
Abstract
Understanding the health benefits of education is vital in setting policy priorities, especially in lower-income countries. Using the instrumental variable with panel data estimation approach, this study utilizes data from the Thailand Vietnam Socio Economic Panel to provide comparative evidence of the health benefits of education in two countries. The findings indicate that highly educated people are likely to report better current health status, reduced probability of having serious diseases in both countries, increased body mass index (BMI) in Vietnam and decreased BMI in Thailand. Additionally, the benefits of education on health are significant among Vietnamese men, Thai women, and Vietnamese ethnic minorities. The results also suggest that the positive effect of education on health can be explained by higher household income. Thus, promoting education among vulnerable groups, including women and ethnic minorities, should be particularly prioritized to mitigate the gaps in health inequities.
Introduction
Education and health are two essential topics, not only to policy makers and health practitioners but also to researchers, especially in developing countries. An in-depth understanding of this relationship can contribute to reducing health disparities and improving people’s health. This research theme is specifically important in the South-East Asia region, where inequalities in health outcomes and health service access are more severe (World Health Organization [WHO], 2009). During the COVID-19 pandemic, this topic has drawn much attention. Education is one of the determinants influencing the willingness to vaccinate against COVID-19, which impacts people’s health status and the success of vaccination programs. Recent research has found that people in low-educated groups are hesitant and reluctant to vaccinate in Bangladesh (Abedin et al., 2021). Similar results are also found in Austria (Humer et al., 2021) and Canada (Racey et al., 2021). These outcomes imply that more efforts are needed from the governments to alter the willingness to vaccinate among those with lower educational levels.
Previous studies have shown controversial outcomes about the impact of education on health. The positive effect of education on health was found in some studies (James, 2015; Ma et al., 2018; Raghupathi & Raghupathi, 2020; Savelyev et al., 2022; Tran & Tran, 2019). In contrast, other studies found that education’s health benefits do not exist (Braakmann, 2011; Clark & Royer, 2013; Xie & Mo, 2014). A more detailed discussion about these studies is presented in the next section. Given these conflicting findings, further research is needed to determine the relationship between education and health in a more specific context.
Therefore, to contribute to the ongoing debate and provide more knowledge about this topic, this study investigates the relationship between education and health in Vietnam and Thailand. These two countries have a combination of similarities and differences that create the potential for comparative analysis. Although both nations are characterized by some similar key demographic factors, their perspectives on education, healthcare system, economic development progress, and political system differ significantly. Nation Master (2020) has shown that the total number of primary-school-age children who are not enrolled in either primary or secondary schools in Thailand is twice as high as in Vietnam. Additionally, while government spending on education in Vietnam is lower (2.47 billion USD, compared to Thailand’s 12.54 billion USD), it accounts for a higher percentage of GDP (6.85%) than Thailand’s 5.79%. Furthermore, both the adult literacy rate and literacy of the total population in Thailand are slightly higher than those in Vietnam. These differences can be considered when conducting this cross-national comparative research, which facilitates a better understanding of the connection between the level of development in a country and the effect of education on the health of that country’s people.
Only a few studies closely related to this topic have been carried out in Vietnam and Thailand. For example, Dang (2018) discovered the relationship between education and healthcare utilization in Vietnam using a regression discontinuity design. Those findings showed that highly educated people have a higher level of inpatient utilization in the public health sector and a lower level of outpatient utilization in private and public health sectors. More importantly, Dang also found that income and the likelihood of having health insurance are potential mechanisms of the causal impact of education on healthcare utilization. However, only a few papers have explicitly examined whether these are truly mechanisms of how education affects health. Therefore, such an extension is conducted in the present study.
Loichinger and Pothisiri (2018) used data from the Survey of Older Persons in Thailand to reveal the impact of education on health indicators. They found a positive education gradient for difficulties with activities of daily living and poor self-rated health but not for functional limitations. However, the authors only focus on the health prospects of education among older people, which can be extended to a more general population. The lack of empirical research on how education affects health in developing countries, where levels of both schooling and health have been rising rapidly, requires further research to enrich extant sources of literature in this field. Moreover, this relationship can be important not only for policymaking but also for the healthcare system. With this knowledge, policymakers can undertake plausible plans to achieve specific healthcare objectives, such as health equality in society.
The present study attempts to fill these gaps in the literature on existing controversial evidence by providing an understanding of how education affects health in Thailand and Vietnam. It is also one of the first few papers to examine the health benefits of education in Vietnam and one of the first few comparative studies on this topic. Moreover, this study employs the distance to school location as an instrumental variable to address the potential endogeneity problem of the education of individuals, which appears to be overlooked in the existing literature. Lastly, supposing that a relationship between education and health exists, this study also examines the possible mechanisms through which education affects health, enriching the literature on this topic and suggesting potential policy implications to amplify positive effects.
The study is organized as follows. The literature review is provided in Section 2. Section 3 describes the data and how the variables are constructed and presents the methodology and estimation strategy. Results are discussed in different aspects in Section 4. Section 5 concludes the study.
Literature Review
This paper is based on a conceptual framework of health production initiated by Grossman (1972) that considered health stock an important contribution to human capital development and emphasized the relationship between education and health. Several pathways can explain the impact of education on health. At the individual level, Ross and Wu (1995) proposed that education improves health directly and indirectly through work and economic conditions, social-psychological resources, and a healthy lifestyle. For example, education can give access to better health inputs and allow individuals to use them more efficiently (Smith-Greenaway, 2013). Additionally, education contributes to human capital by developing a range of both cognitive and non-cognitive skills (the latter are also known as personality traits), greater awareness of health, a greater sense of control, and higher levels of social support. Last but not least, more-educated individuals have fewer negative health behaviors (e.g., Li & Powdthavee, 2015).
