
Abstract
The present study examined the psychometric properties of the Interpersonal Emotion Regulation Questionnaire (IERQ) in a Colombian sample of 726 participants. A linguistic adaptation was conducted and Evidence for internal structure, relationships with other relevant variables, and construct discrimination was gathered. The Colombian version of the IERQ demonstrated excellent to good inter-rater agreement, supporting content validity. Confirmatory factor analysis revealed excellent fit indices for a four-factor model, consistent with previous research. The four-factor model demonstrated invariance across gender, parenthood status, and mental health diagnosis. Discriminant validity was supported by significant differences between the IERQ dimensions and intrapersonal emotion regulation strategies. The instrument exhibited excellent internal consistency. Correlations with cognitive reappraisal, suppression, reward probability, and life satisfaction ranged from negligible to moderate. However, no significant correlations were found with emotional symptoms. The Interpersonal Emotion Regulation Inventory (IERQ) has proven to be a robust psychometric instrument for assessing interpersonal emotion regulation in the Colombian population.
Plain Language Summary
Emotions are not only managed individually but also through interactions with other people. For example, we might talk to a friend when we feel sad or seek advice when we are anxious. This process is known as interpersonal emotion regulation, the ways in which people use social relationships to manage their emotions.
This study evaluated the Interpersonal Emotion Regulation Questionnaire (IERQ), an instrument designed to measure how individuals regulate emotions through others, in a large Colombian sample of 726 participants. The questionnaire was translated and linguistically adapted to ensure that the items were culturally appropriate.
The results showed that the Colombian version of the IERQ works well and measures the same four key areas identified in international studies: seeking comfort, perspective-taking, social modeling, and enhancing positive emotions. The analysis confirmed that the questionnaire is valid for use across men and women, people with and without children, and those with or without a mental health diagnosis.
The IERQ also showed good reliability, meaning that its results are consistent and trustworthy. It was moderately related to other ways of managing emotions, such as cognitive reappraisal and expressive suppression, as well as to life satisfaction and experiences of reward in everyday life.
Overall, this study demonstrates that the IERQ is a reliable and useful tool for understanding how people use their relationships to manage emotions in Colombia. It can be applied in research, mental health settings, and community programs to better understand emotional well-being and social support processes.
Keywords
Introduction
In clinical psychology, emotional regulation (ER) is a fundamental topic of study, and its definition has evolved over time. Initially, it was understood as the process of influencing which emotion one feels, when it occurs, how it is expressed, and how it is experienced (Gross, 1998). It has also been defined as the set of goal-oriented processes that influence an emotional state’s trajectory, change, and continuity (Gross, 2015; Sheppes et al., 2011), whether one’s own or another’s (McRae & Gross, 2020). More recently, it has been investigated through various empirically supported approaches and perspectives (De los Santos, 2022).
Evidence-based psychology has proposed examining the transdiagnostic processes that influence and explain psychological difficulties (Bullis et al., 2019; Frank & Davidson, 2014). In this sense, emotion regulation (ER), understood as a transdiagnostic process, is directly or indirectly associated with all psychopathologies or problems of clinical interest (Coenye et al., 2022), such as mood disorders, depression, insomnia (Horato et al., 2022; Predatu et al., 2020), anxiety (Agako et al., 2021), social anxiety (Aldao et al., 2014), personality disorders (Salgó, Salgó, Bajzát, & Unoka, 2021; Salgó, Szeghalmi, et al., 2021), eating disorders (Khosravi, 2020; Naumann & Svaldi, 2021), dissociative disorders (Nester et al., 2022), among others. In turn, ER is interrelated with other transdiagnostic processes such as avoidance, behavioral activation, repetitive negative thinking (González et al., 2017), worry, and rumination (Vizioli, 2022). Therefore, studying ER is not only theoretically relevant but also central for understanding risk and maintenance factors across a wide range of mental health problems.
Traditionally, research on ER has focused on its intrapersonal aspects, especially those related to suppression and reappraisal (Sánchez-Teruel & Robles-Bello, 2018). However, this process involves covert repertoires and more observable strategies such as seeking advice from others (Aldao et al., 2010), giving rise to the social characteristic of ER: the interpersonal aspect. Also understood as a process, Interpersonal Emotion Regulation (IER) is relevant both in basic research and in clinical evaluation and practice (Fernández-Álvarez et al., 2018).
Within ER, it could be stated that strategies are divided into two broad categories: intrinsic (intrapersonal) strategies and extrinsic (interpersonal) strategies; both associated with psychopathology (Sheppes et al., 2015). Research in this field has focused more on intrinsic (intrapersonal) ER strategies, that is, those for changing one’s emotions without the need for another, ignoring the use of extrinsic (interpersonal) strategies. Despite their importance in interpersonal relationships, only a few studies have examined this part of the process (Altan-Atalay & Saritas-Atalar, 2019). From this perspective, IER represents a core interpersonal process through which people seek support, co-regulate emotions with others, and maintain or repair social bonds, making its valid assessment crucial for understanding social functioning and adjustment.
Extrinsic or IER strategies aim to socially modify one’s own emotions through others, as well as to influence the course and emotional experience of others (Hofmann et al., 2016). These have attracted the interest of researchers relatively recently (Nozaki & Mikolajczak, 2020). Based on what Hofmann and Doan (2018) have stated, as the process of social development occurs, emotions need to be understood, experienced, and regulated according to the specific needs of each stage of the life cycle. This is achieved with the help of a person other than the individual, who facilitates the modification of the emotional process that is being experienced. Therefore, the current social context ends up being essential when it comes to understanding one’s own emotions and generating an adaptive response (Hofmann & Doan, 2018). For this reason, it is relevant to delve deeper into IER strategies since, in addition to involving people different from the individual (Barthel et al., 2018), human beings, being gregarious and experiencing an affective state, normally choose to do so in the company of another who helps them make sense of their affective response (Zaki & Williams, 2013). Additionally, it is relevant in clinical practice, since it has been found that rigid IER is associated with the presence of signs and symptoms indicative of psychopathology (Aldao & Dixon-Gordon, 2014; Hayes & Hofmann, 2018). Consequently, valid measures of IER are needed not only for basic research but also to inform relational, family, and group-based interventions that target how people seek and provide emotional support in real-life contexts.
