
Abstract
Adherence to treatment of diabetes mellitus (DM) can support successful therapy due to drug consumption over longtime periods. The objectives of this study are to evaluate the treatment adherence in DM as related to the quality of life and to evaluate factors associated with adherence and quality of life. This study used the Brief Medication Questionnaire (BMQ) to measure patients’ adherence. The Diabetes Quality of Life Clinical Trial Questionnaire (DQLCTQ) was used to measure patients’ quality of life. Subjects of this cross-sectional study were DM patients attending two private hospitals in Yogyakarta and who had been taking DM medications for more than 6 months. Statistical analyses used in this study were student’s t test and regression linear test. We recruited 65 DM patients who met the inclusion criteria. There were no significant differences of BMQ screens and DQLCTQ functions between monotherapy and combination therapy groups (p> .05). The BMQ screens’ score of combination therapy were higher than monotherapy groups. The physical function, health distress, and mental health of combination therapy groups were higher than monotherapy group. The male patients had significantly higher score of regimen domain of BMQ than female patients (0.35 and 0.17, respectively). The older age has the lower score of treatment effect of DQLCTQ (p< .05). The belief, recall, and belief about adverse drug reaction of BMQ have positive correlation with physical function (r = .542, .424, and .640, respectively). Our study concluded that the quality of care, sex, and age may predict patients’ adherence and quality of life. There were positive correlation between patients’ adherence and quality of life.
Background
The success of medical treatment is influenced by the quality of health services and patient adherence to their treatment plan (Hsu et al., 2014). Therapeutic treatments will not achieve optimum effects without patient awareness, because without it, therapy can fail or complications may eventually lead to fatal events (Hussar, 1995).
A number of studies have shown that patient adherence during chronic treatment such as diabetes mellitus (DM), asthma, cardiovascular diseases, high cholesterol, breast cancer, and glaucoma is commonly low. The discontinuation rates of the medication on the 30 days of treatment reached 42% and non oral treatment of DM had the high risk of discontinuation (Vanelli et al., 2009; Zullig et al., 2015). Research involving outpatients shows that more than 70% of patients do not adhere to correct administration and appropriate medicine dosage (Basuki, 2009). According to the World Health Organization (WHO) report in 2003, average of patient adherence in long-term therapy for chronic diseases in developed countries is only 50%, while in developing countries, it is even lower (Asti, 2006). The prevalence of nonadherence in diabetic patients is high, due to the duration of treatment, and may lead to an increase in mortality, morbidity, and other adverse effects (Blackburn, Swidrovich, & Lemstra, 2013; Delamater, 2006). The other previous study showed that nonadherence in oral antidiabetic treatment was associated with the incidence of end-stage renal disease, and the effect was more significant in the polytherapy of oral antidiabetic treatment and under the metformin polytherapy, besides other risk factors (Chang, Chien, Lin, Chiou, & Chiu, 2015).
Adherence to treatment involves patient psychology, such as knowledge and motivation. Adherence is also influenced by the quality of interaction between patient and health provider (Delamater, 2006; Sarafino, 1998; Taylor, 2006). There are some annoying patient behaviors, such as expression of criticism and anger, ignoring doctor’s advice, asking for laboratory tests, asking for medications that according to the doctor are not needed, and other things that reflect nonadherence. Under such conditions, the quality of medical services will negatively affect, so it is necessary to encourage conditions that improve individual motivation toward the adoption of long-term treatment, including their quality of life (Sarafino, 1998). A previous study about health-related quality of life (HRQoL) of type 2 DM patients in Bangladesh showed that some patients’ characteristics like age, gender, income, education, family history, duration of DM, and treatment prescribed could affect patients’ quality of life (Saleh, Mumu, Ara, Hafez, & Ali, 2014). Other previous study in Malaysia reported that the use of insulin could give negative impact to the patients’ quality of life. Patients treated with insulin, who also supported by strict lifestyle management, got desired glycemic control. However, that management could cause the deterioration in quality of life (Daher et al., 2015).