At the community level, individuals with more education also benefit from health-related characteristics of the environment, such as food access, spaces and facilities for physical activity, access to health care, community economic resources, lower levels of criminal violence, and less environmental exposure to toxins (Zimmerman & Woolf, 2014). At the society level, health equity is mainly determined by social context, which is shaped by social policies. For example, social services, healthcare systems, and insurance policies can amplify or buffer society’s health consequences. However, education, institutions, and other resources play an important role in the decision-making process regarding social policies. As such, this study contributes to the expanding literature and provides empirical evidence on the relationship between education and health. Figure 1 summarizes the conceptual framework of this relationship.

Conceptual framework.
The first line of the previous literature shows evidence supporting the positive effect of education on health. Using changes in compulsory schooling laws in Germany, Kemptner et al. (2011) found a strong positive effect of education on men’s long-term illness and weaker evidence of weight problems among both genders. Similarly, using the changes in compulsory education law in the U.S. as an instrument for education, Lleras-Muney (2005) suggested that education has a causal impact on mortality. James (2015) indicated an effect of education on body mass index (BMI), waist circumference, and weight using U.K. post-compulsory education reform. Ma et al. (2018) found that education has an impact on hypertension and diabetes in Ireland by exploiting policy changes. Tran and Tran (2019) revealed the positive effect of education on self-reported health, physical health, mental health, and long-term health conditions among Australian women using the spouse’s education as an instrument for years of schooling. Raghupathi and Raghupathi (2020) indicated that people with higher educational attainment have better health and lifespans compared to their less-educated counterparts in OECD countries for the period 1995 to 2015. Tran et al. (2021) found that higher education levels lead to a higher level of eudaimonic well-being, hedonic well-being, positive affect, and reduced psychological distress among Australian women. More recently, Savelyev et al. (2022) found a beneficial causal effect of education on health and longevity using twin data in the U.S.
Nevertheless, many other studies present mixed results. Using the regression discontinuity method, Zhong (2016) found that better education reduces the probability of having poor self-assessed health or disabilities and increases the probability of having chronic diseases in China. Gathmann et al. (2015) found that higher education leads to a small reduction in mortality among men, but not for women. Fonseca et al. (2019) found that education leads to better health, including a reduction in reporting poor health, self-reported difficulties with activities of daily living, chronic illness, heart disease, and arthritis; they found no conclusive evidence of education’s influence on the risk of cancer, stroke, and psychiatric illness.
Other studies fail to reveal any correlation between education and health. Using a French longitudinal dataset, Albouy and Lequien (2009) failed to find the causal effect of education on health. Likewise, Braakmann (2011) and Clark and Royer (2013) found little evidence that education improves health in Britain. In China, Xie and Mo (2014) found no causal impact of education on either perceived health or anthropometric health.
Only a few studies examine this topic in the context of emerging countries. For example, Jensen and Lleras-Muney (2012) found that education leads to a lower probability of smoking and daily or regular drinking in the Dominican Republic. In Zimbabwe, Agüero and Bharadwaj (2014) discovered that highly educated women are more committed to HIV-preventing behavior by having fewer sexual partners and obtaining more knowledge of HIV transmission. In conclusion, previous studies analyzing the relationship between education and health have generated various and sometimes conflicting results. Our aim is to shed more light on the causal effect of education on health outcomes in a lower-income context by studying the population in Vietnam and Thailand—both emerging countries.
Methodology
Data
This study uses a panel data set “Thailand Vietnam Socio Economic Panel.” Funded by the German Research Foundation (DFG), the survey covers around 4,200 representative households in rural provinces in Thailand and Vietnam who were interviewed in 2007, 2008, 2010, 2011, 2013, 2016, and 2017. The overall purpose of the project is to complement existing panels in industrialized countries by establishing a unique, multipurpose, and long-term socio-economic panel in the emerging economies of Thailand and Vietnam. More details about the dataset can be found at the project webpage https://www.tvsep.de/overview-tvsep.html. To achieve the objective of the project, the sample was created to be representative of the rural population in Northeast Thailand and Central Vietnam, so many conditions are imposed in the sampling strategy (Hardeweg et al., 2013). The data set consists of answers to questions about demographics, health, education, agriculture, and so on, providing us with sufficient data to conduct this study. Additionally, the data are collected in Thailand and Vietnam with a similar design, allowing us to conduct a comparative study for this topic.
Health measures
This study uses three health measures to examine the impact of education on health. From the data set, they are current health status, having serious diseases, and BMI. For the current health status measure, respondents are asked how healthy they are on three scales ranging from (1) “Sick” to (2) “Can manage” to (3) “Healthy.” For ease of interpretation, we convert this variable into a dummy variable with a value of 1 if the respondents answer they can manage their health or are healthy and 0 for sick. The validity of these self-assessed health measures is described by the level of predictive power concerning the actual health condition, which is confirmed over time in previous literature (Schnittker & Bacak, 2014). Nevertheless, self-reported measures can be biased, depending on socio-economic factors (Ziebarth, 2010). Therefore, this study also employs objective health measures to address any potential reporting bias. Apart from the subjective health measures, respondents are asked whether or not they have serious diseases such as pneumonia, heart diseases, and poliomyelitis. If they have any of those conditions, the answer is “Yes” and “No” otherwise. The questionnaire also provides information on the weight and height of interviewees. Thus, we also obtain BMI as an alternate measure of health, which is one of the major predictors of individuals’ health (Gugushvili & Jarosz, 2019; Tam & Yeung, 2018), especially to diagnose obesity (Wickramasinghe et al., 2005). The BMI is winsorized at level 1st and 99th percentiles to remove the outliers.
