
Abstract
The COVID-19 pandemic exposed frontline healthcare workers (HCWs) to mental health problems and various challenges that impacted their job satisfaction. We explored the job satisfaction and psychosocial/mental well-being of COVID-19 frontline HCWs in Uganda. This was a mixed-methods study conducted at Mulago National Referral Hospital (MNRH), Entebbe Regional Referral Hospital (ERRH), and Uganda Virus Research Institute (UVRI). A pre-tested self-administered questionnaire and Four Focus Group Discussions (FGDs) were used for data collection. A five-point Likert scale was used for the quantitative data to measure mental well-being and job satisfaction. Bloom’s cut-off was used to categorize participants’ job satisfaction and mental well-being into good (≥80%), moderate (60% - <80%), and poor (<60%). FGDs were audio-recorded, transcribed, and analyzed thematically using NVivo version 12 software. 218 participants participated in the quantitative survey and 24 of them further participated in the FGDs. 51.4% (n = 112) were males, aged 18 to 39 years (77.5%, n = 169) and 50.9% (n = 111) were at MNRH. Overall, 54%, 28%, and 18% of the participants reported moderate, good, and poor job satisfaction respectively. Satisfaction with salary (2.6 ± 1.2) and compensation (risk) allowances (2.4 ± 1.3) was particularly low. Furthermore, 35%, 33%, and 32% of the participants reported moderate, good, and poor mental well-being respectively. Anxiety, burnout, stigma, and discrimination contributed to poor psychosocial/mental well-being. Less than half of the frontline HCWs reported good job satisfaction and psychosocial/mental well-being. There is a need for prioritization of the psychosocial well-being of frontline HCWs, in addition to improvement of remuneration systems.
Plain language summary
During the COVID-19 pandemic, healthcare workers risked their lives to save others. We investigated the mental well-being and job satisfaction of frontline healthcare workers (HCWs) in Uganda working in COVID-19 Treatment Units at Mulago National Referral Hospital (MNRH), Entebbe Regional Referral Hospital (ERRH), and Uganda Virus Research Institute (UVRI). Our study found that less than half of the HCWs working in the COVID-19 treatment units reported good job satisfaction. Many were dissatisfied with their salary and compensation (risk) allowances. Additionally, nearly one third of HCWs experienced low psychosocial/mental well-being, which was linked to fear, anxiety, stress, burn-out, stigma, and discrimination. We also found that better job satisfaction was associated with improved psychosocial well-being. Therefore, it is crucial to prioritize the mental well-being of frontline healthcare workers and enhance their pay systems.
Introduction
Coronavirus disease 2019 (COVID-19) was first identified in Wuhan City, China in December 2019 and described as a disease characterized by rapid transmission from one person to another (Wu et al., 2020; Zhou et al., 2020). To mitigate its quick spread, the World Health Organization (WHO) declared COVID-19 disease as an international public health emergency at the beginning of February 2020, requiring all countries to join efforts in the fight against this disease (Tang et al., 2020). After the first case of COVID-19 was confirmed in Uganda on March 21, 2020, the number of confirmed cases increased to 212 by May 21, 2020, (Migisha et al., 2020) and to 40751 by April 02, 2021(Ministry of Health, 2021). The rapidly increasing number of cases in the country, in addition to the widespread global reports about Healthcare workers (HCWs) who had contracted the disease and died, potentially exposed Uganda’s HCWs to psychological distress and threatened their devotion to the fight against this disease (Bandyopadhyay et al., 2020; Moorthy & Sankar, 2020)
Healthcare workers are vital to the effective control and management of pandemics (Ives et al., 2009). They were reference points for citizens as to how best the pandemic could be contained (Wang et al., 2020). Healthcare workers who were directly involved in the diagnosis, treatment, and care of patients with COVID-19 were predisposed to mental health problems including anxiety, distress, depression, insomnia, anger, and fear (Xiong & Peng, 2020). These mental health challenges among frontline HCWs negatively impacted healthcare provision further compounding the pandemic’s strain on health systems (Maliwichi et al., 2024). The high prevalence of mental health problems among frontline HCWs could be attributed to occupational stressors which include overwhelming workload, long working hours, manpower shortages, lack of specific drugs and medical equipment, lack of personal protective equipment (PPE), fear of infection, exposure to patient suffering and death, and inadequate support systems. Concerns about the health of self and that of their families, the potential discrimination or stigma associated with the disease, isolation, separation from families, physical violence, and loss of life, are all contributors to the poor mental well-being of frontline HCWs (Maliwichi et al., 2024; Muzyamba et al., 2021; Xiong & Peng, 2020). Both immediate and prolonged consequences of the pandemic on the mental health of HCWs are irrefutable. However, at the time of this study, the mental well-being of frontline HCWs was of little focus in Uganda.