Now, IER is understood as a process that has some characteristics that differentiate it from other processes underlying ER, such as: 1) It is a regulatory process through which one seeks to modify or continue an emotional state and is driven by a “motive” (prosocial, work-related). 2) It seeks to alter the affective channel over cognitive and behavioral change. 3) It is deliberate and intentional: the person who uses IER strategies is aware and invests a large amount of personal resources for this purpose. And 4) its implementation has a social objective that facilitates and improves interpersonal relationships (Niven, 2017). Additionally, IER is associated with variables such as attachment, reinforcement sensitivity (Altan-Atalay, 2019), attachment styles (Gökdağ, 2021; Grisham et al., 2018), and empathy (Zaki, 2020).
Hofmann et al. (2016) designed a tool that measures the interpersonal aspects of emotion regulation: the Interpersonal Emotion Regulation Questionnaire (IERQ). Its original version was designed in the United States, is composed of 20 items that evaluate 4 factors, each in turn composed of five items with good internal consistency: Enhancing Positive Affect (α = .89), Perspective Taking (α = .91), Soothing (α = .94), and Social Modeling (α = .93) (Hofmann et al., 2016).
The IERQ has been validated in several countries, such as: Germany (Pruessner et al., 2019), Iran (Abasi et al., 2021), Turkey (Koç et al., 2019), India (Kanth & Indumathy, 2022), and Italy (Messina et al., 2022). Sample sizes in these adaptations ranged from 302 participants in Turkey to 729 in Germany. In relation to the reliability of the IERQ dimensions, the study in Germany and Italy presented Cronbach’s Alpha internal consistency coefficients ≥0.80. However, with a Turkish population, the Improving Positive Affect and Perspective Taking dimensions showed indices between questionable and acceptable (<0.60 and <0.80, respectively). Only the study in Germany reports good test-retest reliability (≥.72). All the studies referred to confirm the four-factor structure proposed by the creators of the questionnaire (Hofmann et al., 2016). The studies in India, Italy, and Turkey present fit indices between fair and adequate (CFI > 0.90 and RMSEA < 0.08) and those in Germany and Iran reported good fit indices (CFI > 0.95 and RMSEA < 0.05).
For evaluations and interventions to be more precise and effective, it is necessary to have instruments that allow for the reliable assessment of this process. In Colombia, there are two validated instruments for measuring ER. The first is the Difficulties in Emotion Regulation Scale (DERS) designed by Gratz and Roemer (2004) and validated by Muñoz-Martínez et al. (2016). The second instrument validated in the country is the Emotion Regulation Questionnaire (ERQ) designed by Gross and John (2003) and validated in Colombia by Canales et al. (2024), which has good psychometric properties. Both instruments, however, focus primarily on intrapersonal emotion regulation (e.g., understanding, accepting, and managing one’s own emotions, cognitive reappraisal, and expressive suppression) and do not explicitly assess how people use others to regulate their emotions or how they attempt to influence others’ emotional states.
Within the Colombian context, no scientific literature was found specifically associated with Interpersonal Emotion Regulation (IER) that encompasses the social aspect of interaction and the effect of these interactions on one’s own and others’ emotions. Since Colombia is a multicultural and ethnically diverse country (Chaves et al., 2022), it is relevant to have an instrument that can identify, within social and individual practices, whether these strategies are related to mental health problems and afflictions, and at the same time complement interventions that focus on the regulation and management of problems, not only from an individual perspective, but also from a social and contextual aspect. In this sense, the IERQ fills an important gap by providing a brief, theory-based measure of interpersonal (extrinsic) emotion regulation strategies, allowing researchers and clinicians to capture co-regulation processes that are not covered by existing ER measures in Colombia.
The present study aimed to gather validity and reliability evidence for the Interpersonal Emotion Regulation Questionnaire (IERQ) in a Colombian sample, following the Standards for Educational and Psychological Testing of the American Educational Research Association, American Psychological Association, and National Council on Measurement in Education (American Educational Research Association et al., 2014). First, we conducted the linguistic adaptation and content evaluation of the questionnaire through expert-judge review. Second, we conducted a clarity (face validity) test using a small sample. Third, we examined psychometric properties of the IERQ by: (a) confirming its original four-factor internal structure; (b) testing measurement invariance across gender, parenthood status, and mental health diagnosis; (c) assessing discriminant construct validity among the IERQ dimensions; and (d) analyzing relations with other variables, including intrapersonal emotion regulation strategies (Emotion Regulation Questionnaire, ERQ), emotional symptomatology (Depression, Anxiety, and Stress Scales, DASS-21), response-contingent positive reinforcement (Reward Probability Index, RPI), and life satisfaction (Satisfaction with Life Scale, SWLS). Additionally, internal consistency indices (Cronbach’s α and McDonald’s ω) were computed to assess the IERQ’s reliability. Given the foregoing, this research corresponds to an instrumental quantitative study (Reivan-Ortiz et al., 2022; Salas-Picón & Avendaño-Prieto, 2021).
Method
Participants
Participants in this instrumental study were drawn from three sources corresponding to the main phases of the validation process: (a) expert judges for content validity, (b) a pilot sample for the clarity (face validity) test, and (c) a community sample for the examination of the internal structure, measurement invariance, reliability, and relations with other variables.
Content Validity (Expert Judges)
Six expert judges participated in the item content evaluation. Three judges held master’s degrees, and three had doctoral degrees. Professional experience ranged from 10 to 18 years, while experience in clinical supervision ranged from 6 to 13 years. In terms of specialized areas, 5 judges had experience with child populations, 5 with adolescents, 5 with adult care, and 2 with couples therapy. All 6 judges had experience in research.