One method for understanding patient adherence is the use of the Brief Medication Questionnaire (BMQ). The questionnaire illustrates the patient’s assumptions toward medication, including necessity, awareness, illustration of painful effects, and excessive drug use (Menckeberg et al., 2008). A previous study conducted on type 2 DM patients in Iran concluded that low BMQ scores were related to low patient adherence, which resulted in experiences of adverse drug reaction by patients (Delamater, 2006).
The Diabetes Quality of Life Clinical Trial Questionnaire (DQLCTQ) is one of the DM quality of life questionnaires developed by the United Kingdom Prospective Diabetes Study (UKPDS) group. This instrument has been piloted in San Francisco, California, and Lyon, for type 1 and type 2 DM patients. The items measured in the DQLCTQ include 8 domains: physical function, energy/fatigue, health distress, mental health, satisfaction, treatment satisfaction, treatment flexibility, and frequency of symptoms. Total scores vary between 0 (poor quality of life) and 100 (highest quality of life). The higher scores indicate a better health status (Shen et al., 1999). To date, there have been no studies in Indonesia with the objective of exploring patient adherence and quality of life in DM patients or to analyze predictors using the BMQ and DQLCTQ questionnaires. The objectives of this research are to evaluate the treatment adherence in DM as related to the quality of life and to evaluate factors associated with adherence and quality of life.
Method
Participants
This study used a cross-sectional design and the data were collected prospectively. We conducted this study at two private hospitals in Yogyakarta. The subjects of this research were all type 2 DM outpatients who had used a minimum of 6 months monotherapy or combination therapy since diagnosis. Inclusion criteria were type 2 DM patients, at least 6 months after initial diagnosis, who voluntarily became involved in the research, and were literate. Exclusion criteria were type 2 DM patients who were suffering chronic disease complications, patients with psychiatric diseases and who did not volunteer to enroll in this research. We excluded these patients by finding the diagnoses in their medical records. By excluding the complications of the patients, we also excluded the patients with comedications. Patients who used monotherapy DM treatment had only one kind of DM medication, whether oral or injection. Patient who used combination DM therapy used a combination of more than two types of DM medication as well as oral–oral, oral–injection, or injection–injection (combination of short acting insulin and medium acting insulin).
We conducted and compared our study in two private hospitals which are under the similar organization in Yogyakarta. The differences between the hospitals are the location, the capacity, and the status of hospital. The Hospital A is located in the city, higher capacity and having status as education hospital. However, the Hospital B is located in urban area, lower capacity and the education hospital status is still submitted to the government. Thus, the differences between the hospitals could be according to the typical of the patients which came around the city and the urban area. Both of the hospitals are the referral hospitals from the primary health care, and the government health insurance has been applied in the two hospitals. There are no differences between the treatment guideline, due to the universal health coverage applied in the hospitals.
Patients at both hospitals were asked to join the research voluntarily and to give their informed consent. To aid quality control during data collection, the researcher accompanied the patients while they completed the questionnaires. This research was approved by the Research Ethic Committee of University of Muhammadiyah Yogyakarta.