Job satisfaction is defined as a pleasing or positive emotional situation resulting from the appraisal of one’s job experience (Diakos et al., 2022). Job satisfaction of frontline healthcare workers is directly associated with better control of major health crises (Yu et al., 2020). Previous studies conducted in the earlier Severe Acute Respiratory Syndrome (SARS) outbreak in 2003 and the influenza pandemic in 2004/2005 revealed that HCWs reported reluctance to work, contemplated resignation and many were less likely to report to duty (Bai et al., 2004; Balicer et al., 2006). Considering the sudden outbreak and the rapid increases in the number of COVID-19 cases, frontline HCWs were faced with intense workloads, higher risks of infections, and heavier physical and mental stresses which threatened their job satisfaction (Yu et al., 2020). In China, to ensure that frontline HCWs were motivated enough to participate in the control of the pandemic, the National Health Commission of the People’s Republic of China issued the “Notice on Providing Full Security for Frontline HCWs and their Families.” This was intended to support the security, psychological, and other needs of frontline HCWs and their families; and positive outcomes were observed following this intervention (Yu et al., 2020). Based on the experiences in China, evaluating the level of job satisfaction and intervening appropriately is key to maintaining high-level health services during pandemics.
Despite the impact of the pandemic on healthcare workers’ mental well-being and job satisfaction, there were hardly any studies evaluating the effect of the pandemic on Uganda’s COVID-19 frontline HCWs, at the time we conducted this study. Therefore, this study aimed to explore the mental well-being and job satisfaction of frontline healthcare workers in Uganda during the COVID-19 pandemic.
Methods
Study Design
A descriptive cross-sectional survey using mixed-methods sequential exploratory study design was conducted from 20th July 2020 to 23rd October 2020.
Study Site and Setting
The study was carried out in two COVID-19 treatment facilities and one COVID-19 testing facility. The treatment facilities were Mulago National Referral Hospital (MNRH) and Entebbe Regional Referral Hospital (ERRH), and the testing facility was the Uganda Virus Research Institute (UVRI). Both MNRH and ERRH were the main referral centres for the management of complicated COVID-19 cases in Uganda.
ERRH is in Entebbe town, Wakiso District, approximately 44 km by road, southwest of MNRH. MNRH is the main national referral hospital located in Kawempe Division, Kampala district. Each of the two hospitals had over 150 healthcare workers involved directly or indirectly in the management of COVID-19 disease. UVRI is the national reference laboratory for viral diseases and is one of the mandated centres for validating COVID-19 diagnostics and providing external quality assurance.
Study Population
We recruited healthcare workers (medical doctors, nurses, laboratory personnel and pharmacists) who were directly involved in the management of COVID-19 cases in ERRH, MNRH and UVRI.
Sampling
Quantitative Survey
We enrolled all HCWs actively working in the COVID-19 treatment units of the selected health facilities in the study. The HCWs were enrolled based on their availability before their daily work shift, to prevent COVID-19 transmission to the study team.
Inclusion and Exclusion Criteria
○ Healthcare workers that were 18 years and above, and actively managing COVID-19 patients in the selected facilities.
○ Healthcare workers who were severely ill were excluded from participating in the study.
Qualitative Survey
Healthcare workers were informed about the Focus Group Discussions during the Quantitative part of the study. Those who were willing to participate were then scheduled for the FGDs. Six participants were recruited per FGD, and these discussions were carried out until data saturation was reached.
Data Collection
Quantitative Data Collection
A self-administered questionnaire was used to collect this data. The questionnaire was pretested among 10 HCWs at Kiruddu National Referral Hospital (KNRH), a COVID-19 treatment site. Irregularities were reviewed by an infectious disease specialist at the Infectious Disease Institute at Makerere University and addressed before the final version of the questionnaire was approved. Data from the pre-testing exercise was not included in the final data set.
The questionnaire was divided into three sections:
(i) Nine questions on socio-demographic characteristics.
(ii) Twelve questions on job satisfaction; These questions were adopted from the study done by Hagopian et al. (2009) and were modified accordingly to suit the COVID-19 scenario.
