
Abstract
Misophonia is a disorder of decreased tolerance to specific sounds or stimuli associated with such sounds, called triggers. The aim was to validate a questionnaire on self-perception of the type of sound, visual identification, and origin of sounds in adults with suspected misophonia by Spanish-speaking people. An interview was conducted with a total of 395 participants, divided into four distinct blocks of questions: the trigger of misophonia, the visual identification of gestures or actions related to selective sounds, the emotional closeness between listener and sender, and the impact on the daily personal relationships of the person with misophonia. Each block used classical test theory to factorially validate the instrument. The first group of questions gave as a result four factors: mouth and throat sounds, environmental sounds, material sounds, and pronunciation sounds (Cronbach’s alpha = .929; KMO = 0.894). The second group identified two dimensions of reaction to actions and gestures, one related to movements of the mouth and throat and the second to body movements or exaggerated gesticulation (Cronbach’s alpha = .840; KMO = 0.819). The third block linked low and high emotional closeness factors (Cronbach’s alpha = .690; KMO = 0.633). The fourth block obtained a factor for daily chores and another for affective relationships (Cronbach’s alpha = .861; KMO = 0.820). The questionnaire offers valuable insights into the nature of misophonia, and the necessity for further research in this field. These findings emphasize the importance of developing a comprehensive understanding of misophonia to enhance diagnosis.
Plain language summary
Misophonia is a condition in which certain sounds cause discomfort. Researchers validated a self-assessment questionnaire for Spanish-speaking adults with suspected misophonia. The questionnaire explored sound types, visual identification, and emotional impact. It revealed factors related to mouth and throat sounds, environmental sounds, material sounds, and pronunciation sounds. Understanding misophonia is relevant for accurate diagnosis and future research
Introduction
According to data from the Global Burden of Disease (GBD) (2018), mental health and substance abuse issues affect approximately 11% to 18% of the global population, equivalent to around 970 million individuals. Among the most common mental health problems are depression, anxiety, and alcohol and drug use disorders (Dattani et al., 2019). However, there are ongoing discoveries of new mental disorders that the World Health Organization (2019) in the International Classification of Diseases 11th edition (ICD-11) and the American Psychiatric Association (2022) do not currently recognize. Examples of such complex neurophysiological and behavioral disorders include misophonia and hyperacusis.
The term Misophonia was initially introduced by P. J. Jastreboff and Jastreboff (2003) and combines the Greek words μíσoς (mísos) ‘aversion’ and φων
Other frequently encountered examples include tinnitus, which is the perception of sound in the absence of an external source (Levine & Oron, 2015; Møller, 2011), and phonophobia, which is an irrational fear that arises in the presence of specific sounds, leading to a hypersensitivity towards them (Theodoroff et al., 2019). While these conditions are distinct, numerous studies have demonstrated a significant correlation between them (Potgieter et al., 2019; Swedo et al., 2022).
An estimated 60% of individuals with misophonia also experience tinnitus, and a higher percentage may have comorbid personality disorders (Bruxner, 2015; P. J. Jastreboff & Jastreboff, 2015; Schröder et al., 2013; Webber et al., 2014; M. S. Wu et al., 2014). Misophonia has a significant impact on the personal and social lives of patients, often leading to depression and even suicidal ideation (Edelstein et al., 2013; P. J. Jastreboff and Jastreboff, 2003; Schröder et al., 2013; M. S. Wu et al., 2014; Zhou et al., 2017). Schröder et al. (2019) and Dozier and Morrison (2017) propose that misophonia involves involuntary physical and emotional responses to trigger stimuli. Individuals with this condition frequently report deterioration in communication with family and close relationships, which can result in the breakdown of romantic partnerships, unemployment, and social isolation (Schwartz et al., 2011; Zhou et al., 2017). There are treatments such as the use of portable white noise devices to reduce awareness of aversive sounds (P. J. Jastreboff and Hazell, 2004), Autonomous Sensory Meridian Response (ASMR) sounds (Rouw & Erfanian, 2017), and cognitive-behavioral therapy (Bernstein et al., 2013; Muller et al., 2018), however, have yielded mixed or incomplete results (Dozier et al., 2017; Hadjipavlou et al., 2008; P. J. Jastreboff et al., 1996; Palumbo et al., 2018).