Questionnaires
We used the Indonesian version of the BMQ and an already validated Indonesian version of the DQLCTQ. The two questionnaires were used in this study due to the availability of DQLCTQ in Bahasa Indonesia and the short version of BMQ. Adherence to treatment was measured by the BMQ with the screen of dose regimen, recall, access, and belief. The regimen screen has 0 to 5 scale; however, the recall, access, and beliefs screens have 0 to 2 scale. There are also three questions about fear or worry about drug side effect which has 0 to 3 scale. The higher scale of screens is the better compliance and positive concern about recall, access, and beliefs, and less fear about side effect. This questionnaire has 0 to 1 scale which shows the higher score is the better adherence (Svarstad et al., 1999). This study was preceded by a forward–backward translation from the original version of BMQ to obtain an Indonesian BMQ version and was followed by pilot testing and a validity and reliability test for DM patients. Validation and reliability tests using the Indonesian version of the BMQ were conducted on 20 DM patients. Forward and backward translation of the BMQ was carried out before this study. Two Indonesian translators who were experts in the English language performed the forward translation process. Discussions were carried out to compare the questionnaires and agree on one version in Bahasa Indonesia. The Indonesia version was backward translated by a native speaker who was fluent and understood Bahasa Indonesia. To corroborate the translation result, an Indonesian who was an expert in the English language performed a backward translation. The comparison of the two results from the backward translation and the original version of the questionnaire were performed, and one version in Bahasa Indonesia was obtained with the same content as the original version.
The results of a pilot test on the first draft of the Indonesian BMQ version were related to the layout of the questionnaire. The respondent suggested a clearer layout for the questionnaire to make it easier to answer. Pilot testing also showed that there were no significant differences in the domains of beliefs and adherence among healthy respondents and sick respondents (p> .05). However, a significant difference was seen in the dosage regimen domain among healthy and sick respondents (data not shown). This result can be explained because healthy respondents did not take drugs, so there could be no problem with their dosage regimen.
We used the Cronbach’s alpha coefficient which was more than .7 to meet the criteria of validity. Furthermore, the construct validity to measure the convergent and discriminant validity of Indonesian version of BMQ was performed (Pérez-Escamilla, Franco-Trigo, Moullin, Martínez-Martínez, & García-Corpas, 2015).
Patient quality of life was measured with the DQLCTQ with the domains of physical function, energy, health distress, mental health, satisfaction, treatment satisfaction, treatment effect, and frequency of symptoms. This questionnaire has 0 to 100 scale which shows the higher score is the better quality of life. The Indonesian version of DQLCTQ has been validated in the previously study (Hartati & Asdie, 2003).
Statistical Analysis
Cronbach’s alpha coefficient was defined to understand the reliability of Indonesian version of BMQ. Pearson-correlation test was performed to understand the construct validity of Indonesian version of BMQ. The item of questionnaires met the convergent validity if significantly related to its domain and met the discriminant validity if the relation between item and its domains was higher than its relation with other domains (Perwitasari et al., 2011).
The differences between the BMQ and DQLCTQ scores, between the monotherapy and combination therapy groups, and between the two hospitals were tested using the student’s t test (for parametric tests) or the Mann–Whitney test (nonparametric tests). Regression linear tests were used to understand the predictors of adherence and quality of life.
Results
An earlier step in our study was the translation and validation of the Indonesian version of the BMQ. The Indonesian DQLCTQ was available as a validated version.
Table 1 presents the Cronbach’s alpha value (>.70), which shows that all BMQ domains met the criteria for reliability. The results of the validation test can be seen in Table 2. All questions and domains of the Indonesian BMQ version met discriminant and convergent validity with significant results (p< .01), except for Question Number 7c on the regimen domain and the Question Number 2 of recall domain. That was because there was only one answer from the respondent, so it was not possible to have variation.
Reliability Test of Indonesian Version of BMQ.

Note. BMQ = Brief Medication Questionnaire.
Test Validity Result of BMQ Indonesia Version.