(iii) Five questions assessed mental well-being. These questions were adopted from the World Health Organization mental well-being index (Topp et al., 2015).
Six questions assessed stigma. These questions were developed based on three aspects; discrimination, acceptance, and fear, which were adopted from the study done by See et al., (2011) and were modified accordingly to fit the COVID-19 scenario.
Qualitative Data Collection
We conducted 4 Focus Group Discussions (FGDs) to explore the opinions and experiences of the frontline HCWs. Each FGD comprised six participants; each group was made up of either only doctors, nurses, laboratory personnel or pharmacists. Additionally, each group consisted of participants from both ERRH and MNRH. The investigators underwent training before conducting the FDGs. Consent was sought from the participants before audio-recording these sessions. The discussions which were 60 min long were all moderated by NT using a topic guide (Appendix 1) and notes were taken by AG. The FGDs were conducted until data saturation was reached. The audio recordings were later transcribed verbatim and cross-checked by another member of the team for completeness and accuracy.
Data Analysis
Quantitative Data
Data was entered into Google Forms and exported to Microsoft Office 2019 for cleaning and coding. All analyses were performed using STATA 15.0 (StataCorp LLC, College Station, Texas, USA). Categorical variables were summarized as frequencies and percentages whereas numerical variables were summarized as mean and standard deviation. Responses to questions on job satisfaction scores were coded as; strongly disagree-1, disagree-2, neutral-3, agree-4, and strongly agree-5. For mental well-being, responses were coded as; not at all-1, less than half of the time-2, more than half of the time-3, most of the time-4, and all of the time-5. Job satisfaction and mental well-being scores were calculated for each participant by summing up scores for individual items on both scales and converted into percentages. Bloom’s cut-off was used to categorize participants into good (≥80%), moderate (60% - <80%), poor (<60%) job satisfaction, and mental well-being.
Multiple linear regression analysis was used to assess the association between overall job satisfaction and mental well-being, and the socio-demographic variables. Assumptions for multiple linear regression (Linearity, existence of a relationship, independence, normality, and homoscedasticity) were first tested and found to be fulfilled. Multicollinearity was assessed using correlation coefficients (r > 0.7). Outliers were assessed using dfbetas and Cooks’ distance, and none was greater than 0.5. Results were presented as unadjusted and adjusted coefficients, 95% confidence intervals, and p-values. A p-value < .05 was considered statistically significant. Pearson’s correlation was used to assess the correlation between job satisfaction scores and psychosocial/mental well-being scores.
Qualitative Data
Data was organized and managed using Nvivo software Version 12. Thematic and content analysis was also done using Nvivo software version 12. The initial codebook was developed by AT after carefully analyzing the text, line-by-line in each transcript through open coding. AT assigned codes to relevant segments of the text, and similar or related codes aggregated to form themes. Themes/codes were derived in relation to the research questions/objectives and literature. A narrative was generated from the dominant themes. Some quotes were used to represent the narrative.
Results
Quantitative Data
Demographic Characteristics of Participants
Of the 218 COVID-19 frontline healthcare workers who participated in the study, 51.4% (n = 112) were males, aged 18 to 39 years (77.5%, n = 169). Slightly more than half of the HCWs were working at MNRH (50.9%, n = 111) and the majority (33.0%, n = 72) were nursing officers. Additionally, 34.4% (n = 75) of the participants had a 2–4 years’ level of experience (Table 1).
Socio-demographic Characteristics of the Participants.

Job Satisfaction of Frontline Healthcare Workers
Overall, 54%, 28%, and 18% of the HCWs had moderate, good, and poor job satisfaction, respectively. Most of the participants strongly agreed or agreed that they had received adequate training to manage COVID-19 patients (89.0%, n = 194), had the flexibility to balance the demands of work and personal life (80.7%, n = 176), and that compensation (risk) allowances were important (85.8%, n = 187). Satisfaction with salary (2.6 ± 1.2) and compensation (risk) allowance (2.4 ± 1.3) was particularly low (Table 2).
Job Satisfaction Among Healthcare Workers During the COVID-19 Pandemic.

