
Abstract
The lack of access to adolescent and youth-friendly services is a global concern due to its negative impact on adolescent health. Adolescents and youth-friendly services have been identified as responsible for improving access to sexual and reproductive health services for the adolescent population. Less research has been done to determine how accessible these services are. This study explored adolescents’ perceptions regarding access to Adolescent and Youth-Friendly Services in the eThekwini district. A quantitative descriptive design using a probability random sampling technique was adopted. A self-administered questionnaire was used to collect data from 377 adolescents between 16 and 24 years old. Descriptive analysis was used to analyse data. Most respondents (57%) agree that policies and procedures were in place. Most (79%) perceived respect and equal treatment, 62% stated convenient operational hours, shorter waiting times and swift referrals and 77% disclosed that the service package, information, and education resources were available. In comparison, 47% indicated involvement in decision-making, 72% confirmed the competency of healthcare providers, 73% revealed sufficient consultation time, 66% reflected on sufficient equipment and suppliers, and 86% confirmed the aesthetical environment. Adolescents in this study appreciated accessing the Adolescent and Youth-Friendly Services. This study highlights the necessity of implementing adolescent-focused policies and processes to increase service access. It also stresses the importance of community outreach initiatives to empower adolescents and increase access to services and adolescents’ involvement in the facilities. Further studies should be conducted to elucidate the reasons behind the elevated levels of adolescents pregnancies when services are accessible.
Keywords
Introduction
The World Health Organisation (WHO) classified adolescents as 10 to 19 years and youth aged 15 to 24. Adolescence is a unique phase that allows society to value adolescents’ contributions and ensure optimal investments to support healthy growth and development. Hence, the health and lifestyle of young people are important determinants of future illness. Adolescents are generally not exposed to health screenings for sexually transmitted illnesses (STIs), drugs and alcohol. They usually visit health facilities once they experience a minor ailment. Improving adolescents’ health is critical for well-being and economic growth.
Adolescents are healthy but have unique health requirements. According to the literature, despite adolescents being considered healthy, around 1·49 million deaths occurred in 2020 globally (WHO, 2023). The mortality rate is higher in sub-Saharan countries than in high-income countries. Adolescents in these countries experience STIs, including HIV/AIDS, unsafe abortion, unintended teenage pregnancy, mortality and morbidity related to pregnancy, non-communicable diseases, nutritional disorders, as well as high rates of injury and violence (Liang et al., 2019).
It was crucial to ensure that this generation cohort was healthy. According to Garney et al. (2024), ensuring adolescents have access to high-quality healthcare was crucial for preventing and intervening early to foster healthy habits and enhance general health. Adolescents require healthcare services that are safe, supportive and tailored to their specific requirements to ensure Sustainable Development Goal 3, Target 3.7, are met to guarantee universal access to sexual and reproductive health (SRH) services and rights by 2030. In 2002, the WHO advocated the implementation of Adolescent and Youth Friendly Services (AYFS), which has been implemented globally.
Adolescent Sexual and Reproductive Health (ASRH) Implementation Guideline 2011 stated that for health facilities to be adolescent-friendly, they should incorporate characteristics like convenient service time, convenient location of health facility, adequate space including waiting space, maintenance of privacy, welcoming environment, availability of information, education and communication (IEC) materials and trained healthcare providers (HCPs) (Pandey et al., 2019).
The AYFS is an evidence-based public health intervention aimed at the prevention of abortion and pregnancy while promoting the use of contemporary contraception (Habitu et al., 2021). The AYFS promotes access to health services, SRH information, and skills development to help adolescents make informed decisions about their health (Ninsiima et al., 2021).
Various pieces of literature have identified a lack of provider competency, provider attitude, confidentiality breaches, privacy, inconvenient operating hours and long waiting times, physical inaccessibility of services, lack of awareness and shortage of medicine and supplies as barriers to accessing services (Garney et al., 2024; Moolla et al., 2023; Nmadu et al., 2020; Otieno et al., 2020; Parmar et al., 2024; Sidamo et al., 2021).
The South African (SA) Government, in acknowledging the challenges and needs of adolescents and youth, implemented programs and policies to improve access to adolescent reproductive health. The AYFS has been implemented as a standard-driven strategy consistent with WHO global standards for exceptional adolescent healthcare services.
The SA government has implemented the AYFS to increase the accessibility of services to adolescents and youth. South Africa invented robust laws and policies, such as the National Adolescent Sexual Reproductive Health Rights (ASRHR) Framework Strategy 2015; National Adolescent and Youth Health Policy 2017 (AYHP); The Choice on Termination of Pregnancy Amendment Act 1 of 2008 and National Youth Policy 2020 to 2030. These policies ensure the delivery of equitable services and allow adolescents to access contraceptives and terminate a pregnancy without parents’ consent.
Despite all these initiatives, a high number of young women in SA are still exposed to unplanned pregnancies, unsafe sex, STIs, including HIV and engage in unsafe abortions, which are detrimental to their health. KwaZulu-Natal (KZN) was among the top three provinces with high teenage pregnancies. In the 2022/2023 financial year, the KZN province had about 35,000 pregnancies (Sharma, 2023). SABC News reported that the KZN province has the highest burden of HIV, and eThekwini district is home to 60% of the HIV burden. The prevalence was among those aged 13 to 19 (SABC News, 2021). To close this gap, the researcher has explored adolescents’ perceptions of accessing the AYFS in the eThekwini health district.
Aim of the Study
To explore adolescents’ perceptions of accessing AYFS in the eThekwini health district.
Conceptual Framework
The researcher used the Donabedian conceptual framework of healthcare quality assessment (Donabedian, 1966). Donabedian (1980), cited in (Kumah et al., 2024), defined healthcare quality as using medical services and strategies to optimize health benefits while minimising risk. Donabedian’s framework categorises factors influencing quality into structures, processes, and outcomes. This framework categorizes adolescent care into three specific domains: the structure of care delivery, the process of interaction between adolescents and HCPs, and outcomes which pertain to the health status of adolescents and youth and satisfaction with the care provided.
The structure was related to the facility’s characteristics and health literacy, which included policies and procedures defining the required service package and equity and non-discriminatory policies, convenient location, welcoming and clean environment, adolescent participation, adequate medicines and supplies, health education, community outreaches, convenient operating hours, HCP competencies, signposts, health information, materials and education.
The process pertained to exchanging health-related information, encompassing HCP competence and attitude, community support, equity and non-discrimination, appropriateness of care, referral system, adolescent participation, and knowledge enhancement.
The outcome denoted the impact of care on the health status of the adolescent, covering enhancements of knowledge, modifications in behaviour, and increased patient satisfaction. This includes convenient working hours, minimum waiting time, a welcoming and clean environment, privacy and confidentiality, adequate equipment, medicine, suppliers and technology, effective services, and adolescents receiving friendly, supportive, respectful, non-discriminatory and non-judgemental care. Health services must be accessible to address the needs of adolescents within the facility or via referral and outreach.
Methods
Study Design and Setting
A quantitative cross-sectional descriptive design was used to explore adolescents’ perceptions of access to AYFS at eThekwini health district to establish baseline data, identify trends, inform decision making and understand complex phenomena. A quantitative cross-sectional descriptive design is a research approach employed to collect and analyze numerical data at a single point in time to describe characteristics, trends, or relationships within a population (Ghanad, 2023). The study was conducted in four Community Health Centers and eight Primary Health care clinics within the eThekwini health district.
Population, Sample Size and Sampling
This study’s target population comprised 20,000 adolescents who had visited the AYFS in the eThekwini district in the past six months. The Raosoft online sample size calculator (2020) calculated the sample size. It applied standard statistical formulas to calculate an appropriate sample size, ensuring reliable and generalizable results. It helped reduce sampling bias and ensured that the sample accurately represented the target population. Determining the optimal sample size helped the researchers avoid unnecessary data collection, saving time and resources. The researcher used the Raosoft parameters of a margin error of 5%, a confidence level of 95%, a population size of 20,000, a response distribution of 50% and a sample size of 377. The random sampling technique was adopted to sample adolescents between 16 and 24 years who visited the selected AYFS in the eThekwini health district.
Data Collection Tool
A structured self-administered questionnaire was used. The researcher adapted the Youth-Friendly Health Services-South Africa (YFHS-SA) (Boersema et al., 2019), which was adapted from Youth-Friendly Health Services-World Health Organisation + Questionnaire (YFHS-WHO + Questionnaire) (WHO, 2009). The questionnaire was adapted to ensure that relevant questions were included to determine adolescents’ perceptions of accessing the AYFS at eThekwini health district. Cronbach’s alpha was calculated after a self-administered questionnaire was adopted to assess the internal consistency reliability of the instrument. The Cronbach’s alpha score for the questionnaire was .9. Cronbach’s alpha value of .70 or above is considered acceptable reliability (Taber, 2018), while that of .96 is considered excellent reliability (Ameh et al., 2017). The questionnaire comprised sociodemographic characteristics and ten subscales, and it utilised a Likert scale to capture the adolescents’ responses. The five-point Likert scale indicated strongly agree, agree, unsure, disagree, and strongly disagree.
Ethical Considerations
The study received ethical approval from the Humanities and Social Sciences Research Ethics Committee (HSSREC/00004775/2022) and the Provincial Department of Health (NHRD Ref: KZ_202212_014). Written permission was obtained from the healthcare facilities. The study was explained to each respondent, and time was given to ask questions. Information about the study, the participant’s right to withdraw, and voluntary participation were provided to all respondents. Those who agreed to participate in the study signed a written informed consent. The signed consent forms were detached from the questionnaires to eliminate any potential connection. To ensure confidentiality and anonymity, the questionnaire did not require personal data. Respondents were guaranteed confidentiality and anonymity, which were maintained from data collection to the presentation of the results.
Data Collection Process
The researcher arranged with the facilities operations managers regarding a convenient day and time to meet with the adolescents. The participants were contacted and invited to participate in the study. Each respondent was informed that completing the questionnaire would take about 30 min. An information letter detailing the purpose of the study, a consent form and a questionnaire were handed to each respondent. Once they decided to enrol, a declaration and consent form was signed. The researcher collected all completed questionnaires and consent forms. Consent forms were kept separate from the questionnaire to ensure anonymity. Data collection was done from August to December 2023.
Data Analysis
The data was thoroughly checked to ensure quality and completeness, with no missing values and consistency, before being entered into an Excel spreadsheet (Microsoft, USA). The data were cleaned, coded, and transferred to the Statistical Package for Social Sciences (SPSS) version 29.0 to derive meaningful conclusions. The descriptive analysis described the sociodemographics and the adolescents’ perceptions of accessing AYFS at eThekwini health district. The Pearson Chi-Square Test (χ2) was used to determine whether a significant association existed between sociodemographic traits and the independent variables. The results were presented as frequencies, percentages, mean and standard deviation. The Likert scale options for the participants’ perceptions of adolescents strongly agree and agree were merged into positive scores, and strongly disagree and disagree were merged into negative scores.
Results
Understanding the data’s nature and the scores’ distribution is crucial before applying any statistical analysis. The nature of the data determines the appropriate statistical tests to use, and the distribution of scores can provide important information. For example, parametric tests may be appropriate if the data are normally distributed, while non-parametric tests may be more appropriate for non-normally distributed data. Additionally, examining the distribution of scores can help identify potential outliers or other issues that need to be addressed before conducting statistical analysis. Three hundred seventy-seven questionnaires were distributed to the respondents, and 357 questionnaires were returned. The 95% response rate was considered to be excellent.
Sociodemographic Characteristics
The sociodemographic characteristics of adolescents were analysed according to gender, age, current status, where they are currently studying, highest level of education completed, marital status, and employment status. Table 1 reflects the sociodemographic characteristics of respondents. The respondents were 86% females and 14% males. Age in years between 15 and 24; mean 2.56 and standard deviation .497. Currently studying mean 1.37 and standard deviation .484. The highest level of education was completed from junior to tertiary; the mean was 1.94, and the standard deviation was .539. Marital status from single to other; mean 1.18 and standard deviation .692. Work status; mean 1.86 standard deviation .348.
Sociodemographic Characteristics.

