
Abstract
Achieving good health in retirement has become a key priority for aging societies. This study examines the relationship between retirement and retirees’ health in rural Vietnam, using data from the Thailand Vietnam Socio-Economic Panel. The analysis employs multiple approaches, including fixed effects, random effects, and instrumental variable models, to assess the impact of retirement on health, with a focus on various health indicators. The study found that retirement is linked to a positive change in body mass index (BMI, measured in kilograms per meter squared [kg/m2]) among rural Vietnamese populations, but the effect varies by socio-demographic factors. Men and the Kinh ethnic majority experienced an increase in BMI, while women and ethnic minorities did not. These findings not only highlight the positive impact of retirement on health but also emphasize the importance of developing tailored health programs and policies to support diverse groups of retirees in rural areas, where access to healthcare and social services may be limited. The study contributes to the existing literature on retirement and health in emerging economies, offering critical insights for policymakers, healthcare providers, and employers to design effective interventions that address the unique needs of Vietnam’s aging population.
Introduction
Retirement has been drawing attention in labor economics as a significant life transition for many older adults, representing a major change in daily routines, social roles, and financial circumstances (Hansson et al., 2018). Empirical evidence shows that retirement can have both positive and negative effects or no major impact on the mental health of older individuals. On the positive side, a number of studies have found a positive effect of retirement on well-being (Gorry et al., 2018; Latif, 2011; Zhu & He, 2015). Intuitively, retirement can provide opportunities for increased leisure time, improved health, and reduced stress. Some studies have found that retirement can lead to improved mental and physical health (Gall et al., 1997; Tran & Zikos, 2019; Westerlund et al., 2010). Retirement can also have an impact on social connections and relationships (Comi et al., 2022). On the opposite side, retirement is found to be related to a lower level of life satisfaction (Bonsang & Klein, 2012), social isolation/loneliness (Shin et al., 2019), reduced income (Segel-Karpas et al., 2013), worse physical and mental health, and a lost sense of purpose (P. L. Hill & Weston, 2019). Diverging from the clear evidence, another strand of empirical literature indicates that retirement has no major impact on well-being (Fonseca et al., 2014).
Vietnam has undergone significant socio-economic changes, including the development of market relations and the transformation of traditional society. These changes have created forms and levels of socio-economic risk for the elderly population. In 2023, the proportion of people over 65 years old in Vietnam was 9% and was projected to be 14% by 2036 (United Nations Population Fund, 2023). This trend in the aging population is potentially due to factors such as increased life expectancy, declining birth rates, and the aging of the baby boomer generation. The main source of Vietnamese old people’s income comes from children’s support (38%). While the policy of raising the retirement age has just been implemented, only 15% of Vietnamese old people receive pensions and 10% receive social support. Numerous old Vietnamese are reported to be struggling with life due to financial burdens (International Labor Organization [ILO], 2022). The current situation reflects the contrast and inadequacy of retirement and health regulations. Moreover, the aging population is expected to have significant social and economic impacts, including increased demand for healthcare and aged care services, changes to the labor force and workforce participation rates, and potential strain on government budgets and social welfare programs. Thus, understanding the effects of retirement on health would be valuable in the context that this demographic group becomes a larger proportion of the population and resources to support them become scarce. Moreover, Vietnam has a significant rural population. In 2022, the proportion of Vietnamese that lived in rural areas was roughly 66% (World Bank, 2023). As a result, the necessity to enhance the health of older individuals in rural Vietnam has been becoming increasingly critical.
Studies on retirement and health in Vietnam are necessary due to the socio-economic changes, unique experiences of older adults, and inadequate evidence on the effect of retirement on health. By conducting this research, the findings can contribute to the knowledge about retirement and its impact on health in Vietnam, which can inform the development of policies and interventions to support the aging population in the country. In particular, the findings of this study will provide critical academic and practical implications. First, the results will contribute to the existing literature on health economics and labor economics about the relationship between retirement and health in rural Vietnam. Second, the current research provides valuable insights for policymakers, employers, and healthcare professionals, who can use this information to develop programs and interventions to support retirees in rural Vietnam in maintaining good health.
To contribute to the existing literature, this study examines the effect of retirement on health from several different perspectives. First, this study is one of a few to examine the effect of retirement on health in Vietnam. Second, the endogeneity of the retirement variable which is normally neglected in previous literature in Vietnam is addressed. Lastly, the dataset employed is collected from rural Vietnam in three provinces Hue, Dak Lak, and Ha Tinh to reduce the heterogeneity and contribute to the current literature in Vietnam.
The paper is structured as follows. The next section summarizes the literature so far in the field. Then, the methodology presents the data source, key variables and estimation method. The fourth section illustrates the results using various estimation methods. It comes to the discussion section next, and the last section concludes the paper.
Literature Review
The impact of retirement on health can be both positive and negative, as numerous longitudinal studies indicate potential benefits for both physical health and mental well-being. Fruitful evidence has shown that retirement improves general health (Coe & Zamarro, 2011) and enhances physical functioning (Joyce et al., 2010; Mänty et al., 2018). Gorry et al. (2018) utilized panel data to investigate retirement’s impact on health, life satisfaction, and healthcare utilization, providing strong evidence that retirement enhances self-reported health, mental well-being, and life satisfaction while improving functional limitations over time. Fleischmann et al. (2020) further supported the positive association between retirement and mental health, suggesting that retirement can serve as a relief and contribute to overall well-being. These findings collectively suggest that, while retirement can enhance physical and mental health, its effects may vary based on individual and contextual factors. However, Jokela et al. (2010) found mixed results when examining the relationship between retirement, mental health, and physical functioning longitudinally, indicating variability in individual experiences.