Clarity/Face Validity
For the clarity evaluation, a sample of 20 adult participants from Bogotá D.C. was recruited, consisting of 10 males and 10 females, with an age range between 21 and 35 years. The majority of participants (14) were professionals in the social sciences. All participants completed an online form to evaluate the clarity of the items from the adapted version of the IERQ.
Main Validation Sample
Through a non-probability convenience sampling, 726 Colombian adults over the age of 18 consented and completed the Microsoft form. The sample included 79.6% (n = 570) women and 20.3% (n = 146) men, with ages ranging from 18 to 64 years (M = 37, SD = 14.3). Of the sample, 54.1% (n = 388) reported being single, 19.8% (n = 142) married, 18.4% (n = 132) in a common-law union, 4.8% (n = 35) divorced, and 2.6% (n = 19) in other relationship statuses. In education levels, the majority reported having a university degree (37.8%) or a postgraduate degree (37.1%), followed by a technical degree (15.8%) and a high school diploma (8.7%). As for occupation, 70.2% reported being employed, followed by 14.9% unemployed, 9% students, and 5.6% others. The socioeconomic level was reported as low for 30.7% (n = 221), middle for 44.2% (n = 317), and high for 24.7% (n = 178). Additionally, 316 (44.1%) participants reported having children.
Regarding mental health, 38.5% reported having received some treatment in mental health settings. At the time of the survey, 206 participants reported being prescribed psychotropic medications. Finally, 185 (25.8%) reported a mental health diagnosis.
Instruments
Emotion Regulation Questionnaire (ERQ)
The ERQ (Gross & John, 2003) assessed individual differences in emotion regulation strategies, specifically suppression and cognitive reappraisal. The Colombian validation (Canales et al., 2024) consisted of 10 items with a 7-point Likert scale (1 = Totally disagree; 7 = Totally agree). Both dimensions demonstrated acceptable reliability (α = .77 for suppression and α = .76 for reappraisal). The two-factor model showed good fit indices (RMSEA = 0.058; SRMR = 0.061; CFI = 0.96) (Canales et al., 2024).
Depression, Anxiety, and Stress Scales (DASS-21)
The DASS-21 (Antony et al., 1998) was employed to measure symptoms of depression, anxiety, and stress. The Colombian validation (Ruiz et al., 2017) included 21 items with a 4-point Likert scale (0 = Did not occur at all; 3 = Occurred very much, or most of the time). The Colombian validation reported a three-factor structure with an additional second-order factor, showing excellent fit indices (RMSEA = 0.049, CFI = 0.99, NNFI = 0.99) and excellent internal consistency for the total scale (α = .93) and its dimensions: depression (α = .87), anxiety (α = .84), and stress (α = .81) Ruiz et al. (2017).
Reward Probability Index (RPI)
The RPI (Carvalho et al., 2011) aimed to measure the magnitude of environmental reward, an indirect measure of response-contingent positive reinforcement (RCPR), through the dimensions of reward probability and environmental suppressors. The Colombian validation (Reyes-Buitrago et al., 2023) comprised 20 items with a 4-point Likert scale (1 = Strongly disagree; 4 = Strongly agree). Both dimensions, reward probability and environmental suppressors, showed high reliability (ω and α > .85). The two-factor model presented good fit indices (RMSEA = 0.059, NNFI = 0.971, CFI = 0.977, GFI = 0.978) (Reyes-Buitrago et al., 2023).
Satisfaction With Life Scale (SWLS)
The SWLS (Diener et al., 1985) was used to measure global life satisfaction. In the Colombian validation (Ruiz et al., 2019) the internal consistency (α = .89) was good. The fit indices for the one-factor model showed a good fit in the Colombian sample (RMSEA = 0.052; CFI = 0.99; NNFI = 0.99) (Ruiz et al., 2019).
Sociodemographic Survey
An ad hoc sociodemographic survey was developed to collect information on age, sex, marital status, occupation, education level, and city of residence.
Procedure
The present instrumental study was conducted in four distinct phases, corresponding to the main sources of validity and reliability evidence described in the Introduction.
Phase 1: Translation and Adaptation
The initial stage of the study included obtaining permission from the original author of the IERQ. The translation of the IERQ items into Spanish was performed based on the original English version, and this translation was then subjected to a back-translation into English to ensure conceptual equivalence. Particular attention was paid to the translation of emotionally dense terms such as “upset,” which in English can cover a broad range of affective states. For these items, alternative Spanish renderings were discussed, and the Italian and German versions of the scale were consulted to guide decisions and preserve the intended emotional nuance.
Phase 2: Expert Review and Clarity Evidence
Six expert judges, specializing in clinical psychology and psychometrics, evaluated the Spanish translation of each item in terms of pertinence, coherence, relevance, semantics and syntax, and sufficiency, as well as the sufficiency of items within each dimension. Inter-rater agreement was assessed using the Kappa statistic, leading to final linguistic adjustments. Items that did not meet the expert judges’ criteria were revised using input from the Italian and German versions and then rephrased to be natural and culturally appropriate in Colombian Spanish. Subsequently, evidence of item clarity was obtained through direct ratings of comprehensibility and wording adequacy from 20 adult participants, who completed an online form focused exclusively on the clarity of the adapted IERQ items.
Phase 3: Online Questionnaire Administration
The questionnaire, including informed consent, sociodemographic questions, the IERQ, and the additional measures, was developed using ® Microsoft Forms. Participants were recruited and the questionnaire was administered via social media platforms (Facebook, Instagram, WhatsApp).
Phase 4: Data Analysis and Feedback
Data analysis focused on evaluating the psychometric properties of the Spanish version and conducting confirmatory factor analysis to validate the proposed four-factor structure. Upon completion, individual results were shared with participants who requested them, alongside information about national mental health resources.
Data Analysis Plan
Descriptive statistics (frequency, central tendency, and dispersion) were used to characterize the sample.
