
Abstract
Campus sexual assault has been recognized as one of the most pressing issues on college campuses and an epidemic across the U.S. This study aims to explore perceived prosocial behavior change of one bystander intervention training in two different modalities: synchronous virtual via Zoom and asynchronous online training via a learning management system (LMS). To date, no research study evaluates the same bystander intervention program across different intervention delivery modalities. This research is the first to examine the relationship between intervention delivery modality and post-evaluation questions and serves as a pilot study for future research. Secondary data used in this study were collected between October 2020 and April 2021. The study sample consisted of first-year college students enrolled at a public midsize southeast university in the United States. The total population of this study includes (n = 195) first-year students who completed the bystander intervention training (BIT) and the post-evaluation survey. To examine the significant association between each post-evaluation question and racial identity, gender identity, and sexual orientation a Fisher’s exact test was conducted. In the LMS modality, Black/African American participants (n = 19) had 92% times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to White/Caucasian participants (n = 30). The need for adaptive college campus programming that meets the expectations and needs of students today is a valuable contribution to public health. This study aims to open a research pathway to provide further recommendations to enhance inclusion efforts for sexual assault prevention programming.
Plain language summary
The purpose of this study is to understand if there are differences in racial and gender identities along with sexual orientation as it relates to perceptions of bystander intervention. The training consisted of two online platforms, one with a facilitator and one without. Research is the first of its kind to evaluate only online bystander intervention training among 195 undergraduate students. Results indicated Black/African American participants had 92% times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this bystander intervention non-facilitator training compared to White/Caucasian participants. This study is limited with no control group and cannot be assumed true at other institutions. This study is unique in its ability to adapt programming during COVID-19 and evaluate the different identities in relationship to a broad-scope program.
Introduction
Campus sexual assault has been recognized as one of the most pressing issues on college campuses and an epidemic across the U.S. (Rice, 2018). In the last 30 years, sexual assault statistics on college campuses have remained vastly unchanged (Vagianos, 2017). Recently, data has shown a 13% prevalence rate among all gender identities who had experienced sexual victimization while attending college (Cantor et al., 2020; Woods et al., 2020). It is estimated that 1 in 5 women and 1 in 16 men are sexually assaulted while in college (Krebs et al., 2007). Study findings in the 2016 American College Health Association (ACHA) revealed that within the previous 12 months, 11.4% of females, 4.4% of males, and 22.4% of transgender students experienced sexual touching without consent (ACHA, 2016). Moreover, data supports that females and TGQN (transgender, genderqueer, non-conforming, questioning, or something not listed) are at the highest rates of victimization while in college (ACHA, 2016).
Conceptualization of Campus Sexual Assault
College campuses pose a higher risk of sexual assault compared to national rates (Garcia et al., 2012; Krebs et al., 2007). Studies indicate that since entering college, 22% of students reported experiencing at least one incident of sexual assault, with higher rates among women and gender-nonconforming students (Mellins et al., 2017). Transgender, genderqueer, and nonconforming individuals also face elevated risks of sexual assault compared to cisgender females and males (Campus SaVE | RAINN, n.d.). Prior victimization of sexual assault is a significant predictor of re-victimization during college (Conley et al., 2017; Cusack et al., 2021; Hetzel-Riggin et al., 2021; Mellins et al., 2017; Neilson et al., 2018; Walsh et al., 2012). Further, alcohol consumption is commonly associated with sexual assault incidents, contributing to at least half of reported cases (Beaver, 2017).
Survivors of sexual violence often experience long-term health consequences, including anxiety, depression, post-traumatic stress disorder (PTSD), eating disorders, suicidal ideation or attempts, substance misuse, poor academic performance, physical injury, sexually transmitted infections (STIs), fear of intimacy, and somatization (Amar & Gennaro, 2005; Banyard et al., 2020; Black et al., 2011; Campbell et al., 2003; Campbell et al., 2009; Classen et al., 2005; Fisher et al., 2000; Gidycz et al., 1995; Gidycz et al., 2008; Jordan et al., 2014; Kaura & Lohman, 2007; Krauss et al., 2021; Okuda et al., 2011; Shorey et al., 2008; Zinzow et al., 2010).
Underreporting is a significant issue in addressing sexual assault, with most incidents going unreported to authorities (Kelly & Stermac, 2008). Hindrance of reporting can be contributed to fear of retaliation and knowledge of the perpetrator (Rape, Abuse and Incest National Network [RAINN], 2020). There is a misperception that false reporting is relatively high, however, false reporting is relatively rare, comprising only 2% to 10% of reported cases (Lonsway & Archambault, 2019; Lisak et al., 2010; NSVRC, 2021). Due to variation in state laws related to rape and consent, impacting survivors’ willingness to report and exacerbating the problem. Reporting sexual assault can be a complex process for college students, involving multiple systems such as law enforcement, campus police, and Title IX offices (Hirsch & Khan, 2020, p. xix). Shame and silence within college communities contribute to the underreporting of sexual assault incidents (Hirsch & Khan, 2020, p. xix). Furthermore, the readability of reporting instructions can also present barriers to reporting (Taylor, 2018).
The profound impact of experiencing sexual violence can affect personal health and wellness, mental health, and academic health. Health outcomes associated with interpersonal violence include, but are not limited to; eating disorders; suicidal ideation or attempts; binge drinking and substance misuse; poor academic performance; physical injury; sexually transmitted infections (STIs); fear of intimacy; and somatization (Amar & Gennaro, 2005; Banyard et al., 2020; Black et al., 2011; Campbell et al., 2003; Campbell et al., 2009; Classen et al., 2005; Fisher et al., 2000; Gidycz et al., 1995, 2008; Jordan et al., 2014; Kaura & Lohman, 2007; Krauss et al., 2021; Okuda et al., 2011; Shorey et al., 2008; Zinzow et al., 2010).
Evolution of Policies Addressing Campus Sexual Assault in the U.S
Campus sexual assault has been a recognized issue since as early as 1950 (Hirsch & Khan, 2020, p. xxii). Over the years, various policies, acts, and guidance have been implemented, shaping the landscape of sexual assault on college campuses in the United States. This section discusses key milestones in this evolving landscape.
Title IX of the Education Amendments of 1972 (Title IX)
In the early 1970s, discussions surrounding campus sexual assault gained momentum on college campuses nationwide. Advocates successfully lobbied for the enactment of Title IX of the Education Amendments of 1972. Title IX ensures that no individual in the United States is excluded from, denied benefits of, or discriminated against in any education program or activity based on their sex. It also encompasses sexual harassment and sexual violence, including rape, sexual assault, sexual battery, and sexual coercion (Know Your Rights, 2021). Title IX requires federally funded institutions to distribute a policy against sex discrimination, appoint a Title IX Coordinator, and establish procedures for reporting and addressing complaints promptly and effectively. Title IX has also been extended to protect LGBTQ+ and gender and sexual minority (GSM) students. However, criticisms have emerged, highlighting the need to address historical policies that perpetuate racial and gender inequities. The U.S. Department of Education issued a guidance letter reaffirming Title IX protections for transgender students, providing crucial support for their rights (Office for Civil Rights Blog - 20210726, 2021).