Years of schooling
The Vietnamese education system includes 5 years of primary school, 4 years of secondary school, 3 years of high school, and 4 years of university (an exception is 6 years for medical-related universities). Students can optionally take vocational training for 2 years or a college diploma for 3 years. Finally, the master’s degree and Ph.D. programs require, respectively, 2 years and 3 years of study. Regarding Thailand’s education system, primary school (Prathom) consists of 6 years, and then the next 3 years are for lower secondary school (Matthayom). After, students have two options: spending either (1) 3 years in upper secondary school (Matthayom 4–6) or (2) 3 years for a vocational certificate (PWC 1–3). Students who complete upper secondary school can enter universities, while those with a vocational certificate can obtain a diploma of vocational certificate (PWS) after 2 years of additional study.
The present study employs the years-of-schooling variable as the key independent variable to proxy for education. The actual years of schooling are reported in the year 2013, 2016, and 2017 but not in the four previous waves. As the data only provide the actual years of schooling in some years, to make the variable consistent across all waves, this paper derives this variable by accumulating the number of years based on the individual’s highest reported level of educational attainment. For example, the duration of schooling for those who graduated from high school is set as 12 years. This approach has been used in previous literature using Vietnamese or Thai data sets (Doan et al., 2018; Liu, 2004; Warunsiri & McNown, 2010). A summary can be found in Table 1.
Education System in Vietnam and Thailand.

Instrumental variable: Distance to school
The respondents are asked the following question “Where did you obtain your highest educational degree?” The answers given are (1) in the same village/commune; (2) in the same district (rural areas); (3) in the same district (urban areas); (4) in the same province (rural areas); (5) in the same province (urban areas); (6) in another province (rural areas); (7) in another province (urban areas); and in Bangkok, Hanoi, Ho Chi Minh City, Laos, Cambodia, other Asian countries and other countries. We then generate the dummy variable of distance to school by denoting value 0 if the interviewees reply from (1) to (4) and 1 for other answers. This variable represents whether individuals obtain education from relatively distant from their residence. In Vietnam, individuals deciding to pursue a school located in the same province in the urban area or different provinces, cities, or countries account for 26.12%, whereas this figure is 20.54% in Thailand. Further discussions of the instruments are presented in the next section.
Estimation sample
The estimation sample includes data from seven waves in the years 2007, 2008, 2010, 2011, 2013, 2016, and 2017. We include additional controls for gender, age, age squared, household size, a dummy of ethnicity, a set of dummies of marital status, employment status, wave dummies, and regional dummies (Hue, Ha Tinh and Dak Lak in Vietnam and Buriram, Nakhon Phanom, and Ubon Ratchathani in Thailand). We also perform a variance inflation factor (VIF) analysis and find no multicollinearity among the independent variables in the model. After excluding observations with missing responses to the questions required for the analysis, the final sample corresponds to an unbalanced panel of 28,725 observations (13,703 for women and 15,022 for men) in Vietnam and 35,118 observations (17,552 for women and 17,566 for men) in Thailand.
Table 2 provides descriptive statistics for the whole sample of the respondents in both countries. Our estimation sample shows that Vietnamese people obtain an average of 8.6 years of schooling and Thai people obtain 7.89 years. Regarding three health-related variables, Vietnamese people are likely to have better health status while they are also more likely to admit to having serious diseases than Thai people. Additionally, the mean BMI ratio among Thai respondents is 22.59, higher than the mean BMI of 20.2 of the people in the Vietnamese sample.
Descriptive Statistics.

Estimation model
To examine the impacts of education on health outcomes, we consider the following health production function:

in which
The first methodological issue relates to the individual fixed effects. Unobserved individual-specific characteristics such as ability or family background are likely to influence the schooling decision. Using the advantages of longitudinal data, we can consider two approaches: a fixed effects or a random effects model. We would like to employ the latter approach for several arguments. First, the random effects estimator is widely favorable in many aspects of applied statistics (Cameron & Trivedi, 2009). Additionally, as the educational variable does not vary substantially over most adult lifetimes, the utilization of models relying only on within-individual variation becomes problematic (Nikolaev, 2018). Lastly, if the fixed effects model is applied, many time-invariant characteristics such as gender and ethnicity are omitted from the model. To deal with the case of remaining unobserved individual fixed effects, we follow Mundlak’s (1978) approach, in which the means of time-variant predictors are added to proxy the fixed effects (Chamberlain, 1982).
Another problem that arises during the process of estimating the parameter α correctly is that several issues regarding the years-of-schooling variable could cause an endogeneity problem because individuals make their schooling decisions rather than having it assigned randomly. The first problem is that health can have a reverse effect on education (Eide & Showalter, 2011; Ma et al., 2018; Taras & Potts-Datema, 2005). For instance, students with illnesses can have difficulties at school, affecting both academic performance and educational attainment, preventing scholastic development (e.g., Schulte-Körne, 2016). Another issue relates to omitted variables that might have an impact on both education and health simultaneously (Fuchs, 1982; Grossman, 2008). One common approach to address the endogeneity problem is using the instrumental variables (IV) method. The method requires that instruments must meet two requirements: (1) they must satisfy the orthogonality condition to
This study employs the distance between the individual and educational institution as an instrument for years of schooling, which has been used the most often in the context of educational research (Pokropek, 2016). According to the economic theory of human capital, education can be treated as an investment. Consequently, people consider their costs and potential benefits when making schooling decisions. Costs include tuition fees, effort, and time spent, while benefits are the future earnings and externalities (Roland, 2016). Based on this theory, the motivation for this instrument is, holding other things constant, the lower the cost of enrollment, the higher the educational attainment (Murnane & Willett, 2010). This approach has been applied empirically in previous literature. For instance, geographic variation in college proximity (Card, 1995), distance from the respondent’s high school to the nearest junior college (Rouse, 1995), geographic proximity to Catholic schools (Neal, 1997), or distance to college (Dee, 2004) have been used as an instrument variable. Another available instrument in our dataset is parental’s education. However, we decide not to use this variable to avoid the potential problem of measurement errors caused by rural-to-urban migration (e.g., Pham et al., 2018) or extended families.