The mechanisms underlying the heterogeneous effects of retirement on health have been widely studied. Nishimura et al. (2018) examined the reasons for variations in health outcomes following retirement, identifying the choice of analysis method as a key factor influencing previous findings. By applying a fixed analytical approach, they found positive effects of retirement on self-reported health, depression, and activities of daily living across several countries. However, the health effects of retirement are highly dependent on individual circumstances. For instance, voluntary retirement is generally associated with improved mental health, whereas involuntary job loss tends to have adverse effects (Picchio & Ours, 2020). Moreover, the health benefits of retirement may diminish over time (Jokela et al., 2010). Furthermore, the mode of retirement transition also plays a role in post-retirement well-being. Vaus et al. (2007) compared abrupt and gradual retirement and found no significant differences in positive post-retirement attitudes between the two groups. Additionally, Xue et al. (2020) conducted a systematic review on the impact of retirement on cardiovascular disease and its risk factors, reporting mixed findings—some studies indicated an increased risk among retirees, while others found no effect or a temporary increase in risk during the first year after retirement. Similarly, Zhou et al. (2020) analyzed data from China and found inconclusive evidence regarding the relationship between retirement and healthcare utilization. These findings underscore the complexity of retirement’s impact on health, highlighting the need for further research that considers individual and contextual factors.
The relationship between retirement and health in rural areas has been the focus of several studies, highlighting the unique challenges faced by retirees in these settings. Handley et al. (2021) investigated the impact of employment and retirement on the health and well-being of rural Australians, emphasizing the significant role of work transitions in shaping health outcomes. Laberon et al. (2019) examined retired farmers in rural France and found that the psycho-social transition to retirement significantly influences well-being and mental health. This psycho-social transition refers to the disruptive changes in socio-economic status and psychological perceptions associated with retirement, including whether it is perceived as a gain or loss, or as a positive or negative event (Laberon et al., 2019). Additionally, Sanders et al. (2016) analyzed healthcare utilization patterns among retirement-age migrants and long-term residents in rural areas, revealing distinct factors affecting healthcare access and selection between these groups. These findings emphasize the importance of studying retirement and health in rural contexts, where limited healthcare infrastructure, social isolation, and economic factors may further shape post-retirement well-being.
Research on the relationship between retirement and health in Vietnam remains limited. Dang (2022) emphasized the scarcity of studies examining the causal effects of retirement on health and healthcare utilization, underscoring the need for further research, especially as Vietnam’s aging population grows. Vu and Nguyen (2021) investigated the quality of life among district hospital nurses with musculoskeletal symptoms, finding that individuals in the 50 to 60 age range, which is the final working years before retirement in Vietnam, experienced a decline in quality of life. This finding suggests potential health challenges associated with the retirement transition. Given the handful studies assessing the causal relationship between retirement and health outcomes in Vietnam, it is essential to provide empirical evidence to enhance understanding of the broader health implications of retirement and to inform policies that improve well-being and healthcare access for retirees.
Methodology
Data
The Thailand Vietnam Socio Economic Panel—data is a dataset collected in rural provinces in Central Vietnam that are representative of rural areas characterized by agriculture, low incomes, and poor infrastructure. In close collaboration with research communities in Thailand and Vietnam, the Leibniz Universität Hannover and the University of Göttingen jointly conducted the research project. Nine surveys encompassing around 4,400 households in 440 villages across six provinces in Thailand and Vietnam were carried out between 2007 and 2022. The project aims to expand the panel household surveys conducted in Thailand and Vietnam in order to gain better knowledge of the development of income and poverty in both countries’ rural areas. One of the main guiding concepts of the data collection process is to produce high-quality data. The data will also facilitate the formulation of policies aimed at enhancing rural residents’ quality of life. Three provinces in Vietnam (Ha Tinh, Thua Thien Hue, and Dak Lak) are where the data is gathered. The Thailand Vietnam Socio Economic Panel data is ideal for our study because it provides information on our variables including health, retirement pension, and other demographic variables such as education, marital status, and economic sectors. Moreover, the format of the data is designed as panel data, allowing models such as fixed effects.
Key Variables
Retirement
Our first variable of interest is retirement. Given that the exact question about retirement status is not available in the dataset, we construct this variable as a binary for those who received retirement pensions. For simplicity, we have several assumptions relating to retirement status. We assume retirement is permanent, which means that they have no longer come back to employment (Bauger & Bongaardt, 2016; Yeung & Zhou, 2017). The current definition of self-reported retirement has often been used in different disciplines, including economics (Horner, 2014; Kesavayuth et al., 2016; Mazzonna et al., 2017), and has been shown to have good validity (Talaga & Beehr, 1995).
Health-Related Measurements
Our second variable of interest is health-related measurements. First, we use the self-reported health status, in which the respondents are asked how healthy they are at the time of being asked. If they answer “good” or “can manage,” the variable values one and zero otherwise. Similarly, respondents are asked to compare their health status last year and their health status 5 years ago. If they answer “better” or “same,” these two variables value one and zero otherwise. We strongly believe this variable is a complement to the previous one as it provides health status over time, rather than at one point in time. We also consider two other measurements of health, including having serious diseases and the body mass index (BMI). In the questionnaire, people were asked whether they had been suffering from any serious disease or injury. The answers span various diseases such as cancer, diabetes mellitus or coronary heart disease. If respondents report having experienced any serious disease or injury, the variable values one and zero otherwise. Lastly, as weight and height are provided in the data, we obtain the BMI by taking weight divided by squared height. Moreover, to eliminate potential outliers from the BMI, we winsorize this variable at the 1st and 99th percentiles. To sum up, our health-related dependent variables include current health status, health status compared to last year, health status compared to 5 years ago, serious diseases and BMI. However, all variables are self-assessed health status. Although it is most frequently used in social science research and can capture various aspects of health, it might have some shortcomings (Au & Johnston, 2014). For example, self-assessed health status can be broad and subjective as individuals can have their own interpretation and it is quite brief to reflect different aspects of health.