The Clery Act (Campus Security Act)
The term “date rape” gained attention in the 1980s, sparking discussions about sexual violence on campuses (Kamenetz, 2014). In 1990, the Clery Act was passed in memory of Jeanne Clery, a college student who was raped and murdered in her dorm room. The Act requires colleges to report on-campus crimes and issue timely warnings to the campus community about known risks (Clery Act, n.d.; Violence Against Women Act, 2014).
Dear Colleague Letter of 2011
In 2011, the U.S. Department of Education for Civil Rights issued the Dear Colleague Letter (DCL), which emphasized Title IX’s role in addressing sexual violence. It outlined requirements for institutions, such as designating a Title IX Officer and providing complaint procedures (Dear Colleague Letter from Acting Assistant Secretary for Civil Rights Seth M. Galanter, 2020).
Violence Against Women Reauthorization Act
The Violence Against Women Act (VAWA), first enacted in 1994, was the first policy to address domestic violence and sexual assault as crimes. VAWA has undergone multiple reauthorizations and amendments, with the most recent one in 2021 aiming to address sexual violence in educational settings. The Act establishes an interagency task force to develop consistent responses and programming for high-risk populations, including LGBTQ+ students, and mandates the development of an online survey tool for campus safety (Jackson Lee, 2021).
Campus SaVE Act (VAWA Reauthorization)
In 2013, the Campus SaVE Act expanded and amended the Clery Act as part of VAWA (Campus SaVE | RAINN, n.d.; Clery Center, n.d.). This Act consolidated reporting requirements and expanded rights for campus interpersonal violence survivors, focusing on transparency and accountability for institutions in addressing and preventing sexual assault on campus. It also required institutions to provide resources for victims and implement prevention programming, including bystander intervention tactics (Campus SaVE | RAINN, n.d.; Clery Center, n.d.).
These policies have significantly shaped how campuses address and respond to sexual violence, providing support to survivors and fostering a safer campus environment. However, continued efforts are necessary to confront historical inequalities and implement effective policies across all U.S. higher education institutions.
Bystander Intervention Model
In 1968, Darley and Latané found that victims are less likely to offer help if other people are present in emergency situations which later would be known as the Bystander Intervention Model and used across the nation as a best-practice intervention for interpersonal violence programming. Later this model also demonstrates that the bystander effect is present even in non-emergency situations (Darley & Latané, 1968). Importantly, Aronson et al. (2016) note that helping someone is inversely related to the number of people present. Throughout the studies conducted by Darley and Latané, two constructs have been identified as the potential influence on bystander behavior (1) diffusion of responsibility and (2) social influence. Further research has shown that the intentional and evidence-based advancement of bystander intervention has the potential to reduce the prevalence of sexual assaults on campuses (Labhardt et al., 2017). To date, bystander intervention and gender-based violence programs are widely implemented on many college campuses in the U.S.
Although the bystander intervention model is widely disseminated on college campuses, there is a lack of diversity in program modality. Studies describe bystander programs to be primarily conducted in small groups and with a peer-led facilitator (Banyard et al., 2007; Coker et al., 2011; Kleinsasser et al., 2015; Potter & Moynihan, 2011). Further, small in-person program modalities can require human and financial capital, continued training of program leaders, lack of reach across campus populations, and reduction of public health impact (Kleinsasser et al., 2015; Salazar et al., 2014). Currently, there continues to be a lack of understanding of the impact of various intervention delivery modalities of learning that can be effective in bystander knowledge and efficacy (Devine, 2018).
Impacts of COVID-19
COVID-19 has exacerbated the economic and societal repercussions of sexual violence, leading to a heightened fragility in reporting structures for survivors. Similar to Hurricane Katrina, sexual assault incidents increased during the pandemic (Walker, 2020). Quarantine and lockdown measures further compounded the issue by limiting access to crucial services like therapy, community safe spaces, and intensive care units (Rousseau, 2020). Survivors were forced to endure unhealthy environments which contributed to negatively impacting their mental health, and increasing the risk of future assault and revictimization (Rousseau, 2020).
The reporting of sexual violence during disasters is often considered a “luxury issue,” adding to the existing problem of underreporting among sexual assault survivors (Klein, 2004). The continuation of isolation during COVID-19 burdened survivors with a lack of support, resources, and triggered trauma, further affecting their mental and physical well-being (MNCASA, 2020; UN Women, 2020). With colleges transitioning to online learning, students were cut off from critical resources like Title IX and community service providers (Klein, 2004; Ruiz et al., 2020). Surprisingly, there was a decrease in emergency department admissions for sexual assault and domestic violence, mirroring the luxury issue concept (Muldoon et al., 2021).
In contract, as the pandemic unfolded, the Alliance to End Sexual Violence reported an overwhelming increase in demand for local rape crisis centers, highlighting the lack of funding allocated to necessary services (Klein, 2004). Evidence shows that rates of sexual violence tend to increase during crises or emergencies (Klein, 2004; Walker, 2020). To emphasize that there is a difference between increased rates compared to those that choose to report. Although rates increase, reporting to certain entities (e.g., Title IX and emergency departments) may decrease due to availability and access during shutdown and contributing access to resources. Evidence shows that rape crisis centers have been overwhelmed with a surge in calls, reporting an increase of 40% in demand for services since the pandemic outbreak (Walker, 2020).
Research on the impact of racial inequity and sexual violence specifically among college populations is limited, but it indicates a stark impact on women of color and marginalized survivors (Ruiz et al., 2020). Studies suggest that racialized women, including Indigenous, Black, and other minorities, are at a higher risk of gender-based violence during the COVID-19 pandemic's response and recovery phases (Khanlou et al., 2021; Ruiz et al., 2020). Approximately 33% of college students in 2021 identified as Black/African American, Hispanic, or multiracial, emphasizing the importance of sexual violence programming and its impact on societal and health outcomes (College Enrollment Statistics, 2021). The studies discussed here underscore the far-reaching effects of sexual violence, encompassing economic impact, health outcomes, inequality, racism, and socio-economic disparities. Adaptive programming tailored to individual needs and resource availability during emergencies is vital in providing support to survivors of sexual violence.
Bystander Intervention Programming on Campuses
Technology plays a pivotal role in understanding how students are learning and engaging in bystander intervention and how these programs can effectively be administered (Mujal et al., 2021). “Bystander intervention programs could then be a tool utilized to debunk rape culture and provide victims with confidence and additional support to report a sexual assault” (Labhardt et al., 2017). In a 2015 study, Kleinsasser et al. (2015) found that an online bystander intervention program resulted in increased levels of prosocial self-efficacy feelings compared to the control group. Evaluating innovative approaches to engaging and empowering bystanders on college campuses is a valuable contribution to social justice and public health.