Unfortunately, our data set does not provide information on the number of schools in the areas or the distance to the nearest school. Instead, we have the respondents’ answers to “Where did you obtain your highest educational degree?” For the validity of our instrument, two requirements must be met: distance to school must meaningfully correlate with years of schooling and should otherwise have no effects on health outcomes. First, regarding the potential relationship between distance to school and years of schooling, this condition is likely to be met. Most of the recognized schools are located in big towns or big cities. They are likely to have better facilities, closer access to the labor market, and higher quality. Thus, students might decide to study far away from their homes if they value the reputation and the quality of the school, providing them with a higher level of educational attainment. Second, it must be assumed that there is no causal relationship between distance to school and health outcomes and that no unobservable factors are related to both variables. In other words, the choice of which school to attend must be strictly exogenous. However, this assumption is difficult to hold because unobservable factors may be driving both individual choices of where to get an education (Kling, 2001) and individual health. To mitigate the problem, we follow the strategy suggested by Dee (2004) by including many control predictors such as gender, age, household size, ethnicity, employment status, marital status, and series of time and province dummies. Moreover, we also add the mean of time-variant predictors to reduce the impacts of individual fixed effects. To sum, distance to school might not be a perfect instrument given its limitations, but it is useful in an attempt to overcome the endogeneity problem—a common methodological stumbling block in education research.
Overall, to overcome the abovementioned issues, this study utilizes the random effect instrumental variable (RE-IV) approach to tackle the potential bias. The intuition of the RE–IV method is strong as the RE element with Mundlak’s transformation helps control for unobserved heterogeneity, and the IV method helps control for time-varying unobservables and reverse causality. Accordingly, in the first stage, years of schooling are regressed on the distance-to-school variable in the following equation:

in which

in which Êit is the predicted years of schooling, derived from Equation (2). Therefore, the key coefficient α is the effect of education on health outcomes. We will use the RE-IV regression in Stata 14. Huber/White/sandwich estimators are obtained to estimate the variance–covariance matrix corresponding to the parameter estimates.
Results and Discussions
Instrument variable estimation
With the two-stage estimation procedure outlined above, Table 3 presents the result from the first-stage regression. The first stage illustrates the relationship between years of schooling and the instrument of distance to school location. The result indicates that distance to school location highly correlates with years of schooling at a significance level of 1% for both countries. It can be interpreted that if individuals decide to pursue a school located in the same province in the urban area or different provinces/cities or countries, they are likely to have 3.1 more years of schooling in Vietnam and 2.6 more years in Thailand than their counterparts. This result is consistent with the expectation that distance to school positively correlates with years of schooling. Thus, distance to school location is a strong predictor of years of schooling. Moreover, the reported F-statistic is higher than the rule-of-thumb value of 10 suggested by Staiger and Stock (1997), leading to the rejection of the null hypothesis of a weak IV.
First-Stage Regression of RE-IV Estimation.
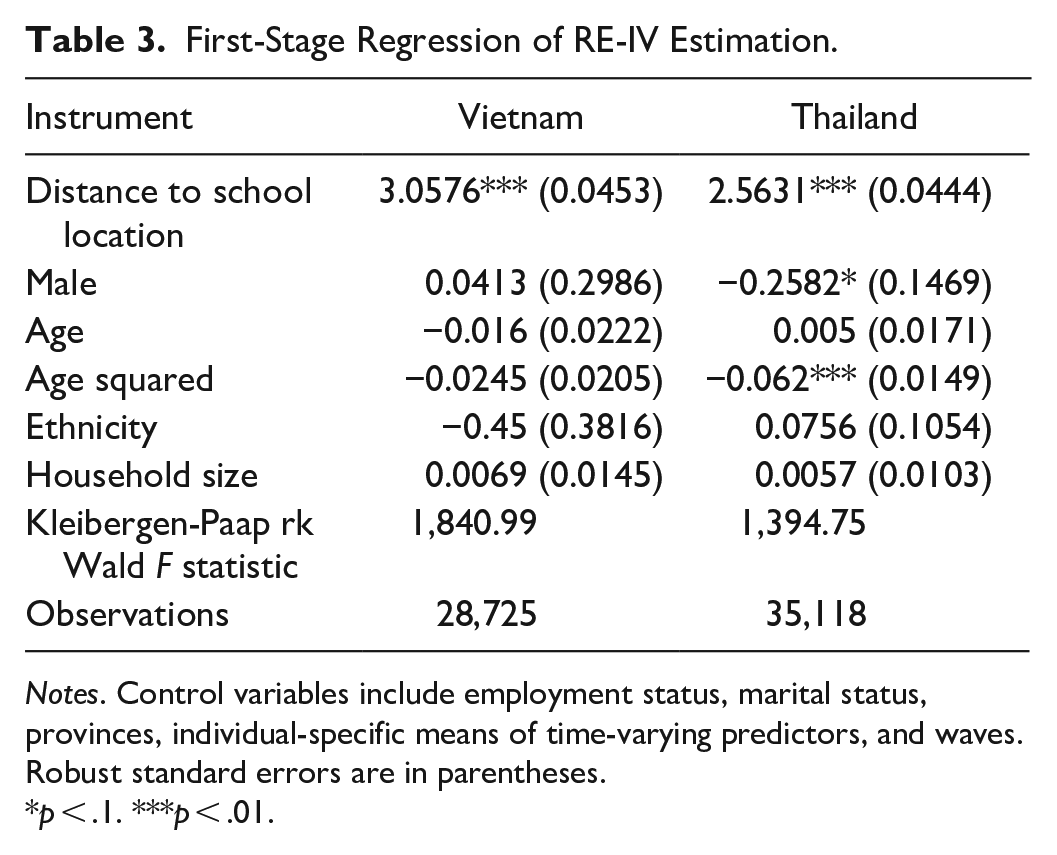
Notes. Control variables include employment status, marital status, provinces, individual-specific means of time-varying predictors, and waves. Robust standard errors are in parentheses.
