, the five most correct answers were items 27, 28, 24, 21, and 22 (92.4%, 92.1%, 91.3%, 89.9%, and 89.9%), while the most incorrect items were items 5, 19, 15, 25, and 7 (95.8%, 76.3%, 70.4%, 69.9%, and 69.9%).

The percentage of correct and incorrect responses for each PCKN item (N = 355).
Attitude Toward Death and EOL Care
The average total score for attitudes toward death and EOL care was 94.75 (SD = 9.73). Most participants (64.2%, n = 228) demonstrated a good attitude, while 35.8% (n = 127) showed a moderate attitude; no participants scored in the low range (Table 3). As shown all detail in Table 4, the top three items with the highest average scores were: Item 11, 16, and 17. Conversely, the items with the lowest average scores were Item 8, 1, and 20.
Attitude Toward Death and EOL Care (N = 355).

Perceived Self-Efficacy in EOL Care
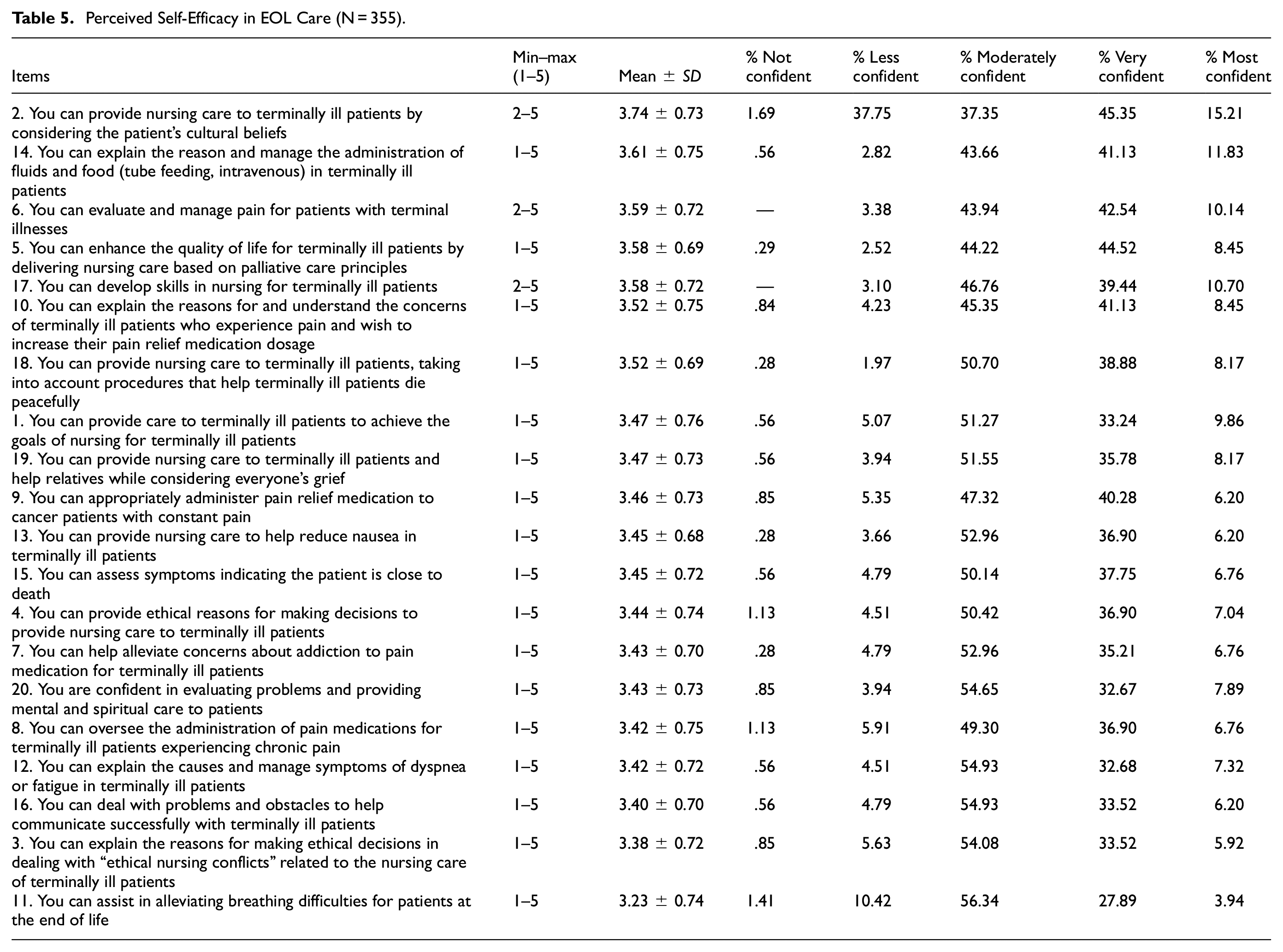
The mean of the total score for perceived self-efficacy in EOL care was 69.90 (SD = 10.93; Table 3). As shown in Table 5, the item with the highest average score was 2, followed by 14, and 6. The item with the lowest average score was 11.