Summary of Online Sexual Violence Training
Culture of Respect has developed a comprehensive matrix containing detailed information about various sexual violence prevention programs, including program type, audience, estimated costs, and program specifics (Find the Right Tool | Culture of Respect, n.d.). Analysis of the matrix data in 2021 revealed that only 18% of programs were exclusively offered online, 47% were conducted solely in person, and 34% provided both online and in-person training. Figure 1 illustrates the national distribution of program modalities, highlighting the limited availability of online programming even post-COVID-19 pandemic.

Sexual violence prevention programs offered online, in-person, and both programs on U.S. college campuses as of 2021.
Figure 2 showcases the associated costs of these programs, indicating that some institutions face budget constraints when implementing sexual violence-specific initiatives. Determining exact prices was often challenging, requiring demos, or consultations. Roughly 29% of programs fell within the $100 to $999 cost range, while only 15% explicitly disclosed prices exceeding $1,000. Additionally, 24% of programs did not have publicly available prices and required a demo request to gain access to price information. Approximately 21% of all programs offered no-cost options, encompassing either the entire program or specific components. These figures were developed by researchers based on available information using the matrix, providing insights into the current modalities and costs of violence prevention programming. However, it's essential to note that these figures do not encompass all violence prevention training, as they only include information publicly accessible without a demonstration request through Culture of Respect.
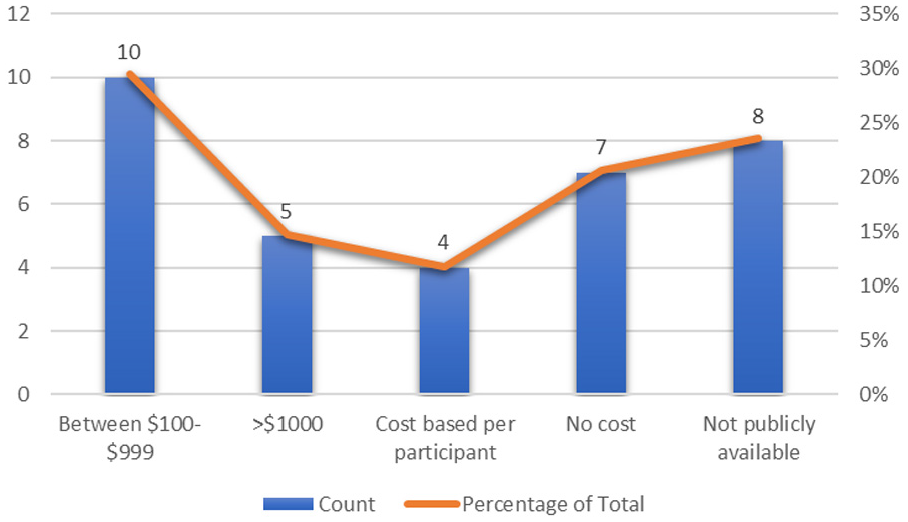
Sexual violence prevention program cost on U.S. college campuses as of 2021.
Study Significance
To better support survivors of sexual violence, it is crucial to have adaptive programming tailored to individual needs and resource availability during emergencies. Online bystander intervention has emerged as a flexible and budget-friendly addition to traditional methods (Devine, 2018). However, in the face of budget cuts and remote education, there is a lack of research on which intervention modalities may be more effective in fostering self-efficacy (Devine, 2018; Kleinsasser et al., 2015). This study focuses on two online modalities, synchronous sessions via Zoom with live facilitators and asynchronous sessions through a self-paced learning management system (LMS).
Bystander intervention training (BIT) was offered at no cost to undergraduates, graduates, faculty, and staff at the institution through three modalities, in-person, synchronous via Zoom, and asynchronous via the institution’s LMS. In-person and via Zoom had a live trained facilitator leading the training while the LMS modality did not have a live facilitator, but pre-recorded facilitators led asynchronous videos. Assessment of program cost and procedural steps were done prior to the start of this study. Original data were collected between 2018 and 2021 BITs. During 2019, all BITs were offered in-person and facilitated by trained student workers or staff members, however, demographic data was not collected. Therefore 2019 data were excluded from the present analysis. In 2020, the adaptation to online programming quickly became the norm as the COVID-19 pandemic created stay-at-home orders, however, a continuation of programming was needed. During the pandemic and into 2021, BITs were hosted by a trained facilitator via Zoom in a synchronous virtual format or as an asynchronous course on the institution’s LMS. Data used in this study was collected between October 2020 and April 2021, as this was the timeframe of collection of first-year course enrolled students who completed the training either via Zoom or LMS.
All delivery modalities consisted of approximately 1 hr of content delivery, with two knowledge checks taking less than 5 min embedded in the content. Demographic information was evaluated during the first knowledge check. All participants were required to complete the two knowledge checks and a post-evaluation survey to receive course credit.
The institution’s BIT was developed by trained staff and graduate students using evidence-based resources such as RAINN, NSRVC, Culture of Respect, ACHA, It’s On Us, and best-practice intervention strategies. The synchronous delivery included a PowerPoint presentation with prompts led through guided facilitation while the asynchronous delivery included pre-recorded videos embedded into the content platform. All modalities entailed first-hand examples of non-binary characters involving alcohol use who experienced sexual assault. Through facilitated discussion questions, the participants had to discuss verbally or through discussion boards the scenario and the approach to being an active bystander. Moreover, the participants were asked by the facilitator about the race and gender identities in this scenario to further provide students with myths regarding the victim and perpetrator. Participants were surveyed in a knowledge check to further understand myths on survivorship, mental health, and false reporting.
Topics covered in the course included the importance of being an active bystander and outlined practical steps for protecting targets of abusive behavior and preventing future violence. Objectives of the BIT included: identifying the concepts, barriers, and benefits of bystander intervention; exploring effective approaches for bystander intervention such as distracting, supporting survivors, and reporting; content coverage of consent, healthy relationships, sexual assault, harassment, non-consensual pornography, and gender violence; review of campus and community resources.
The purpose of this secondary data analysis is to explore the perceived prosocial behavior change of one bystander intervention training in two different modalities: synchronous virtual via Zoom and asynchronous online training via a learning management system (LMS). The use of sexual assault and sexual violence are often used throughout this paper as interchangeable terms.
The purpose of this study is two-fold (1) to evaluate post-evaluation questions in relation to two intervention delivery modalities (synchronous virtual Zoom and asynchronous LMS) and (2) to understand the associations between post-evaluation questions among subgroups of racial and gender identities and sexual orientation among first-year course students at a public midsize Southeast regional university in the United States. This study seeks to evaluate to achieve its purpose by posing four research questions (RQ1) to compare ordinal post-evaluation questions between synchronous and asynchronous intervention delivery modalities; (RQ2) to compare post-evaluation questions between synchronous and asynchronous modalities among racial identities; (RQ3) to compare post-evaluation questions between synchronous and asynchronous modalities among gender identities; (RQ4) to compare post-evaluation questions between synchronous and asynchronous modalities among sexual orientation.
Methods
This study used secondary data collected from cross-sectional posttest-only design with no control group. Data used in this study were collected between 2020 and 2021, during the months of October to April. The study sample consisted of first-year college students enrolled at a public midsize southeast regional university in the United States.