To assess the linguistic adaptation and content validity of the instrument, expert judges evaluated the adapted version. Cohen’s Kappa (Randolph, 2005) was used to measure inter-rater agreement, with values below .40 indicating poor agreement, .40 to .75 indicating fair to good agreement, and above .75 indicating excellent agreement. Items with median ratings below 4 and means below 3.5 were considered for modification.
Following Lim’s (2024) taxonomy, evidence of face validity was gathered. To ensure that the items appeared to measure what they were intended to measure, 20 potential participants from the target population conducted a subjective evaluation. The kappa coefficient was calculated using the previously described criteria.
To assess the construct validity of the IERQ, a confirmatory factor analysis (CFA) was conducted. Given that the original study identified four factors, and these findings have been replicated in subsequent research, the goodness-of-fit of the proposed models was evaluated. The following fit indices were used to assess model fit: Bentler Comparative Fit Index (CFI), Tucker Lewis Index (TLI), Normed Fit Index (NFI), Incremental Fit Index (IFI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Cut-off values considered indicative of acceptable model fit were as follows: RMSEA < 0.05, CFI ≥ 0.95, NFI, NNFI, IFI, and AGFI > 0.90, and SRMR < 0.05 (Kline, 2023).
Multi-group CFAs were conducted to test configural, metric, scalar, and strict factorial invariance across groups defined by sex (men vs. women), parenthood status (with vs. without children), and self-reported mental health diagnosis (yes vs. no), using the criteria suggested by Lippke et al. (2007; ΔTLI < 0.050), Putnick and Bornstein (2016; ΔSRMR < 0.015), and Cheung and Rensvold (2002; ΔCFI < 0.010 and ΔRMSEA < 0.015).
The heterotrait-monotrait ratio of correlations (HTMT; Henseler et al., 2015) was calculated to assess the discriminant validity of the IERQ subscales. Values below 0.90 indicate evidence of discriminant validity (Lim, 2024). Additionally, this same index was used to account for discriminant validity with cognitive emotion regulation strategies.
Cronbach’s alpha (α) and McDonald’s omega (ω) were calculated to assess the internal consistency of the scale. Item-total and item-subscale correlations were also examined. Values of α and ω below .70 were considered questionable, while values above .70 were considered adequate (Frías-Navarro, 2022).
Pearson correlation coefficients were calculated to examine the relationship between the IERQ and other relevant constructs. Effect sizes were interpreted using the guidelines proposed by Goss-Sampson and Meneses (2019): a correlation coefficient less than .10 indicates a negligible relationship, between .10 and .29 indicates a small relationship, between .30 and .49 indicates a moderate relationship, and .50 or greater indicates a large relationship (Goss-Sampson & Meneses, 2019).
The Online Kappa Calculator (Randolph, 2008) was used to analyze inter-rater agreement among expert judges on their ratings of each IERQ item in terms of pertinence, coherence, relevance, semantics and syntax, and sufficiency, as well as the sufficiency of items within each dimension, and JASP (version 0.18.0; JASP Team, 2022) was used for internal consistency indices (Cronbach’s α and McDonald’s ω), confirmatory factor analyses and measurement invariance models, and correlation analyses between the IERQ and external variables.
Results
Adaptation and Content Validity Evidence
Table 1 presents the inter-rater agreement indices resulting from the expert judges’ review of the items, based on the criteria of relevance, coherence, clarity, semantics/syntax, and sufficiency. The agreement values for the categories of relevance (
Kappa Indices and Inter-Rater Agreement Percentages.

Comparisons of means (M) and medians (m) of judges’ ratings for each item/dimension indicated high scores on Pertinence, Relevance, Coherence, and Sufficiency. The Syntax and Semantics category showed the greatest variability in ratings. Items with medians below 4 and means below 3.5 (items 2, 5, 7, 9, and 10) were reviewed to improve their linguistic adaptation to the Colombian population.
Face Validity (Clarity) Evidence
Subsequently, evidence of face validity was gathered from 20 adult participants to assess the clarity of each statement. This category showed a high percentage of agreement regarding item clarity (overall agreement = 80.35%) and a moderate to good agreement index (Kfree = 0.61), indicating that participants converged in rating the adapted IERQ items as clear and understandable and providing additional support for the linguistic adequacy of the Colombian version before the main validation phase. The final Colombian Spanish version of the IERQ used in this study is provided in the Appendix.
Evidence of Construct Validity
Confirmatory Factor Analysis
To gather evidence of the internal structure validity of the IERQ, a CFA was conducted with three models (Table 2): a one-factor model (1F), a four-factor model according to the original proposal (Hofmann et al., 2016), and a four-factor plus one second-order model (4F+SO). The four-factor model identified in different related studies (Abasi et al., 2021; Kanth & Indumathy, 2022; Koç et al., 2019; Messina et al., 2022; Pruessner et al., 2019) was confirmed. The 4F model showed excellent comparative fit indices (CFI and TLI), incremental fit indices (NFI and IFI), and absolute fit indices (SRMR and RMSEA). Additionally, the 4F model presented an adequate parsimony index (PNFI > 0.800). The four-factor plus one second-order model also showed excellent fit indices, however, the values were slightly lower in all indices except for parsimony (PNFI > 1). Given the results obtained, the 4F model was chosen.
Goodness-of-Fit Indices of the Tested Models.

Note. Bold values indicate the model with the best overall fit across the reported fit indices.
Figure 1 displays the standardized factor loadings for the four-factor model. All items showed acceptable standardized factor loadings; item 1 presented the lowest loading (λ = .47) but remained above the commonly used .40 cutoff in CFA and was therefore retained based on both statistical and theoretical considerations.