Estimation Sample
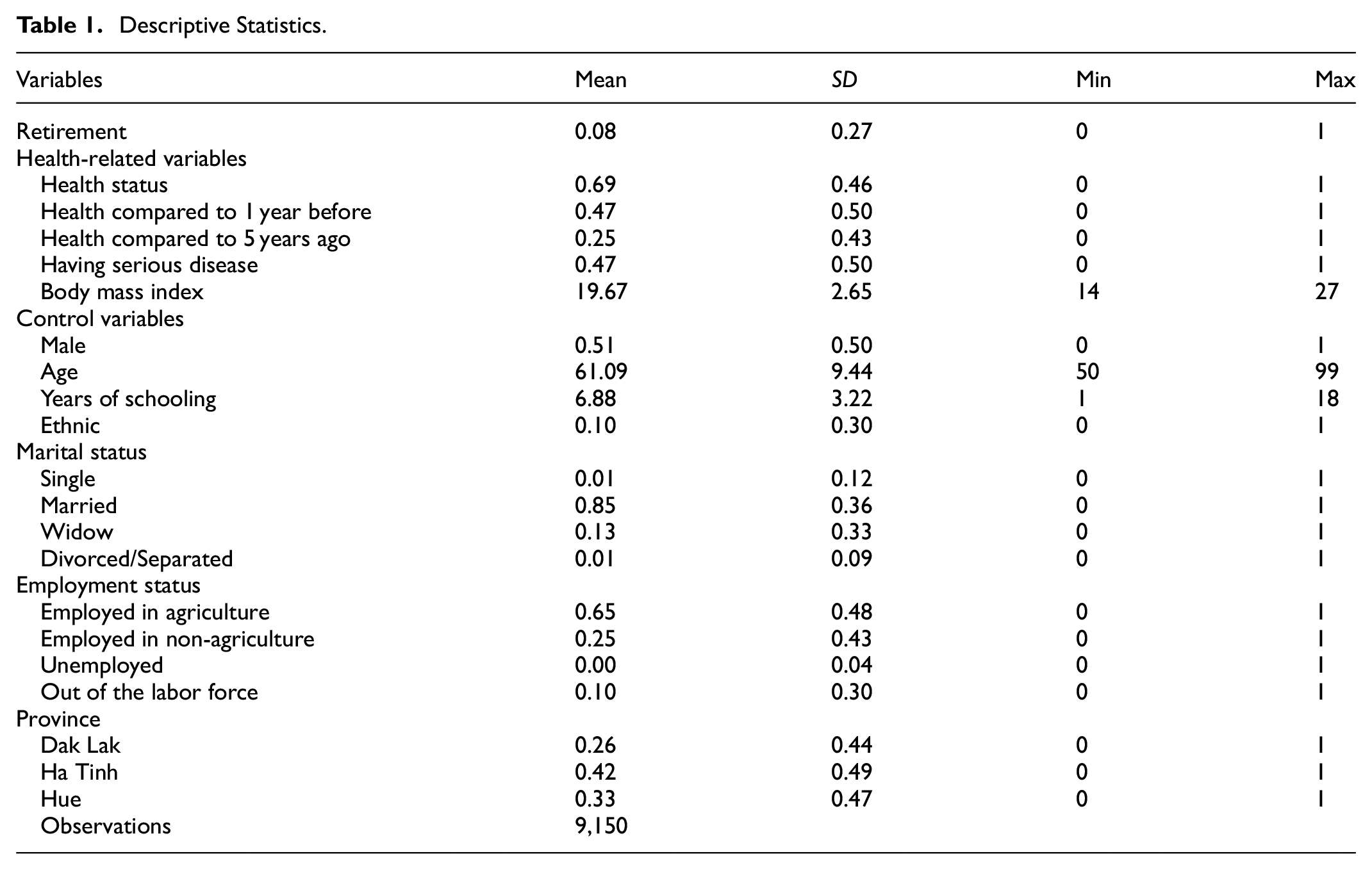
As this study focuses on retirement, we exclude individuals who are aged below 50 years old. To isolate the effect between retirement and health, we add control variables including years of schooling, age, a dummy of male and ethnicity, a series of dummies of marital status, employment status, province of residence, and waves. After we eliminate the missing values from all variables, the final sample consists of 9,150 observations in Vietnam from seven waves between 2007 and 2017. Table 1 shows the descriptive statistics of the sample.
Descriptive Statistics.
Empirical Approach
The basic model is based on the equation as follows:

where
However, it is possible that individuals’ characteristics may impact or bias both the predictor (retirement) and outcome variables (health). In a broader context, this is the case that there is a correlation between error terms and predictor variables. If so, the coefficient is biased. Thus, to manage the unobserved individual characteristics in the context of a longitudinal dataset, we used the fixed effects technique to obtain
However, there are some limitations to the fixed effects model. First, there could still be time-varying omitted variables that affect both independent and dependent variables, which do not provide estimates of causal effects (Collischon & Eberl, 2020). Second, fixed effects models can’t be used for time-invariant characteristics such as gender or ethnicity (T. D. Hill et al., 2020), which are often variables of interest to social scientists. Therefore, for future studies, more advanced approaches should be used to examine the relationship between retirement and health.