Original Data Collection Purposes
Original data was used for internal program evaluation of the institutional department’s BITs and were collected from 2018 to 2021. During 2019, BITs were offered in person and facilitated by trained student workers or staff members, however, demographic data was not collected. Therefore 2019 data were excluded from the present analysis. In 2020, the adaptation to online programming quickly became normalized as the COVID-19 pandemic created stay-at-home orders, however, a continuation of programming was needed. During the pandemic and into 2021, BITs were hosted by a trained facilitator via Zoom in a synchronous virtual format or as an asynchronous course on the institution’s LMS. Data used in this study were collected between October 2020 and April 2021, as this was the timeframe of collection of first-year course-enrolled students who completed the training either via Zoom or LMS.
Instrumentation
The original data were collected using a cross-sectional post-test questionnaire convenience sampling including Likert-scale and open-ended questions with no control group, referred to in Appendix A. This research study was conducted using secondary data provided through Qualtrics post-evaluation survey responses. Data was sorted, matched, and de-identified using Microsoft Excel. Additionally, IBM SPSS and Microsoft Excel software were used for data analysis and interpretation.
Exclusion Criteria
Students who did not identify as enrolled in the first-year course were excluded from the study population. Participants that identified as faculty or staff members were excluded from the study due to the focus being on student behavior change. Those who did not complete the demographic information and the post-evaluation were not included in the overall analysis. The original data collection did not include a question about prior knowledge or education on bystander intervention training.
Human Participant Compliance Statement
Permission was obtained from the university’s Institutional Review Board Protocol No. H22271 prior to analyzing secondary data for this study. Data was coded to connect participants’ demographic information to post-evaluation data. Demographic information was collected at the first knowledge check, then post-evaluation data only collected student identification numbers, first and last name. Data was matched according to the student’s identification, first and last name, and email address by the Principal Investigator.
Due to the three-step matching process, a small loss to study was expected, although participants were required to complete all knowledge checks and post-evaluation to receive credit and a certificate for participating in the course. Nine participants were loss unmatched. Following the matching process, a separate “Research Dataset” was created by the Principal Investigator with no direct identifying information (e.g., first name, last name, email address, or student ID). Participants were de-identified and information in the “Research Dataset” only included demographic information and relevant post-evaluation data related to this study. Only survey items containing matched participant data were utilized for data analysis.
Sample and Population
The research study population included all first-year students enrolled in a bachelor’s program at the public midsize Southeast regional university (N = ∼22,000).
Sample Size
The sample population of students enrolled in the first-year course at the institution (n = ~1,000) included all students enrolled in a bachelor’s program regardless of classification or transfer credits. A total of (n = 207) first-year course-enrolled students completed the BIT between October 2020 and April 2021. Participants who did not complete the entire post-evaluation (n = 12) therefore were excluded from the study population. The total study population of this research study includes (n = 195) first-year students who completed the BIT and the post-evaluation survey via Qualtrics and meet eligibility criteria.
Measures
Preexisting data from a post-evaluation of undergraduate students was collected between October 2020 and April 2021, during the Fall 2020 and Spring 2021 semesters, and were utilized for secondary data analysis in this study.
All measures in the post-evaluation were previously used for program planning and improvement. The original data were collected using a cross-sectional post-test questionnaire convenience sampling with no control group. Table A1 illustrates the quantitative Likert-scale questions selected by the researchers for this study. In this dataset and during the original data collection, the term “successful student” was interpreted based on participants’ perceptions, encompassing factors such as positive grades, retention, matriculation through their degree, academic coping and resilience, health and wellbeing, mental health, and overall perceptions of success (see Table A1).
Design and Statistical Analysis
This study focused on, (1) determining the influence of BIT and two modalities among all first-year course-enrolled participants and (2) determining the influence of BIT and two modalities on subgroups within the study population. Research subquestions, relevant research information, variables, and types of measurement used in this research study see Table 1.
Plan for Analysis.
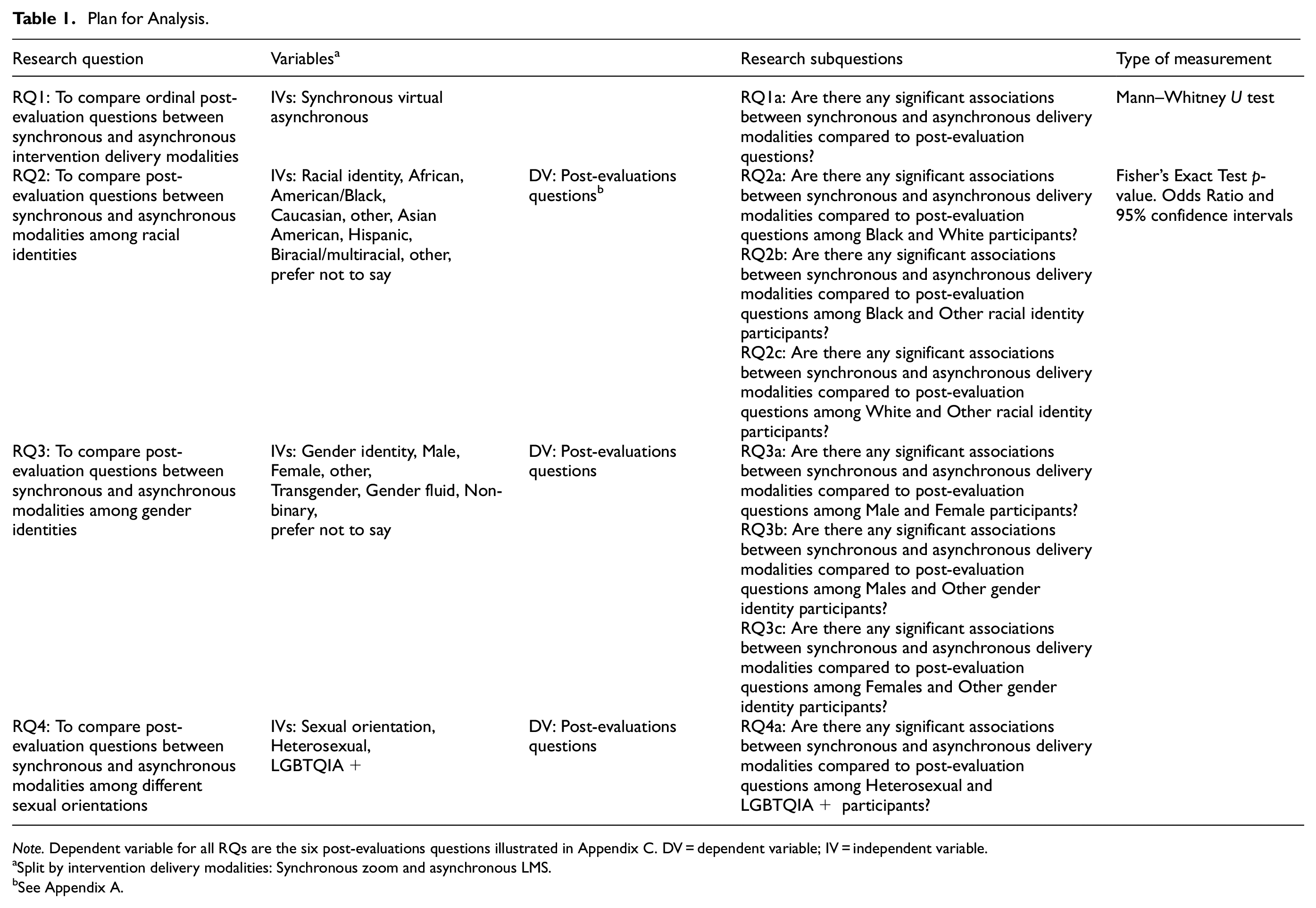
Note. Dependent variable for all RQs are the six post-evaluations questions illustrated in Appendix C. DV = dependent variable; IV = independent variable.