From the multiple linear regression statistical model, frontline HCWs who worked as volunteers had higher job satisfaction (r = 8.6, 95%CI: 3.9–13.3, p < .001) compared to the permanently employed. In addition, participants on short-term contracts had better job satisfaction (r = 5.4, 95%CI: 1.5–9.2, p = .006) as compared to the permanently employed (Table 3). The adjusted R2 for this model was 0.49, indicating that the model explained 49% of the variability. The regression model was highly significant, F (10, 207) = 128.99, p < .001. The bigger values of the dependent variables indicate higher job satisfaction.
Multiple Linear Regression Analysis of Socio-demographic Variables Associated With Job Satisfaction Among COVID-19 Frontline Healthcare Workers.

The bigger values of the dependent variables indicate higher job satisfaction.
Adjusted R2 = 0.49, F (10, 207) = 128.99, p < .001.
Mental Wellbeing of Frontline Healthcare Workers
More than half of the participants felt cheerful and in good spirits (61.5%, n = 134), and calm and relaxed (52.3%, n = 114) most of the time or all the time. Less than half of the health workers woke up feeling fresh and well-rested (43.1% n = 94) and had their daily lives filled with things that interested them (46.3%, n = 101; Table 4). Overall, 33%, 35%, and 32% of the health workers had good, moderate, and poor mental well-being, respectively.
The Mental Well-being of Frontline Healthcare Workers During the COVID-19 Pandemic.

From the multivariate linear regression statistical model, advanced age (60 years and above) was negatively associated with mental well-being (r = −39.9, 95% CI: −62.1 to −7.7, p = .012). Frontline HCWs on short-term contracts had better mental well-being (r = 6.3, 95% CI: 0.4–12.3, p = .036) as compared to those on permanent employment (Table 5). The adjusted R2 for this model was .64, indicating that the model explained 64% of the variance. The regression model was highly significant, F (10, 207) = 161.26, p < .001. The bigger values of the dependent variables indicate higher job mental well-being.
Multiple Linear Regression Analysis of Socio-demographic Variables Associated With Mental Well-being Among Frontline Healthcare Workers.

The bigger values of the dependent variables indicate higher job psychosocial well-being.
Adjusted R2 = 0.64, F (10, 207) = 161.26, p < .001.
Relationship Between Job Satisfaction and Mental Well-being of Frontline HCWs
Job satisfaction had a positive correlation with the mental well-being of frontline healthcare workers (Pearson’s rho: 0.487, P < .0001, N = 218). Participants with high job satisfaction scores had higher mental well-being scores (Figure 1).
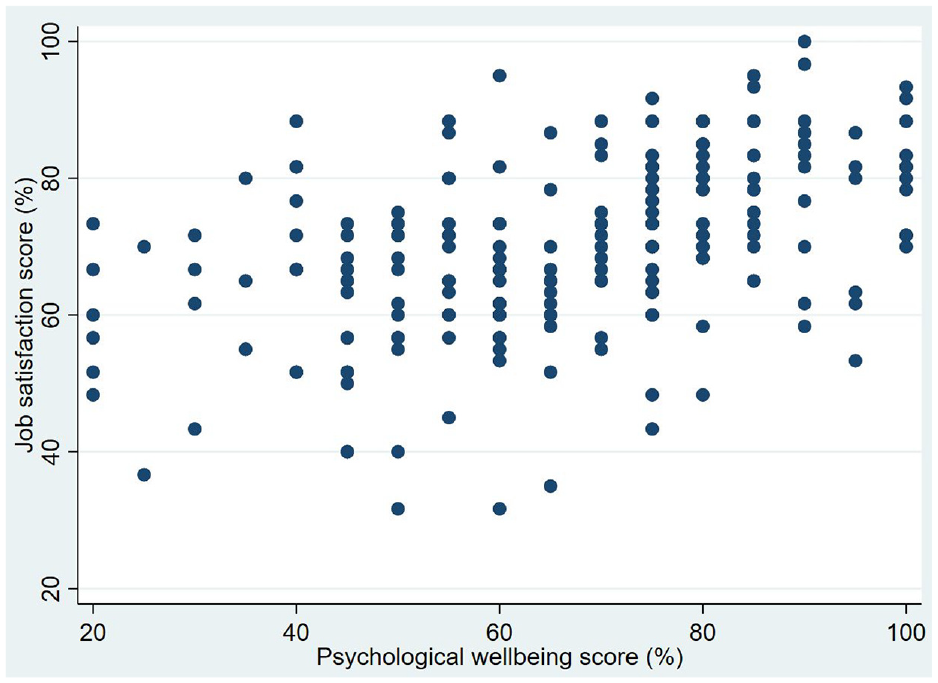
Correlation of mental well-being and job satisfaction among frontline healthcare workers.