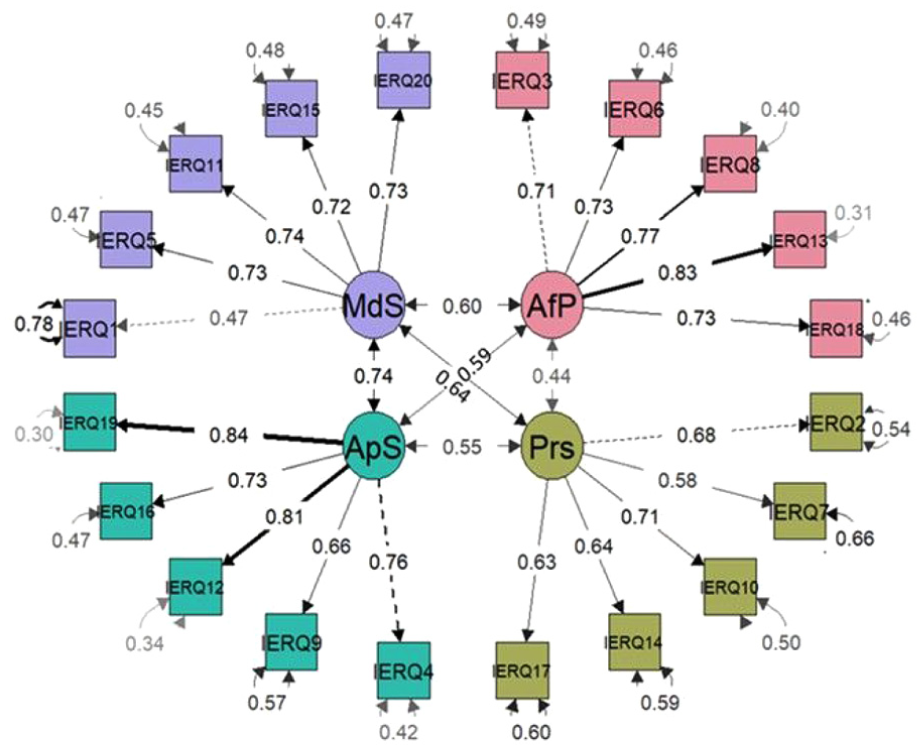
Standardized factor loadings for the four-factor IERQ model.
Factorial Invariance
Factorial invariance was found across sex, parenthood status, and mental health diagnosis across all four levels of invariance tested. Invariance was found for the factor structure (configural), factor loadings (metric), intercepts (scalar), and unique variances (strict), indicating that these parameters were equivalent for men and women, parents and non-parents, and individuals with and without a mental health diagnosis (Table 3).
Comparison of Fit Indices for Assessing Factorial Invariance of the 4F IERQ Model Across Sex, Parenthood Status, and Mental Health Diagnosis.

Discriminant Validity of the IERQ Factors
Regarding evidence of discriminant validity, Table 4 presents the HTMT values among the IERQ subscales. The subscales showed satisfactory discriminant validity when applying the strictest threshold recommended by Henseler et al. (2015) of 0.85. The HTMT values among the subscales can be observed in Table 4.
HTMT Values of IERQ Factors.

Note. EPS = enhancing positive affect; PT = perspective taking; So = soothing; SM = social modeling.
Internal Consistency and Item Discrimination
The IERQ demonstrated excellent internal consistency, as indicated by McDonald’s omega (ω = .91, 95% CI [0.91, 0.92]) and Cronbach’s alpha (α = .91, [0.90, 0.92]). The four dimensions of the IERQ also showed good internal consistency, with omega values ranging from .79 to .89 and alpha values ranging from .79 to .87 (see Table 5). Item-factor correlations exceeded .50, indicating good item discrimination, except for item 1 with a discrimination index of 0.38, which was adequate.
Internal Consistency and Item Discrimination of the IERQ.

Note. EPS = enhancing positive affect; PT = perspective taking; So = soothing; SM = social modeling; D.I. = discrimination index.
An item analysis was conducted to assess their contribution to the scale’s internal consistency. However, no items were removed, as their removal did not significantly improve the internal consistency estimates above the upper limit of the confidence interval.
Evidence of Validity of the Relationship With Other Constructs
Pearson correlation analyses were employed to investigate the relationships between the Interpersonal Emotion Regulation Questionnaire (IERQ) and its four constituent dimensions (Enhancement Positive Affect, Perspective Taking, Soothing, and Social Modeling). Specifically, we examined the correlations between the IERQ and the following constructs: Emotion Regulation (ERQ), as measured by its suppression and reappraisal subscales; Emotional Symptoms, as assessed by the Depression, Anxiety, and Stress Scale (DASS-21); Response Contingent Positive Reinforcement (RCPR), including its reward probability and environmental suppressors subscales; and Life Satisfaction, as measured by the Satisfaction with Life Scale (SWLS).
As shown in Table 6, correlations between the IERQ dimensions and the ERQ suppression subscale were small in magnitude and mixed in direction. One dimension showed a small positive association with suppression, another a small negative association, and the remaining correlations were negligible and non-significant. In contrast, the ERQ reappraisal subscale displayed a clearer pattern, with small to moderate negative correlations for most IERQ dimensions, and the strongest (moderate) association observed for the soothing dimension.
Pearson Correlations of IERQ Dimensions With Each Other and Other Variables.