Perceived Self-Efficacy in EOL Care (N = 355).
Ethical Understanding in Palliative Care
As shown in Table 6, the highest average score is Telling the truth, while the lowest one is administering sedative drugs to soothe a patient with uncontrollable symptoms is ethically appropriate.
The Descriptive of Ethical Understanding in Palliative Care.

The Relationship Between Palliative Care Knowledge, Attitude Toward Death and EOL Care, Perceived Self-Efficacy in EOL Care, Ethical Understanding in Palliative Care, and Fear and Stress Related to Providing EOL Care
Palliative care knowledge was statistically positively correlated with attitude toward death and EOL care (r = .109, p < .05), and Ethical understanding in palliative care (r = .108, p < .05) but was not correlated with perceived self-efficacy in EOL care. Attitude toward death and EOL care was statistically positively correlated with perceived self-efficacy in EOL care (r = .243, p < .01) and Ethical understanding in palliative care (r = .211, p < .01). Perceived self-efficacy in EOL care was statistically positively correlated with Ethical understanding in palliative care (r = .169, p < .01). Fear related to providing EOL care was statistically positively correlated with Stress to providing EOL care (r = .630, p < .01). Fear and stress related to providing EOL care were not correlated with other variables. As shown in Table 7.
The Relationship Among Palliative Care Knowledge, Attitude Toward Death and End-of-Life Care, Perceived Self-Efficacy in Palliative Care, Ethical Understanding in Palliative Care, and Fear and Stress Related to Providing EOL Care (N = 355).

p < .05. **p < .01.
Discussion
This study revealed that nearly half of fourth-year undergraduate nursing students demonstrated a low level of knowledge about palliative care. This could justify the limited inclusion of content on palliative and end-of-life (EOL) care within the nursing curriculum in Thailand. Rather than being addressed as a standalone subject, these topics are incorporated into broader courses, such as Fundamental Nursing and Adult and Gerontological Nursing, with no specific allocation to practicum courses. This is consistent with findings from other countries; China (Meng et al., 2023; Zhou et al., 2021), Malaysia (Ibrahim et al., 2024), Spain (Chover-Sierra & Martínez-Sabater, 2020), and Palestine (Alwawi et al., 2022). The low scores reported in those studies may be attributed to insufficient palliative care education within nursing curricula (Alwawi et al., 2022; Meng et al., 2023).
Questions related to the philosophy and core concepts of palliative care had the highest accuracy rates, exceeding 90%. In contrast, knowledge of symptom management was notably weaker, with correct responses ranging from 30% to 53%. A particularly striking finding was that 95.8% of participants incorrectly answered the question about whether families are required to stay at the patient’s bedside until death (False). These results suggest that a culturally relevant observation is the high rate of incorrect responses to the bedside presence question, potentially reflecting the strong emphasis on familial bonds in Thai and other Eastern cultures, where staying with a dying loved one is often seen as a moral or cultural duty.
Most participants demonstrated a good attitude, while one-third of them showed a moderate attitude; no participants scored in the low range. The study is congruent with the previous study (Alwawi et al., 2022; Haroen et al., 2023; Laporte et al., 2020; Meng et al., 2023; Shigwedha et al., 2022). The characteristics of participants show that nearly half of them reported having prior experience with EOL care, and the majority had received information about palliative care. The experiences with terminally ill patients were identified as the most significant factor shaping attitudes toward EOL care, followed by personal experiences with a relative (Laporte et al., 2020). This could explain that a positive attitude may be attributed to students’ recognition of caring and providing holistic, compassionate care as fundamental values of the nursing profession.