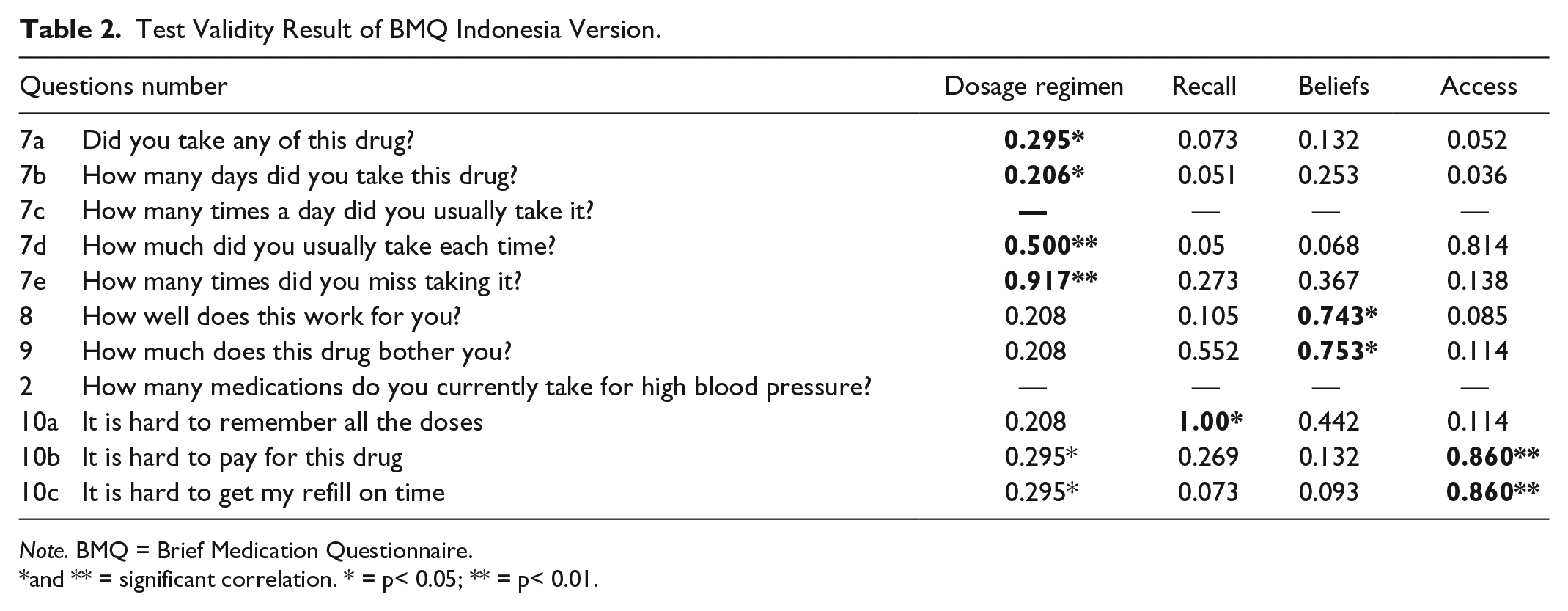
Note. BMQ = Brief Medication Questionnaire.
and ** = significant correlation. * = p< 0.05; ** = p< 0.01.
Table 3 presents patient characteristics; most of the patients were female (52.3%), mean average was 57.69 ± 11.41, and they were prescribed combination therapy for DM treatment (66.2%). The score of BMQ screen was good, which mean that the patients adhere to the regimen of the treatment (4.45 ± 0.95), the patients had a good recall of their medication (1.92 ± 0.97), the refill of medication was affordable (1.93 ± 0.30), the belief about the effectiveness of their medication was good (1.71 ± 0.55), and there was less fear or worry about the side effect (2.55 ± 1.53).
Patients’ Characteristic, BMQ Scores, and DQLCTQ Scores (N = 65).

Note. BMQ = Brief Medication Questionnaire; DQLCTQ = Diabetes Quality of Life Clinical Trial Questionnaire.
The results of the BMQ and quality of life analysis regarding the type of patient treatment (monotherapy and combination therapy) are shown in Tables 4 and 5. There were no significant differences of BMQ screens between the types of treatment. Moreover, there were no quality of life differences between the monotherapy and combination therapy groups.
The Score Differences of Indonesian Version of BMQ Screen.