Adolescents’ Perceptions of Accessing the AYFS
Policies and Procedures That Promote Accessibility, Affordability, Confidentiality, and Privacy in the HC Facility
Most Health Services Are Available in This Health Facility
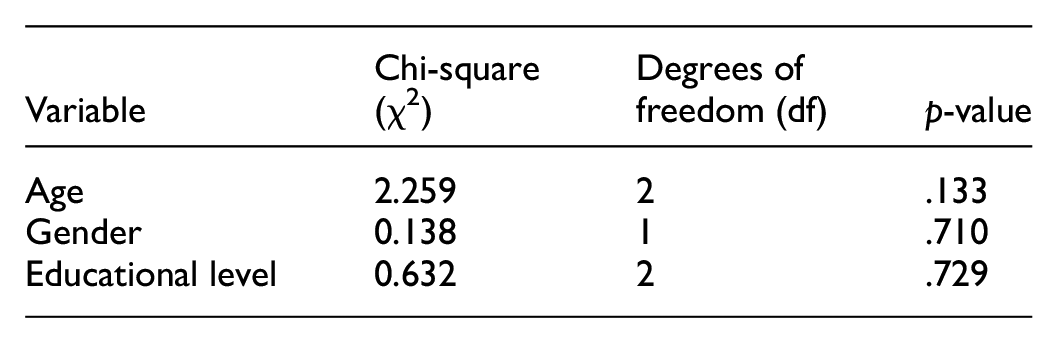
Out of 357 respondents, 162 (45.4%) agreed, 108 (30.3%) were unsure, and 87 (24.4%) disagreed that services were offered in the health facility. The descriptive statistics showed a symmetrical distribution; thus, it is shown as a bell-shaped distribution curve as the values for skewness were <1. This suggests approximate symmetry (or mild skewness). Since skewness is slightly positive (0 < skew < 1), there may be a small tail on the right with a mean of 1.79. The mean represents the central value of the dataset. A standard deviation of .809 indicated the spread of the data around the mean. A low standard deviation (closer to 0) meant data points were clustered near the mean. Since the distribution was bell-shaped and skewness <1, most students scored around 1 to 3, with fewer at the extremes. This suggests that the data was well-suited for further parametric statistical analysis. As demonstrated in Figure 1. The Pearson Chi-Square Test (χ2) was used to determine whether there was a significant association between categorical variables such as sociodemographic traits like age, gender, and education level. The results were:


Depict a bell-shaped distribution curve showing that most of the adolescent healthcare service packages available.
Age, gender, and education did not significantly influence the variable tested, such as attitudes or behaviour. The low χ2 values also suggest that the observed data was not significantly different from the expected data under the assumption of no association.
The Services at AYFHS Are Free of Charge
95.0% of respondents agreed, while 5.0% were unsure that services were free. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.05 and a standard deviation of .219. A mean of 1.05 suggests that most students scored very low. The mean was pulled to the right due to extremely high values (outliers). Positive skewness (>1) meant that a few students scored much higher than the rest. A positively skewed distribution meant the right tail was longer, and most values were concentrated on the lower end, with fewer high values. The low standard deviation (0.219) meant that most scores are tightly clustered near 1, with only a few higher scores pulling the mean upward. See Figure 2. The Pearson Chi-Square Test (χ2) was used to determine if there was a statistically significant association between categorical variables. Results:

A positively skewed graph showing that services at the AYFS are free of charge.
There was no statistical evidence to suggest a correlation between these sociodemographic traits and the dependent variable. The observed distribution of responses was similar to what would be expected under random chance, meaning no strong pattern exists in the data.
The Information Shared with the Healthcare Provider Is Kept Confidential
Out of 357 respondents, 308 (86.3%) agreed,16 (4.5%) were unsure, and 33 (9.2%) respondents disagreed that confidentiality was maintained. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.23 and a standard deviation of .602. See Figure 3. The Pearson Chi-Square Test (χ2) assesses whether there is a statistically significant association between categorical variables. Results were:


A positively skewed graph shows that information shared with HCPs was kept confidential.
There was no statistical evidence to suggest a correlation between these sociodemographic traits and the dependent variable.
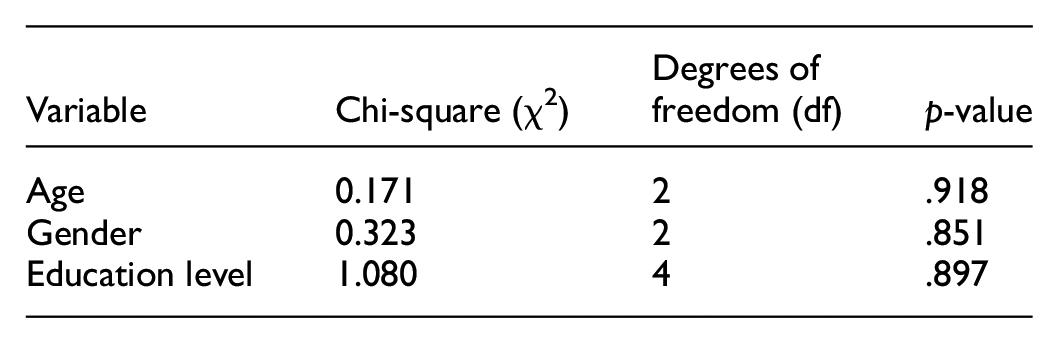
The Discussion with the Healthcare Provider Is Interrupted by Other People
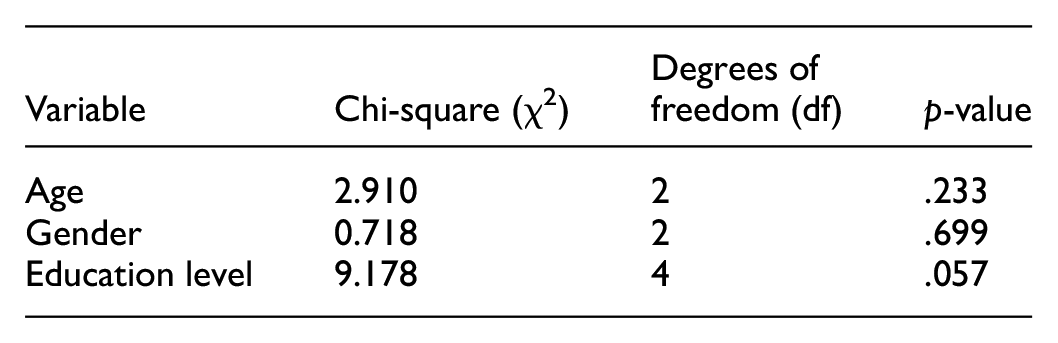
Of the 357 respondents, 219 (61.3%) disagreed, 111 (31.1%) agreed, and 27 (7.6%) were unsure that consultations were interrupted. The descriptive statistics showed a negatively skewed (left-skewed) distribution curve as the values for skewness was <-1, with a mean of 2.30 and a standard deviation of .914. A negatively skewed (left-skewed) distribution meant that most values were on the higher end, with a few low values pulling the tail to the left. The mean was lower due to extremely low values. The left tail was longer, showing a small number of significantly low values. As demonstrated in Figure 4. The Pearson Chi-Square Test (χ2) was used to assess whether there was a statistically significant association between categorical variables. Results were:


A negatively skewed distribution showing that discussion with HCPs was uninterrupted by others.
The distribution of responses did not show strong correlation patterns, meaning these traits did not significantly influence the outcome of this analysis. While the education level variable (p = .107) was closer to significance, it still does not meet the 0.05 threshold, meaning no firm evidence of a relationship exists.
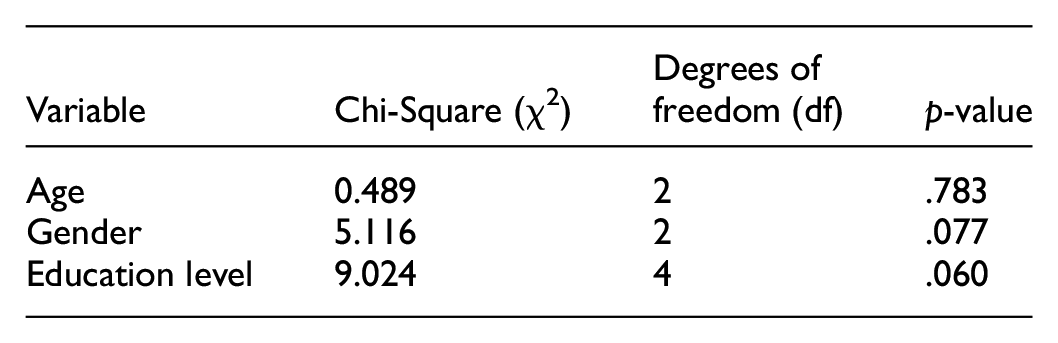
Other Clients Visiting the Health Facility Could Hear the Discussion with the Healthcare Provider
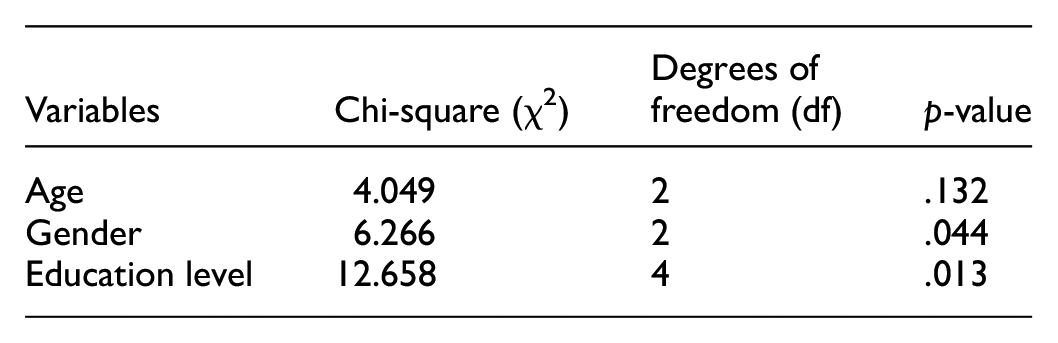
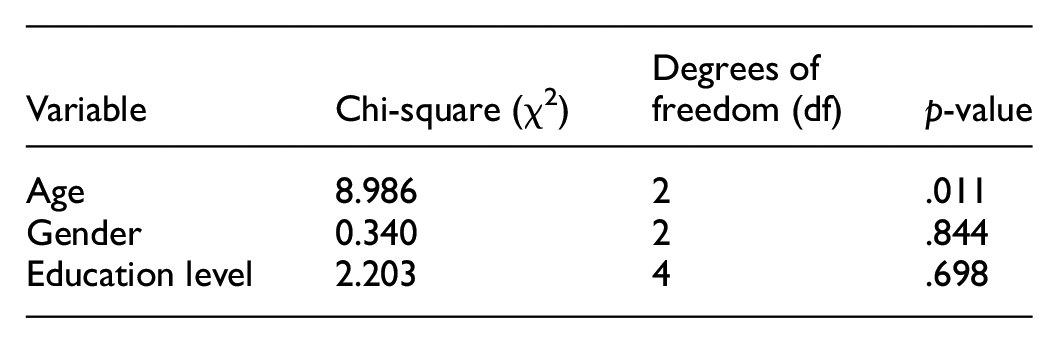
Of the 357 respondents, 233 (65.3%) disagreed, 96 (26.9%) agreed, and 28 (7.8%) were unsure of whether other clients visiting the health facility heard the discussion with the healthcare provider. The response from respondents was negative. The descriptive statistics showed a negatively skewed (left-skewed) distribution curve as the values for skewness was <−1 with a mean of 2.38 and a standard deviation of .881. The Pearson Chi-Square Test (χ2) determines whether there was a statistically significant association between categorical variables. Results were:

Age and education level showed statistically significant relationships with the dependent variable, indicating that these factors play a role in influencing the outcomes. Gender did not show a statistically significant relationship, meaning it did not significantly affect the outcome variable.
Healthcare Providers Treat All Adolescent Clients Equally and Respectfully and Are Non-Judgemental
The Healthcare Provider Respects Adolescents and Youth and Maintains Their Privacy
Of the 357 respondents, 299 (83.8%) agreed, 49 (13.7%) disagreed, and 9 (2.5%) were unsure that staff respected adolescents and youth and maintained their privacy. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.30 and a standard deviation of .697. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

Education level was significantly associated with the dependent variable, influencing the outcome. Age and gender did not show a significant association, meaning they did not play a key role in influencing the outcome variable.
The Healthcare Provider Was Non-Judgemental and Approachable
Out of the 357 respondents, 287 (80.4%) agreed, 53 (14.8%) disagreed, and 17 (4.8%) were unsure that the healthcare provider was non-judgemental and approachable. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.34 and a standard deviation of .724. The Pearson Chi-Square Test (χ2) was used to determine whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits (age, gender, education level) showed a statistically significant relationship with the dependent variable because all p-values were greater than .05. The education level was closer to significance, meaning it might have influenced the outcome, but more data or a different statistical test might have been needed to confirm this.
The Healthcare Provider Knows About Adolescents’ and Youths’ Concerns and Needs
Of the 357 respondents, 299 (83.8%) agreed, 35 (9.8%) disagreed, and 23 (6.4%) were unsure that healthcare providers were knowledgeable about adolescents’ and youths’ concerns and needs. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.26 and a standard deviation of .624. See Figure 5. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association existed between categorical variables. Results were:

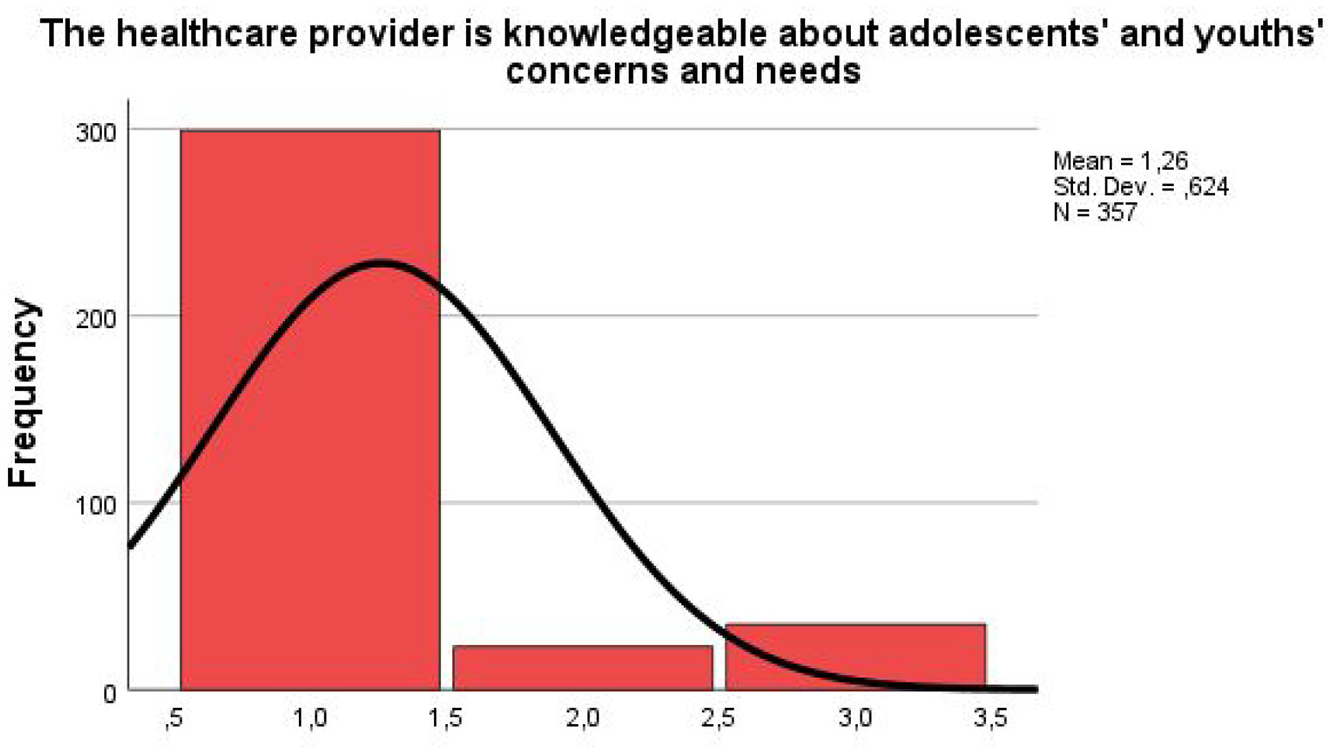
A positively skewed distribution curve of HCP’s knowledge about adolescents’ concerns and needs.
None of the sociodemographic traits showed a statistically significant relationship with the dependent variable because all p-values were greater than .05.
The Healthcare Provider Seemed Interested in What the Adolescent and Youth Had to Say
Out of 357 respondents, three quarters, 272 (76.2%), agreed, 60 (16.8%) disagreed, and 25 (7.0%) were unsure that healthcare providers showed interest in what the adolescent and youth had to say. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.41 and a standard deviation of .761. The Pearson Chi-Square Test (χ2) determined whether there was a statistically significant association between categorical variables. Results showed:

The Healthcare Provider Would Respect the Opinions and Decisions of Adolescents and Youth, Even if They Were Different from His or Hers
Of the 357 respondents, 242 (67.8%) agreed, 68 (19.0%) disagreed, and 47 (13.2%) were unsure that healthcare providers respected the opinions and decisions of adolescents and youth even if they were different from theirs. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.51 and a standard deviation of .795. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

None of the sociodemographic traits showed a statistically significant relationship with the dependent variable, as all p-values are greater than .05.
The Healthcare Provider Treats Adolescents and Youth in a Supportive and Considerate Manner
Out of 357 respondents, 289 (81.0%) agreed, 54 (15.1%) disagreed, and 14 (3.9%) were unsure that the healthcare providers treated adolescents in a supportive and considerate manner. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.34 and a standard deviation of .727. The Pearson Chi-Square Test (χ2) determined whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits showed a statistically significant relationship with the dependent variable, as all p-values are greater than .05.
The Point of Health Service Delivery Has Convenient Hours of Operation and Ensures Consultations Occur in a Short Waiting Time, With or Without an Appointment, and (Where Necessary) Swift Referral
The working days and hours of the health facility are convenient
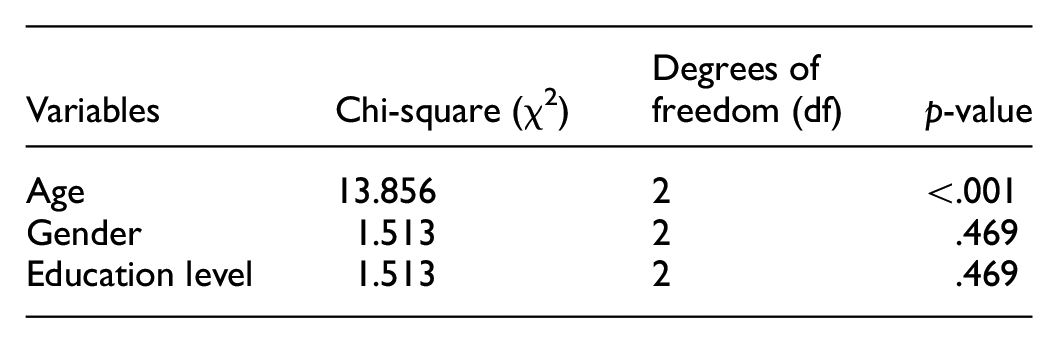
Of the 357 respondents, 254 (71.1%) agreed, 68 (19.0%) disagreed, and 35 (9.8%) were unsure that the working days and hours of the health facility were convenient. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.48 and a standard deviation of .795. The Pearson Chi-Square Test (χ2) was used to determine whether there was a statistically significant association between categorical variables. Results were:

Age had a statistically significant relationship with the dependent variable, meaning that age influenced the outcome. Gender and education level had no significant relationship, meaning gender did not influence the outcome.
The Waiting Times to See the Healthcare Provider Are Reasonable
Out of 357 respondents, 190 (53.2%) agreed, 149 (41.7%) disagreed, and 18 (5.0%) were unsure that the waiting time for consultation with the healthcare provider was reasonable. The descriptive statistics showed a symmetrical distribution since skewness was slightly positive (0 < skew < 1), with a mean of 1.89 and a standard deviation of .969. See the Figure 6. The Pearson Chi-Square Test (χ2) assesses whether there was a statistically significant association between categorical variables. The results were:

Denoting standard distribution curve of the waiting time for consultation.
Age was highly related to the dependent variable, strongly influencing the outcome. Gender and education level did not have significant relationships, meaning these variables did not influence the outcome.
The Healthcare Provider Turns Away Adolescents Who Visit the AYFHS Without an Appointment
Of the 357 respondents, 219 (61.3%) agreed, 73 (20.4%) disagreed, and 65 (18.2%) were unsure that the healthcare provider did not turn away adolescents who visit the AYFHS without an appointment. The descriptive statistics showed a symmetrical distribution distribution since skewness was slightly positive (0 < skew < 1), with a mean of 1.59. and a standard deviation of .808. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. The results were:
Gender and education level had statistically significant relationships with the dependent variable, meaning these factors influenced the outcome. Age had no significant relationship with the outcome.
The Healthcare Provider Explains Where Adolescents and Youth Are Referred and When to Go
Of the 357 respondents, 298 (83.5%) agreed, 40 (11.2%) disagreed, and 19 (5.3%) were unsure that the healthcare provider explained where adolescents and youth were referred and when to go. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.26 and a standard deviation of .624.
The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

Education level had a statistically significant relationship with the dependent variable, meaning education level influenced the outcome. Age and gender did not have significant relationships, meaning these factors did not influence the outcome.
The Point of Health Service Delivery Has an Appealing and Clean Environment
The Health Facility Is a Welcoming Place to Visit
Of the 357 respondents, 285 (79.8%) agreed, 60 (16.8%) disagreed, and 12 (3.4%) were unsure that the health facility was a welcoming place to visit. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.37 and a standard deviation of .755. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

None of the sociodemographic traits had statistically significant relationships with the dependent variable. This means there was no evidence to suggest that these factors influence the outcome in your study population.
The Surrounding Areas and the Health Facility’s Consultation Room/Examination Room Are Clean
Out of 357 respondents, 330 (92.4%) agreed, 17 (4.8%) disagreed, and 10 (2.8%) were unsure that the surrounding areas and the health facility’s consultation room/examination room were clean. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.12 and a standard deviation of .452. The Pearson Chi-Square Test (χ2) evaluated whether there was a statistically significant association between categorical variables. Results were:
Age had a statistically significant relationship with the dependent variable, meaning age influences the outcome. Gender and education level did not have significant relationships, so they did not influence the outcome.
The Point of Health Service Delivery Is to Provide Information and Education Through Various Channels
The Health Facility Has Informational/Educational Materials on Adolescent Health Topics
Of the 357 respondents, 300 (84.0%) agreed, 40 (11.2%) disagreed, and 17 (4.8%) were unsure that the facility had informational/educational materials on adolescent health topics. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.27 and a standard deviation of .651. The Pearson Chi-Square Test (χ2) determined whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits had statistically significant relationships with the dependent variable. This means there was no evidence to suggest that these factors influenced the outcome in this study population.
The Materials Contain Information That Is Useful, Easy, and Interesting to Read
Out of 357 respondents, 275 (77.0%) agreed, 68 (19.0%) disagreed, and 14 (3.9%) were unsure that the information contained was helpful, easy, and enjoyable to read. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.42 and a standard deviation of .791. The Pearson Chi-Square Test (χ2) evaluates whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits had statistically significant relationships with the dependent variable.
Adolescents and Youth Know the Reproductive Health Services Offered at This Health Facility
Out of 357 respondents, 253 (79.0%) agreed, 82 (23%) disagreed, and 22 (6.2%) were unsure that adolescents and youth knew the reproductive health services offered at the health facility. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.52 and a standard deviation of .843. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