Results
The Relationship Between Retirement and Health
Ordinary Least Squares
First, we estimate the relationship between retirement and health by using the OLS approach as the benchmark. Table 2 shows that retirement is positively associated with better health status with a coefficient of 0.05 at a significance level of 1%. Similarly, the coefficient between retirement and health status compared to last year is positive and statistically significant at a p-value <.05, highlighting that retirement correlates with improved health status after one year. Lastly, being retired is associated with a higher level of BMI of 0.85 at a p-value <.01. This finding indicates that retirement correlates with a higher probability of gaining weight. In contrast, it is shown that retirement is not associated with health status compared to 5 years and having serious diseases, even with a 10% significance level. Overall, the findings suggest that retirement correlates with improved current health outcomes, health status compared to last year and higher levels of BMI. However, as there are limitations of the OLS method, such as unobserved characteristics of respondents as mentioned above, we move to the fixed and random effects approach in the next section.
Retirement and Health—OLS Approach.

Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
Fixed Effects and Random Effects Approach
Table 3 presents the estimations of the relationship between retirement and health using both fixed effects and random effects. The fixed effects approach only highlights one statistically significant coefficient between retirement and BMI at p-value <.05. For random effects model, the coefficients for health status, health status compared to 1 year and BMI are statistically significant at p-value <.05. We also perform Hausman’s specification test for model selection at the bottom of the table. The test compares the estimators from both fixed and random effects models. The null hypothesis indicates that the estimator of the random effects model is an efficient and consistent estimator of the true parameters, which means that there is no systematic difference between the two estimators. Otherwise, if there exists a systematic difference in the estimates, we have reason to doubt the assumptions on which the efficient estimator is based. Overall, this test allows us to decide between fixed or random effects. If the p-value <.05, fixed effects model is preferred and the random effects model, otherwise.
Retirement and Health—Fixed Effects and Random Effects Approach.

Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
The findings show that, out of five models, three models with current health status, having serious diseases and BMI should be estimated by using fixed effects while random effects are preferred for the other models with health status after 1 and 5 years. Therefore, retirement is shown to have no association with current health status, and having serious diseases based on fixed effects model and health status after 5 years based on random effects model. More importantly, retirement is associated with higher levels of BMI in both models and health status compared to last year in random effects model at p-value <.05.
The threshold of BMI for Asian populations is lower than 18.5 for underweight, normal weight between 18.5 and 22.9, and higher than 23 for overweight. Given the positive association between retirement and higher levels of BMI, we need to look at the distribution of BMI in our sample in Figure 1. The mean BMI is 19.67 as shown in Table 1 and the median BMI is 19.53. The shape of a bell is shown in this histogram. It can be inferred that most of our respondents are close to the bottom threshold of normal weight. Thus, when retirement is associated with higher levels of BMI, it is likely a positive sign of respondents’ health for the majority of individuals with low BMI.

Histogram of BMI.
Robustness Checks
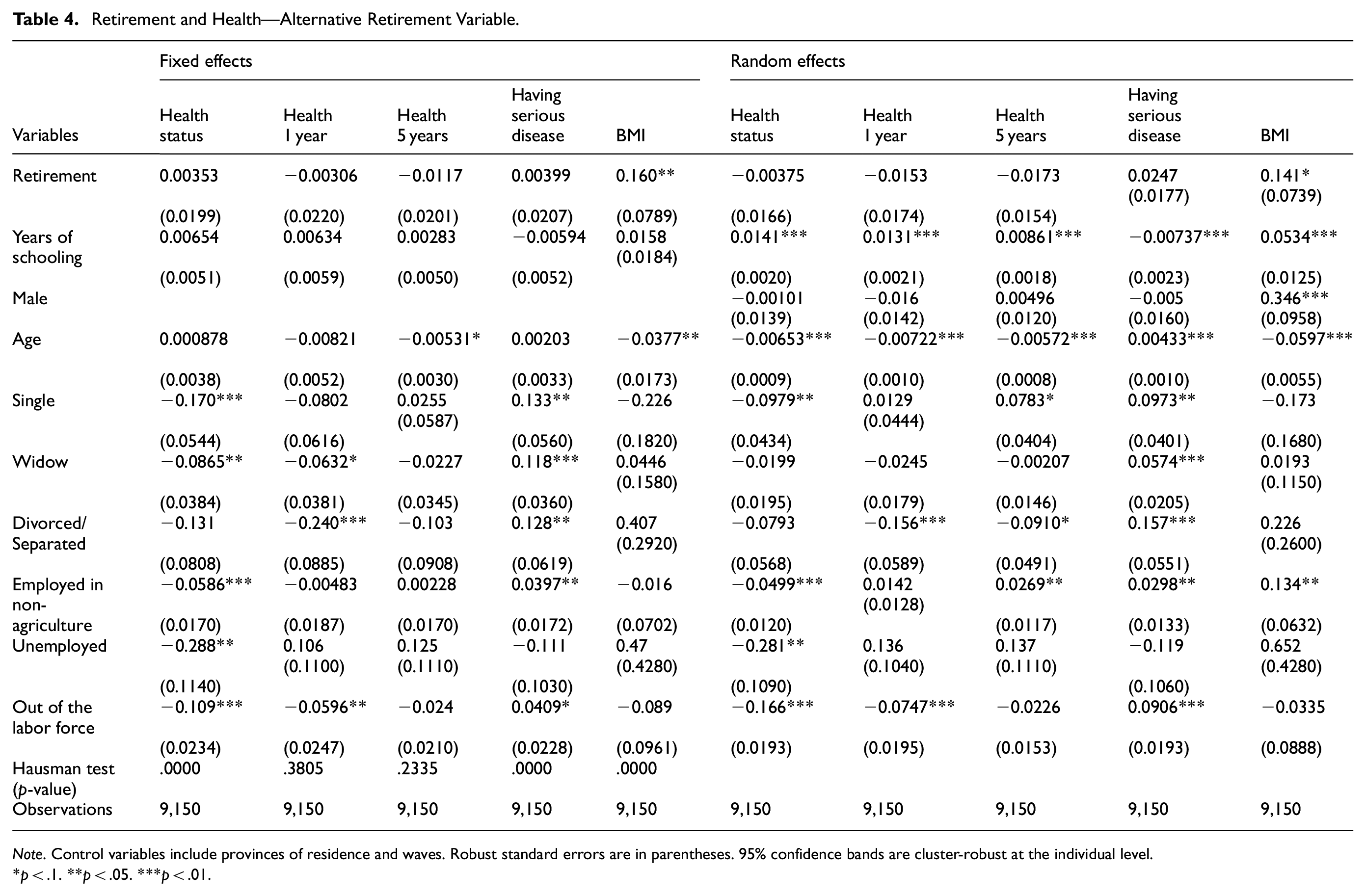
We first perform a robustness check using a broader definition of retirement. Basing the dummy solely on pension eligibility risks misclassifying informal-sector workers who stop working well before they qualify for benefits. Therefore, we construct an alternative retirement proxy based on age thresholds: 65 for males and 55 for females. We select these thresholds based on the statutory age for retirement in Vietnam, which is 60 for men and 55 for women and we suppose that male workers in the informal sector might delay retirement due to lack of pension access (Thi, 2024). If they are older than the age cut-off, the retirement variable values 1 and 0 otherwise. Table 4 reports the results using this alternative definition and shows that the relationship between retirement and BMI remains positive and statistically significant, consistent with our main findings.
Retirement and Health—Alternative Retirement Variable.
Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
As mentioned in the section “Methodology,” fixed effects models have certain limitations. Thus, to ensure the robustness of the findings, we apply the IV method to examine the relationship between retirement and health in Vietnam. This method allows us to handle the endogeneity of retirement variable. The instrumental variable used in this study is the statutory age for retirement in Vietnam, which is 60 for men and 55 for women. When people reach this age, it is likely that they will retire, which establishes the relationship between retirement and reaching the statutory retirement age. Additionally, this statutory retirement age is exogenous as it is applied widely and has no direct relationship to people’s health. These two arguments potentially satisfy the requirements of a qualified IV for the estimation. Then, we create a dummy IV. If respondents reach the retirement age (60 for men and 55 for women), the value is one and zero otherwise. The rationale for employing pension eligibility as a measure aligns with numerous prior research findings in the literature, which affirm that social security benefits play a crucial role in determining an individual’s retirement date (Atalay et al., 2019; Engels et al., 2017). Eligibility is exogenous when controlling for age since the eligibility ages are specified by law (Horner, 2014). To put it another way, other than retirement decisions, there is no reason to believe that our instrument will directly affect someone’s health (Kesavayuth et al., 2016; Rohwedder & Willis, 2010; Zhu & He, 2015). Figure 2 presents regression discontinuity plots of the mean of retirement status and BMI against age, separately by gender. In the upper panels, we observe a clear discontinuity in the probability of retirement at the statutory retirement age for both men and women, confirming the strong relevance of the age threshold as an instrument for retirement. In contrast, the lower panels show no evident jump in BMI at the same cut-off points, suggesting that statutory retirement age does not directly affect BMI. This also holds for the remaining covariates, including years of schooling, an ethnicity dummy, and a series of indicators for marital status, employment status, province of residence, and survey waves—all of which are unlikely to change during the retirement transition, as shown in Appendix 1. The table shows that point estimates are small and associated with high p-values, indicating no systematic evidence of discontinuities in these predetermined covariates at the cut-off. These diagnostics support the validity of the instrumental variable by demonstrating both its relevance and satisfaction of the exclusion restriction.

Regression discontinuity graphs of retirement and BMI versus age by gender.
The estimation includes two stages as follows:

in which

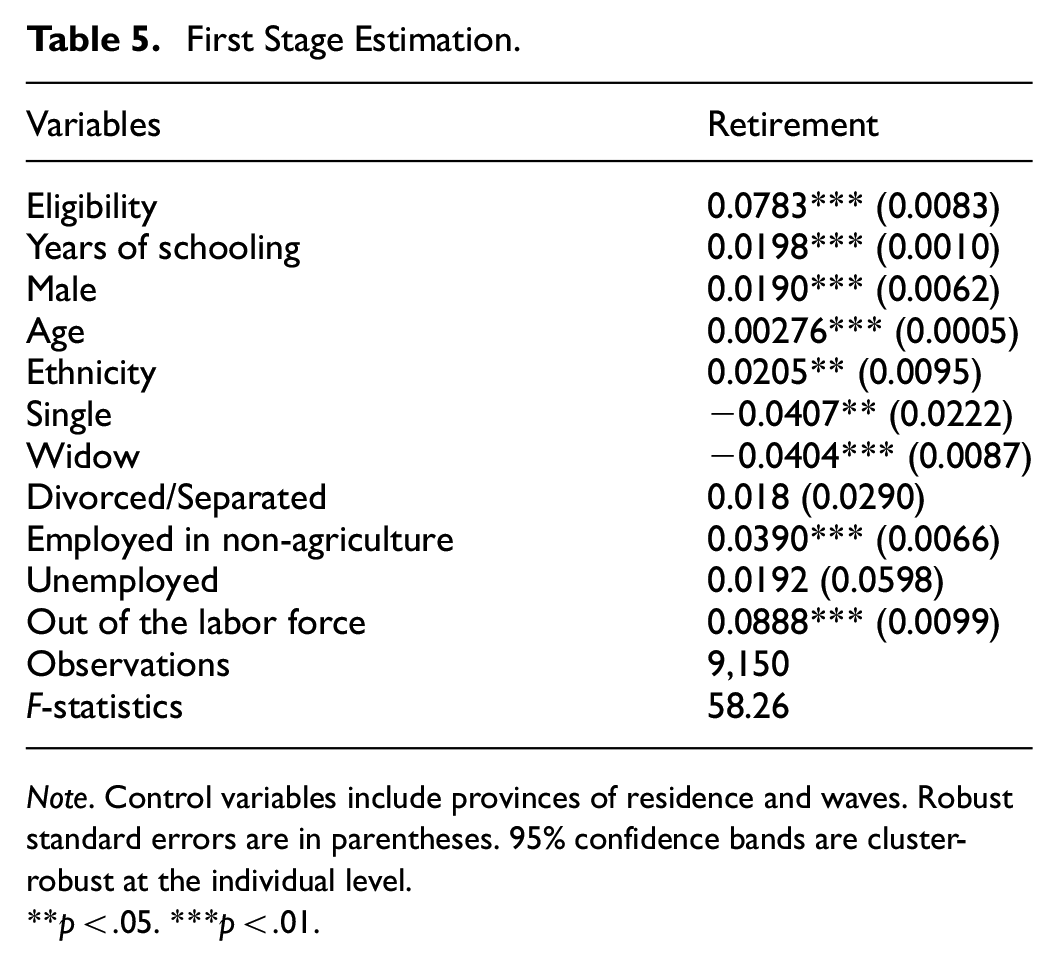
Table 5 shows a positive and statistically significant effect between retirement and being qualified for statutory retirement age. In particular, being qualified for statutory retirement age is associated with a probability of being retired by 7.8% at a significance level of 1%. Moreover, the F-statistic for the significance of the IV indicates that our instrument is a strong predictor for retirement decisions. The first-stage F-statistic is above the rule-of-thumb value of 10 suggested by Staiger and Stock (1997), allowing us to reject the null hypothesis of weak IVs.
First Stage Estimation.
Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .05. ***p < .01.
The second-stage results are presented in Table 6. The table indicates that retirement has a positive impact on BMI at p-value <.01, which is consistent with our previous findings, lending further support to our estimations. The results also suggest that other health measurements do not change at retirement.
Retirement and Health—IV Approach.

Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
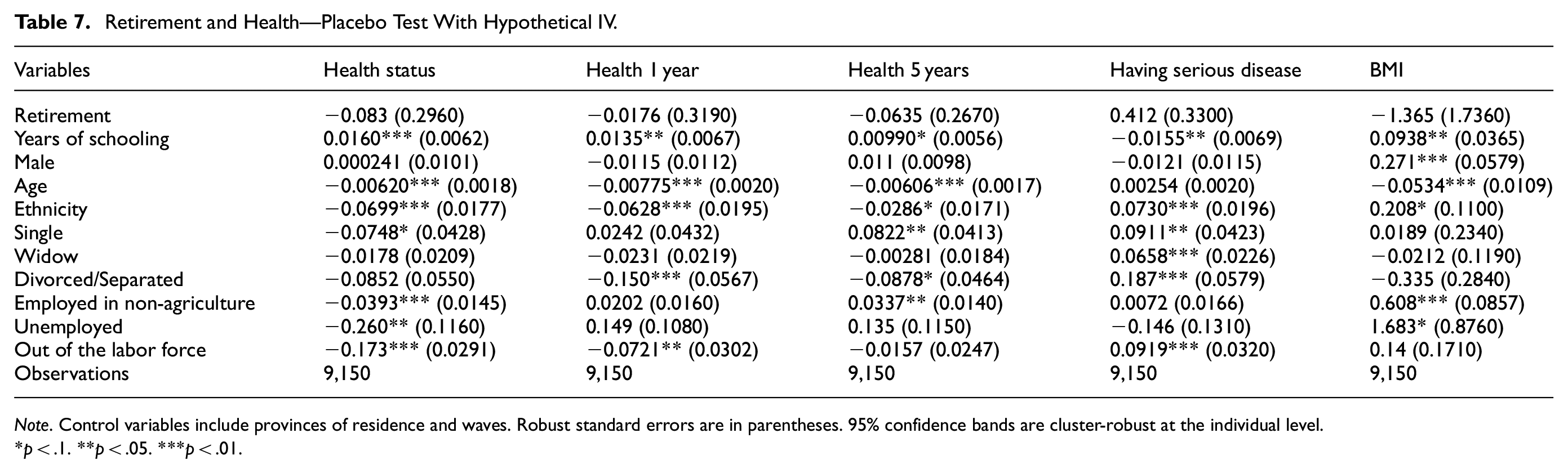
Additionally, to ensure the validity of the IV and our findings, we performed a placebo test using a fake statutory age for retirement of 65 for men and 60 for women. Table 7 shows that hypothetical IV produces a null result, meaning that there is no relationship between retirement and health. These findings reassure the validity of the true statutory retirement age as the valid IV for estimating the causal effects of retirement on health.
Retirement and Health—Placebo Test With Hypothetical IV.
Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
Lastly, we conduct a robustness check by incorporating income as a control variable in the IV model. In particular, we include the logarithm of monthly household income per capita as an additional control variable. This variable is converted to purchasing power parity dollars in 2005 by the data provider. Additionally, we winsorize it at 1st and 99th percentiles to eliminate outliers before applying the logarithmic transformation. As shown in Table 8, our main findings remain robust, highlighting the validity of our estimates. Moreover, income has a positive effect on health, highlighting its role as a key determinant.
Retirement and Health—IV Approach With Control of Income.

Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
Analysis by Gender and Ethnicity
From the main analysis, the fixed effects model does not allow adding time-invariant variables such as gender or ethnicity. Thus, we will disaggregate the sample by gender and ethnicity to examine the heterogeneity of the relationship between retirement and health. Table 9 shows the estimations by gender using the fixed effects approach. It can be inferred from the table that the statistically significant association between retirement and BMI was only realized among men but not women. Overall, the association between retirement and health is mainly driven by men.