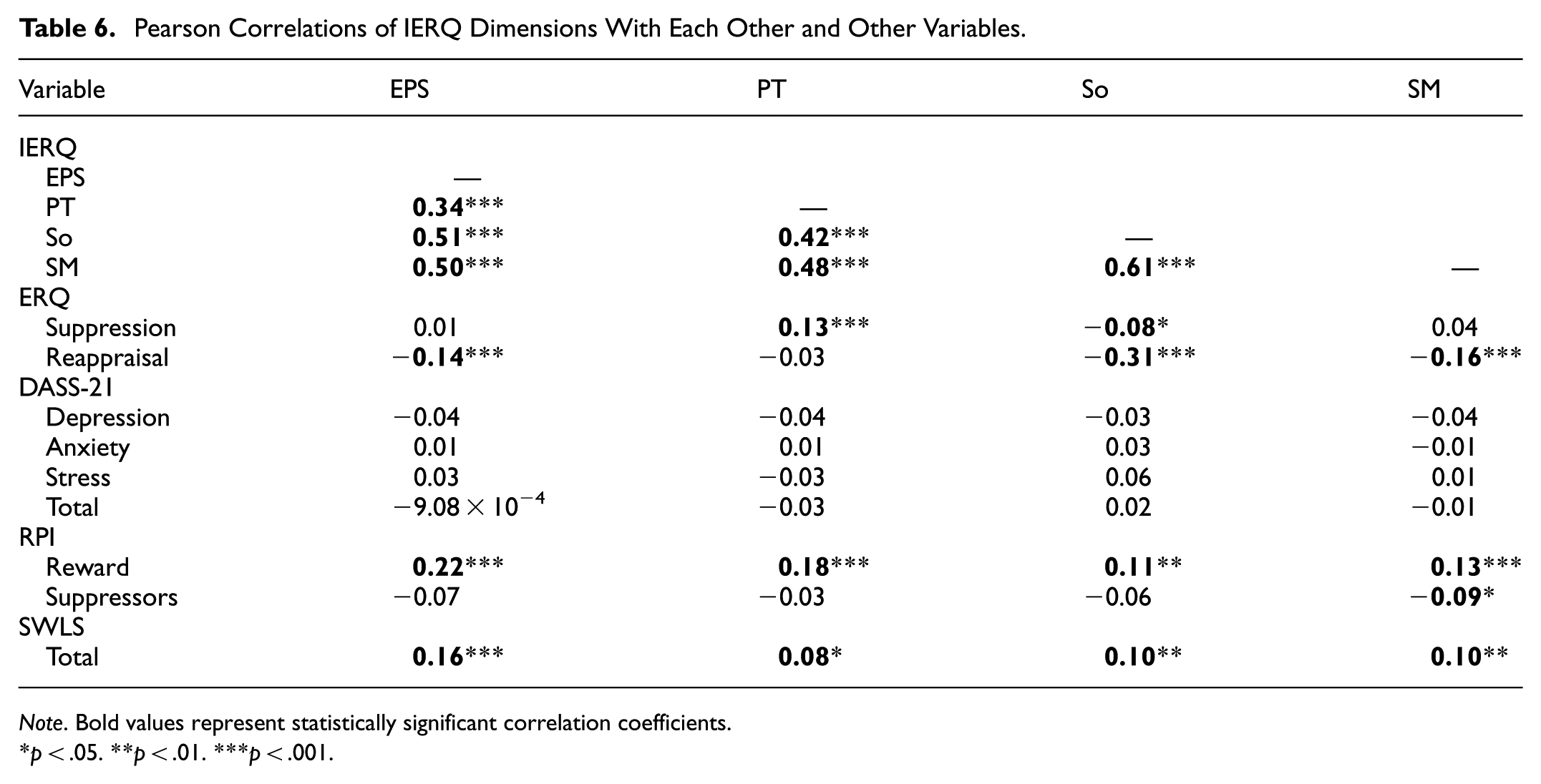
Note. Bold values represent statistically significant correlation coefficients.
p < .05. **p < .01. ***p < .001.
Correlations between the IERQ and specific and general emotional symptoms (DASS-21 and its subscales) were nonsignificant and negligible. Conversely, reward probability demonstrated significant positive correlations (p < .01) with all four IERQ factors, although these correlations were of a small magnitude. Environmental suppressors, on the other hand, exhibited negligible correlations with the IERQ dimensions. Lastly, life satisfaction (SWLS) showed significant correlations, ranging from negligible to small, with the IERQ dimensions (Table 6).
Discriminant Validity of the Construct With Respect to Cognitive Reappraisal and Suppression
To assess the discriminant validity of the IERQ dimensions in relation to the cognitive emotion regulation strategies of reappraisal and suppression, the heterotrait-monotrait ratio of correlations (HTMT) was calculated. The results, presented in Table 7, support the discriminant validity of the IERQ subscales from the ERQ subscales, as all HTMT values fell below the recommended threshold of 0.85 suggested by Henseler et al. (2015).
Monotrait and Heterotrairt Ratio of IERQ Subscales With ERQ.

Note. EPS = enhancing positive affect; PT = perspective taking; So = soothing; SM = social modeling.
Discussion
This instrumental study investigated the psychometric properties of the Spanish adaptation of the IERQ in a sample of 726 Colombian adults, integrating three complementary phases: expert-judge content review and linguistic adaptation, a clarity evaluation with adult participants, and a main psychometric validation phase. The four-factor model originally proposed was confirmed in the main validation sample. Moreover, measurement invariance was demonstrated across sociodemographic, social interaction, and clinical interest variables. Nonetheless, some findings diverged from those reported in previous validation studies.
Regarding linguistic adaptation and content validity, the Colombian version of the IERQ showed adequate indices and agreement percentages among expert judges. The criteria of pertinence, coherence, semantics/syntax, and sufficiency showed intermediate-to-excellent consistency indices, and items 2, 5, 7, 9, and 10 were modified based on the judges’ suggestions. The final version with the modified items presented an intermediate-to-good consistency index (α = .61, 80.35%) for the clarity criterion, as determined by the clarity study. Both the expert judgment and the clarity test provide evidence of content validity for the Colombian adaptation of the IERQ. At the same time, the adaptation process highlighted the challenges of translating affective terms such as “upset” across languages and regional varieties of Spanish, in line with prior work on lexicosemantic diversity in the emotional domain (e.g., Bourdin, 2015; Díaz et al., 2022; Zapata-Orozco et al., 2020). These considerations are particularly relevant in a culturally and linguistically diverse context such as Colombia and underscore the importance of combining statistical evidence with careful linguistic and cultural review when adapting emotion-related measures.
Regarding evidence of internal structure validity, confirmatory factor analysis (CFA) corroborated the four-factor model (original model) with excellent fit indices, similar to those reported in the original study (Hofmann et al., 2016) and subsequent studies by Pruessner et al. (2019), Abasi et al. (2021), Koç et al. (2019), Kanth and Indumathy (2022), and Messina et al. (2022). When testing the second-order factor, excellent fit indices were also found, although they did not match those of the four-factor model. Standardized factor loadings of each item with its dimension were greater than 0.46.