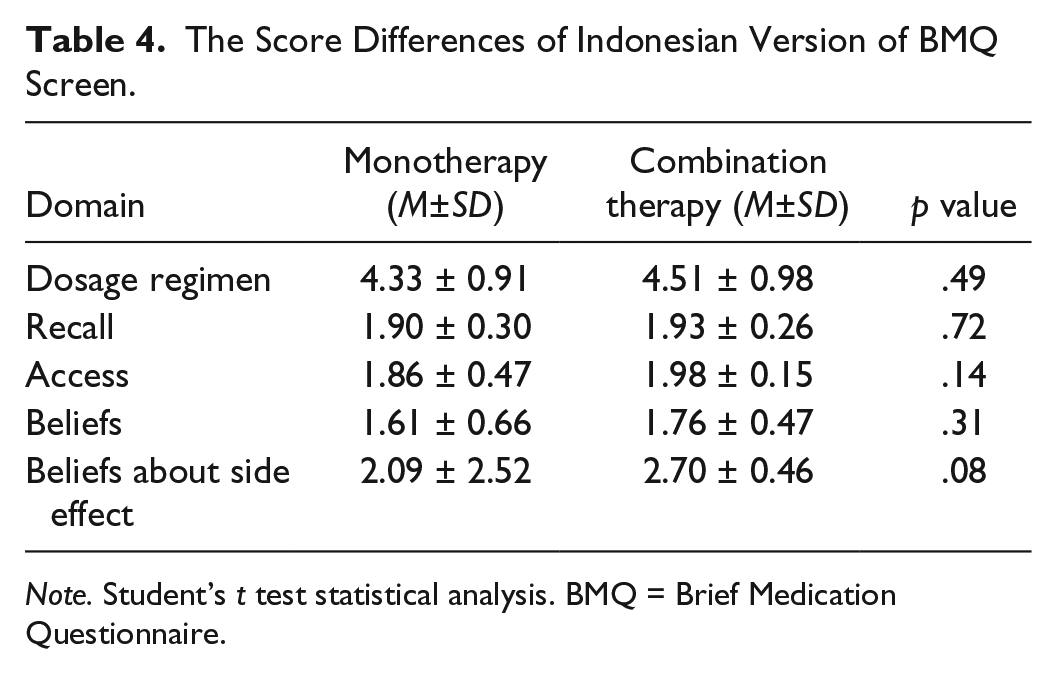
Note. Student’s t test statistical analysis. BMQ = Brief Medication Questionnaire.
The Differences of Quality of Life Domains.

Note. Student’s t test statistical analysis.
We analyzed the scores differences of BMQ domains and quality of life domains between two hospitals. The dosage regimen shows significant differences between the two hospitals, which is patients of Hospital B had a higher mean score for dosage regimen than those of Hospital A (4.18 ± 1.20 and 4.74 ± 0.51, respectively; p< .01). Furthermore, there was significant difference between the two hospitals in the treatment effect domain (p< .01). Patients of Hospital B had a higher mean treatment effect than those of patients at Hospital A. Generally, the quality of life domains score was more than 70, which showed that the quality of life at both hospitals was quite high, except for the treatment effect domain at Hospital A (59.24 ± 12.9 and 75.00 ± 20.7, respectively) and the patients’ satisfaction domain in both hospitals (data were not shown).
Regarding the demographic factors in this study, we found that only the BMQ regimen domain was significantly different between sexes. The mean score of the regimen domain of male patients was higher than for female patients (0.35 and 0.17, respectively; p = .03). However, only the treatment effect domain of the DQLCTQ showed a significant difference between sexes with the score of male patients being higher than for female patients (71.96 and 62.47, respectively; p< .01). However, patient age significantly affected the DQLCTQ treatment effect domain (r = .28, p< .02, data were nor shown).
According to the correlation between BMQ domain and quality of life domain, we find that beliefs, recall, and beliefs about adverse event screens of BMQ had positive correlation with physical function (r = .542, .424, .640, respectively; p< .05, data were not shown).