Stigma Among COVID-19 Frontline Health Workers
More than half of the participants (67.9%, n = 148) strongly agreed or agreed that they “have not had trouble from people because they manage COVID-19 patients or test people for COVID-19.” However, nearly half (49.6%, n = 108) of the participants strongly agreed or agreed that they “worry about telling people that they manage or test for COVID-19” (Table 6).
Stigma-related Experiences Among COVID-19 Frontline Healthcare Workers.

Qualitative Data
From the FGDs held, four major themes were obtained:
Frontline Healthcare Workers’ Attitudes Toward Managing COVID-19 Patients
Frontline HCWs in all four FGDs comprised of contract and permanent staff. These included doctors, nurses, pharmacists and laboratory personnel. Some respondents expressed a positive attitude toward the treatment of COVID-19 patients. They felt obliged to treat these patients, despite the stressful circumstances they were experiencing during the pandemic:
When we finish our studies, we swear the Hippocratic Oath that we must serve. We are supposed to attend to these patients. That’s our job. (M4)
Some patients expressed gratitude and appreciation toward the frontline workers which motivated them to continue serving them. The HCWs felt that their efforts were recognized and valued:
Sometimes patients recognize the job well done and are very thankful. These complements are reminders that what we’re doing is relevant and being appreciated. (E2)
Psychosocial Challenges
Respondents were anxious about and afraid of contracting COVID-19 while managing these patients especially at the beginning of the pandemic. They often read reports about several people succumbing to this disease in other countries like Italy. However, this fear and anxiety reduced over time:
At first, you could find that when I sneeze, I’m like, this must be COVID. But I managed to overcome this fear. (M6)
Some respondents were also afraid of infecting family members and neighbors with COVID-19. As a result, they had to temporarily stay away from their family and neighbors who also commonly expressed their fear of interacting with the frontline HCWs.
When my family got to know that I was going to be in the COVID-19 treatment centre, they were scared that I might infect them with the disease. As a result, I got somewhere else to stay in the meantime, to avoid mixing with my family members. (M2)
Respondents reported experiencing stress, exhaustion, and burn-out due to heavy workload and long working hours, without day-offs:
You may be burnt out yet there’s no one to leave on station, so it psychologically tortures you. You find you have an off, but you can’t even get to enjoy it because you’d be punishing a patient. (E22)
Some respondents suffered stigma and discrimination that were associated with taking care of COVID-19 patients. They reported that community members and neighbors kept away from frontline workers.
Stigma was very apparent in the first days when the disease was quite novel and the breaking news about the disease was very precarious. When getting transportation to work and your drop off was Mulago, they would leave you behind if you identify as a health worker in Mulago. (M3)
The children of one of the participants were isolated from others because their parent was a COVID-19 Frontline Healthcare worker.
At home, people started ignoring me. They also started ignoring my child by not allowing her to play with their children. (E5)
Barriers to Job Satisfaction
The inadequate medical supplies and equipment made it difficult for the HCWs to handle the unexpectedly overwhelming numbers of patients. Additionally, limited bed space and lack of ventilators in the ICU were also reported as challenges by some of the participants:
I think COVID-19 exposed the gap in Uganda’s health system. Before COVID-19, there were like probably close to 200 active ICU beds in the country, including those in private facilities. (E5)
Many of the respondents reported poor availability of PPE. This affected their commitment to the management of COVID-19 patients as it was not practically possible for them to enter COVID-19 treatment rooms or touch a patient without PPE. They mentioned that they also did not want to be infected with COVID-19.
For example, when I come and there is no PPE, I cannot dare enter those treatment rooms. For me to work, PPEs must be there. I take it that my life comes first, and other things come later. (M1)
Frontline workers were also challenged by the frequent drug stock-outs. Furthermore, most of the drugs were not on the essential drug list and outsourcing was very difficult:
I work in the pharmacy department. There are some drugs the national referral doesn’t have on their essential drug list. However, they are prescribed by the doctors, so because of that as the pharmacy department, we are tasked to get medication from outside. Outsourcing was a little bit difficult, and still is a little bit difficult but we are handling it. (M3)
Moreover, due to limited research in COVID-19 treatment and management, the majority of the HCWs including doctors and nurses doubted the treatment given to patients. They thus lacked confidence in treating COVID-19 patients because they felt that the available management guidelines were not based on evidence. Some resorted to “trial and error” further compromising the quality of care for these patients.