p < .1. ***p < .01.
Table 4 presents the analysis results of the impact of education on health in Vietnam and Thailand using the basic ordinary least squares (OLS) method and RE-IV method. In particular, we regress three measures, including current health status, having diseases, and BMI, on the key explanatory variable years of schooling. The estimation also includes control variables: gender, age, age squared, ethnicity, household size, dummies of employment status, marital status, provinces, and waves. It can be inferred from this table that education has a positive impact on all health outcome variables. In particular, the result shows that an additional year of schooling increases the probability of reporting a better health status by 0.5% and reduces the chances of having serious diseases by 0.8% using the RE-IV method in Vietnam. We also observe a similar impact of education on health among Thai people. However, education increases the BMI ratio among Vietnamese people while decreasing BMI among Thai people. The descriptive statistics show that the mean BMI ratio among Thai respondents is 22.59, higher than that of the Vietnamese respondents, at 20.2. Given the normal range of BMI for Asians (WHO Expert Consultation, 2004) between 18.5 and 23, we believe that these results imply better health for both countries because the BMI mean for Thai is closer to the upper threshold while the increasing BMI is considered as a good indicator of health for Vietnamese. According to Pham et al. (2017), Vietnamese health professionals believe undernutrition should be a higher priority than controlling obesity. Thus, education is shown to have a positive impact on people’s health in both countries. Intuitively, highly educated individuals are likely to have better health than their counterparts. Lastly, the results from the RE-IV method are consistent with outcomes from the OLS method across all of the health measures. Almost all of the magnitudes of the RE-IV method are larger than results from the OLS approach in almost all cases, indicating the potential biases from the OLS approach due to the possible endogeneity from the education variable. Given that the OLS estimation provides biased results, the RE-IV approach is applied for the rest of the study.
The Relationship Between Education and Health.

Notes. Control variables include employment status, marital status, provinces, individual-specific means of time-varying predictors, and waves. Robust standard errors are in parentheses.
p < .1. **p < .05. ***p < .01.
The positive effect of education on health aligns with the previous literature. Similar results have been found in many countries such as Germany, the U.S., the U.K., China, Ireland, and Australia (James, 2015; Kemptner et al., 2011; Lleras-Muney, 2005; Ma et al., 2018; Tran & Tran, 2019; Zhong, 2016). Although much previous study has been conducted in developed countries due to the availability of the data, the benefits of education on health are also found in emerging countries like Vietnam and Thailand. Therefore, this study enhances the necessity of education in developing countries.
Aggregate Analysis
Aggregate analysis by gender
This section investigates the heterogeneity of the effect of education on health across different demographic groups by gender and ethnicity. Table 5 presents the results of the impact of education on health by gender. In Thailand, all of the coefficients are statistically significant for female respondents, showing that the positive impact of education on health exists among women. This is consistent with the previous literature that indicates that women seem to enjoy more benefits of education through employment opportunities in the labor market (Yousefy & Baratali, 2011) or better maternal health (Weitzman, 2017).
Effect of Education on Health by Genders.