Discussion
In general, we found positive correlation between adherence to medication and quality of life. Patient demographic factors like age and sex affect patient’s adherence and quality of life. There are no significant differences of BMQ screens and DQLCTQ functions scores between monotherapy and combination therapy. On the contrary, there are some significant differences of BMQ screens and DQLCTQ functions scores between the two hospitals. Our findings were supported by previous study which stated patient’s access to drugs which was definitely determined by the distance between the patient’s house and the hospital, the duration of disease, complexity of treatment, polytherapy, psychological factors, safety, and tolerability became potential reasons for patients’ nonadherence. It means that adherence will decline with an increase in drug numbers (García-Pérez, Álvarez, Dilla, Gil-Guillén, & Orozco-Beltrán, 2013).
According to high scores of BMQ screens and moderate scores of DQLCTQ, it can be a challenge for health care providers, especially pharmacists, nurses, doctors, and psychologists, to motivate patients to carry out their therapy properly. Of course, this is not an easy thing, because collaboration from various health personnel is needed to help patients to adapt to their disease and treatment. Previous studies have stated that DM health care teams should collaborate to support patients to cope with the disease and treatment, and thus to improve their adherence (Delamater, 2006). Another previous French study shows that most diabetic patients have medium adherence which is affected by demographic factors, health provider-related factors, and disease treatment-related factors (Miv et al., 2012). Some factors may be modifiable, meaning that the health care provider can give individualized patient recommendations. However, some demographic factors like older age and complexity of disease and treatment could not be modified.
According to the DM treatment type, the score of all screen in BMQ for combination therapy is higher than for the monotherapy group. A previous study also shows that decreased adherence was related to polytherapy (Claxton, Cramer, & Pierce, 2001). This factor can be modified by changing the medication into a simple regimen which can be managed by patients. There was also no difference in quality of life between the monotherapy group and combination therapy. The previous study used the EuroQol five dimensionsquestionnaire (EQ-5D), which only consisted of five questions; this certainly helped the patients to fill in the questionnaire with ease. This study shows that patients with low adherence have a low quality of life (Saleh et al., 2014). In contrast, the current research showed that, on average, a patient’s quality of life was quite good (score >75) except on some domains such as satisfaction and treatment effect. This difference could be caused by sample number, variation due to the instrument that was used, and differences in hospital service quality. Other previous studies regarding factors related to the quality of life of diabetic patients stated that DM had a negative impact on patients’ quality of life and that comorbidity may further decrease patients’ quality of life (Wändell, 2005).
Patients’ quality of life at both hospitals was only significantly different with regard to the domain of treatment effect. This treatment effect can be categorized into therapeutic effects and adverse effects. Adverse effects of treatment may appear when the drug is taken for a long time period or may be due to the interaction with other drugs taken for other pathologic conditions. Previous studies showed that nonadherence of DM patients was significantly related to medication-adverse effect (Chao, Nau, & Aikens, 2012; Rwegerera, 2014; Wabe, Angamo & Hussein, 2011). DM patients who experience complications may be given more than three types of drug, which could result in drug interaction and adverse effects (Curkendall, Thomas, Bell, Juneau, & Weiss, 2011; Nau, 2012). From the interview with patients, we understand that such issues will of course affect patient quality of life as patients may avoid taking DM medication, and therefore, therapeutic effects will decrease. However, if a patient decided to continue on taking DM medication despite the unpleasant side effects, the patient may suffer during treatment. In general, the quality of life for DM patients at both hospitals was quite high, with scores >75, except for some domains such as satisfaction and treatment effect. Most of the type 2 DM patients experienced hypoglycemia (around 57%; Nau, 2012), which could have affected adherence (Chao et al., 2012; Nam, Chesla, Stotts, Kroon & Janson, 2011). Because of the long duration of treatment, other adverse effects such as constipation, headaches, and water retention may also result in nonadherence in diabetic patients (García-Pérez et al., 2013). Poor adherence can have clinical impacts such as a decrease in glycemic control, complication of the disease, mortality, and hospitalization (American Diabetes Association [ADA], 2013; Blackburn et al., 2013; Ho et al., 2006). In this study, we did not take the data of adverse effect experienced by the patients. However, we can see patients’ perceptions about adverse effect in the beliefs domain of BMQ. We can see the hypoglycemia effect from the domain of treatment effect and frequency of symptoms of DQLCTQ, because DQLCTQ adopted the hypoglycemic fear survey in its domain (Shen et al., 1999). The beliefs domain in Hospital B was higher than the beliefs domain in Hospital A, meaning that patients in Hospital A did not understand about the treatment and the treatment’s effect. However, there were three questions about the fear of patients toward adverse effect. The patients in both of the hospitals had less fear or worry about drug adverse event. This finding was also supported by higher score of treatment effect of DQLCTQ, whereas the higher score of Hospital B reflected that patients in Hospital B had better treatment effect than Hospital A. According to the patients’ adherence, we can see that patients in Hospital A had lower score of adherence than Hospital B, and it could be due to the higher adverse effect fear experienced by patients of Hospital A.