Split by intervention delivery modalities: Synchronous zoom and asynchronous LMS.
See Appendix A.
Descriptive Statistics
Participants were asked on the first knowledge checkpoint to self-identify their classification (freshman, sophomore, junior, senior), gender identity (male, female, transgender, other), racial identity (African American/Black, Caucasian, Asian American, Hispanic, Biracial/Multiracial, Other, Prefer not to say), sexual orientation (heterosexual, questioning, lesbian, gay, other), affiliated group (estudent-athlete, Fraternity and Sorority Life, first-year student course, faculty/staff, university health course). Only participants affiliated with the first-year course were included in data collection and analysis. The characteristics of independent variables including racial and gender identities and sexual orientation were recorded and measured in the results section of this study. Demographic data from the institution indicated in 2021, the student population's racial and gender identities align with the sample population. Females (60%), males (40%), White/Caucasian (57%), Black/African American (27%). No data was available for sexual orientation for the institution. Participant demographic data was compared to ensure the sample was representative of the institution’s population.
Comparisons Between Synchronous and Asynchronous Intervention Delivery Modalities
RQ1 aimed to determine if there was a significant association between post-evaluation questions and intervention delivery modality, associated with each specific post-evaluation question. Due to the distribution of data, the independent t-test assumptions were not met. Therefore, the non-parametric two-tailed Mann–Whitney two-sample rank-sum test was conducted to compare each post-evaluation question and intervention delivery modality, Zoom, and LMS. The two-tailed Mann–Whitney two-sample rank-sum test is an alternative to the independent sample t-test but does not share the same assumptions (Conover & Iman, 1981). A Mann–Whitney U test is used to compare two independent groups when the dependent variable is ordinal or continuous (Conover & Iman, 1981). There were 136 observations in the Zoom group and 59 observations in the LMS group.
Comparisons Between Synchronous and Asynchronous Delivery Modalities Compared to Post-Evaluation Questions Among Racial Identities, Gender Identities, and Sexual Orientation
To compare the associations between each post-evaluation question and the independent variables, racial identity (RQ2), gender identity (RQ3), and sexual orientation (RQ4) a Fisher’s exact test was conducted. A Fisher’s exact test examines the relationship between two nominal variables. It examines the cell counts of each combination of variables and compares the count with the expected value for that cell. Therefore, a Fisher exact test that does not make the assumptions of value size was most appropriate (Mehta & Patel, 1983).
Fisher’s exact test is similar to the Chi-square test of independence, but in this test, the p-value is computed exactly without using estimation to determine if the null hypothesis was met. This test also does not have any assumptions for the cell counts like the Chi-square test of independence, so usually, Fisher’s exact test is used on smaller datasets. Due to sparse data and one or more cell counts in the table less than 5, a Chi-square test of independence was not the appropriate measure due to the assumptions of value size per cell of the contingency table (Mehta & Patel, 1983). Fisher’s exact test is a nonparametric test to evaluate the significance between two nominal variables (Ember, 2016). Odds ratio (OR) were utilized to understand associations of Fisher’s exact tests with a p-value less than .05. The p-value is used to evaluate the results of the test. An alpha level of .05 was used when assessing the statistical significance of each post-evaluation question by modality based on subcategories of racial identity, gender identity, and sexual orientation. An alpha value of .10 was used to assess marginal significance due to the small sample size (n = 195) of each post-evaluation question by modality.
Due to sparse secondary data, the responses were categorized into nominal binary data to meet the parameters of Fisher’s exact test between racial identity, gender identity, and sexual orientation (see Figure 3). The Likert-scale responses were coded into one binary nominal variable negative response (3,2,1) coded 0 and positive responses (4,5) coded 1.

Binary coded variables explanation.
Results
Participant Characteristics
In total, 195 first-year students completed BIT for the institution. Frequencies and percentages were calculated for racial identity, gender identity, and sexual orientation split by synchronous Zoom and asynchronous learning management systems (LMS). Table 2 illustrates the percentage distribution of intervention delivery modality for each identity group. A total of n = 136 participants completed the synchronous Zoom bystander training and n = 59 completed the asynchronous LMS without a facilitator. In the overall sample, participants that completed the survey were primarily White, heterosexual, females. An exploration of participants’ self-identified demographic variables varied by modality (see Table 2).
Demographic Characteristics.

Note. Listed as n (%).
Demographic data from the institution indicates that in 2021, the student population’s racial and gender identities align with the sample population. Females (60%), males (40%), White/Caucasian (57%), and Black/African American (27%). No data was available for sexual orientation for the institution.
Research Question 1
To Compare Ordinal Post-Evaluation Questions Between Synchronous and Asynchronous Intervention Delivery Modalities
No significant differences were observed between intervention delivery modalities and any of the post-evaluation questions at the alpha level of .05. This suggests that the distribution of each question for the Zoom group was not significantly different from the distribution of each question for the LMS group. Table 3 presents the comparisons between intervention delivery modalities and post-evaluation questions from the Mann–Whitney U tests.
Associations Between Intervention Delivery Modalities and Post-Evaluation Questions.