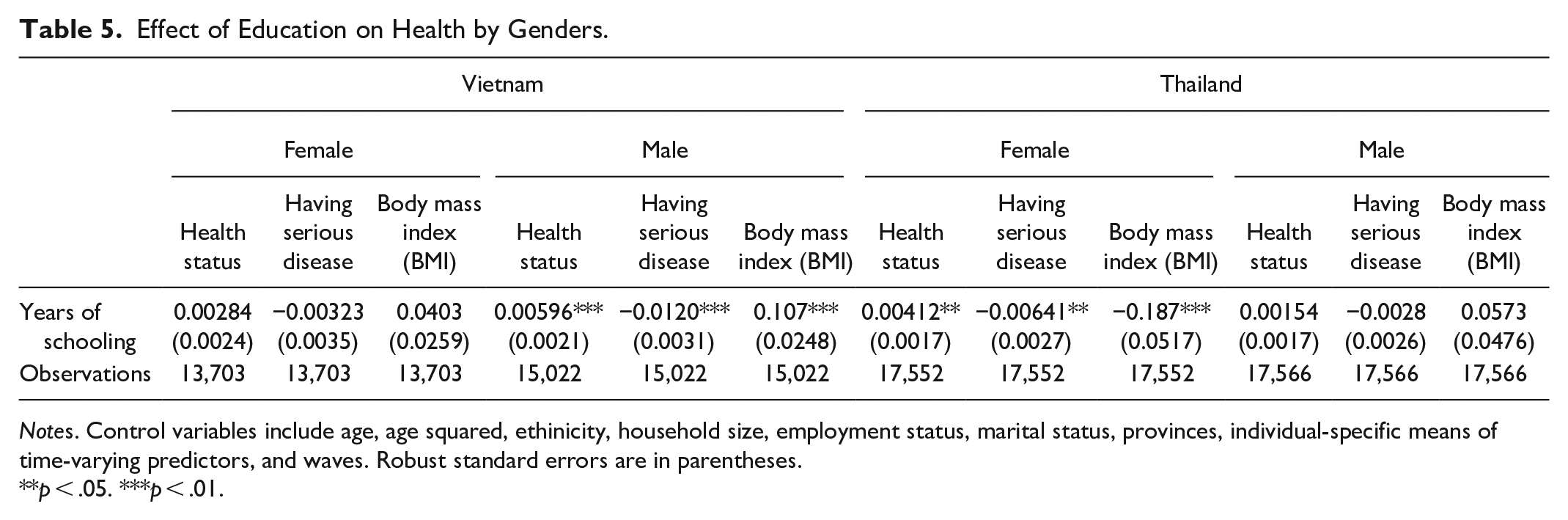
Notes. Control variables include age, age squared, ethinicity, household size, employment status, marital status, provinces, individual-specific means of time-varying predictors, and waves. Robust standard errors are in parentheses.
**p < .05. ***p < .01.
In Vietnam, surprisingly, education is shown to have no effect on all of the health outcomes among women, whereas this effect exists among men. Having noticed that the data of this paper are drawn from three provinces in rural areas in Vietnam where most of the habitats rely on agricultural business, the results might reflect the fact that the access to education among women is limited. The education gap between men and women in Vietnam still exists despite the efforts of the Vietnamese government (Mai & Brundrett, 2020). From our estimation sample, Vietnamese women obtain 8.2 years of schooling while the average years of schooling among men is approximately 8.9 years. There are some possible explanations for this finding. First, Confucianism’s emphasis on the family heavily dominates women’s lives. Women face social injustice and discrimination in the Confucian structure of society (Gao, 2003). Household chores and childcare responsibilities are still primarily performed by Vietnamese women (Teerawichitchainan et al., 2010). Second, women’s health also involves maternal health. A study by Nguyen et al. (1993) shows that most women had their first birth before age 20, whereas women with higher education have a significantly higher age at first birth than those with little or no education. Additionally, rural women and those with little or no education married at significantly younger ages than urban women and those with secondary education. Thus, young age marriage can interfere with schooling and even cause educational setbacks among women. Women’s education should not be undervalued. The previous literature shows that educated women have better employment opportunities, have better health conditions, and better childcare (e.g., Shieh & Halstead, 2009). Despite the lack of evidence of the effect of education health among women in rural provinces in Vietnam, the benefit of education might exist in other forms such as better employment chances or their children’s health. Therefore, the return on education might be underestimated if other non-monetary benefits of education are ignored (Vila, 2000).
Aggregate analysis by ethnicity
In terms of ethnicity, a study by Cooper (2002) suggested that education is a more suitable instrument to investigate the ethnic inequality in health than social class. Additionally, the study indicates that education has a different impact on the health of ethnic groups, suggesting that educational disadvantage is a major factor in explaining the higher morbidity. Table 6 shows the effect of education on health between the majority Kinh people and the ethnic minorities. In particular, education improves current health status, reduces the probability of having serious diseases, and increases BMI among Kinh people. Additionally, education is much more important to health for ethnic people because education improves current health status and reduces the probability of having serious diseases which leads to a crucial implication of improving the health of the ethnic community. In contrast, in Thailand, the coefficients of education on health are significant across three health outcomes of the Thai majority, whereas the coefficients are insignificant among Thai ethnic minorities. Vietnam has 53 ethnic minorities, accounting for 14.6% of the total population in 2015. Most live in mountainous and highlands areas with very limited access to infrastructure, healthcare, and education (UNDP, 2016). Moreover, they also account for as high as 50% of the total poor population (World Bank, 2013). Due to the isolated living areas, there are fewer opportunities for exchanges and integration with the broader society, leading to a very low school enrollment rate at the required age.
Effect of Education on Health by Ethnicity.

Notes. Control variables include gender, age, age squared, household size, employment status, marital status, provinces, individual-specific means of time-varying predictors and waves. Robust standard errors are in parentheses.
p < .1. **p < .05. ***p < .01.
The Explanation of the Positive Effect of Education on Health
How is education associated with income and health insurance?
This section examines the mechanisms through which education has an impact on people’s health. Two possible channels are considered in this paper: health insurance and household income. The literature has shown that educated people are likely to have a higher concern about their health (Cutler & Lleras-Muney, 2008). The probability that a highly educated person buys health insurance is higher than their less-educated counterparts. Moreover, the positive impact of health insurance on health or health care utilization has been confirmed in the previous literature. Many medical studies have shown that health insurance has a positive impact on people’s mortality (e.g., Woolhandler & Himmelstein, 2017), use of healthcare services, and reduced depression and financial strain (Baicker et al., 2013). Furthermore, Sommers et al. (2017) showed evidence that health insurance affects many aspects that have an impact on health, such as strengthened financial security and more access to healthcare utilization. People with health insurance tend to have a higher level of hospital admission, longer inpatient medical care, and more inpatient services (Sepehri et al., 2006; Thanh et al., 2014). Thus, it is justified to consider whether health insurance is truly a mechanism of how education affects health. Additionally, income is a crucial resource to improve people’s health (Braveman et al., 2010; Doorslaer & Koolman, 2004). People with higher income are able to buy healthy foods, afford expenses for physical activities or recreational activities and have better access to higher quality healthcare services, which may have an impact on people’s health. Thus, this paper employs household income and health insurance as mechanisms to see how higher educated people improve their health. The household income is converted into 2005 PPP$ using a conversion rate provided by the data provider for both countries. To remove the outliers of income, we have winsorized at level 1st and 99th percentiles. Lastly, we apply the logarithm function to obtain our final variable. Health insurance is a dummy variable with a value of 1 if the respondents answer they have life insurance, health insurance, or disability health insurance and 0 otherwise.