Analysis by Gender.

Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
Table 10 presents the results between Kinh people (the majority) and ethnic minorities. It can be inferred from the table that the association between retirement and BMI is observed only among Kinh people but not among ethnic minorities. The coefficient is statistically significant at p-value <.01. However, it does not necessarily mean that the health benefits of retirement do not exist among them as the number of observations for ethnic minorities in the sample is quite small. Thus, these results might need to be elaborated further in future studies.
Analysis by Ethnicity.
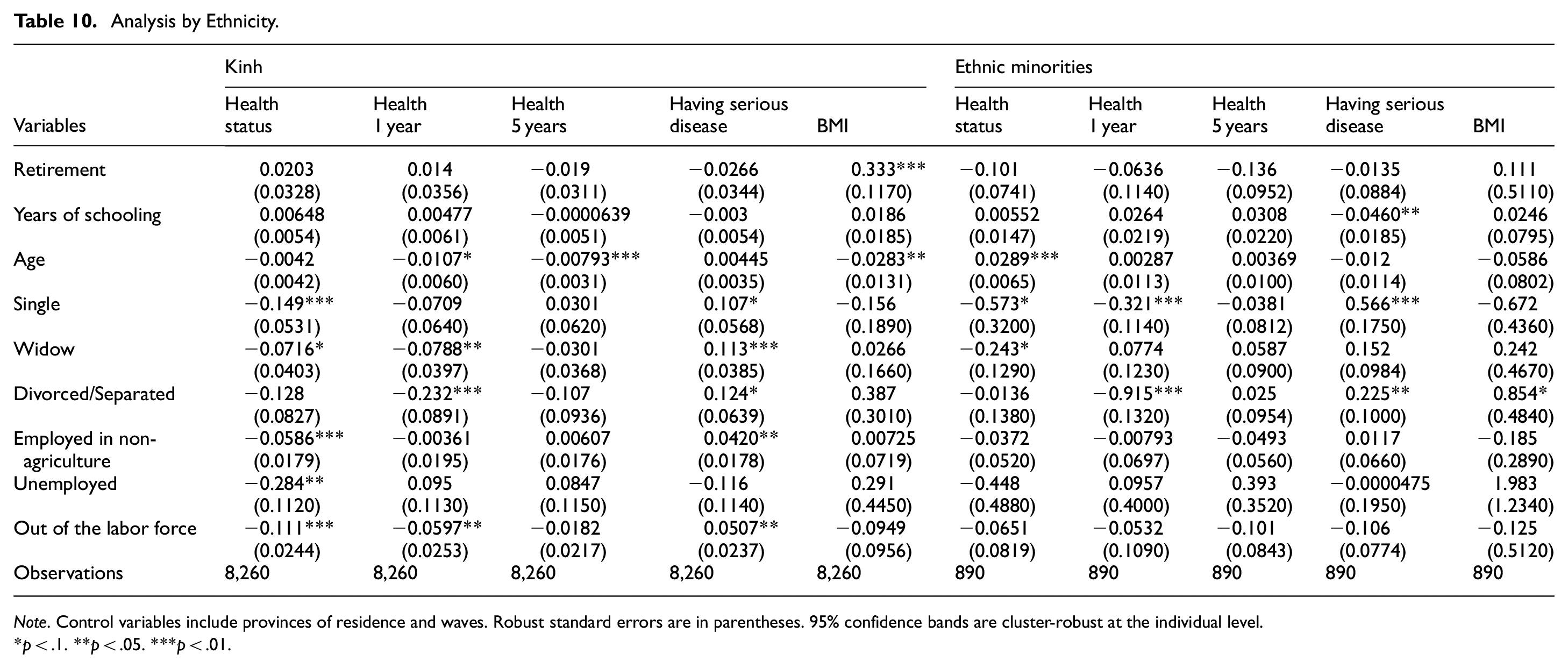
Note. Control variables include provinces of residence and waves. Robust standard errors are in parentheses. 95% confidence bands are cluster-robust at the individual level.
p < .1. **p < .05. ***p < .01.
Discussion
Our findings consistently align with previous studies on the impact of retirement among older individuals (Comi et al., 2022; Gorry et al., 2018; Latif, 2011; Tran & Zikos, 2019; Zhu & He, 2015). This study contributes to the growing body of literature on emerging economies, where rapid population aging and limited resources for elderly care pose significant challenges to the social security system. By providing empirical evidence on the relationship between retirement and health, our insights are crucial for shaping targeted policies that promote both physical and mental health among older adults. This is particularly relevant in contexts where the demand for labor increases alongside an aging population, which raises the critical need for strategies that balance workforce participation with the health and welfare of retirees.
The first important finding of this research is the positive impact of retirement on health among rural Vietnamese. In particular, retirement is shown to have a positive effect on the level of BMI. This finding is very important as Vietnam has just applied the new adjustment on retirement age according to Article 169 of the Labor Code in 2019 (Ministry of Labor War Invalids and Social Affairs, 2023) stipulating retirement ages in Vietnam as follows: Under normal working conditions, employees’ retirement ages will progressively rise to 60 for women in 2035 and 62 for men by 2028. Beginning in 2021, employees’ retirement ages under normal working conditions will be 60 years, 3 months for men and 55 years, 4 months for women. These ages will advance annually by 3 months for men and 4 months for women. According to the aforementioned legislation, a person can retire in Vietnam in 2022 at the age of 60 years, 3 months for men and 55 years, 4 months for women. After each year, it will rise by 4 months for females and 3 months for males. When the government increases the retirement age, the benefit of retirement on health will be forgone by delaying retirement, reducing the welfare of people about to enter retirement. The decline in health quality is particularly concerning in developing countries like Vietnam, where healthcare systems are limited as there has been no clear evidence on whether the benefits of an additional year of work outweigh the potential health costs for older individuals after retirement. Thus, enhancing people’s health before and after transitioning to retirement requires inclusive supportive programs to compensate for the forgone benefit. For example, several other studies have revealed the mechanisms of how retirement affects health, such as more time spent on physical activities or social interactions. Thus, intervention programs, such as local retirement clubs or social programs for retirees, are essential to enhance well-being and healthier lifestyles for newly entered retirees.