No statistically significant relationships were found for age, gender, and education level.
Adolescents Are Actively Involved in Decision-Making Regarding Designing, Assessing, and Providing Health Services
Adolescents and Youth Contribute to Decisions About How Health Services Should be Delivered to Adolescent Clients
Out of 357 respondents, 181 (50.7%) agreed, 105 (29.4%) disagreed, and 71 (19.9%) were unsure that adolescents and youth contributed to decisions about how health services should be delivered to adolescent clients. The descriptive statistics showed a symmetrical distribution distribution since skewness was slightly positive (0 < skew < 1), with a mean of 1.79. and a standard deviation of .871. See Figure 7. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:
Normal distribution curve.
No statistically significant relationships were found for age, gender, and education level. However, education level was very close to statistical significance, suggesting a potential trend that may become significant with a larger sample size.
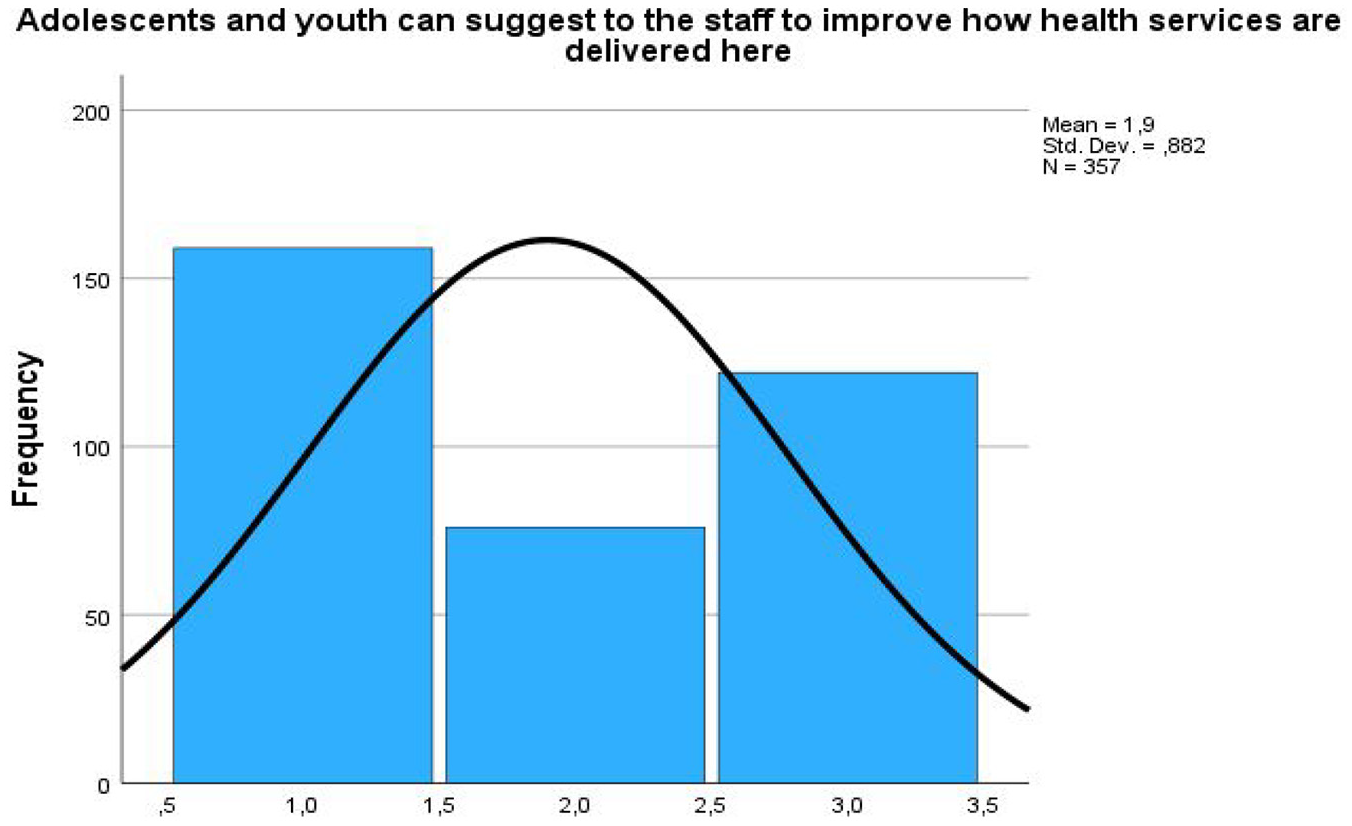
Adolescents and Youth Can Suggest How to Improve the Health Services Delivered to the Staff
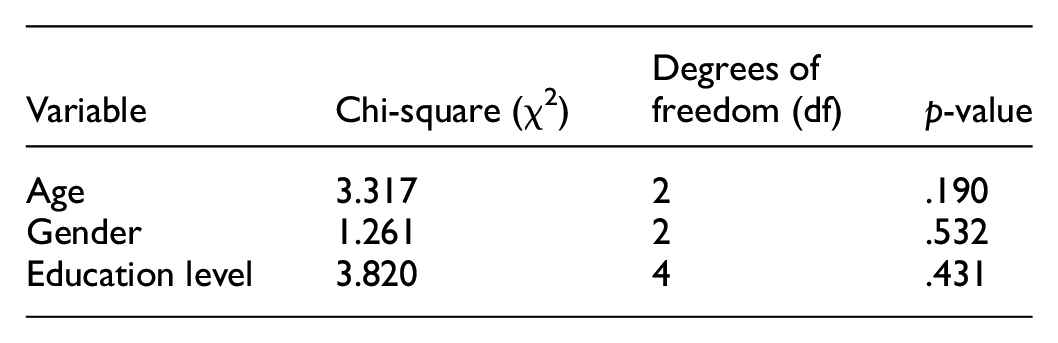
Of the 357 respondents, 159 (44.5%) agreed, 122 (34.2%) disagreed, and 76 (21.3%) were unsure that adolescents and youth suggested to the staff how to improve health services delivery. The descriptive statistics showed a symmetrical distribution distribution since skewness was slightly positive (0 < skew < 1), with a mean of 1.90. and a standard deviation of .882. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

No statistically significant relationships were found for age, gender, and education level. However, gender was relatively closer to significance, suggesting a possible trend that could become significant with a larger sample size or further analysis.
The Required Health Care Package Is Provided to Fulfil the Needs of All Adolescents, Either at the Point of Health Service Delivery or Through Referral Linkages
Adolescents and Youth Receive the Health Services They Need to Deal with Their Health Concerns or Problems
Of 357 respondents, 302 (84.6%) agreed, 29 (8.1%) disagreed, and 26 (7.3%) were unsure that the required health care package was provided to fulfil the needs of all adolescents either at the point of health service delivery or through referral linkages. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.24 and a standard deviation of .586. The Pearson Chi-square test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:
No statistically significant relationships were found for age, gender, and education level. This suggests that sociodemographic traits did not significantly affect the dependent variable in this study.
Adolescents and Youth Are Referred to Other Health Facilities for Health Services Not Available at This One
Of 357 respondents, 250 (70.0%) agreed, 67 (18.8%) were unsure, and 40 (11.2%) disagreed that adolescents and youth were referred to other health facilities for health services not available. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.41 and a standard deviation of .684. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant association exists between categorical variables. Results were:

Gender was significantly associated with the dependent variable. Age and education level did not show significant relationships.
Healthcare Providers Are Competent to Work with Adolescents and Provide the Required Health Services
The Information Provided to the Adolescents and Youth During the Consultation Is Clear and Helpful
Of 357 respondents, 328 (91.9%) agreed, 23 (6.4%), and 6 (1.7%) were unsure that the information provided to them during the consultation was clear and helpful. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.15 and a standard deviation of .504. The Pearson Chi-Square Test (χ2) determined if there was a statistically significant association between categorical variables. Results were:

Gender was significantly associated with the dependent variable. Age and education level were not significantly associated.
The Information Provided to Adolescents and Youth for Their Follow-Up Visit(s) Is Clear
Of 357 respondents, 320 (89.6%) agreed, 26 (7.3%) disagreed, and 11 (3.1%) were unsure that the information provided to adolescents and youth for their follow-up visit(s) was evident. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.18 and a standard deviation of .540. The Pearson Chi-Square Test (χ2) was used to examine whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits showed a statistically significant association with the dependent variable.
Adolescents and Youth Are Involved in Decision-Making Regarding Their Care After Receiving Adequate Information on Different Treatment/Treatment Methods
Of 357 respondents, 239 (66.9%) agreed, 73 (20.4%), and 45 (12.6%) were unsure that adolescents and youth were involved in care decisions after receiving adequate information on different treatment/treatment methods. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.54 and a standard deviation of .812. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant relationship exists between categorical variables. Results were:
None of the sociodemographic traits showed a statistically significant relationship. However, gender and education level were closer to significance, indicating a potential trend that may warrant further investigation.
Adolescents and Youth Are Given Their Preferred Treatment/Method of Contraception
Of 357 respondents, 137 (38.4%) agreed, 63 (17.6%) disagreed, and 157 (44.0%) were unsure that adolescents and youth were given their preferred treatment/method of contraception. The descriptive statistics showed a symmetrical distribution distribution since skewness was slightly positive (0 < skew < 1), with a mean of 1.79. and a standard deviation of .720. The Pearson Chi-Square Test (χ2) assessed whether a statistically significant relationship exists between categorical variables. Results were:

There was a significant correlation between education level and the dependent variable. Age and gender did not show statistically significant relationships with the dependent variable. The findings indicate that education level may influence the outcome, while age and gender might not.
Healthcare Providers Dedicate Sufficient Time To Work Effectively with Their Adolescent Clients
Adolescents and Youth Are Given Enough Time to Discuss Their Issues Related to Sexual and Reproductive Health
Out of 357 respondents, 252 (70.6%) agreed, 76 (21.3%) disagreed, and 29 (8.1%) were unsure that enough time was given to them to discuss their issues related to sexual and reproductive health. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.51 and a standard deviation of .823. The Pearson Chi-Square Test (χ2) examined whether a statistically significant association exists between categorical variables. Results were:

None of the sociodemographic traits showed a statistically significant association with the dependent variable.
The Healthcare Provider Answers Adolescent and Youth Questions Relaxedly
Of 357 respondents, 274 (76.8%) agreed, 67 (18.8%) disagreed, and 16 (4.5%) were unsure that the healthcare provider answered adolescent and youth questions relaxedly. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.42 and a standard deviation of .788. The Pearson Chi-Square Test (χ2) examined whether there was a statistically significant association between categorical variables. Results were:

None of the sociodemographic traits showed a statistically significant association with the dependent variable.
The Point of Health Service Delivery Has the Required Equipment, Supplies, and Essential Services Necessary to Deliver the Required Health Services
The Point of Health Service Delivery Has the Equipment, Supplies, and Essential Services Necessary to Deliver the Required Health Services
Of 357 respondents, 231 (64.7%) agreed, 65 (18.2%) were unsure, and 61 (16.9%) disagreed that the point of health service delivery had the required equipment, supplies, and essential services necessary to deliver the required health services. The descriptive statistics showed a positively skewed distribution curve as the values for skewness were >1, with a mean of 1.52 and a standard deviation of .770. The Pearson Chi-Square Test (χ2) was used to determine if there was a statistically significant association between categorical variables. Results were:
None of the sociodemographic traits showed a statistically significant association with the dependent variable.
Tables 2 and 3 summarise the frequencies for adolescent perception on accessing the AYFS and descriptive statistics of variables, respectively.
Frequency Table for Adolescents’ Perceptions on Accessing Adolescent and Youth-Friendly Health Services.
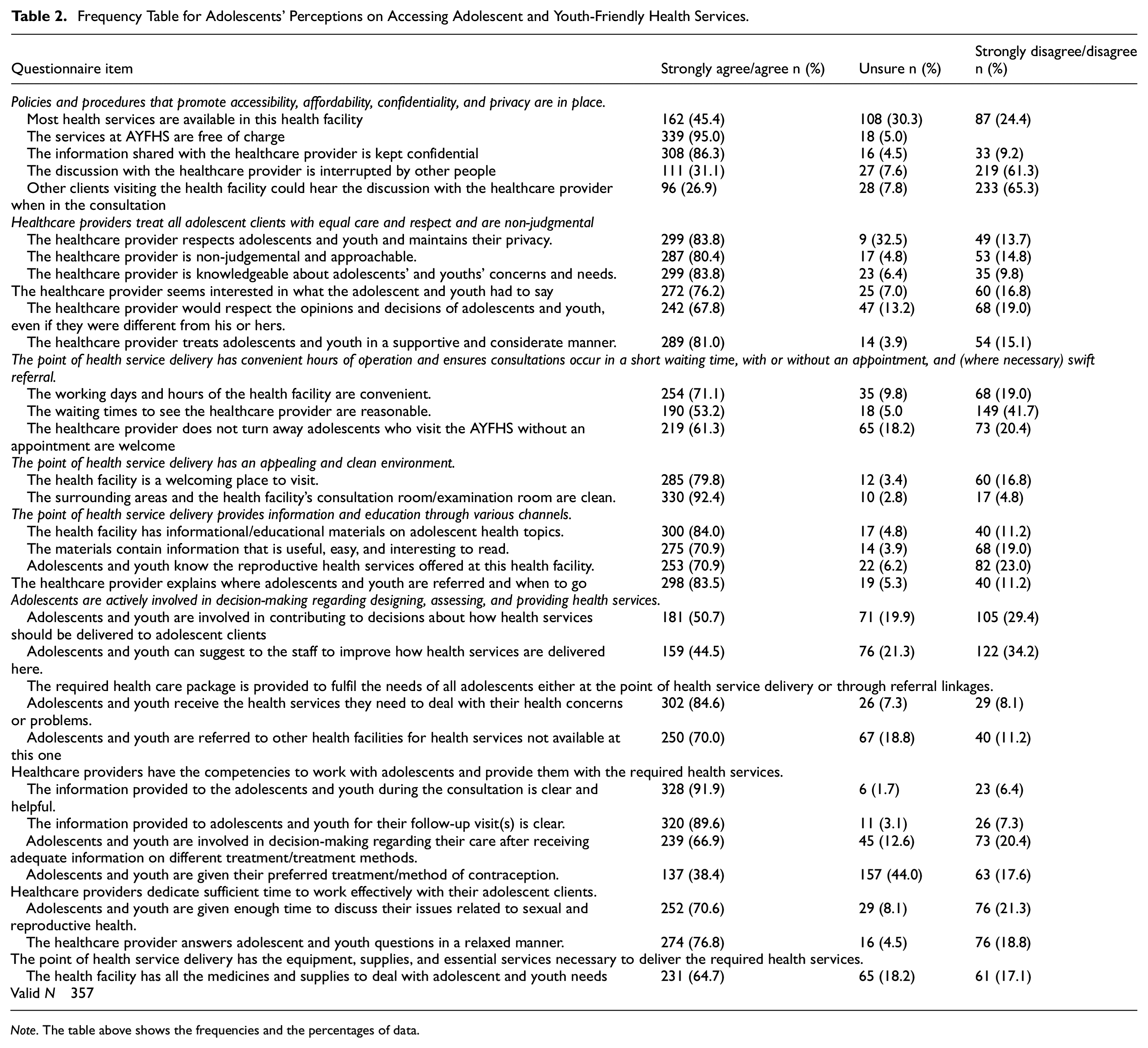
Note. The table above shows the frequencies and the percentages of data.
Descriptive Statistics of Variables.