Table 7 indicates that additional years of education are positively associated with higher household income and a higher probability of having health insurance among Vietnamese and Thai people. Overall, it is possible that people with higher education are likely to have better health because they have higher income and are more likely to be insured. This hypothesis is formally tested in the next section.
The Potential Mechanisms of Income and Health Insurance.
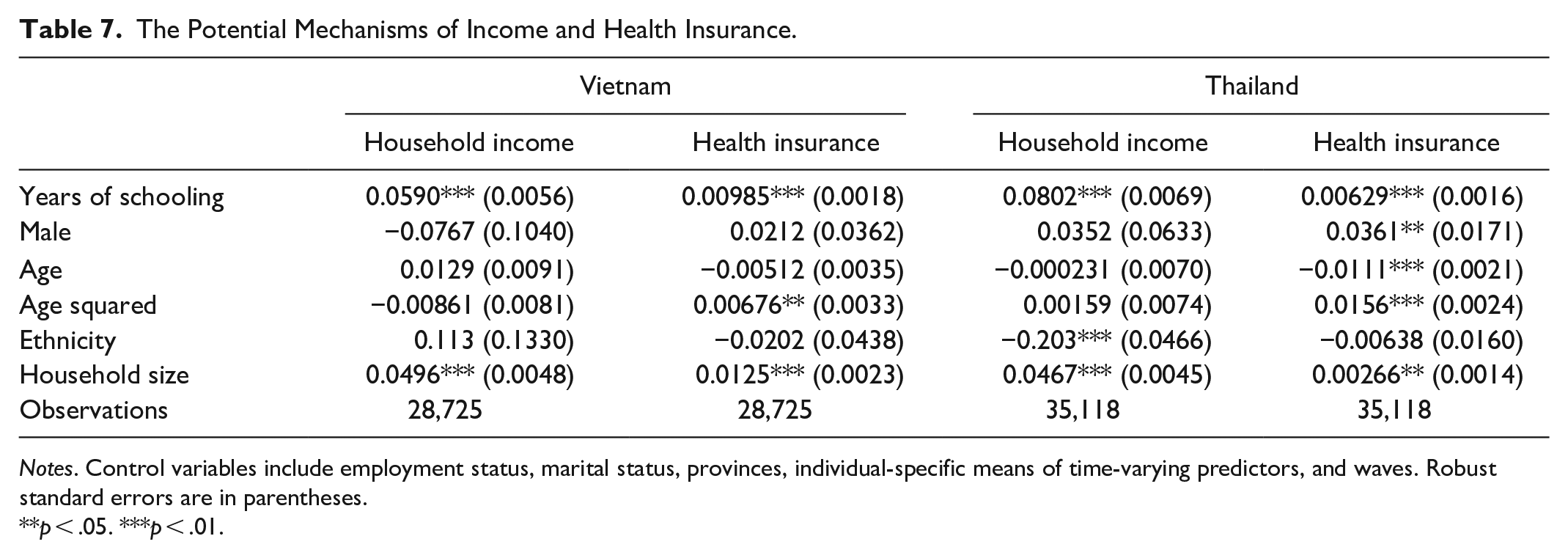
Notes. Control variables include employment status, marital status, provinces, individual-specific means of time-varying predictors, and waves. Robust standard errors are in parentheses.
**p < .05. ***p < .01.
Mediation analysis
Given the previous results, household income and health insurance may be factors that partially explain the positive effect of education on health. A formal mediation analysis proposed by Baron and Kenny (1986) is conducted to perform to confirm the mediation role, in which the two proposed mediators are included as additional regressors. Two requirements must be met to ascertain that income and insurance are valid mediators. First, the main effect of education is expected to drop once these mediators are controlled for in the regression models. Second, the proposed mediators must remain statistically significant. Additionally, the Sobel (1982) test is employed to determine whether such a drop in coefficients of the main effect is statistically significant. In other words, this test examines whether the indirect effect of education on our health via the possible mediators (i.e., income and insurance) is statistically significant. The formula of the Sobel test is derived as t-test:
Specification 1 in the odd columns in Table 8 estimates our models without controlling mediators including income and health insurance, while specification 2 includes them. First, all relationships between education and health remain significant except for health status in Vietnam. Second, regarding the magnitude, the effect on health status reduces by 50.6% when two mediators are controlled. Similarly, there is a reduction in the effect of having serious diseases and BMI, which drop by 35% and 32.4%, respectively. All coefficients of income are found to be statistically significant except for the relationship between education and having serious diseases. Lastly, the results of the Sobel test show that the indirect effects of income are statistically significant, indicating that household income is a mediator of the positive effect of education on Vietnamese people’s health, including current health status and BMI. However, the coefficients of having health insurance are insignificant in Vietnam, indicating that health insurance does not mediate the relationship between education and health outcomes.
Mediation Analysis.