The findings provide partial support for the SCT, which posits a relationship between personal factors (knowledge, attitudes, ethical understanding, fear, stress), behavioral factors (providing EOL care), and environmental factors (curriculum, cultural context). The study found a statistically significant positive correlation between palliative care knowledge and attitude toward death and EOL care. Previous research has similarly demonstrated that higher levels of palliative care knowledge are significantly associated with more positive attitudes toward palliative care (Lo Iacono et al., 2023; Meng et al., 2023). This suggests that as students’ knowledge of palliative care principles increases, their attitudes towards death and providing EOL care tend to become more positive. This aligns with the SCT assertion that knowledge, as a personal factor, can influence affective states and beliefs (Bandura, 1986).
Contrary to the SCT framework, the study found no statistically significant correlation between palliative care knowledge and perceived self-efficacy in EOL care. Suggested that while knowledge of palliative care is present, it does not directly translate to a stronger belief in one’s ability to perform EOL care tasks. This finding remains a subject of ongoing debate and inconsistency in the literature (Kim et al., 2020; Zhou et al., 2021), which warrants further exploration. It is possible that the type or depth of knowledge assessed was insufficient to impact self-efficacy. For instance, a strong understanding of philosophical principles (as indicated by high accuracy rates in those areas) might not directly build confidence in performing specific practical skills like symptom management, where knowledge was lacking. Studies highlight the effectiveness of palliative care education for nursing students, including an online palliative care course (Sayın Kasar, 2023), a two-week palliative care course during clinical internships (Haroen et al., 2023), and a simulation program (Yoong et al., 2023). Educational activities involving scenario-based simulations enhanced students’ confidence and self-efficacy by allowing them to practice discussing patients’ goals, fears, and end-of-life preferences (Rauch et al., 2023). This underscores the value of enactive mastery experiences (Bandura, 1986), which may be insufficiently incorporated into the current curriculum.
The study found positive correlations between ethical understanding and palliative care knowledge, attitudes toward EOL care, and self-efficacy. A strong ethical foundation enhances knowledge, attitudes, and confidence in EOL care, potentially reducing anxiety and increasing competence. This aligns with Social Cognitive Theory, which highlights the role of personal factors, such as values and beliefs, in shaping self-efficacy (Bandura, 1986). Key ethical issues included truth-telling, the right to care, nutrition, and medication for symptom management.
The lack of correlation between fear, stress, and other variables (knowledge, attitude, self-efficacy, ethical understanding) is noteworthy and requires further investigation. Similar findings were reported in studies from China and Spain, where fear was not linked to attitudes toward EOL care, but decreased with advanced clinical experience (Li et al., 2023; Maestro-González et al., 2025). According to Social Cognitive Theory, low self-efficacy can increase fear and stress (Lipp et al., 2023; Liu et al., 2024), suggesting that limited practical experience or the emotional challenges of EOL care may be more influential in this context.
The study’s observation that limited dedicated curriculum time and lack of specific lecture hours and practicum in palliative care may contribute to knowledge gaps highlights the role of environmental factors in SCT. The structure of the nursing program influences the learning opportunities and skill development, which in turn can impact knowledge and self-efficacy. Furthermore, the culturally significant finding regarding families’ need to stay at the bedside underscores how environmental factors, such as cultural norms, can influence beliefs and attitudes towards EOL care.
Strengths and Limitations
This study possesses several notable strengths. Grounded in Social Cognitive Theory (SCT), it offers a strong theoretical foundation to explore the complex relationships among knowledge, attitudes, self-efficacy, fear, stress, and ethical understanding in the context of end-of-life (EOL) care. Integrating cognitive, emotional, and ethical dimensions allows for a comprehensive view of nursing students’ readiness to provide palliative care, representing their competencies. Additionally, a large sample size enhances the reliability and precision of the results. The cultural contextualization of findings, particularly regarding familial expectations at the end of life, adds valuable insight to the global discourse on palliative care education.
However, several limitations should be acknowledged. The cross-sectional design limits the ability to draw causal inferences and does not capture how students’ competencies develop over time. The use of convenience sampling from Thailand restricts the generalizability of findings to other cultural or educational contexts. Self-reported questionnaires may be subject to response bias, with participants potentially overestimating their knowledge or self-efficacy. Although steps were taken to reduce fatigue, the questionnaire’s length (approximately 80 items) may have impacted response accuracy. Additionally, the brief measure used to assess ethical understanding may not fully capture the complexity of ethical issues in palliative care. The study also does not deeply examine how Thai cultural factors influence students’ attitudes and self-efficacy. Finally, the lack of correlation between fear, stress, and other variables is an unexpected finding that warrants further investigation to better understand their independent role in end-of-life care preparation.
Recommendation
Future research should focus on longitudinal studies to assess the long-term impact of palliative care education and clinical experience on nursing students’ competencies. A more diverse and randomized sample, incorporating participants from various regions and backgrounds, is essential, and multi-center studies across different countries would offer a broader perspective on palliative care competencies. Additionally, future studies should include objective measures of competency, such as clinical performance evaluations or standardized tests, and consider mixed-methods approaches, like qualitative interviews or focus groups, to provide deeper insights into students’ experiences. Cultural factors should be explored in greater depth, potentially through qualitative methods, to understand how cultural beliefs influence attitudes and self-efficacy. The use of more comprehensive instruments and methods, such as ethical case discussions or reflective journals, could offer a richer understanding of students’ ethical reasoning. Lastly, investigating the sources of fear and stress in end-of-life care through qualitative interviews would be valuable, with findings used to develop interventions such as stress management workshops, mentorship programs, or peer support groups to help students manage the emotional challenges of palliative care.
Conclusion and Implications for Nursing Education
In conclusion, while the study provides some support for the relationships proposed by SCT, particularly between knowledge and attitudes, and attitudes and self-efficacy, the lack of a direct link between knowledge and self-efficacy, and the unique findings regarding fear and stress, suggest the need for a more nuanced application of the theory in the context of palliative care education for Thai nursing students. Addressing the identified knowledge gaps through curriculum reform and focusing on building self-efficacy through practical experiences are crucial steps in preparing competent and confident future palliative care nurses.
Based on the SCT framework and these findings, interventions aimed at enhancing nursing students’ self-efficacy in palliative care should go beyond simply increasing theoretical knowledge. Incorporating more hands-on clinical experiences, simulation-based learning focused on symptom management, and opportunities for positive enactive mastery experiences are crucial. Furthermore, addressing attitudes through reflective exercises and discussions, alongside strengthening ethical understanding, may indirectly boost self-efficacy. Recognizing and addressing culturally specific beliefs about EOL care within the curriculum is also essential for providing culturally sensitive education. Future research could explore the specific types of knowledge and experiences that most significantly impact self-efficacy in EOL care among nursing students in this cultural context.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251368448 – Supplemental material for Palliative Care Competencies of Undergraduate Nursing Students in Thailand
Supplemental material, sj-docx-1-sgo-10.1177_21582440251368448 for Palliative Care Competencies of Undergraduate Nursing Students in Thailand by Suchira Chaiviboontham, Piyawan Pokpalagon, Autchareeya Patoomwan, Tiraporn Junda, Bualuang Sumdeangrit and Kanitha Hanprasitkum in SAGE Open
Footnotes
Acknowledgements
The authors extend gratitude and acknowledge all participants for their invaluable cooperation in this study.
Ethical Considerations
This study was approved by the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA: MURA 2017/232). The study strictly adhered to ethical guidelines outlined in the Declaration of Helsinki. All participants were provided with comprehensive information regarding the study’s objectives and procedures, and their participation was voluntary. Confidentiality of the participants was ensured, and they had the option to withdraw from the study at any point without providing a reason or facing any consequences. Written consent was obtained from all participants prior to their involvement in the study.
Consent to Participate
All participants were asked for informed consent before filling out the questionnaire.
Consent for Publication
Not applicable.
Author Contributions
SC: Conceptualization; methodology; data collection and analysis; project administration; resources; first draft writing and editing; provide conclusion and recommendation. PY: Conceptualization; methodology; data analysis; validation; writing and editing; provide conclusion and recommendation; finalized the final version; corresponding author. BS and TJ: Conceptualization; methodology; data analysis; writing review and editing; provide conclusion and recommendation. AP and KH: Conceptualization; methodology; writing review and editing; provide conclusion and recommendation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.