Regarding the measurement invariance of the IERQ, the hierarchical invariance model sequence showed that the original four-factor model fit the data in all restrictive models across the different groups compared. The IERQ was found to be invariant, allowing for comparisons between groups. Specifically, the four-factor model showed invariance in relation to gender (men vs. women), parenthood status (participants with and without children), and mental health diagnosis (having vs. not having received a mental health diagnosis).
Therefore, at the configural and metric invariance levels, these results suggest that, according to each criterion, interpersonal emotion regulation tends to be conceptualized similarly and the same meaning is attributed to the latent constructs (Van de Schoot et al., 2012). Similarly, intercepts and residuals are the same across groups, given the results at the scalar and residual levels (Putnick & Bornstein, 2016). The relevance of this evidence lies in the fact that it will allow for more reliable comparisons between these subgroups, thus avoiding method bias when making comparisons (Putnick & Bosrnstein, 2016; van de Schoot et al., 2012). Including parenthood status as a grouping variable is particularly pertinent because having children represents a central interpersonal and caregiving role that is closely tied to everyday emotion regulation in social contexts; showing that the IERQ is invariant in parents and non-parents therefore supports its use in comparing interpersonal emotion regulation processes across these relational contexts. Considering that the social and cultural aspect is closely linked to the gregarious character and this, in turn, to IER (Kappas, 2013), the factorial invariance found in the demographic and related contextual aspects constitutes a relevant contribution. Regarding the finding of invariance between those who reported having a mental health diagnosis and those who did not, its relevance is evident given the recent/growing field of study of IER and mental health indicators (Akkuş et al., 2025).
Another contribution of this research was the analysis of the IERQ’s discriminant validity. Evidence of discriminant validity was found for the IERQ subscales, meeting the stricter criterion (0.85) suggested by Henseler et al. (2015) for HTMT values. However, for related constructs like the IERQ dimensions, a threshold of 0.90 is recommended (Lim, 2024). Furthermore, HTMT values were calculated between the IERQ factors and the ERQ factors (reappraisal and cognitive suppression). The HTMT values were <0.85, indicating evidence of discriminant validity within the IERQ factors and ERQ factors. These findings suggest that the items within each IERQ dimension measure distinct aspects of interpersonal emotion regulation. Future studies should replicate these results, as there is a lack of previous research examining this aspect of the IERQ’s validity. This study is the first to evaluate the discriminant construct validity of the IERQ.
Regarding the IERQ’s reliability, internal consistency, and item discrimination, the results showed excellent psychometric properties (George & Mallery, 2019). McDonald’s omega (ω = .914, 95% CI [0.905, 0.923]) and Cronbach’s alpha (α = .913, [0.904, 0.922]) indicated high internal consistency. Similar results were reported in the Iranian version (α = .92; Abasi et al., 2021). Concerning the dimensions, the results obtained were similar to those reported in the original study (α values between .85 and .91; Hofmann et al., 2016), as well as in German (α values between .81 and .91), Italian (α values between .81 and .88), and Indian samples of husbands (α values between .72 and .83) and wives (α values between .72 and .83). The evaluation of the impact of item removal on the scale’s reliability showed that removing items did not increase the scale’s internal consistency; except for item 4, which when removed increased ω and α values, although it did not exceed the upper limit of the confidence interval. Completing the reliability analysis of the scale, adequate item discrimination indices were found (r > .383). This suggests that all items contribute meaningfully to the measurement of the construct.
Regarding validity evidence in relation to other variables, some correlations aligned with theoretical expectations. Small but significant positive correlations (p < .001) were found between the IERQ dimensions and the ERQ and its reappraisal dimension; except for the Perspective taking dimension, which had an irrelevant magnitude. As expected from the theory (Aldao et al., 2010), the suppression dimension of the ERQ showed negative correlations with the IERQ dimensions, consistent with findings from a recent adaptation of the IERQ in Uruguay, which also reported links between the two instruments. However, similar to the present study, these relationships were small, irrelevant, or not statistically significant (Anselmi et al., 2023).
Regarding the IERQ and the RPI, correlations with the reward probability dimension and IERQ four factors were positive, while correlations with the suppressors subscale were negative and irrelevant. As expected from the theory, IER is associated with reward sensitivity, which has been linked to seeking and contingently responding to social interactions (Altan-Atalay & Saritas-Atalar, 2019). Furthermore, Response Contingent Positive Reinforcement (RCPR), like REI, has been associated with attachment and attachment styles, and with the development of socioemotional behaviors, which may explain behaviors related to social withdrawal and emotional symptoms in response to low rates of RCPR due to inadequate primary attachment models (Sandhu & Sharma, 2015).
The SWLS exhibited moderate, positive correlations with interpersonal emotion regulation strategies. While these findings align with previous studies (Bojórquez et al., 2019; Castro et al., 2021), it is important to note that the strength of these relationships can vary across studies, as evidenced by contradictory findings reported by Tepeli Temiz and Elsharnouby (2022).
Some correlation results were unexpected based on the scale’s empirical background. No relationships were found between emotional symptoms (DASS-21 and its dimensions) and interpersonal emotion regulation strategies (IERQ), except for an irrelevant correlation between the Depression subscale and the Perspective Taking dimension. This is similar to findings reported by Canales et al. (2024) in their validation of the ERQ in Colombia and Zhao et al. (2023) in their validation of the IERQ in China, who reported very low correlations between the ERQ and IERQ factors with the DASS-21 and its scales. These results align with Visted et al.’s (2018) systematic review and meta-analysis, which concluded that despite improvements in reported emotional symptoms, difficulties in emotion regulation persisted, posing a risk for future relapses, suggesting a complex relationship between emotion regulation and psychopathology. From a measurement standpoint, the absence of substantial associations with the DASS-21 and its subscales is consistent with good discriminant validity of the IERQ with respect to general emotional symptoms, in the sense that interpersonal emotion regulation is not merely a proxy for distress. At the same time, this pattern may also indicate that interpersonal emotion regulation, as measured here, is only weakly related to concurrent symptom severity in this type of community sample. For this reason, we avoid treating the lack of strong correlations as unequivocal evidence of discriminant validity and instead consider it a preliminary finding that must be interpreted with caution.