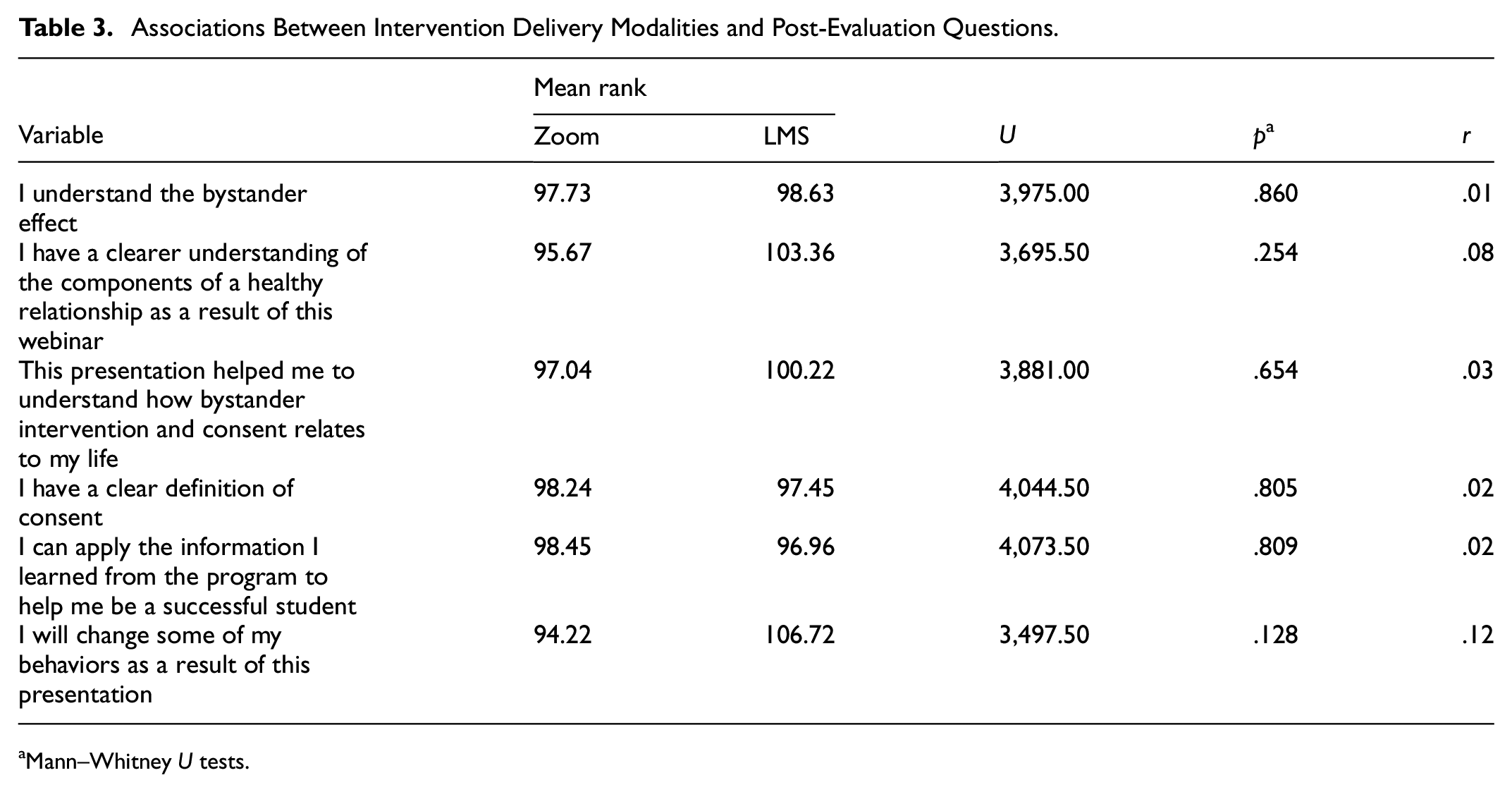
Mann–Whitney U tests.
Research Question 2
To Compare Post-Evaluation Questions Between Synchronous and Asynchronous Modalities Among Racial Identities
Racial identity and gender identity were significantly associated with the question, “I will change some of my behaviors as a result of this presentation.”Table 4 presents the comparisons between Zoom or LMS modalities among demographic variables using Fisher’s exact test. In LMS modality delivery of BIT, the odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT was 92% lower for White/Caucasian participants relative to Black/African American participants (OR = .08; 95% CI [.01, .71]), p = .008.
Associations Between Black/African American and White/Caucasian Participants Positive Responses in LMS Modality.

Note. Two-tailed significance. OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Research Question 3
To Compare Post-Evaluation Questions Between Synchronous and Asynchronous Modalities Among Gender Identities
In LMS modality delivery of BIT, females had 6.12 times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to males, OR = 6.12; 95% CI [1.67, 22.48], p = .008. Table 5 presents the comparisons of males and females in LMS intervention delivery modality.
Associations Between Males and Females Positive Responses in LMS Modality.
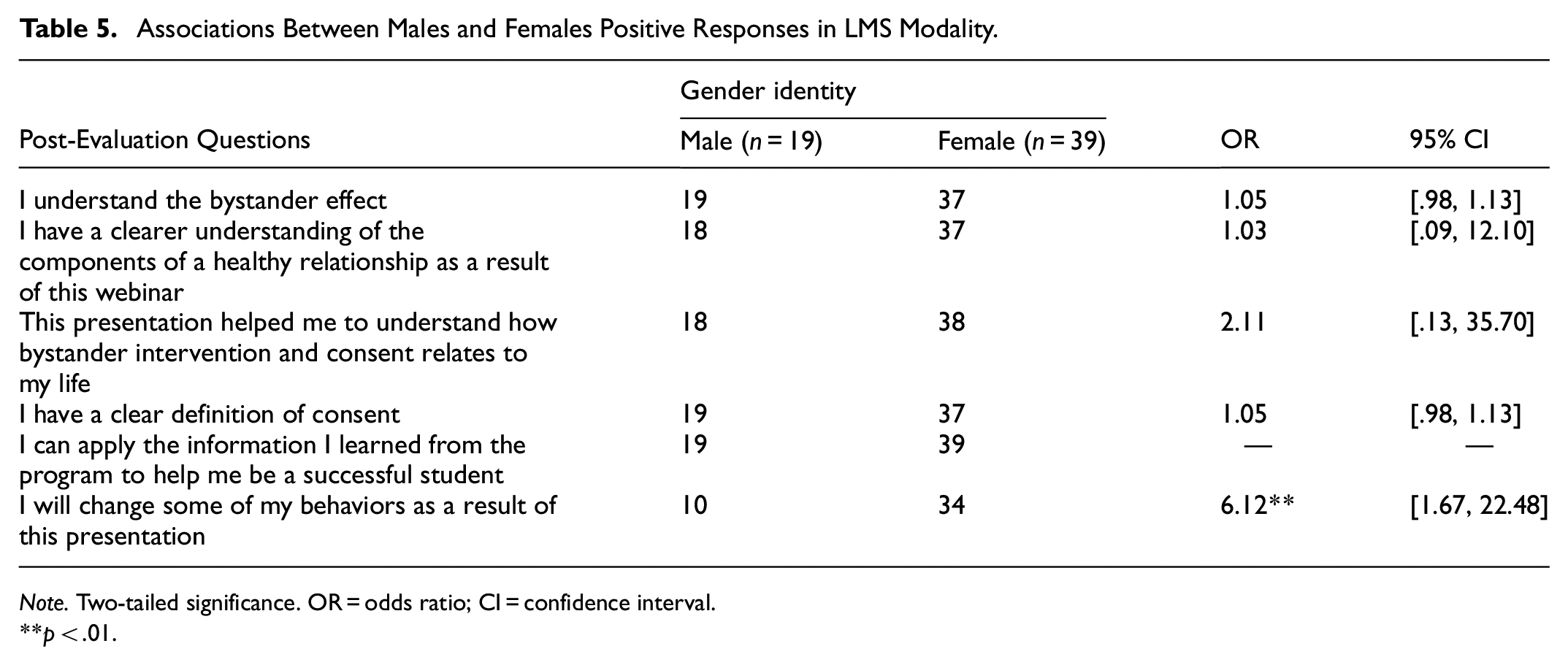
Note. Two-tailed significance. OR = odds ratio; CI = confidence interval.
p < .01.
To further explore this association, racial identity, and gender identity for LMS BIT modality were combined. Black/African American female participants had 1.42 times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to White/Caucasian female participants (OR = 1.42; 95% CI [1.04, 1.93]), p = .044. Table 6 summarizes the associations between combined racial identity and gender identity for LMS significant associations described above. No other significant associations were found with combined racial and gender identities, likely due to limited response data. Figure 4 summarizes the significant associations found in this section. The critical findings and the implications for practice, policy, and research have been effectively summarized. (Tables 7 and 8).
Associations Between Black/African American Females and White/Caucasian Females in LMS Modality.

Note. Two-tailed significance. OR = odds ratio; CI = confidence interval.
p < .05.

Odds ratio and confidence intervals of change in behavior and positive responses by gender and race, respectively, for LMS.
Critical Findings.
Implications of the Review for Practice, Policy, and Research.

Research Question 4
To Compare Post-Evaluation Questions Between Synchronous and Asynchronous Modalities Among Different Sexual Orientations
No significant associations were found among sexual orientation or other questions. Results for the nonsignificant associations between racial identity, gender identity, and sexual orientation in Zoom and LMS intervention delivery modality.
Discussion
It is essential to recognize the public health implications of this research, particularly concerning the health outcomes and academic well-being of college students. The economic burden of sexual assault on college campuses is significant, making effective intervention programs crucial in mitigating the issue (Brodsky, 2014). By expanding knowledge and understanding of bystander intervention training, this research aims to provide valuable insights into addressing sexual violence within college communities.
Relevant Findings
The following section is organized by research questions. When relevant, this section includes where the findings confirm, contradict, or further illuminate the gap in knowledge previously found in the literature. Banyard et al. (2004) conducted a study aiming to explore the community impact of the bystander approach as a means to address community-level issues. Additionally, self-efficacy theory suggests that adopting new behaviors can lead to a ripple effect of change both in the individual and the environment (U.S. Department of Health and Human Services, 2005). Community-level change results from the cumulative effect of individual behavior change (Salazar et al., 2014). Leveraging technology and LMS, sexual violence prevention programming can effectively influence social and cultural norms, challenge rape beliefs, raise awareness about victim-blaming, reduce toxic masculinity, and destigmatize the topic. This research contributes valuable insights to current studies, emphasizing behavior change and suggesting promising directions for future research on diverse populations and different intervention delivery modalities.
Differences Between Modalities. In Spring 2020, approximately 1,300 colleges and universities canceled in-person classes and shifted to fully online instruction (Smalley, 2021). Moreover, the hardship of the economy of the COVID-19 pandemic had a stark effect on university funding that was already financially constrained (Dickler, 2020). Consistent evidence has demonstrated that in times of crisis or emergency rates of sexual violence increase (Klein, 2004; Walker, 2020). Since the rise of COVID-19 in communities, rape crisis centers have been overwhelmed with an upsurge in calls (Walker, 2020).
RQ1 aimed to understand the association between post-evaluation questions and BIT delivery modalities of synchronous Zoom compared to asynchronous LMS. In the present study, no significant associations were found between any post-evaluation questions and the intervention delivery modalities.
In an earlier study, Johnson et al. (2021) conducted an evaluation of two instructional modes, in-person and synchronous online, revealing their effectiveness in fostering positive student outcomes over time. This study does not directly address change over time, Johnson et al. (2021) emphasize the importance of comprehending student outcomes over time concerning sexual violence and comparing different modalities. In another study, participants that viewed an online asynchronous intervention, “Take Care” found that results indicated online BIT may be an effective adaptation to sexual violence prevention (Kleinsasser et al., 2015). Devine (2018) indicates that in-person training has high self-efficacy scores, but self-efficacy was not significantly related to intervention between online and in-person.
Understanding the impact of different intervention delivery modalities on participant responses is crucial for public health initiatives. Research question one examines the association between intervention delivery modalities and participant post-evaluation responses to facilitated learning versus self-paced learning. A lack of significance uncovering this association could reveals that there is no significance of having in-person or online bystander training whether a live facilitator is necessary for building self-efficacy in bystander prosocial behavior, further research is needed on this topic with the potential of leading to cost savings and wider program reach if facilitators are not required. This research question sheds light on the existing gap in the literature concerning two online intervention delivery modalities, in contrast to previous studies comparing in-person interventions with online approaches. The study contributes to the current literature and knowledge by affirming that no significant differences were observed among bystander intervention delivery modalities. Continued research is needed to understand the longitudinal effects that modality has on change in bystander behavior.
Differences Between Racial Identities. In the asynchronous LMS BIT, results identified a significant association between perceived behavior change in the question, “I will change some of my behaviors as a result of this presentation.” In the LMS modality, Black/African American participants had 92% times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to White/Caucasian participants. This however was not significantly associated via Zoom which may offer insight into the potential barriers to synchronous facilitation or potential implicit biases occurring with a live facilitator compared to an asynchronous delivery modality. Measuring bias was outside the scope of this study, but a future direction to consider collecting qualitative data to further understand the barriers or benefits to the different intervention delivery modalities. The 95% CI [.01, .71], is a narrow range that represents decreased variability in the data to assess accuracy. Although, the sample size for Black/African Americans was less than n = 30 therefore this small sample size cannot be assumed to be generalizable.
In order to gain deeper insight into the relationship between racial and gender identities, the study combined race and sex variables. The previous description of the SHIFT research in this study highlights the intersectional factors impacting people of color, particularly Black survivors of sexual assault. Astonishingly, the reported prevalence of rape among Black women is 21.2%, although evidence suggests this figure is significantly lower than the actual incidents of assault (Breiding et al., 2015; Hirsch & Khan, 2020, pp. 244–255; James et al., 2017; The Criminal Justice System: Statistics | RAINN, n.d.).
Differences Between Biological Sex Identities. In the asynchronous LMS BIT, results indicated a significant association between perceived behavior change in the question, “I will change some of my behaviors as a result of this presentation.” In the LMS modality, females had 6.12 times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to males. Moreover, research supports that female students reported significantly greater intent to intervene compared to males (Hoxmeier et al., 2020). This finding supports the current study’s findings. The 95% CI [1.67, 22.48], is a wide range that represents increased variability in the data to assess accuracy. Although the sample size for males was less than n = 30 therefore this small sample size cannot be assumed to be generalizable. The small sample size is likely the contributing factor to the wide range confidence interval.
Limited findings were identified on the relationship between gender identity and BIT behavior change related to the post-evaluation question described above. Findings from this study aligned with other studies which found women report higher levels of bystander efficacy (Amar et al., 2014). Au contraire, this study observed lower levels of intention to act as a positive bystander relative to other research (Amar et al., 2014).
Research demonstrates that there is a lack of consistency or knowledge of gender differences in sexual violence prevention programming with regard to proximity to change resulting in behavior change. Theoretically, the behavioral intent is proximal to actual behavior but is a significant limitation of all bystander intervention programs (Hoxmeier et al., 2020). It can be assumed that gender norms and roles are a factor contributing to the difficulty to measure this area of interest.
Additionally, a lack of data revealed that (n = 2) Black/African American males were enrolled in this research BIT for LMS which illustrates the gap in sample size to draw adequate conclusions. Further, the role of hypermasculinity, toxic masculinity, and cultural norms in male-identified spaces could be a contributing factor to the limited number of males enrolled in this study BIT and a future area of research to investigate social norms and barriers to opting out of sexual violence prevention programming.
Differences of Combined Racial and Biological Sex Identities. This study supports current research in BIT. In a study by Brown et al. (2014), results indicated that Black students, especially Black females, reported greater bystander behaviors. This aligns with 6 comparing Black/African American females to White/Caucasian Females which found that Black/African American female participants had 1.42 times greater odds of agreeing or strongly agreeing to change some behaviors as a result of this BIT compared to White/Caucasian female participants in LMS modality. The 95% CI [1.04, 1.93], is a narrow range that represents decreased variability in the data to assess accuracy. Although the sample size for both Black and White females was less than n = 30 therefore this small sample size cannot be assumed to be generalizable.
Research specific to racial identities and sexual violence programming on college campuses is only found in a few studies to date. The book “Sexual Citizens” by Hirsch and Khan (2020) is a recent publication that invests in understanding the racial disparities existing in sexual violence programming, however, there is still a wide research gap in this area. This study contributes to the body of knowledge by addressing the perception of behavior change in an asynchronous LMS that can be used for future practical use and in the development of programming to address upstream and downstream racial disparities in victim-blaming, support services, cultural norms, policies, program planning that are related to sexual violence prevention programs.
No significant associations were found between RQ2a via Zoom, RQ2b, and RQ2c in Zoom or LMS. This is likely due to the limited sample size, little to no negative responses among the small sample size, and no comparative pre-test. This is a limitation of this study addressed in the limitations section.
Differences Between Sexual Orientation Identities
No significant associations were found among heterosexual and LGBTQIA+ participants, but it is important to highlight the need to include LGBTQIA+ participants and ask sexual orientation questions in future sexual violence SV work. “There is a compelling and urgent need for intervention and prevention strategies that are relevant, appropriate, and accessible to LGBTQ communities” (NSVRC & PCAR, 2012). Current protocols focus primarily on heterosexual students and this study is not without that limitation.
This study encompasses LGBTIA+ participants in data collection and analysis, however, a barrier to this study is a small sample size. Research states that past SV research has controlled for sexual identity and excluded the population from research results (Siepser et al., 2019). A total of (n = 39) participants self-identified as LGBTIA+ which offers promise to further explore the relationship between BIT modalities. In this study, it is valuable insight that among the overall participant percentage more students identified as LGBTIA+ in LMS compared to Zoom, 22% and 19% respectively. This contributes information for future research that the potential for anonymity in an online learning environment may contribute to more students self-identifying as LGBTIA+. This study, similar in participants’ racial identity, had a higher level of LGBTQIA+ participants compared to other study populations regarding bystander intervention training on college campuses. This provided context to this study that included mostly first-time enrolled college students might not have had a coming out experience yet or are still hesitant to self-identify in the LGBTQIA+ community. The need for further research may provide insightful information for bystander intervention modalities across different age groups.
Limitations
Despite its valuable insights, this study has several limitations. The small sample size and subsample sizes exploring post-evaluation questions may have affected the study’s findings. The study sample primarily consists of White heterosexual females, reflecting the institution’s enrollment, but future research should aim for a more diverse and representative sample to gain insights into subpopulations. Generalizability is limited as the data was collected from a single university’s program, without a control group or pre-test, making it challenging to measure program effectiveness and participants’ prior knowledge. The use of secondary data also presented data quality and availability issues. Additionally, the study was conducted during the COVID-19 pandemic, potentially impacting social support systems and access to resources, affecting prosocial behavior. Cross-sectional data hinders the ability to predict long-term behavior changes, making future longitudinal research important. Students’ familiarity with the online learning platform could be a potential limitation affecting knowledge. Type I errors were considered in the analysis, but future research should further address potential confounding variables. Confidence intervals with large ranges might be due to limited subsample size, requiring further investigation. Moreover, online bystander intervention training findings have been contradictory, necessitating more research as students adapt to online learning environments and align training with federal guidelines. Overall, more qualitative and quantitative research is required in sexual violence prevention training and intervention delivery modality to develop effective and comprehensive strategies.
Conclusions
The study findings indicate differences in perceived behavior change among students based on LMS intervention delivery modality, particularly showing increased odds for female students, Black/African American students, and Black/African American female students. It is important to acknowledge that this research centers specifically on bystander intervention, which relates to someone not directly involved intervening to alter outcomes. This study does not focus on the perceived barriers to intervening nor the impact of bystander intervention. The study establishes associations between bystander perceptions and subgroups of racial identity, gender identity, and sexual orientation but does not claim causality. Due to the lack of a pre-test, no baseline was established, but the study provides valuable insights for future university interventions, training, and evaluation recommendations. It is a valuable contribution sexual violence prevention to assess two online training programs, offering a pilot opportunity to understand modalities that may best serve college students in the post-COVID-19 era. Continued efforts to implement similar training that evaluates an array of included identities referred to in this study across U.S. college campuses, specifically in departments such as Title IX, Student Wellness, Health Centers, and Sexual Assault Response Teams.
The study aimed to promote an understanding of online training options and enhance public health and inclusion efforts for practical use and research. Sexual violence is a complex issue with upstream and downstream factors and social determinants of health, and this research highlights increased self-reporting among LGBTIA+ students in an LMS format and higher odds of behavior change perception among Black/African American participants. Ultimately, the goal of this research is to provide tools to create a culture of informed bystanders and continue progressing toward addressing sexual violence effectively.
Footnotes
Appendix A
Omitted Post-Evaluation Questions from Original Data Collection.

| Original post-evaluation question | Question type (Qual/Quant) | Rationale for omission |
|---|---|---|
| Name three sexual assault prevention resources available to you on campus or in the community | Qual: Open-ended | Omitted due to revealing identifying information about the institution and community |
| Define bystander intervention | Qual: Open-ended | Omitted due to this study using quantitative responses via Likert-Scale questions |
| What did you like best about this program? | Qual: Open-ended | Omitted due to irrelevant topic and process evaluation measure for the department |
| How can this program be improved? | Qual: Open-ended | Omitted due to irrelevant topic and process evaluation measure for the department |
| I believe the services provided by the X Department helps students succeed in school | Quant: Likert-scale | Omitted due to irrelevant topic and process evaluation measure for the department |
| I enjoyed the presentation and would recommend it to a friend | Quant: Likert-scale | Omitted due to this study measuring individual-level behavior change and the broad nature of the verbiage “enjoyed” |
Acknowledgements
I thank my dissertation committee for the wealth of knowledge and discussion that took place to finalize this work. I would like to acknowledge the labor that the Student Wellness department have put in developing a program for students and the future of research this may lead to.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.