The table above of descriptive statistics shows the mean, standard deviation and skewness of the variables.
Standard deviation (σ).
Discussion
The adolescents in this study perceived the AYFS as adolescent-friendly. This was because the adolescents reported that some policies and procedures promoted accessibility, affordability, confidentiality, and privacy were in place. The services for the AYFS were found to have most packages of services, services offered at no cost, the consultation room provided auditory privacy, and confidentiality was maintained. This was consistent with the Swedish and El Salvador studies, in which adolescents and youth perceived AYFS as friendly (Granados Castro & García Sura, 2024; Thomson et al., 2022). The adolescents in Sweden identified accessibility, safety, privacy, respect, and a holistic and empowering approach as significant characteristics of youth friendliness (Thomson et al., 2022). The El Salvador adolescents reported that the HCPs displayed respect, trust and privacy. This aligns with the study conducted in Mexico, which indicated that exclusive AYFS provided more suitable and welcoming services (Pastrana-Sámano et al., 2020). The HCPs in Mexico were found to be respectful. This was in line with other literature from Sweden, Mexico and Kenya. Where free services promoted access (Nyaga et al., 2023; Pastrana-Sámano et al., 2020; Thomson et al., 2022). Adolescent services are considered more likely to be used if they are free or low-cost.
The Global standard about facility characteristics outlines that the facility should maintain privacy and confidentiality. To adolescents’ lack of privacy and confidentiality is viewed as a barrier to service utilisation. Maintaining privacy and confidentiality is viewed as a facilitator for adolescents and youth to utilise the AYFS. According to Dayal and Gundi (2022), a lack of privacy results in distrust of the HCPs. These results are comparable to the Nepal and Sweden studies, where the HCPs maintained confidentiality, and adolescents claimed that the service’s secrecy was why they kept using it (Napit et al., 2020; Thomson et al., 2022). The findings correspond with existing literature from Malawi, which indicates that HCPs exhibit friendliness, warmth, understanding, approachability, and respect for privacy and confidentiality (Barden-O’Fallon et al., 2020).
This study found that HCPs treated all adolescent clients with equal care and respect and were non-judgmental. This may have been because the respondents reported that the HCPs were respectful, non-judgemental, supportive, attentive and knowledgeable about adolescents’ concerns and their opinions and decisions were appreciated. This corresponded with the El Salvador study, where respect, trust, and privacy provided by HCPs were rated high (Granados Castro & García Sura, 2024). These findings concur with other pieces of literature from India, Malawi and Sweden, where HCPs were reported to be respectful, non-judgemental and treated adolescents as adults (Dayal & Gundi, 2022; Sibande & Malapela, 2024; Thomson et al., 2022). A positive attitude of HCPs plays a crucial role in adolescents’ decision-making about accessing the AYFS. An AYFS where HCPs are non-judgemental, approachable and friendly are likely to be accessed by adolescents. The opposite was true. Where HCPs display a terrible attitude toward adolescents, that facility is likely to be underutilised. Adolescents want to be understood and respected to feel comfortable communicating their issues. HCPs engaged in AYFS must receive specialised training to effectively address adolescents’ varied concerns. HCPs must engage in continuous professional development to remain informed about new advancements, ensuring their knowledge and competence in effectively addressing adolescents’ needs.
This study reported that the AYFS had convenient working days and hours, reasonable waiting times, and no appointment needed. The healthcare provider explained where adolescents and youth were referred and when to go. These findings also coincided with the Malawian study reflecting adolescents’ satisfaction with working days and operating hours (Sibande & Malapela, 2024). The results coincided with the literature from Mexican and Ghana, where the waiting time was reasonable except on certain occasions (Kpiinfaar et al., 2024; Kumah et al., 2024; Pastrana-Sámano et al., 2020). In this study, the respondents’ satisfaction with the waiting time might have been because adolescents in school uniforms are fast-tracked. Accessibility to the AYFS was marked by convenient operating hours, shorter waiting times with or without appointments, and swift referrals. Implementing flexible operating hours tailored to adolescents’ schedules makes it easier for adolescents to access services. Adolescents during the day are most likely to be at school or work, and if operating hours coincide with school and working hours, they will not be able to access the services. This was supported by Australian literature, where adolescents preferred appointment times outside of school hours (Turner et al., 2017). Operating after hours and during the weekend will mostly be acceptable to adolescents, and services will be utilised. The results contrast those from North-Western Nigeria, Nepal and Sweden, where the operation and school hours were aligned (Napit et al., 2020; Nmadu et al., 2020; Thomson et al., 2022).
The respondents from this study noted that the AYFS was welcoming, and the surrounding areas and the consultation room/examination room were clean. This coincided with the results from a study in Malawi, where the adolescents were satisfied with the cleanliness of the environment of the health facility (Sibande & Malapela, 2024).
This study found that The AYFS had informational/educational materials on adolescent health topics, and they had knowledge of SRHS. These findings aligned with literature from Ghana, where information on SRH was available and very useful (Kpiinfaar et al., 2024; Kumah et al., 2024). This finding could be due to the availability of outreach programmes that increase awareness and knowledge, thus improving access to AYFS. This was consistent with the findings from Northern Ethiopia, Ghana and Malawi, where adolescents utilised the service because of the prior knowledge of SRHS offered (Abdurahman et al., 2022; Kpiinfaar et al., 2024; Sibande & Malapela, 2024). Access and utilisation of the AYFS are determined by knowledge of SRHS offered. Knowledge and awareness of the AYFS and services offered facilitate the adolescents’ access to and utilisation of health services. Facilitating access to health information is crucial for enhancing the global health information system (Muscat et al., 2025). In the present study, what may have contributed to the adolescent being knowledgeable about SRH was their increased age and that they may have experienced SRH needs. In the Ethiopian study, the adolescents were much younger, and even though they might have experienced SRH needs, they lacked SRH literacy and also feared stigmatization (Sidamo et al., 2024).
Meaningful youth participation is one of the guiding concepts in delivering critical SRHR programs. This principle requires adolescents to participate in decision-making. This coincides with the current findings, where the respondents indicated that they contributed to how the AYFS were delivered and were allowed to suggest how service delivery can be improved. These results correspond with the scoping review, in which youth engagement at all levels of an organization was found to be a core component of youth-friendly services (Hawke et al., 2019). These findings align with another South African study, where government sectors enabled youth participation (Jacobs & George, 2022).
The respondents in this study indicated that the HCPs dedicated sufficient time during the consultation and were relaxed when answering questions. This was consistent with Sweden and Malawi studies, where adolescents stated that HCPs listened to youth during consultations (Sibande & Malapela, 2024; Thomson et al., 2022). The findings align with those observed in Australia, where adolescents appreciated practitioners who refrained from using medical jargon, actively listened, provided assurances regarding confidentiality, and respected their perspectives and choices (Turner et al., 2017). This was in line with studies conducted in Mexico, Switzerland, Italy and Germany, where HCPs appreciated and paid attention to their adolescents’ suggestions (Granados Castro & García Sura, 2024; Wangmo et al., 2019). The findings align with those observed in Northern Sweden, where healthcare professionals were regarded as motivated, engaged, and knowledgeable about youth. The clinics prioritise confidentiality and adopt a youth-centred, holistic approach (Thomée et al., 2016). These findings contradicted the Ghana study, which indicated that the HCPs did not respect the adolescents’ viewpoints (Abuosi & Anaba, 2019)
Strengths and Limitations
This research’s strength was that it was population-based and used the probability sampling method. Respondents were chosen randomly using a simple random sampling technique to provide a representative sample of participants in the study area. This manuscript was part of a doctoral study. The adolescents in this study had positive perceptions of accessing the AYFS. This was facilitated by the availability of policies and procedures promoting accessibility, affordability, confidentiality, and privacy.
This study was limited to eliciting only the respondents’ perceptions regarding access to the AYFS within the selected health district. No follow-up was conducted to assess their experiences with the AYFS. The Respondents may have exhibited social desirability bias by providing answers they perceived as expected rather than reflecting their genuine experiences. This was reflected by the respondent’s perceptions, which contradict the prevalence of unplanned pregnancies and STIs, including HIV, among adolescents in this health district. Information bias was possible as the respondents might have given more or less information based on a Likert scale. Acquiescence bias was also possible since most respondents only select positive answer choices.
Conclusion
This study revealed that adolescents’ perceptions of accessing the AYFS were generally good. The AYFS provided the necessary package of services, whether onsite or offsite, through referral. The services were accessible to adolescents as they were free, provided by HCPs with a positive attitude and privately and confidentially. However, the adolescents’ perceptions do not tally with the prevalence of unplanned pregnancies and STIs, including HIV occurrence among adolescents in this health district. Some study variables had a small majority, which means that other respondents disagreed with the statement, and others were unsure of the variable.
Recommendations
The results of this study call for a more proactive approach to implementing outreach programmes to create awareness about the AYFS. This can be done through health promotion activities that increase access to information and knowledge of ASRH services offered in the AYFS, thus promoting adolescents’ access and utilisation of services. Given that the adolescents’ perceptions of being actively involved in decision-making regarding designing, assessing, and providing health services had the lowest average, the health facilities should involve adolescents in the organisation’s structures so that they can discuss issues that impact their health. It is recommended that further studies should conducted at a broader scale and involving a different research approach.
Further studies are recommended that could address the issue of acceptability and efficiency of the AYFS as the contribution to why outcomes of the implemented services remain negative when the adolescent perceives the input and the process as good.
Significance of the study
This study examined adolescents’ perceptions regarding access to AYFS within the eThekwini health district. The results advance our knowledge of AYFS’s accessibility, affordability, availability, and suitability for addressing adolescents’ concerns. This indicated that the AYFS had effectively been implemented with appropriate structural and process measures for service provision. The positive perceptions exhibited by the respondents in this study reflect this finding.
The significance of the study was that South Africa has made significant strides toward achieving Sustainable Development Goal (SDG) 3.7, which aims to ensure universal access to sexual and reproductive healthcare services by 2030. The study found that SRH services were available, affordable, acceptable and accessible for all, including adolescents, rural populations, and people with disabilities.
Footnotes
Acknowledgements
Gatekeepers and all the respondents from the four Community Health Centers and eight Primary Health Care clinics within the eThekwini health district. Prof. Dagmar M. Haller and Dr Boersema for permitting the use of the questionnaire.
Ethical Considerations
The study received ethical approval from the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal (HSSREC/00004775/2022) and the KwaZulu-Natal Provincial Department of Health (NHRD Ref: KZ_202212_014). A written informed consent was obtained from those who agreed to participate in the study.
Consent for Publication
All authors have received a final version of this manuscript and provide consent for its publication.
Author Contributions
PPK contributed to the project’s conceptualisation, study design, data collection, data analysis, drafting and editing of the manuscript. SWM contributed to the study design, data analysis, and manuscript editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This manuscript is submitted in partial fulfilment of the requirements for a PhD at the University of KwaZulu Natal.
Data Availability Statement
All data generated and analyzed during the current study are included in this manuscript. The current study’s data are available from the corresponding authors upon reasonable request.