These findings suggest that emotion regulation strategies, both intra- and interpersonal, may mediate the relationship between responses to the environment and emotional symptoms. However, they do not appear to be the sole explanatory factor for such symptoms. According to the process-based approach to psychology (Hayes & Hofmann, 2018), the effectiveness of emotion regulation strategies may vary across individuals. Previous studies have shown that emotional symptoms can predict difficulties in emotion regulation, but not necessarily vice versa (Fernandez et al., 2016; Messina et al., 2023). Additionally, some research suggests that emotion regulation strategies may act as a buffer against emotional distress (Liu et al., 2021). The results of the DASS-21, which correlated as expected with other scales, support the validity of the measures used in this study. In this context, we interpret the weak IERQ symptom associations as tentatively supporting discriminant validity with respect to general distress, while also recognizing that they may reflect limited convergent validity with symptom measures in non-clinical samples. Longitudinal and clinical-outcome studies are needed to determine whether IERQ scores predict changes in symptoms and functioning over time and to clarify the conditions under which stronger links with psychopathology emerge.
Limitations and Future Directions
A major limitation of the present study was the difficulty in obtaining a nationally representative sample, as most participants were from the capital city, Bogotá D.C. This resulted in a geographic sampling bias, as the five regions of Colombia were not equitably represented. Future research should involve a larger and more geographically diverse sample, which would allow for greater generalizability of the results and contribute to the standardization of the instrument.
Additionally, it is recommended to balance the gender distribution in future studies, given the predominance of women in the current sample. Furthermore, it would be interesting to analyze differences based on marital status and living arrangements.
The topic of interpersonal emotion regulation is relatively new in the Latin American and national context. Therefore, more research is needed to explore its relationship with other variables and to better understand its role in the Colombian population. Considering the influence of culture on emotion regulation processes (Hofmann & Doan, 2018; Liddell & Williams, 2019; Jobson et al., 2022), it is essential to consider Colombia’s cultural diversity when designing future studies.
At the item level, item 1 showed the weakest performance among the indicators of its factor. Specifically, it presented the lowest standardized factor loading (λ = .47) and the lowest corrected item-total correlation. Removing this item led to a slight increase in Cronbach’s α and McDonald’s ω; however, these values did not exceed the upper bound of the confidence intervals for the reliability estimates of the full scale, suggesting that the item does not materially compromise the internal consistency of the dimension. Given its theoretical relevance and non-redundant content, we decided to retain item 1 while recommending that future studies continue to monitor its performance and consider potential wording refinements if necessary.
Finally, it is recommended to include the assessment of additional behavioral problems or psychological difficulties in future studies, as suggested by previous research (Schwartz-Mette et al., 2021).
Conclusion
In conclusion, the Interpersonal Emotion Regulation Questionnaire (IERQ) has proven to be a sound psychometric instrument for assessing interpersonal emotion regulation in the Colombian population. However, further research is recommended to contextualize its functioning in different populations and explore its clinical implications. The use of the IERQ in conjunction with other instruments that assess social components could enrich its practical application. Additionally, research on the performance of the IERQ in clinical populations is suggested to determine its utility in assessment and diagnosis. The results of this study highlight the relevance of interpersonal emotion regulation in understanding emotional and social functioning and open up new avenues of research to explore the consequences of its impairment.
Footnotes
Appendix
Acknowledgements
We extend our sincere gratitude to all individuals who contributed to this study. We extend our appreciation to the expert judges for their invaluable input during the content evaluation. We are also thankful to those who participated in the clarity assessment of the IERQ’s linguistic adaptation for Colombia. Finally, we are profoundly grateful to all participants in the final form administration, whose collaboration was essential for the completion of this research.
Ethical Considerations
This study was conducted as part of a master’s thesis in Clinical Psychology at Fundación Universitaria Konrad Lorenz and followed the ethical guidelines of the Psychology Research Center of this institution. The project’s development and final presentation were evaluated through a blind peer-review process, in accordance with the Center’s procedures for student research. The study adhered to the Declaration of Helsinki on ethical principles for research involving human participants and to Colombian regulations for health research (Law 1090 of 2006, Law 1616 of 2013, and Resolution 8430 of 1993).
Consent to Participate
Informed consent was obtained from all participants before data collection. Consent was obtained electronically and included information about the study objectives, procedures, requirements, potential risks and benefits, the voluntary nature of participation, confidentiality of the information, joint handling of anonymized data, the process for receiving feedback on results, and contact details for the responsible researcher, in line with Law 1090 of 2006.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Hofmann receives financial support by the Alexander von Humboldt Foundation (as part of the Alexander von Humboldt Professur), the Hessische Ministerium für Wissenschaft und Kunst (as part of the LOEWE Spitzenprofessur), the DYNAMIC center, funded by the LOEWE program of the Hessian Ministry of Science and Arts (Grant Number: LOEWE1/16/519/03/09.001(0009)/98), the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Project-ID 521379614 – TRR 393SFB/Transregio 393 and the Excellence Cluster EXC3066 “The Adaptive Mind”. He also receives compensation for his work as editor from the American Psychological Association and royalties and payments for his work from various publishers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request from the corresponding author*.
Use of AI-Assisted Tools
Grammarly and a generative artificial intelligence tool (ChatGPT, OpenAI) were used to assist with grammar, phrasing, and style editing in the preparation of this manuscript. These tools were not used to generate scientific content, conduct data analyses, or formulate the study’s hypotheses, results, or conclusions. All AI-assisted suggestions were reviewed and edited by the authors, who take full responsibility for the final content of the article.