Notes. Control variables include gender, age, age squared, ethinicity, household size, employment status, marital status, provinces, individual-specific means of time-varying predictors, and waves. Robust standard errors are in parentheses. Sobel tests are presented in square brackets.
**p < .05. ***p < .01.
Turning to Thailand, almost all of the magnitude of this effect is reduced when the mediators are controlled in specification 2. In particular, the main effect drops in the case of health status by 14.3%, by 16.4% for having serious diseases, and increases by 25.9% for BMI. Moreover, the coefficient of health insurance is only significant for BMI at a p-value < 0.01 and for having serious diseases at a p-value < 0.05. However, because the direct effect between education and BMI does not drop and the Sobel test for health insurance does not pass (less than the threshold of a 1.96%–95% confidence interval), health insurance is not the mediator in the relationship between education and health outcomes. Additionally, all of the coefficients of household income are insignificant. Thus, neither income nor health insurance mediates the relationship between education and health among Thai people.
Conclusion
Without realizing the non-monetary benefits of education, returns to education can be undervalued. This study provides evidence of the relationship between education and health in three rural provinces in Vietnam and Thailand. To tackle the potential endogeneity problem, the distance to school location is used as the instrument for an individual’s education. Using the RE-IV approach, the results indicate that more highly educated people are likely to report a better current health status, reduced probability of having serious diseases in both countries, increased BMI in Vietnam and reduced BMI in Thailand. Additionally, there is evidence that the effect is heterogeneous in terms of gender and ethnicity. The results also suggest that household income is the mechanism of how education affects health in Vietnam. The evidence contributes to the extension of the current literature on the positive effect of education on health, highlighting the importance of education in developing countries.
This study has some limitations. Because the data are collected from three rural provinces in Vietnam and in Thailand, the conclusions from the results might not be generalizable to other parts of these countries. Therefore, more representative data are needed for further investigation. Moreover, the data of health behaviors or social-psychological capital are not available for further understanding of the mechanisms of how education affects health, which could be an interesting path for future research.
Based on our results, some important implications are suggested for both countries’ investment in education. Because the positive effect of education on Vietnamese people’s health has been validated, it is important for policymakers as a source of reference for strategies to improve people’s health. Although both countries have implemented educational policies such as the National School Health Policy in 1998 in Thailand or continuing educational reforms in Vietnam, several aspects can be further considered. First, health-related courses should be developed as a compulsory curriculum in the school syllabus. For example, the government should provide maternal, reproductive, and medical training courses. For those children born into adverse family environments, early interventions such as childcare centers or home visitations could alleviate some of the initial disadvantages. The policies highlight the importance of early childhood education. Several programs such as the Perry Preschool Project and the Carolina Abecedarian Project in the U.S. have shown wide-ranging benefits, including improved health in later life (Zajacova & Lawrence, 2018). Further research is needed to inform new future model educational programs. Ideally, the health stock accumulated from these investments would reduce the future healthcare expenditure in people’s later life.
The health benefits of education are recognized only in certain demographic groups in Vietnam and Thailand. We recommend governments not to aim to improve health by encouraging education for the whole population, which is costly for the governmental budget, especially in the context of developing countries. Instead, promoting education among vulnerable groups (i.e., women, and ethnic minorities) should be prioritized. For example, women’s education in rural provinces should be a primary concern due to its benefit in terms of employment opportunities, children’s health, and the reduction of underage marriage practices. Accordingly, provincial authorities should encourage women to obtain more education by expanding opportunities such as free basic education, flexible classes, and even employment offers, given their social inequalities.
Regarding ethnicity, the government should continue focusing on the development of ethnic minority communities by promoting education, given the presence of severe health inequity (Målqvist et al., 2013). Although the Vietnamese government has already emphasized the development of these communities by issuing Decision No. 1557/QD-TTg in 2015, setting many objectives for Millennium Development Goals indicators associated with the Sustainable Development Goals, some further aspects can be considered. First, due to the landscape isolation and language barriers, certain details of the legal framework should be modified and specified only for ethnic minority communities. Second, local authorities – with their firsthand understanding of the social and financial situation of their respective communities – should be given a more visible role in the development process of these areas. For example, early childhood education should be emphasized among ethnic children, and the literacy rate of the official language should also be focused on to promote further integration with the larger community. The government should initiate programs involving closing the gaps in educational outcomes between ethnic minority populations and their ethnic majority counterparts to promote health equity. Lastly, given that the positive effect of education on health can be explained by the higher income, household income subsidy from the government, including scholarship, tuition fee reduction, and special education programs for children, can relieve the family’s financial burden and amplify the positive impact of education on health.
Footnotes
Acknowledgements
The data was kindly provided by the Thailand Vietnam Socio-Economic Panel (TVSEP) from the research project “Poverty dynamics and sustainable development: A long-term panel project in Thailand and Vietnam, 2015–2024,” financed by the Deutsche Forschungsgemeinschaft (DFG). I am grateful to the TVSEP team for their support and assistance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by Vietnam National Foundation for Science and Technology Development (NAFOSTED) under grant number 502.01-2020.303.
Research ethics and consent
This study requires no ethics approval and consent for the authors as the analysis used only deidentified existing unit record data from the Thailand Vietnam Socio-Economic Panel (TVSEP).
Data availability statement
Data cannot be shared publicly because the current study is subject to the signed confidentiality deed. Data are available from the Thailand Vietnam Socio-Economic Panel (TVSEP) for researchers who meet the criteria for access to confidential data. The data underlying the results presented in the study is available from the Thailand Vietnam Socio Economic Panel, email: