
Abstract
The study determined the level of treatment adherence motivation in outpatients with diabetes mellitus and examine the relationship between cognitive emotion regulation skills and treatment adherence motivation. This descriptive, correlational study included 458 diabetes mellitus outpatients. Data were collected via an online survey comprising a Patient Information Form, the Turkish Modified Morisky Scale, which assesses treatment adherence through motivation and adherence related knowledge subscales, and the Cognitive Emotion Regulation Questionnaire, which measures adaptive and maladaptive emotion regulation strategies. Analyses included correlations and binary logistic regressions. Participants had a mean age of 51.02 years; 50.4% were women, and 58.7% had type 2 diabetes mellitus. Over half exhibited low motivation for treatment adherence. Motivation was negatively associated with maladaptive strategies such as other-blame (rho = −.181, p < .001) and catastrophizing (rho = −.101, p < .05). Positive reappraisal, an adaptive strategy, was positively associated with motivation. Logistic regression showed that motivation was significantly predicted by positive reappraisal (B = 0.14), catastrophizing (B = −0.12), planning (B = −0.12), and education level (B = −0.30; p < .05). Conversely, treatment knowledge was significantly predicted by age (B = −0.025) and education (B = −0.433), but not by emotion regulation strategies. Over half of the participants of diabetes mellitus exhibited low treatment adherence. Low treatment motivation is common among diabetes mellitus outpatients and is influenced by both emotion regulation and sociodemographic factors. While knowledge alone is insufficient, emotion regulation strategies—especially maladaptive ones—play a critical role. Interventions that combine psychoeducation with emotion-focused approaches may enhance adherence in chronic illness care.
Plain Language Summary
This study examined how motivated people with diabetes mellitus are to follow their treatment plans, and how their emotional coping strategies and knowledge about treatment relate to this motivation. A total of 458 patients with diabetes participated in this study by completing an online questionnaire. The questionnaire included questions about their personal and health information, a scale measuring their motivation and knowledge about following treatment, and how they mentally cope with stress. Participants were on average 51 years old, and slightly more than half were women. Over half of the participants (52.8%) showed low motivation to follow their treatment plans. Interestingly, having more knowledge about treatment didn’t always mean patients were more motivated. People who often blamed others or imagined worst-case scenarios were less likely to feel motivated. Many patients with diabetes struggle with staying motivated to follow their treatment, especially when they use unhelpful emotional coping styles like blaming others or thinking negatively. This suggests that psychological support to improve emotion regulation could help them stick to their treatment better.
Introduction
Diabetes Mellitus (DM) treatment is generally conceptualized within a biopsychosocial framework, incorporating endocrinological interventions, nutritional guidance, and exercise programs. Ensuring patient adherence to their treatment plan is crucial for a successful disease course (AlQarni et al., 2019; Catapan et al., 2021; The American Diabetes Association, 2020). Adherence includes following the recommended medical regimen and organizing daily life according to the disease’s demands. However, the significant lifestyle and behavioral changes required can be challenging for patients to accept and adapt to (Ågård et al., 2016). Reduced treatment adherence in patients with DM is associated with a higher prevalence of cardiovascular and neurovascular complications, sensory impairments, renal dysfunction, and an increased likelihood of surgical interventions such as amputation (Alsahly, 2023; Warren & Hixenbaugh, 2020). Kim et al. (2018) found that poor treatment adherence led to a 41% increase in cardiovascular diseases. Similarly, Algeffari (2018) reported a 35% rise in neurovascular complications, and Gheith et al. (2016) noted a 40% increase in renal problems—emphasizing the importance of adherence through studies. Additionally, there has been a notable rise in psychological clinical symptoms and comorbidities (Alsahly, 2023; Warren & Hixenbaugh, 2020). To summarize, treatment adherence plays a critical role in reducing the morbidity of DM and preventing its complications. Accordingly, there is a clear need for large-scale studies to identify the factors influencing treatment adherence.
DM is a chronic disease prevalent worldwide and projections indicate that by 2045, Turkiye will rank among the top 10 countries with the highest number of DM cases. The prevalence of diabetes in Turkey has reached 13.2% as of 2019 and is expected to rise significantly due to urbanization, lifestyle changes and increasing obesity rates. Given the need for continuous medical assistance DM is a significant concern that healthcare professionals in Turkiye should meticulously address (International Diabetes Federation, 2019; Satman et al., 2013; Teufel et al., 2021). Understanding the impact of Turkiye-specific sociocultural factors on treatment adherence is vital for the development of local health policies and critical to improve the effectiveness of healthcare services.
Studies conducted across different cultures have shown that the extent to which an individual adheres to a treatment plan is influenced by various factors, including gender, age, smoking, alcohol consumption habits, employment status, perceived social support, engagement in daily and social activities, and levels of stress and distress. Disease-related characteristics, such as comorbidity, diabetes symptoms, duration and treatment, as well as age of onset, and collaboration with the health care provider also contribute to determining adherence. One key variable is an individual’s perception of the disease, knowledge and beliefs about DM. Thoughts and feelings about the disease have been shown to impact treatment adherence. Consequently, emotion and thought regulation strategies are crucial factors for DM (Jafari et al., 2024; Świątoniowska-Lonc et al., 2021; Tuobenyiere et al., 2023). In particular, the individual’s motivation for treatment, illness perception and demographic characteristics play an important role in predicting treatment adherence; however, how these factors interact with cognitive emotion regulation has not been sufficiently investigated (Ryan & Deci, 2000).
“Emotional regulation” refers to a person’s ability to initiate, inhibit, sustain or modify emotional arousal to meet their needs (Gross et al., 2006; Koole et al., 2011). The Emotion Regulation Model (Garnefski et al., 2001), which forms the conceptual framework of this study, posits that individuals use four maladaptive and five adaptive cognitive emotion regulation strategies to manage dysfunctional emotional responses. The frequent use of maladaptive strategies is a significant factor in developing conditions such as depression and anxiety disorders (Garnefski et al., 2001, 2002, 2004, 2009). The capacity to regulate emotions effectively is linked to an individual’s ability to survive and learn new coping strategies, thereby providing motivation.(Sheppes, 2020). Emotion regulation has been reported to enhance self-care abilities and quality of life in individuals with DM, and it is recommended that it be integrated into diabetes treatment and care. Indeed, there are also interventional studies focusing on emotion regulation in individuals with diabetes; as seen in the comprehensive literature review, there is no study directly examining the relationship between cognitive emotion regulation strategies and treatment adherence in DM patients (Aliä et al., 2025; Fisher et al., 2019; Javaherforooshzadeh et al., 2024; Seyfollahzadeh Janfada et al., 2023). This important gap is critical for understanding the role of psychological factors in diabetes management. Within the scope of this model, positive refocusing, plan refocusing, positive reappraisal, perspective taking and acceptance are classified as adaptive strategies, while self-blame, blaming others, rumination and catastrophizing are classified as maladaptive strategies. Understanding the role of these strategies in diabetes management will be an important step in the development of interventions to improve patients’ treatment adherence.
In light of these factors, the role of psychological strategies to improve treatment adherence is receiving increasing attention. Adherence to treatment regimens has been shown to improve patients’ quality of life while reducing the risk of microvascular and macrovascular complications, hospitalizations and healthcare costs (Borzouei et al., 2023; Evans et al., 2022; Majeed et al., 2021). As evident in the literature, ensuring treatment adherence in individuals with DM is important not only for patients but also for the sustainability of healthcare services and the associated burden (Aliä et al., 2025; Fisher et al., 2019; Javaherforooshzadeh et al., 2024; Seyfollahzadeh Janfada et al., 2023). Therefore, particularly in societies with rising DM prevalence, there is an increasing need for strategies that promote adherence. Given the need for continuous and multidimensional care, DM poses a significant challenge that requires integrated attention from healthcare professionals. Accordingly, the main research questions of this study are as follows: (1) What is the relationship between cognitive emotion regulation strategies and treatment adherence in diabetic patients? (2) To what extent do demographic characteristics and cognitive emotion regulation strategies predict treatment adherence motivation and level of knowledge about adherence? The following hypotheses were tested in outpatients with diabetes mellitus:
H1a: Adaptive cognitive emotion regulation strategies is positively correlated with treatment adherence motivation.
H1b: Adaptive cognitive emotion regulation strategies is positively correlated with treatment adherence-related knowledge.
H1c: Maladaptive cognitive emotion regulation strategies is negatively correlated with treatment adherence motivation.
H1d: Maladaptive cognitive emotion regulation strategies is negatively correlated with treatment adherence-related knowledge.
H1e: Demographic characteristics and cognitive emotion regulation strategies significantly predict treatment adherence motivation.
H1f: Demographic characteristics and cognitive emotion regulation strategies significantly predict treatment adherence-related knowledge.
Methods
Research Design
The study was descriptive and correlational, utilizing single-time measurements. Data collection followed the Checklist for Reporting Results of Internet e-Surveys published by EQUATOR, which serves as a method and reporting guide for online survey research (Eysenbach, 2012).
Participants
The study was conducted in Izmir, the third-largest city in Türkiye. The research population consisted of outpatients who were receiving treatment at the Diabetes Polyclinics of two private hospitals within the city. Based on administrative records, the average daily number of adult patient admissions to these clinics ranged between 470 and 500. Data collection occurred over a period of 3 months, during which all patients who met the predetermined inclusion criteria were invited to participate in the study. Consequently, the entire eligible population was included, obviating the need for a formal sampling procedure.
Inclusion and exclusion criteria: Participants had to be receiving treatment for DM, have the technological means and skills to use online data collection tools and be able to read and physically complete the data collection form independently. Exclusion criteria included cognitive impairments that hindered comprehension, communication, judgment, and decision-making while completing the data collection form, as well as the absence of a DM diagnosis.
The sample size was calculated using the GPower 3.1.9.7, the effect size was determined to be 0.277, with a power ratio of 0.95, requiring a minimum of 259 samples. Our sample of 458 exceeded this threshold. During the 3-month data collection period, approximately 1,200 unique patients were approached at the endocrinology outpatient clinics of two hospitals in Izmir, Türkiye. After excluding 27 responses due to incomplete data (e.g., >50% missing items) or invalid entries (e.g., inconsistent responses), the final sample consisted of 458 participants. The remaining 715 patients declined participation, primarily due to time constraints or difficulties using the online survey tool. Of these, 485 (40.4%) provided informed consent and completed the online questionnaire. A post hoc power analysis confirmed sufficient power to detect moderate correlations (r = .30) and odds ratios (OR = 2.0) in logistic regression analyses, ensuring robust statistical inferences.
Sociodemographic Characteristics and Medical History
The mean age of the participants was 51.02 ± 18.05 years (min = 18, max = 86). Regarding clinical characteristics, 55.2% (n = 253) had been diagnosed with DM for over 10 years, 58.7% were diagnosed with type 2 diabetes (Tables 1 and 2).
Sociodemographic Characteristics of Patients With Diabetes Mellitus (n = 458).
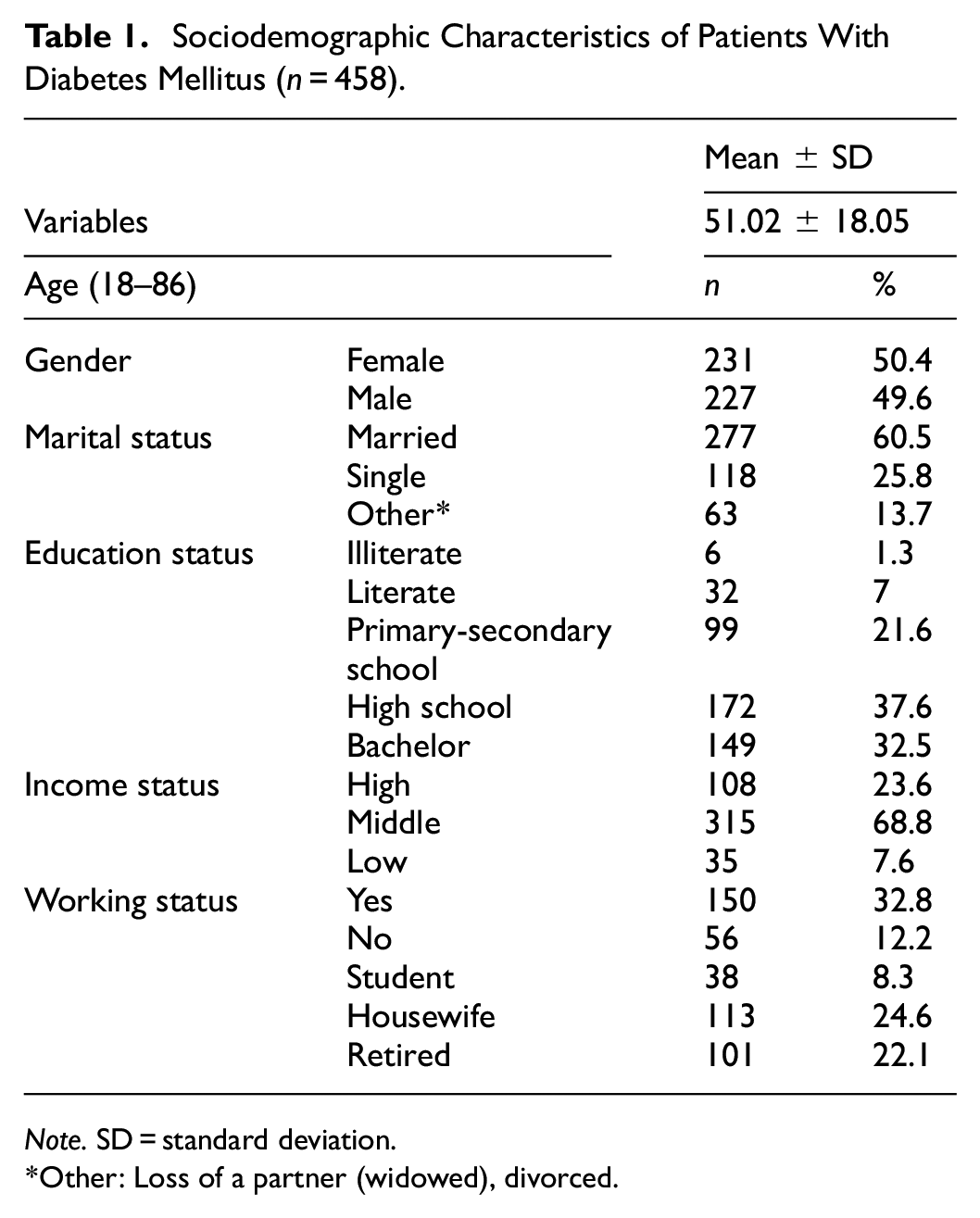
Note. SD = standard deviation.
Other: Loss of a partner (widowed), divorced.
Clinical Characteristics of Patients With Diabetes Mellitus (n = 458).

The percentage of rows was calculated.
Others: Hernia, psoriasis, cancer, sleep apnea, endometriosis, inflammatory rheumatic diseases, vasculitis, Parkinson’s disease, eye diseases, psychiatric diseases, respiratory system diseases.
Data Collection
The study announcement was made in person to patients present at the outpatient clinic. No monitoring or follow-up measurements were conducted. Once the patients expressed their willingness to participate, they could access the survey questions through an online link or by scanning a QR code. The research data were collected using a free online survey tool compatible with any internet-connected electronic device, making it a cost-effective choice. Participants were required to consent to the study by providing their name and surname, which the research team used as a security measure to prevent multiple entries. Four duplicate entries were identified and excluded from the final analysis.
Data Tools
Patient Information Form: The form comprises two sections—sociodemographic and clinical characteristics—totaling 18 questions included: age, gender, education level, occupation, marital status, smoking and alcohol habits, social support perception, DM type, duration, HbA1c levels, treatment regimen, complications, and hospital admissions. The form has been designed by the researchers (Aminde et al., 2019; Özkaptan et al., 2019).
Turkish Modified Morisky Scale (TMMS): This scale, developed by Morisky et al. (1986), was adapted to Turkish culture and examined for psychometric compatibility by Vural et al. (2012). This scale measures treatment adherence, comprising two subscales: motivation (e.g., intent to follow treatment) and knowledge (e.g., understanding of treatment requirements). The scale consists of two sub-dimension—motivation and knowledge—with six yes/no questions. For scoring, the second and fifth questions score “yes” as 1 point and “no” as 0 points, while the other questions score “yes” as 0 points and “no” as 1 point. For motivation subscale (items 1, 2, and 6), a total score of 0 or 1 indicates low motivation, while a score greater than 1 indicates high motivation. For knowledge subscale (item 3, 4, and 5), a total score of 0 or 1 from the indicates low knowledge, while a score greater than 1 indicates high knowledge (Vural et al., 2012). In this study, Cronbach’s alpha was .50, lower than ideal, likely due to the scale’s brevity (six items) and dichotomous response format, which can reduce internal consistency in short scales. Despite this, TMMS was selected for its cultural adaptation to Turkish diabetes patients and its frequent use in similar studies, ensuring relevance and comparability. The scale’s brevity was particularly advantageous for our online survey, aligning with data security priorities and minimizing participant burden in a diverse population (CHERRIES; Eysenbach, 2012).
The Cognitive Emotion Regulation Questionnaire (CERQ): This scale, developed by Garnefski and Kraaij (2007), measures individuals’ ability to regulate their emotions through their cognitive regulation strategies, including adaptive strategies (e.g., positive reappraisal, refocus on planning) and maladaptive strategies (e.g., catastrophizing, self-blame). The scale consists of 36 items and nine sub-dimensions. Higher scores in a sub-dimension indicate more frequent use of that cognitive strategy. The scale uses a 5-point Likert format (1 = never, 5 = always). The nine-factor structure was validated in Onat and Otrar (2010), with five subscales classified as adaptive (positive refocusing, refocus on planning, positive reappraisal, putting into perspective, acceptance) and four as maladaptive (self-blame, rumination, catastrophizing, other-blame). In the Turkish adaptation study by Onat and Otrar (2010), the scale was tested on students aged 18 to 33 from various faculties of a state university, yielding a Cronbach’s alpha coefficient of .78. In this study, the Cronbach’s alpha coefficient for the scale was determined to be .93.
Visual Analog Scale (VAS): The VAS was used to assess participants’ personal perception of adherence to diabetes treatment. This single-item, continuous scale ranges from 1 (very poor) to 5 (excellence), with participants marking their perceived adherence level on a line. The VAS is widely used in medical research to measure subjective constructs, such as treatment adherence, due to its simplicity and sensitivity to individual perceptions (Wewers & Lowe, 1990). In this study, participants responded to the question, “How well do you think you are complying with your diabetes treatment?.”
The developed online form was piloted with 10 participants to gather feedback on the clarity of the questions, the usability of the online tool and the overall data collection process, as well as the final control and editing of the data collection tools. However, the pilot study data were not included in the research sample. The data collection tools are user friendly and require no special conditions. Completing the tools took 15 min on average.
Data Analyses
Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess the data and, Mann–Whitney U and Kruskal–Wallis tests, and Spearman’s correlation analysis were employed (Rho; .00–.19 very weak, .20–.39 weak, .40–.59 moderate, .60–.79 strong, .80–1.00 very strong correlation; Gogtay & Thatte, 2017). To examine whether demographic characteristics and cognitive emotion regulation strategies predicted treatment adherence motivation among patients with diabetes mellitus, a binary logistic regression analysis was conducted. Based on the cutoff values established in the Turkish adaptation study by Vural et al. (2012), motivation scores were recoded into a binary variable. All predictor variables were checked for collinearity. Variance inflation factors (VIFs) were below 2, indicating acceptable levels of multicollinearity. Model fit was evaluated using the likelihood ratio chi-square test (χ2), and the variance explained was reported via Nagelkerke’s pseudo R2. The statistical significance level was set at p < .05.
Ethical Aspects
Research ethics approval was obtained from the Izmir BakirÓay University Ethics Committee for Non-Interventional Clinical Research (Approval Number/ Date: 1229/ 11.10.23), and institutional approval from the study hospitals. Confidentiality was assured, and data collection commenced only after participants confirmed their understanding and agreement. Participants provided their name and surname on informed consent forms, which were stored separately from survey responses to ensure anonymity. Survey data were anonymized using coded identifiers and stored on secure, password-protected systems, with access restricted to two research team members responsible for data management. Participants were informed of their right to withdraw at any time and to refuse the use of their data. Data security was maintained with limited access, restricted to two researchers, and the survey link was deactivated post-collection.
Results
The study tested six hypotheses regarding the relationship between treatment adherence motivation, treatment knowledge, and cognitive emotion regulation strategies, as well as the predictive role of demographic variables. Personal perception of adherence to DM treatment, assessed using the VAS scale, was determined to be 3.41 ± 0.92. Diabetes mellitus treatment adherence characteristics of patients were given in Table 3.
Treatment Adherence Characteristics of Patients With Diabetes Mellitus (n = 458).
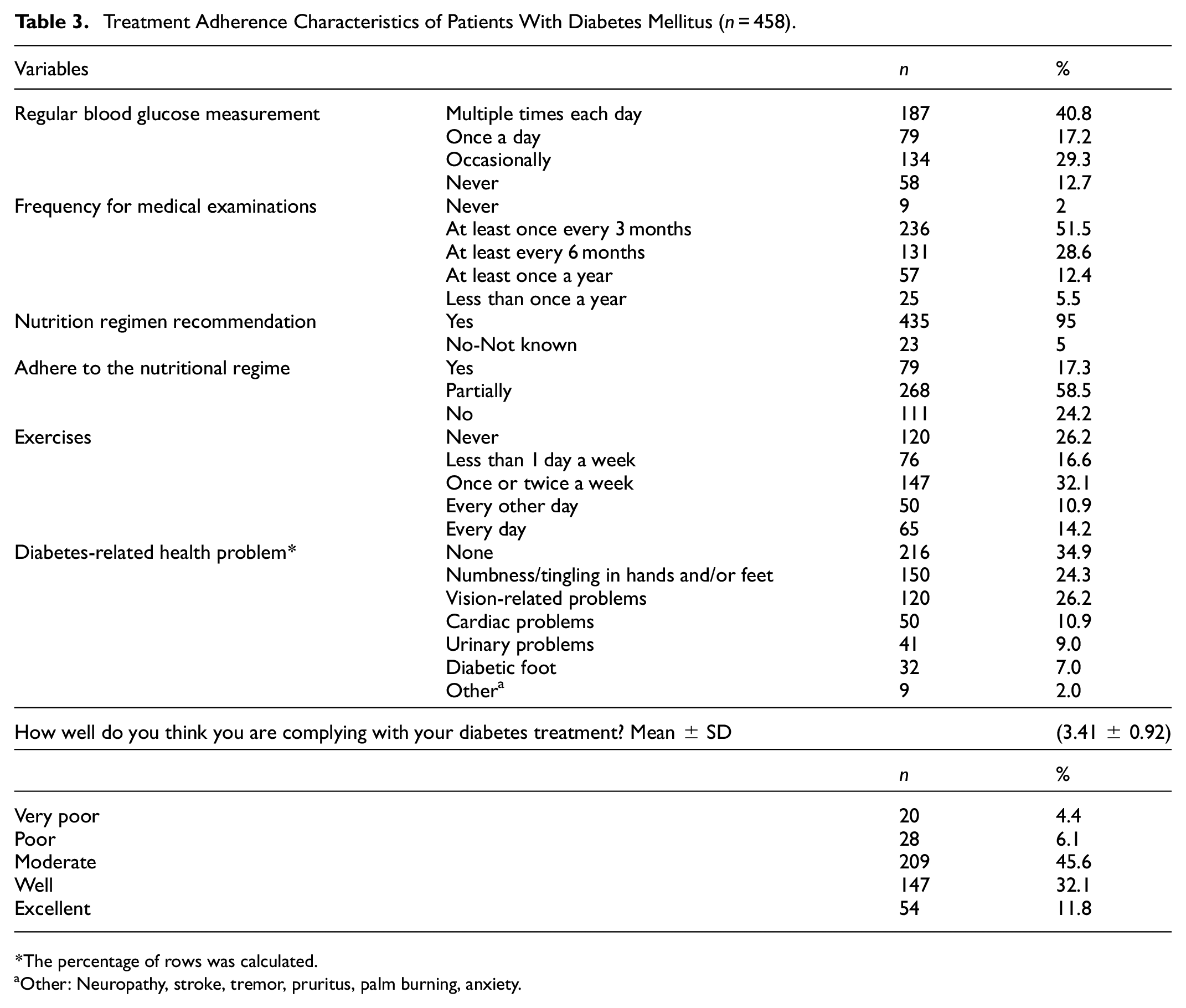
The percentage of rows was calculated.
Other: Neuropathy, stroke, tremor, pruritus, palm burning, anxiety.
Treatment Adherence Motivations and Cognitive Emotion Regulation Strategies
An analysis of the CERQ scores revealed that the most frequently employed strategies, as indicated by the range, were refocusing on planning, positive reappraisal, and putting into perspective (Table 4). More than half of the participants exhibited low motivation (52.8%) and low knowledge (48.5%) regarding treatment adherence. Among cognitive emotion regulation strategies, the most frequently used were refocus on planning (M = 11.48), positive reappraisal (M = 11.12), and putting into perspective (M = 10.13). These results support the importance of assessing individual psychological traits in treatment planning.
The Average Score of Subdimensions of TMMS and CERQ (n = 458).
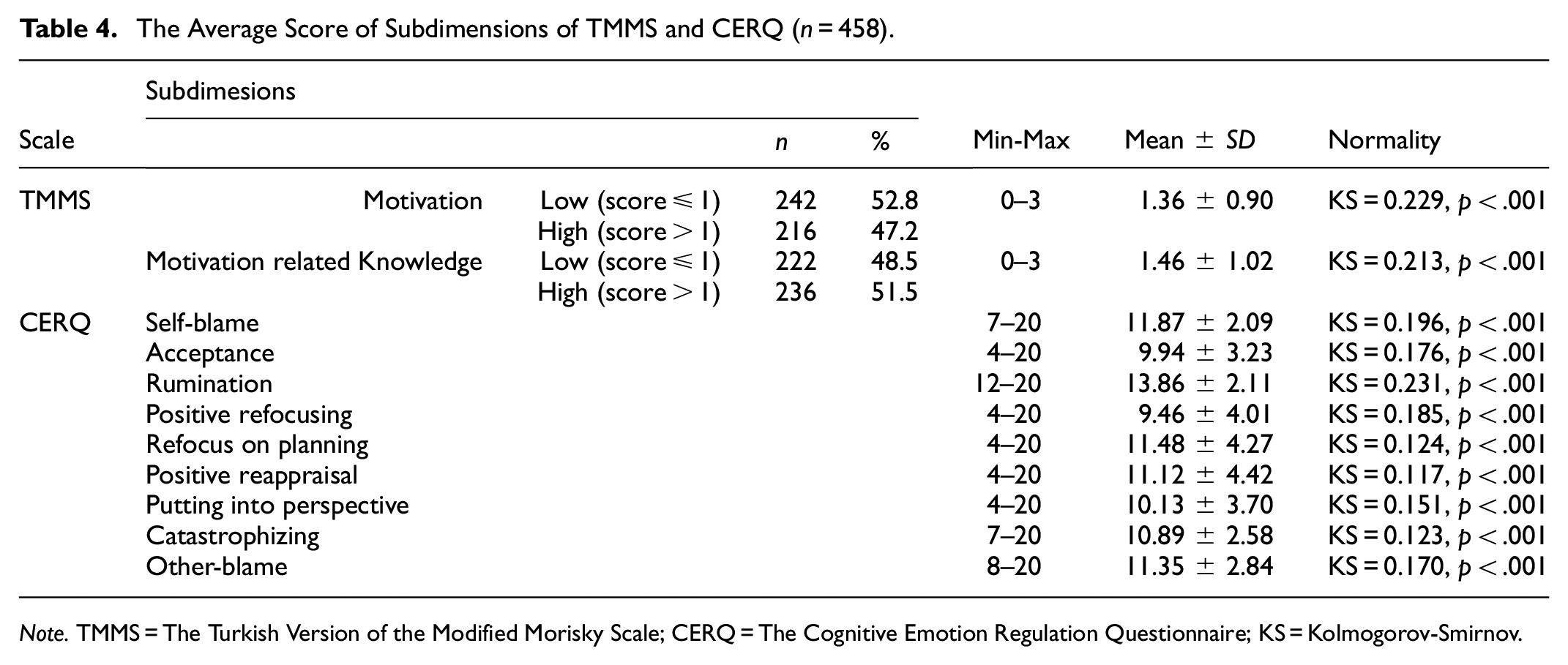
Note. TMMS = The Turkish Version of the Modified Morisky Scale; CERQ = The Cognitive Emotion Regulation Questionnaire; KS = Kolmogorov-Smirnov.
Motivations and Associated Factors for Treatment Adherence
The relationship between the subdimensions of the TMMS—namely, treatment motivation and treatment knowledge—and cognitive emotion regulation strategies (CERQ) is presented in Table 5. A positive and significant correlation was observed between treatment motivation and treatment knowledge (ρ = .201, p < .001), suggesting that patients who are more knowledgeable about their treatment are also more motivated to adhere to it.
The Correlations Between Subdimensions of TMMS and CERQ (n = 458).

Note. MMS = The Turkish Version of the Modified Morisky Scale; CERQ = The Cognitive Emotion Regulation Questionnaire; Rho = Spearman’s correlation.
Very strong.
Strong.
Moderate.
Weak.
Very weak correlation.
Hypothesis H1a, which proposed that adaptive cognitive emotion regulation strategies are positively correlated with treatment adherence motivation, was partially supported. Among the adaptive strategies, positive reappraisal showed a statistically significant positive correlation with treatment motivation (p < .05). However, other adaptive strategies (e.g., planning, acceptance, putting into perspective) did not exhibit significant relationships. Hypothesis H1b was not supported. None of the adaptive cognitive emotion regulation strategies were significantly associated with treatment adherence-related knowledge (p > .05).
Hypothesis H1c was supported. The maladaptive strategies of catastrophizing (ρ = −.101, p < .05) and other-blame (ρ = −.181, p < .001) were significantly and negatively correlated with treatment motivation, suggesting that these unhelpful cognitive patterns are associated with reduced motivation to adhere to treatment. H1d: (Maladaptive cognitive emotion regulation strategies are negatively correlated with treatment adherence-related knowledge.) was not supported. No significant correlation was found between maladaptive emotion regulation strategies and treatment adherence-related knowledge (p > .05).
Predictors of Treatment Motivation and Knowledge: Results From Logistic Regression Analyses
A binary logistic regression analysis was conducted to examine whether demographic characteristics and cognitive emotion regulation strategies significantly predicted treatment adherence motivation among patients with diabetes mellitus. The overall model was statistically significant (χ2(9) = 32.06, p < .001, Nagelkerke R2 = .0506), indicating that the predictors, as a set, reliably distinguished between individuals with low and high treatment motivation. Hypothesis H1e, stating that demographic characteristics and cognitive emotion regulation strategies significantly predict treatment adherence, was supported. The model explained approximately 5.1% of the variance in treatment motivation (Nagelkerke R2 = .051) and correctly classified a notable proportion of cases. A one-unit increase in positive reappraisal was associated with a .14 increase in the log-odds of reporting high treatment motivation, controlling for other variables in the model (Table 6);

Logistic Regression Predicting Treatment Motivation.

Note. B = unstandardized logit coefficient; SE = standard error of B; CI = confidence interval; p values are two-tailed.
Outcome variable coded as 0 = low motivation, 1 = high motivation.
To test whether treatment-related knowledge can be predicted by demographic characteristics and cognitive emotion regulation strategies, a binary logistic regression model was applied to data from patients with diabetes mellitus. The overall model was statistically significant (χ2(9) = 18.35, p < .001, Nagelkerke R2 = .058). Among the predictors, age (B = −0.025, p < .001) and education level (B = −0.433, p < .001) were found to be significant. Specifically, a 1-year increase in age was associated with a 0.025 decrease in the log-odds of reporting high treatment knowledge, while each one-unit increase in education level was associated with a 0.433 decrease in the likelihood of high knowledge, controlling for other variables. None of the cognitive emotion regulation strategies significantly predicted treatment knowledge. Thus, the H1f hypothesis was partially supported: demographic characteristics (age and education) significantly predicted treatment adherence-related knowledge, but cognitive emotion regulation strategies did not. The logistic regression model equation is (Table 7):

Logistic Regression Predicting Treatment Knowledge.
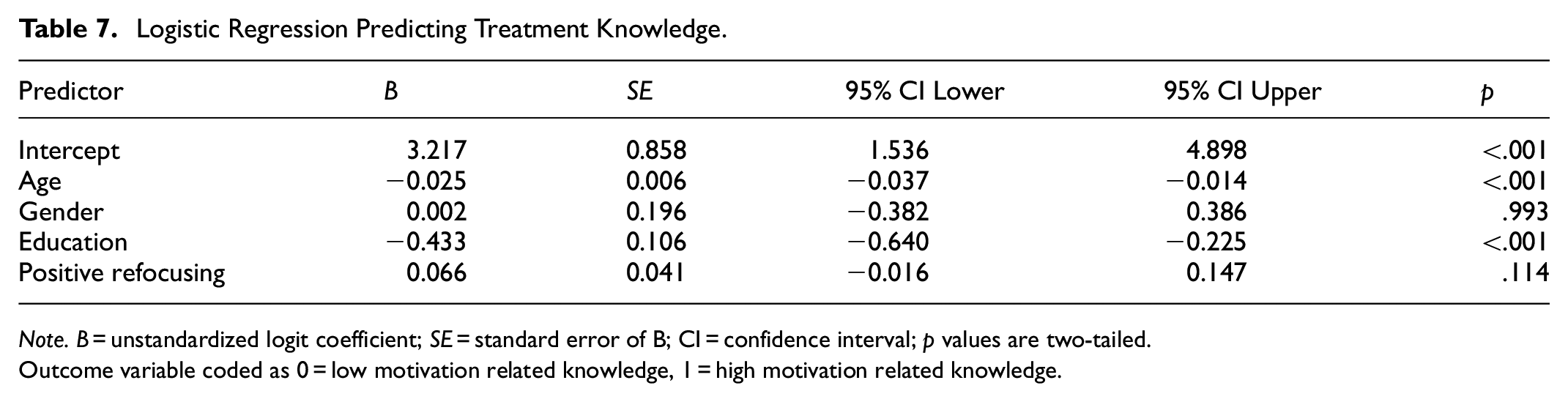
Note. B = unstandardized logit coefficient; SE = standard error of B; CI = confidence interval; p values are two-tailed.
Outcome variable coded as 0 = low motivation related knowledge, 1 = high motivation related knowledge.
Discussion
This study aimed to investigate the relationship between treatment adherence motivation, treatment-related knowledge, and cognitive emotion regulation strategies among outpatients with DM. It also explored whether demographic characteristics and emotion regulation strategies significantly predict these two outcomes. The findings, organized by hypothesis, provide insights into adherence behaviors, psychological factors, and demographic influences.
Treatment Adherence Characteristics
The study, conducted with 458 outpatients with DM, shows that approximately half of the participants (51.5%) had above-average knowledge regarding treatment adherence. Literature studies have shown that high knowledge levels positively influence treatment adherence behavior. Similarly, this research found that increased patient knowledge scores correlated with higher motivation for treatment adherence (Abdulrahman et al., 2020; Waheedi et al., 2017). However, our study also revealed that although over half of the participants had a high level of knowledge about their disease, more than half had low motivation for treatment adherence. In our participant group, knowledge level alone was not sufficient to change adherence motivation, suggesting that the ability to integrate the information one has about DM into one’s daily life may also impact adherence motivation.
Conversely, a recent study by Jamaludin et al. (2021) involving 220 individuals diagnosed with type 2 diabetes reported that 64.5% of the participants had a high level of knowledge about their disease. The authors initially hypothesized that including patients diagnosed with both type 1 and type 2 diabetes would enhance overall knowledge levels (Jamaludin et al., 2021). However, our findings indicate lower knowledge levels compared to the existing literature. This discrepancy may be attributed to the fact that type 1 diabetes patients live longer with their condition and participate in educational programs from an early age, which helps enhance their knowledge levels (Silverstein et al., 2005). The lower knowledge levels observed in our study may be due to the small sample size of patients with type 1 diabetes.
Nearly two-thirds of our participants were diagnosed with type 2 diabetes, which is often diagnosed in adulthood. This may result in reduced motivation during the adaptation process, which requires lifestyle changes. Research findings indicate that compliance with the nutritional regimen increases in diseases diagnosed at an early stage, supporting this claim (Högberg et al., 2003). Therefore, the educational roles of health professionals are particularly important. In addition to providing information about the disease and its treatment, it is crucial to equip patients with practical skills for adapting to their lives and to focus on the factors that complicate adaptation. Our study results indicate a high level of non-adherence to treatment among patients with DM. Specifically, four out of 10 patients do not regularly monitor their blood glucose, and adherence to prescribed dietary and physical exercise regimens is low. Over half of the participants had been diagnosed with and treated for DM for more than a decade, which may have contributed to reduced motivation for adherence. While the age of onset and chronic nature of DM are strong predictors of care behaviors (Jafari et al., 2024), further research is needed to confirm this claim.
Emotion Regulation Strategies and Treatment Motivation
In this study, adaptive cognitive emotion regulation strategies were examined in relation to two key outcomes: motivation for treatment adherence (H1a) and treatment-related knowledge (H1b). Among the adaptive strategies assessed, only positive reappraisal showed a statistically significant and positive correlation with treatment motivation. This finding suggests that patients who actively reinterpret challenging experiences in a constructive light are more likely to maintain motivation toward their diabetes treatment. By fostering psychological resilience, positive reappraisal may empower patients to overcome barriers to adherence, such as treatment fatigue or emotional stress, thereby supporting sustained engagement with diabetes self-management.
In contrast, other adaptive strategies—such as planning, acceptance, and putting into perspective—did not show significant associations with treatment motivation in our sample. This finding raises questions about the functional utility of these strategies in the context of chronic illness management. It is possible that the mere use of these strategies does not guarantee actual behavioral implementation, or that individual or cultural differences modulate their effectiveness. Acceptance is generally viewed as adaptive, its effectiveness may depend on age and context-specific demands (Garnefski et al., 2009). While planning may support goal-setting, it may not translate into motivation if executive function, emotional readiness, or external support is lacking—especially in populations experiencing socioeconomic constraints or healthcare fatigue (Brenner et al., 2017).
Furthermore, none of the adaptive strategies were found to be significantly correlated with treatment-related knowledge. This may suggest that emotion regulation skills influence motivational dimensions more than informational or cognitive awareness. It is also plausible that treatment-related knowledge is acquired through more structured channels (e.g., formal education, physician guidance), rather than through internal emotional processing mechanisms (Ciechanowski et al., 2001). The discrepancy between knowledge and motivation observed in this study—where many participants had adequate knowledge but low motivation—may further support this argument. It suggests that knowledge alone is insufficient to sustain adherence, and emotion regulation capacities such as positive reappraisal may play a more immediate role in activating behavioral intentions.
Maladaptive cognitive emotion regulation strategies were assessed in relation to both treatment adherence motivation (H1c) and treatment-related knowledge (H1d). Participants who frequently engaged in catastrophizing—the tendency to exaggerate the negative consequences of situations—were less likely to feel motivated to adhere to treatment plans. Similarly, those who utilized other-blame—attributing problems to external agents or people—also reported lower motivation levels. These results align with the theoretical understanding that maladaptive strategies increase emotional distress and reduce one’s sense of self-efficacy, both of which are known to diminish treatment adherence behaviors. This finding is also in line with previous research suggesting that maladaptive cognitive styles impair illness management by externalizing responsibility and reinforcing helplessness. For instance, studies have shown that patients with chronic conditions who frequently use negative cognitive regulation strategies experience greater stress and exhibit lower adherence to medical advice (Kane et al., 2018). Moreover, individuals who rely on these strategies may lack the emotional resilience necessary to engage consistently in health behaviors such as medication adherence, blood glucose monitoring, or dietary compliance. These patients might benefit from targeted psychosocial interventions that address maladaptive patterns and promote more constructive emotional coping.
By contrast, none of the maladaptive strategies—including catastrophizing and other-blame—were significantly correlated with treatment-related knowledge. This reinforces the interpretation that cognitive knowledge and emotion regulation may operate as relatively independent domains in diabetes management (Ciechanowski et al., 2001; Leventhal et al., 2020). Patients may acquire treatment-related information through healthcare providers or education but still struggle emotionally to integrate this knowledge into actionable behavior. This disconnect suggests that interventions aiming solely to increase knowledge may fail unless paired with emotion-focused strategies that help individuals manage their psychological responses to chronic illness (Schunk & DiBenedetto, 2020). Addressing these maladaptive strategies through psychoeducational or cognitive-behavioral programs may be an effective approach to enhancing treatment motivation and overall adherence.
Previous studies have highlighted the role of dysfunctional cognitive strategies such as catastrophizing and externalizing blame in diminishing treatment motivation (Bassett et al., 2019; Coccaro et al., 2022; Kane et al., 2018). Our findings reinforce these observations, showing that maladaptive strategies are significantly associated with lower motivation. In addition, cognitive reappraisal strategies like positive reframing appear to buffer the psychological burden of diabetes, supporting adherence. Elevated stress levels and burnout, particularly in patients with poor emotion regulation, may contribute to these associations (Embaye et al., 2023; Ntoumanis et al., 2021).
Implementing functional emotion regulation strategies has been shown to enhance patients’ self-confidence and expectations of success throughout the treatment process. These strategies can also help maintain motivation for health behaviors, such as treatment adherence and regular check-ups (Coccaro et al., 2022; Fall et al., 2021). The process of adjusting to a disease is associated with a sense of self-responsibility, which can be reinforced through effective emotion regulation strategies (Eales & Stewart, 2001). Our findings contribute to the existing literature on disease adaptation motivation by demonstrating that motivation increases as the use of the other-blame strategy decreases. Patients who tend to blame external factors or other people for their problems may also shift responsibility for their health conditions and treatment processes to others. This can lead to a more passive role in the treatment process. Further research into these assumptions would be beneficial. It is plausible to suggest that as the tendency to blame external factors or other individuals increases, patients may become less invested in their treatment plans and less inclined to engage in the treatment process. It is important for health professionals to support patients’ sense of self-responsibility throughout the treatment and care processes. Ensuring that patients understand the treatment and care process and encouraging them to express their feelings and thoughts about it may be crucial for fostering responsibility. Additionally, seeking support from mental health professionals to identify and address the emotional and cognitive obstacles faced by patients who are unable to actively participate in the process may increase treatment adherence.
Predictors of Treatment Motivation
Hypothesis H1e was supported: logistic regression revealed that higher education and refocus on planning were both negatively associated with treatment motivation, suggesting that critical awareness and a gap between planning and action may reduce engagement in diabetes care. In contrast, positive reappraisal was a significant positive predictor (B = 0.14, p = .010), aligning with findings that cognitive reframing promotes emotional resilience and health-related goal pursuit (Ntoumanis et al., 2021). This suggests that interpreting illness in a constructive light supports adherence behaviors.
Catastrophizing, a maladaptive strategy, significantly reduced motivation (B = −0.12, p = .005), reinforcing the idea that exaggerated negative thinking hinders self-efficacy and adherence (Coccaro et al., 2022). Studies show that functional emotion regulation strategies enhance self-confidence and expectations of treatment success (Fall et al., 2021). Effective emotional regulation has also been linked to greater personal responsibility in disease management (Eales & Stewart, 2001). Our findings extend this by showing that lower use of the other-blame strategy is associated with higher motivation. Individuals who externalize responsibility may disengage from self-care, necessitating interventions that reinforce agency and emotional support from health professionals. This supports the notion that exaggerated negative thinking can dampen a patient’s sense of efficacy, increase psychological burden, and obstruct motivation for adherence.
Hypothesis H1f was partially supported: only age and education predicted treatment-related knowledge. Younger and less-educated patients reported higher knowledge, possibly reflecting digital literacy advantages and self-evaluation tendencies among more educated individuals (Lee & Shim, 2025). Interestingly, none of the emotion regulation strategies significantly predicted knowledge, differentiating the predictors of knowledge and motivation. While motivation appears more emotion-driven, knowledge may be shaped by structural and informational factors. This underscores the need for tailored diabetes education that addresses the cognitive and informational needs of diverse groups—especially those assumed to be knowledgeable. While this may appear counterintuitive, it could be explained by greater critical awareness among more educated individuals, who may be more inclined to evaluate their knowledge more cautiously or to self-report uncertainty due to higher expectations about health literacy. This finding aligns with the interpretation that knowledge acquisition is shaped more by informational and educational access than by emotional self-regulation (Marciano et al., 2019). In practical terms, this emphasizes the importance of tailored diabetes education programs that address the informational needs of older and more highly educated patients—groups that might otherwise be assumed to have sufficient knowledge but may benefit from clearer communication and more engaging learning modalities.
The motivation to adhere to DM treatment plans may vary across different cultural contexts. For instance, a similar study conducted in Japan involving patients with type 2 diabetes diagnosed for over a decade revealed a high level of motivation to adhere to treatment regimens (Motoda et al., 2022). The emphasis on collectivism and social harmony in Japan likely encourages patients to follow prescribed treatments to avoid burdening their families and society. Additionally, the Japanese healthcare system offers comprehensive community health and home care services, which may support higher adherence levels (Özkan & Aca, 2021). In contrast, Turkish culture strongly emphasizes family support, but individual beliefs about disease and treatment can vary significantly (Bakan et al., 2017). Factors such as interpretation of disease, experience of illness, understanding of individual responsibility, and health literacy levels may influence diabetes management among Turkish patients. Adherence to treatment regimens is crucial for disease management (Fall et al., 2021). Mental health literacy has also been identified as a potential factor influencing burnout in individuals with diabetes (Jafari et al., 2024). Additionally, cultural dietary practices, which vary widely, can impact diabetes management and treatment adherence (Bakan et al., 2017). Thus, patients require interaction with the healthcare team, guidance for disease management and motivation to adhere to treatment. A culturally sensitive approach is necessary, accounting for societal perspectives on disease and treatment, religious beliefs, traditional practices, health literacy, and health policies. This comprehensive understanding can enhance patient support and treatment adherence. Additionally, the lack of association between emotion regulation and treatment knowledge highlights the need to treat knowledge and motivation as distinct yet interrelated dimensions in diabetes management. Health professionals should design interventions that simultaneously support knowledge transfer and emotional empowerment, as both are critical to improving treatment adherence outcomes (Fain, 2022).
Due to its chronic nature, DM necessitates lifelong adaptation and lifestyle modifications, leading to increased stress and a higher risk of burnout. These factors can significantly hinder disease adaptation (Crum et al., 2020). Research indicates that dysfunctional emotion regulation strategies impede adaptation in individuals with chronic diseases (Bassett et al., 2019). Effective emotional regulation is crucial for adherence to DM treatment (Embaye et al., 2023). Studies have shown a linear relationship between HbA1c levels, an important indicator of treatment adherence in DM and emotional regulation. As HbA1c levels rise, emotional regulation becomes increasingly challenging. Conversely, as emotional regulation deteriorates, HbA1c levels increase (Coccaro et al., 2022). Therefore, emotional regulation significantly influences treatment adherence and the therapeutic process in DM. Our research findings indicate that cognitive emotion regulation strategies impact the motivation to adhere to treatment regimens in individuals with DM, partially. Reduced motivation to adhere to a treatment plan for DM is associated with an increased tendency to ascribe responsibility for adverse events to external factors, such as blaming others and catastrophizing consequences. Increased stress related to diabetes is linked to the use of dysfunctional emotion regulation strategies. Studies have shown that individuals with diabetes who use negative cognitive emotion regulation strategies tend to experience higher stress levels (r = .43; Kane et al., 2018). This suggests that these individuals may have reduced motivation to adhere to treatment regimens. Our study supports this hypothesis, indicating that patients prone to catastrophizing are less likely to follow prescribed treatment plans. The increased stress from catastrophizing thoughts negatively impacts treatment motivation, hinders adherence and leads to poor self-management outcomes (Coccaro et al., 2022). Positive treatment outcomes influenced by effective emotional regulation have been shown to enhance treatment motivation (Ntoumanis et al., 2021). Elevated stress levels have been linked to disrupted eating patterns in individuals with type 1 diabetes and the cognitive reappraisal approach has been shown to mitigate stress and nutritional imbalances effectively (Embaye et al., 2023). Therefore, emotional regulation is a crucial tool for promoting treatment adherence in diabetes management.
Limitations
The sample included patients with both type 1 and type 2 diabetes mellitus. While this enhances generalizability, it also limits the ability to identify condition-specific trends, as the psychosocial and treatment dynamics differ between these subgroups.
Data collection was conducted via online tools, which may have inadvertently favored younger participants who are more familiar with digital platforms. This may have limited the representativeness of older or less digitally literate individuals and constrained the variability of age-related emotional or cognitive patterns.
The majority of participants had lived with diabetes for over a decade. As such, the sample may not adequately represent the emotional and motivational profiles of newly diagnosed patients, who may differ significantly in their treatment engagement and cognitive-emotional responses.
The Turkish Modified Morisky Scale (TMMS), used to assess treatment adherence, showed a relatively low internal consistency in this study (Cronbach’s α = .50). While the TMMS has been validated in previous research, the binary nature of its items and its brevity may have contributed to this outcome. This limitation was acknowledged in line with the reviewers’ feedback, and the scale was retained due to its widespread use, cultural adaptation, and ability to provide subscale-level insights. However, this may limit the precision of adherence measurement and should be considered when interpreting the results.
Although several statistically significant relationships were identified, both the correlational (ρ < .3) and regression analyses (Nagelkerke R2 ranging from .051 to .132) demonstrated modest effect sizes. This suggests that other unmeasured variables—such as mental health literacy, trust in healthcare, or emotional burnout—may play a role in adherence and motivation.
Conclusion
This study revealed that more than half of outpatients with diabetes mellitus had low motivation for treatment adherence, despite moderate-to-high knowledge levels. While knowledge was positively associated with motivation, the use of maladaptive emotion regulation strategies—particularly other-blame and catastrophizing—was linked to decreased motivation. These findings emphasize that knowledge alone is not enough; how patients emotionally process their illness significantly influences adherence. Integrating emotional support, culturally tailored education, and consultation-liaison mental health services into diabetes care is vital. Future research should ensure more balanced sampling across age and illness duration to deepen insights into adherence patterns.
Implications for Practice, Research, and Policy
This study’s novelty stems from its focus on a Turkish population and its unexpected findings regarding education and adherence. Health professionals should incorporate positive reappraisal techniques into diabetes education and strengthen interventions promoting blood glucose monitoring and physical activity. Further studies should examine why higher education levels predict lower motivation and knowledge—possibly involving health literacy or cultural norms. National diabetes programs should leverage Türkiye’s strong family dynamics and incorporate mental health support to reduce maladaptive emotion regulation patterns such as catastrophizing.
Supplemental Material
sj-pdf-1-sgo-10.1177_21582440251363675 – Supplemental material for Treatment Adherence and Cognitive Emotion Regulation Skills in Patients With Diabetes Mellitus
Supplemental material, sj-pdf-1-sgo-10.1177_21582440251363675 for Treatment Adherence and Cognitive Emotion Regulation Skills in Patients With Diabetes Mellitus by Gizem Beycan Ekitli, Özkan Uğuz, Emel Öztürk Turgut and Mahire Olcay Çam in SAGE Open
Footnotes
Acknowledgements
The authors thank the diabetic patients who participated in the study.
Author Note
The manuscript has been edited for English language and spelling by Enago, an editing brand of Crimson Interactive Inc.
Ethical Considerations
Research ethics approval was obtained from the İzmir Bakırçay University Ethics Committee for Non-Interventional Clinical Research.
Author Contributions
Idea/concept: GBE, ÖU, EÖT, MOÇ. Desing: GBE, ÖU, EÖT, MOÇ. Supervision: MOÇ. Data collection: OU. Analysis and interpretation: GBE. Writing: GBE, ÖU, EÖT. Critical review: MOÇ.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The research dataset has been uploaded to the journal system as a Supplemental Document.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.