The second finding of this study is the heterogeneous effect of retirement on health by gender and by ethnicity. As the effect is found among males and Kinh people only, but not for females and ethnic minorities. This suggests that the underlying transition process to retirement differs by demographic group. First, the effect that only exists among males can be potentially explained by the major change in male retirees’ lifestyles. Although the roles and responsibilities of men and women in rural Vietnam can vary based on the specific region, cultural practices, and individual household arrangements, males are more likely to participate in farming activities involving more physically demanding activities such as plowing, planting, and harvesting crops, compared to their female counterparts (Ylipaa et al., 2019). Thus, after retirement, they might spend less time in those strength-required activities, leading to gaining more weight, reflected in an increased BMI.
To promote better health among retirees in the future, several policy implications can be considered. The government needs to advance policies and programs that address the greater rates of underemployment and unemployment, job insecurity, income inequality, and disadvantages encountered in rural and remote areas, as well as the higher rates of health issues and restricted access to healthcare services (Kim et al., 2020; Vu & Nguyen, 2021). For example, community health centers could be established to provide comprehensive primary care services to retirees. This facility could offer regular check-ups, preventative screenings, and chronic disease management to ensure that retirees receive the necessary healthcare support they need. Additionally, telehealth services could be implemented to connect retirees with doctors and specialists and allow for remote consultations, reducing the need for travel and increasing access to specialized care. Moreover, as mentioned above, supportive programs should be specialized for various demographic groups. Lastly, rural areas should be additionally supported by locally tailored methods that address issues related to early intervention or health service accessibility.
Concluding Remarks
Retirement is a turning point in life that brings about changes in daily routines, finances, and social-psychological status. This study uses the Thailand Vietnam Socio Economic Panel - dataset to investigate the association between retirement and health in rural Vietnam. Through the use of a variety of methodologies, such as random effects, fixed effects, and instrumental variable models, the results show that retirement status among Vietnamese in rural areas has a beneficial impact on the health measure of BMI. Nonetheless, the impact and its magnitude vary throughout Vietnamese sociodemographic groups.
Like any other study, this paper has certain limitations. First, the findings from this study might not be generalizable to other populations as the sample was collected from three rural provinces in Vietnam. Second, categorizing health status and retirement from the TVSEP survey as binary variables may lack the validity and reliability required in economic research. For instance, health status is a complex concept that cannot be fully captured by a binary measure, which may cause inaccurate representations. Similarly, retirement decisions may involve gradual transitions or partial employment, which binary categorization fails to reflect. This oversimplification of these measurements may introduce measurement errors, reduce the explanatory power of the analysis, and limit the ability to draw meaningful conclusions. Therefore, future studies should adopt more precise measures of health and retirement status to better capture the true effects of retirement transitions on health. Another limitation is the small number of retirees in the sample, which reduces statistical power and may limit the ability to detect significant effects. Last, given the unavailability of the data, the mechanism of how retirement influences health remained unexplored. Thus, for future studies, several mechanisms such as changes in daily diet, and physical activity frequency should be examined.
Footnotes
Appendix
Continuity-Based Analysis for Covariates.

| Variables | Male | Female | ||
|---|---|---|---|---|
| Regression discontinuity estimator | Robust inference (p-value) | Regression discontinuity estimator | Robust inference (p-value) | |
| Years of schooling | .3480 | .5820 | −.1370 | .4600 |
| Ethnic | .0109 | .7930 | .0166 | .3890 |
| Single | .0023 | .5100 | .0189 | .3730 |
| Widow | .0293 | .0040 | .0102 | .8910 |
| Divorced/Separated | .0100 | .2690 | .0127 | .1680 |
| Employed in non-agriculture | .0362 | .5130 | .0346 | .5610 |
| Unemployed | .0099 | .1180 | −.0006 | .1560 |
| Out of the labor force | −.0143 | .3980 | −.0628 | .0410 |
| Dak Lak | −.0316 | .6710 | −.0247 | .3190 |
| Ha Tinh | .0425 | .7380 | .0403 | .4220 |
| Wave 1 | −.0043 | .8650 | −.0186 | .4570 |
| Wave 2 | −.0211 | .8040 | −.0266 | .1450 |
| Wave 3 | .0167 | .8820 | .0106 | .2410 |
| Wave 4 | .0112 | .7080 | −.0194 | .3280 |
| Wave 5 | .0391 | .5840 | .0539 | .0680 |
| Wave 6 | −.0483 | .6410 | −.0010 | .6520 |
Note. 95% confidence bands are cluster-robust at the individual level.
Acknowledgements
Ethical Considerations
This study requires no ethics approval as the analysis used only deidentified existing unit record data from the Thailand Vietnam Socio-Economic Panel (TVSEP).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Vietnam National Foundation for Science and Technology Development (NAFOSTED) under grant number 502.01-2023.14.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data cannot be shared publicly because the current study is subject to the signed confidentiality deed. Data are available from the Thailand Vietnam Socio-Economic Panel (TVSEP) for researchers who meet the criteria for access to confidential data. The data underlying the results presented in the study is available from the Thailand Vietnam Socio Economic Panel, email:
{kind=link}