According to the hospital’s service, even though Hospital A is located in the city and has higher status level, the Hospital B could provide better health service and could be acceptable to the patients. Thus, Hospital B supported patients’ attempts to adhere to their medical treatment and cope with the disease in their life. The integrated health service in the Hospital B from the physician, nurse, pharmacist, and dietician could support patients’ adherence. A previous study showed that demographic, psychological, social support; health care providers; medical systems; disease; and treatment-related factors can promote diabetic patients’ adherence. Social support given by nurses in DM health care teams may improve glycemic control, lipid levels, and blood pressure levels (Delamater, 2006). The multidisciplinary approach to the diabetes management and the nature of clinical setting can influence patients’ adherence and quality of life (Nau, 2012). The results of the previous study are in line with our study, which showed that the sex and age of patients may influence patients’ adherence and quality of life.
Our study also found that the physical domain of DQLCTQ was affected by BMQ domain such as belief, recall, and beliefs about Adverse Drug Event (ADE). It means that patients’ belief about the effectivity of their medication, and about the ADE and patients’ adherence in taking the medication, can predict patients’ quality of life. These results are in line with previous study in which medication adherence had positive correlation with DM patients quality of life (Chew, 2015). However, previous studies about the correlation of DM patients’ adherence and HRQoL in Pakistan showed that the patient’ HRQoL decreased associated with the poor adherence (Nazir, Hassali, Saleem, Bashir, & Aljadhey, 2015).
To the best of our knowledge, our study was the first to address adherence to treatment in DM patients using the Indonesian version of the BMQ. This questionnaire is suitable for DM patients as it meets minimum requirements for test reliability and validity. Systematic review about validation of questionnaires to measure patients’ adherence in hypertensive patients showed the results of internal validity of BMQ which were on the range 0.60 to 0.73. However, there were no construct validity reported of BMQ in the systematic review (Pérez-Escamilla et al., 2015). Our study presents the good value of Cronbach’s α and acceptable values of convergent and discriminant validities.
The limitation of our study was the small sample size and we only recruited outpatients of DM. We also cannot generalize our findings to all DM patients due to the exclusion criteria in our study which could not find in the medical records. We have conducted the interview training to all researchers involved in this study; however, we cannot standardize the information which should be deeper explored to the patients. For further research, we propose intervention from pharmacists, psychologists, nurses, and physicians as a health care team to work together to improve patients’ adherence to treatment in outpatient and inpatients situation.
Conclusion
Our study concluded that the quality of care, sex, and age may predict patients’ adherence and quality of life. Furthermore, there are positive correlation between patients’ adherence and quality of life.
Footnotes
Acknowledgements
The authors thank to the heads and staffs of the hospitals who assisted the researcher in conducting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support from University of Ahmad Dahlan for the research and/or authorship of this article.