The management plans we are using are not evidence based. We are in a panic, trying out things here and there. We are not doing our best because we don’t have evidence. (M12)
Apart from being a novel disease, COVID-19 also affected a vast number of people because of its nature of transmission. Consequently, the number of available staff was disproportionate to the rapidly growing number of patients.
There is a lot of understaffing here. I feel like we do not have an intensivist. We don’t have that yet. We only have one physician on full time, so if he needs a break, what will happen? (E5)
Poor remuneration in terms of low and/or delayed salaries as well as lack of or delays in receiving risk allowances contributed to dissatisfaction among staff.
Limited and delayed salary causes dissatisfaction and demoralizes the general staff because we come here every day to risk our lives, yet we are not remunerated. We have personal needs and families to take care of. (M13)
Suggestions to Improve the Frontline HCWs’ Job Satisfaction and Psychosocial Well-being
Participants urged the government to increase the health budget to increase the availability of medical supplies, equipment, and infrastructure required for the management and control of such pandemics.
I think it’s high time the government considered WHO’s guidelines on allocation of funds for infrastructure. Let the health budget be increased from 7.5% to at least 15% so that facilities can handle any emerging or re-emerging cases at any time without running to donors. (E15)
Rectification of salary and risk-allowance issues, availing frontline workers with health insurance, and compensation of their family members were also suggested solutions for the improvement of HCWs’ well-being and job satisfaction.
The government and ministry should re-strategize on how well to take care of the healthcare workers because if it was not us, a lot of lives would have been lost. (M1)
Some respondents suggested increasing the number of medical personnel, especially at the laboratory level to increase productivity and shorten the working durations.
I think increasing the number of personnel would help because then I think everyone would have shorter periods of work but very productive. Then, I’ve heard of/seen the UK model where you work for 2 weeks and stay home for 2 weeks. I’m not sure how feasible that is but I’m sure it would make people productive all the time. (E24)
Discussion
Job Satisfaction of Frontline Healthcare Workers
Job satisfaction significantly influences workplace well-being, directly impacting employee productivity and service quality within organizations. High job satisfaction translates into better patient care (Diakos et al., 2022). The results from our study show that 54% of the frontline HCWs were moderately satisfied with their jobs. A similar study done by Diakos et al. (2022), revealed a low level of job satisfaction. Another study done in Vietnam by Thai et al. (2021) also showed low job satisfaction among HCWs during the COVID-19 pandemic. However, in China, a study conducted by Yu et al. (2020) reported decent job satisfaction among the 455 frontline medical staff that participated in the study. This was attributed to the Chinese government’s efforts in the introduction and implementation of measures that promoted the work enthusiasm of the frontline medical staff thereby improving their job satisfaction. Some of these measures included the provision of allowances not subject to identities and job titles, ensuring a conducive working environment, psychological counseling, introduction of reward policies, and recognition of outstanding personnel and groups (Yu et al., 2020).
Compensating healthcare workers with “risk allowances” is crucial to motivate them to continue working despite the risks they face (Chersich et al., 2020). Moreover, a study by Thai et al. (2021), revealed that health workers who received higher incomes demonstrated better job satisfaction. However, satisfaction with compensation/risk allowances and salaries was particularly low in both the quantitative and qualitative aspects of our study. A study by Diakos et al. (2022) also classified pay/salary as unsatisfactory among frontline healthcare workers (Diakos et al., 2022). Low satisfaction with salaries has been a longstanding issue among healthcare workers in Uganda even before the pandemic (Hagopian et al., 2009).
In the present study, health workers who worked as volunteers and on short-term contracts had higher job satisfaction. In a study by Nyende (2014), this was attributed to the need to enhance skills to increase chances of future employment, religious beliefs that emphasized kindness, compassion, and generosity, among others (Nyende, 2014). In our study, the age, and the duration of work experience of the frontline HCWs did not influence job satisfaction. However, a similar study by Yu et al. (2020) described work experience as a positive predictor of job satisfaction. Another study conducted in Serbia demonstrated that younger participants and those with less working experience were negatively influenced by the COVID-19 pandemic and were reassigned to other positions (Dinić et al., 2021). In a study by Diakos et al. (2022), HCWs aged 45 to 55 years were more satisfied with their jobs.
Psychosocial/Mental Well-being of Frontline Healthcare Workers
The World Health Organization recognized the importance of safeguarding the psychosocial well-being of frontline HCWs during the pandemic. In our study, 35%, 33%, and 32% of the HCWs reported moderate, good, and poor mental well-being, respectively. The factors that contributed to the poor mental well-being of the frontline HCWs from the FGD were burnout due to heavy workload and long working hours, and anxiety due to the fear of contracting COVID-19 or infecting family members. Similar studies demonstrated burnout among frontline HCWs (Babamiri et al., 2022; Mushtaq et al., 2022) during the pandemic. High workload is the major contributor to burnout among frontline HCWs (Babamiri et al., 2022). Like our study, multiple studies revealed a high prevalence of anxiety among frontline health workers (Hassannia et al., 2021; Mohindra et al., 2020; Tong et al., 2023). The sources of anxiety may include concerns about the health of self, the spread of the disease, the health of family members, and potential discrimination or stigma associated with the disease (Mushtaq et al., 2022). A study done by Kumar et al. (2020) also revealed that the anxiety was due to the fear of getting infected, being quarantined, and losing life, and as a result, most of the participants in this study were hesitant to work.
Stigma and discrimination against frontline HCWs and their family members also contributed to poor mental well-being in our study. An article written by Poudel, 2020 revealed that several frontline HCWs suffered stigma and discrimination (Arjun, 2020). In India, HCWs were evicted from their homes by landlords who were worried that they could spread the COVID-19 virus (Adam, 2020). The stigma and discrimination were attributed to the unscientific beliefs held by most people about the mode of transmission of the COVID-19 virus (Bagcchi, 2020). It is, therefore, crucial to disseminate accurate and easily understandable COVID-19-related information to the public, to counteract these unscientific beliefs and thus reduce fear and stigma (World Health Organization, 2020).
A thematic review by Philip et al. (2020) demonstrated better psychological well-being among older HCWs during an epidemic outbreak. This is contrary to findings from our study where HCWs aged 60 years and above had poorer mental well-being. Akin to previous studies, (Nielsen et al., 2009), we realized a positive correlation between job satisfaction and mental well-being where participants with high job satisfaction scores had higher mental well-being scores.
Strengths and Limitations
The use of both qualitative and quantitative methods of data collection facilitated a deeper understanding of the HCWs’ experiences and challenges during this pandemic. The inclusion of the different cadres of HCWs that is, doctors, nurses, pharmacists, and laboratory personnel helped us capture the different experiences. The study was conducted in only three facilities, and the sample size was small, limiting country-wide generalization. Respondents could have given socially acceptable responses due to the fear of jeopardizing their jobs. However, this was minimized by strict observation of confidentiality.
Conclusion and Recommendations
At the time of this research, only a small number of frontline healthcare workers expressed good job satisfaction and mental well-being. Creating policies to ensure the safety of frontline healthcare workers, providing them with sufficient risk compensation, and enhancing their current pay systems could potentially improve their job satisfaction. Incorporating mental health support into emergency response plans, reinforcing mental health resources and workforce, tackling stigma, and encouraging healthcare workers to seek help could help safeguard the psychological well-being of all healthcare workers.
Footnotes
Appendix I: Focus Group Discussion Guide
Acknowledgements
We extend our sincere gratitude to the administrators of the three health facilities for welcoming us into their institutions. We also thank all the HCWs for sparing some time to participate in our study.
Authors Contribution
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, and acquisition of data, analysis and interpretation. They all took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Fogarty International Centre of the National Institutes of Health, the U.S. Department of State’s Office of the U.S. Global AIDS Coordinator and Health Diplomacy (S/GAC), and President’s Emergency Plan for AIDS Relief (PEPFAR) under Award Number 1R25TW011213. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Transparency Declaration
The authors affirm that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies in the manuscript have been explained.
Ethical Consideration
The study sought approval from the Mulago Hospital Research and Ethics Committee under protocol number MHREC 1906. Administrative clearance was further obtained from the three health facilities. After explaining the purpose of the study, possible risks, and benefits to the participants, each of them had to sign the approved and well-detailed consent form before joining the study. The study was entirely voluntary and whoever wanted to withdraw, had the right to do so without repercussions. Confidentiality was highly observed as participants were only identified by codes rather than their names and the questionnaires were under lock and key and accessed by only the study team.
Availability of Data and Materials
Data and other supplementary material will not be made available online, but the corresponding author can be contacted to discuss sharing.