Swedo et al. (2022) outline five key domains of misophonia: misophonic triggers, reactions to triggers, influences on reactions, functional impairments, and relationships with other conditions or disorders. Consequently, it is expected that self-report measures will incorporate as many domains as possible, enabling a more comprehensive evaluation of misophonia (Aazh, 2023).
The most widely used questionnaire is the Misophonia Questionnaire MQ (M. S. Wu et al., 2014), while the most widely used scale of dislikes associated with misophonia is the Misophonia Activation Scale MAS-1 (Fitzmaurice, 2010). MAS-1 consists of 11 levels, ranging from not perceiving a sound as annoying (level 0) to thoughts of physical violence towards the sound source or oneself (level 10). Other instruments available include the Misophonia Assessment Questionnaire (MAQ) (Rosenthal et al., 2021); Misophonia Emotional Responses Scale (MER) (Dozier, 2015); Online Misophonia Questionnaire (Rouw & Erfanian, 2017); Selective Sound Sensitivity Syndrome Scale (S-Five) (Vitoratou et al., 2021); MisoQuest (Siepsiak et al., 2020); Misophonia Response Scale (MRS) (Dibb et al., 2021); Duke Misophonia Questionnaire (DMQ) (Rosenthal et al., 2021); Sussex Misophonia Scale for Adolescents (SMS-Adolescent) (Rinaldi et al., 2022); Duke-Vanderbilt Misophonia Screening Questionnaire (DVMSQ) (Williams et al., 2022); and Misophonia Coping Responses Scale (MCR) (Rosenthal et al., 2021). These instruments provide various avenues for assessing misophonia and its associated factors.
Likewise, there is also the Misophonia Physiological Response Scale (MPRS) (Bauman, 2015), the Amsterdam Misophonia Scale (A-MISO-S) (Schröder et al., 2013), and the Misophonia Trigger Severity Scale (MTS) (Dozier, 2015). The limitations of these instruments are that they cannot simultaneously cover the effect of each type of sound on a person: synesthesia from seeing some scenes associated with triggering sounds, the relationship between the reaction between misophonia and emotional closeness with the sender of triggering sounds, and the impact on the daily routine of the person with misophonia. In addition, all these instruments are in English (Ferrer-Torres & Giménez-Llort, 2022a); some are not psychometrically validated; and instruments such as the A-MISO-S have not previously been reported as having been validated in Spanish (Ferrer-Torres & Giménez-Llort, 2022b). Therefore, it is necessary to have a version to assess Spanish-speaking people. Since many social and cultural variables can directly or indirectly influence the level of discomfort towards certain sounds, such as noises made while eating and the tone of speech, these characteristics may be linked to the habits and customs of certain linguistic communities (Ferrer-Torres & Giménez-Llort, 2022a). Therefore, as research on misophonia continues, it requires instruments that can be adapted to different socio-cultural contexts. In particular, this research is expected to provide a new resource for the Spanish-speaking community, which can be replicated in other linguistic communities (Ferrer-Torres & Giménez-Llort, 2022b).
This study aimed to validate a questionnaire on self-perception of the type of sound, visual identification, and origin of sounds in adults with suspected misophonia by Spanish-speaking people.
This psychometric validation is a new questionnaire that was based on the Misophonia Questionnaire (MQ) (M. S. Wu et al., 2014), on the work of other experts in the field (Potgieter et al., 2019; Schwatz et al., 2011), and on the evaluation of the criteria of expert judges in the area of mental health and psychometrics. The MAS-1 scale and the report by Brout et al. (2018) were used to generate the response scales.
A questionnaire was developed inspired by other instruments, primarily the Misophonia Questionnaire (MQ) (M. S. Wu et al., 2014) and the works of Potgieter et al. (2019) and Schwartz et al. (2011). Additionally, an evaluation of criteria by expert judges in the fields of mental health and psychometrics was consulted. It was found that not only mouth and throat sounds (such as slurping and swallowing) are triggers, but also environmental sounds, animal sounds, whispers, among others. These works also highlight the importance of considering that movements associated with certain sounds, such as spitting, form part of the discomfort, thus requiring investigation into their link with misophonia. To create the response scales, the MAS-1 scale and the report by Brout et al. (2018) were used as inspiration.
A pilot version of the instrument was then administered to 179 adults, with an observed internal consistency of a Cronbach’s alpha of .85. Following the expert judgment and the pilot test, the final version of the questionnaire was concluded with the items presented in Appendix 1.
Materials and Methods
The research corresponded to a cross-sectional exploratory study carried out between March and April 2021, which incorporated the inquiry of the misophonia and misokinesia questionnaire (CUDEMM, for its acronym in Spanish: Cuestionario de Misofonía y Misokinesia) through a non-probabilistic convenience sample. Previously, the questionnaire application was approved by the Scientific Ethics Committee of the Universidad Católica del Maule, record No. 25/2021.
The recruitment of the sample was carried out through a call to participate through a personal account on social networks in groups in Spanish, oriented towards the suffering of misophonia. The participants answered the question of informed consent virtually, and then, in the case of acceptance, they were presented with the question, “Do you feel any discomfort when you hear certain types of sounds?” If you answered “Yes,” continue with the questionnaire. Otherwise, you are consulted if you know people with misophonia. The questionnaire, for the moment, does not have clinical validity, since its objective is to explore new aspects of misophonia as a screening tool.
To ensure the authenticity of participants, their email addresses were collected upon accessing the questionnaire, allowing only one response per address. Additionally, two open-ended questions and correlational statistics were used to identify any suspicious cases of duplication.
The inclusion criteria were being of legal age (verified by asking for age and date of birth), being a Spanish speaker (as the instructions and participant recruitment materials were only written in Spanish), and having access to an account on one of the social networks used for distributing the questionnaire. Additionally, participants had to express interest in the topic of misophonia by accepting informed consent to participate in the study. Exclusion criteria included all incomplete questionnaires, as well as those with response patterns suggesting a lack of attention or seriousness from the participant. In this study, we did not observe any fraudulent or duplicate responses.
To ensure consistent psychometric properties, the appropriate sample size for the population of interest (Spanish-speaking adults who have experienced this discomfort before) depended on two main factors. First, the number of participants who responded to each question was considered; ideally, there were ten or more responses per item. Second, the similarity of sociodemographic and psychosocial characteristics in the population where the instrument was used was taken into account. Therefore, as each block of questions was analyzed separately, it was expected that for a set of 21 questions (considering the block with the highest number of items), there would be a minimum of 210 valid responses to reduce biases due to sample size.
This scale was designed based on the levels assigned by the Misophonia Activation Scale (MAS-1) (Fitzmaurice, 2010) and the report by Brout et al. (2018). The scale proposes the following rating: (1) No discomfort or minimal irritation is felt; (2) is hypervigilant; the person asks to stop the sound, covers one ear, or quietly moves away; (3) feels slight discomfort, covers their ears, and feels like running away; (4) feels considerable discomfort; sometimes, when imagining the sound for a later moment, ideas of violence arise; and (5) feels panic, anger, and episodes of physical violence towards others, themselves, or animals.
The questionnaire’s composition is based on four blocks of questions, the first of which presented 21 statements regarding different types of sounds associated with misophonia (Dozier, 2015; M. Jastreboff & Jastreboff, 2014; Schröder et al., 2013; M. S. Wu et al., 2014), to which individuals responded with their level of disgust and reaction to each situation.
Similarly, a second block presented seven questions exploring synesthesia and misokinesia (Brout et al., 2018; Palumbo et al., 2018; Saenz & Kock, 2008). The questions in this block were rated using the same response scale as the first block. Then, a third block asked about participants’ reactions to four types of interpersonal relationships. The response scale used for this was: (1) I contain my emotions; (2) I constantly let others know about my discomfort; (3) I try to escape the noise; (4) I imagine scenes of hatred; and (5) I have fought with others. Finally, the fourth block of questions inquired how misophonia had impacted the respondent’s life in six contexts. The following scale was used for grading: (5) a lot; (4) enough; (3) somewhat; (2) little; (1) almost none; and (0) does not apply. These blocks represent much of the characteristics that Swedo et al. (2022) compiled about misophonia (Figure 1).

Schema of the summary of the characteristics of misophonia according to the work of Swedo et al. (2022, cited by Aazh, 2023).
The study included additional questions. Participants were asked about their gender, age, and whether they engaged in playing a musical instrument. Moreover, they were asked if they experienced any discomfort from bothersome noises while dining out or watching movies, whether they could identify specific triggers for the onset of their misophonia, and if they could mentally visualize the scenes that generate the sounds after reading the initial set of questions.
The instrument had 395 answers extracted from the Google Formulary for 38 questions that constitute the four blocks of 21, 7, 4, and 6, respectively. In these, it is deduced that the minimum question-participant ratio was 18.8 participants for each question, which is methodologically appropriate (Bandalos and Finney, 2019).
Analysis Plan
Initially, the judges’ criteria were applied to assess the questions in block 1. Three experts in the validation of psychometric instruments in the field of mental health were selected, and they unanimously agreed on the final version of the instrument. The agreement coefficient and Russell-Rao statistic were used to demonstrate the questionnaire’s relevance.
To evaluate the item’s ability to function as intended, Cronbach’s alpha coefficient was employed. Exploratory factor analysis was conducted to analyze the questionnaire’s multidimensional behavior, using the principal components as the method of factorial extraction. The Kaiser-Meyer-Olkin (KMO) measure of sample adequacy and Bartlett’s sphericity test were utilized to compare observed and partial correlation coefficients.
The selection of the number of factors or dimensions was based on their representativeness, considering a high explained variance and psychometric interpretation. Subsequently, the resulting factors were rotated using the Promax method with Kaiser normalization, ensuring that correlations between factors were respected. The communality index and uniqueness were used to indicate the representativeness of each item in the selected factors. The Hofmann complexity index was employed to determine the number of factors associated with each item (Hofmann, 1978).
After identifying and describing the questionnaire’s factors, a descriptive analysis was performed to examine the relationship between the factors and the participants’ age and gender. The scores for each factor were calculated as the sum of the associated response grades.
Results
Participant Characteristics
The study included a total of 395 Spanish-speaking participants (337 women, 56 men, and 2 not identified). This type of imbalance often occurs in surveys with online recruitment (M.-J. Wu et al., 2022). Moreover, similar studies (e.g., Dibb et al. 2021; M. S. Wu et al. 2014) have shown a higher prevalence of women with aversions to specific sounds. The age of the participants ranged from 18 to 77 years (mean = 34.15; standard deviation [SD] = 10.22 years).
The majority of participants (343 individuals) reported that their discomfort with certain sounds began spontaneously, without any specific trigger. For 37 participants, the onset of misophonia was attributed to their parents or siblings, while 8 individuals mentioned finding out about it through some form of communication. Only three participants reported that their friends played a role in the onset, while one person mentioned their partner as the trigger, and another individual attributed it to a cousin. The average age at which participants started experiencing discomfort due to certain sounds was approximately 12.97 years (SD = 7.32).
When asked if they had instilled this condition in other people, 31.9% (n = 126) mentioned that to 1 or 2 people; 12.1% (n = 48) between 3 and 5; 5.4% (n = 21) indicated that to 6 or more people; and 50.6% (n = 200) to no one. 17.5% stated that they did not go to the cinema for this reason, and 44% did so rarely. On the other hand, 4.7% do not go out to eat because of this condition, while 40.1% do so occasionally. Also, 3.1% of the participants do not go out to dinner because of the noise when eating, while 55.3% do so but indicate that they put up with the noise.
The majority of participants, specifically 78%, indicated that they had not sought the assistance of a mental health professional. In contrast, 15.9% of the participants reported seeking professional help, but expressed dissatisfaction with the results of their previous experiences.
Finally, in response to the question about mentally visualizing the sounds that trigger discomfort (block 1 questions), 2% of participants (n = 8) answered “none,” 24% (n = 95) answered “some,” 46.5% (n = 184) answered “many,” and 27.3% (n = 108) indicated “all.”
The 38 questions that make up blocks 1, 2, 3, and 4 are presented in Appendix 1, along with their item and descriptive measures.
Next, the factorial psychometric validation results are presented for each of the analyzed blocks.
Block 1: Trigger Sounds of Misophonia
The first block of questions was submitted to expert judgment, which was obtained from the consultation of two professionals to assess the degree of relevance and clarity, subject to the options of good and bad. The simple and Russell-Rao agreement coefficients had the same value for the degree of relevance and clarity, with values = 0.89 and 0.83, respectively.
The reliability analysis gave a Cronbach’s alpha coefficient = .929, indicating high internal consistency. The KMO sample adequacy statistic was 0.894, suggesting that the data was suitable for exploratory factor analysis. The Bartlett sphericity test showed a significant result (p < .001), further supporting the appropriateness of factor analysis. By selecting eigenvalues greater than one, a total of five dimensions were identified, which accounted for 66% of the variance explained. The latent variables identified by the instrument were nasal, mouth, and throat sounds; ambient sounds; material sounds; and pronunciation sounds. The first factor had the highest contribution, explaining 22% of the rotated variance (Table 1).
Matrix of Rotated Factorial Components, Communality, Uniqueness, and Complexity Index of the Items in Block 1.

Note. N = 395. Some membership values exceed unity due to software approximations and rounding.
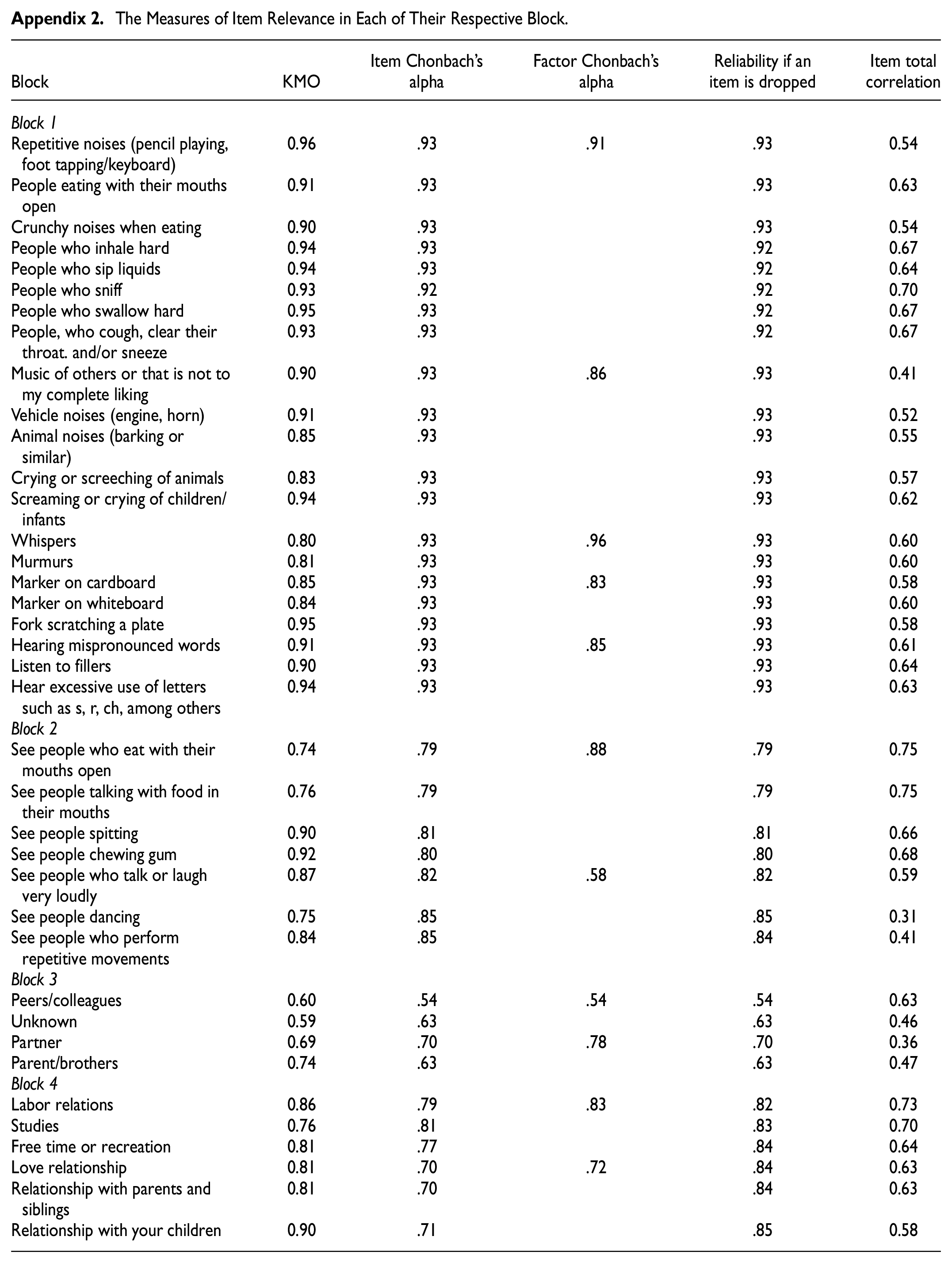
The positive correlation between each item in block 1 can be observed in Appendix 2. The factor analysis yielded the first dimension, which exhibited a Cronbach’s alpha coefficient of .91 (Appendix 2). This dimension consists of the initial eight questions that pertain to “mouth and throat sounds,” such as noises associated with the nose, eating, coughing, sneezing, and throat clearing. The factor demonstrated strong performance in terms of item representativeness (Table 1), although item Q1 was only represented in 32% (communality) and showed some association with approximately three factors (complexity index).
The second factor encompasses “ambient sounds,” including shrieks, cries, and horns. This factor achieved a Cronbach’s alpha of .86 (Appendix 2), and item Q9, while represented by only 35%, is exclusively associated with the second factor (Table 1).
The factor related to “soft sounds,” encompassing whispers and murmurs, exhibited a high level of internal consistency with a Cronbach’s alpha of .96. Table 1 demonstrates that the communalities and complexity index for this factor are both close to unity, indicating a strong representation of the items.
The factor related to “material sounds,” resulting from the friction between certain inert materials, demonstrated good internal consistency with a Cronbach’s alpha = .83. The factor performed well overall, although item Q18 (fork scratching a plate) showed slightly lower representation with a communality of 44% and a complexity index = 2.9 (Table 1). This item appears to be associated with both the “mouth and throat sounds” and “ambient sounds” factors, potentially due to its connection to shared instances of food with others.
Finally, “pronunciation sounds” such as fillers, excessive use of some consonants, and mispronounced words formed a factor with a Cronbach’s alpha = .85. In this case, item Q21 (listening to excessive use of letters such as s, r, and ch, among others) had a complexity index = 2.8 since it was also partially represented by the factors “mouth and throat mouth sounds” and “soft sounds.”
While the promax rotation method yields results similar to the varimax rotation, it allows for the possibility of obtaining oblique factors that are not completely independent. In this study, the factorial correlations exceeded the threshold of 0.40, justifying the use of a rotation method that does not assume orthogonality among factors. As a result, the complexity index predominantly showed values close to 1, indicating that the factors are more representative and do not need to be orthogonal. In other words, the levels of dislike for certain types of sounds may be closely correlated, suggesting that multiple expressions of misophonia can coexist within the same individual.
Block 2: Visual Identification
In this second group of questions (Table 2), the reliability analysis gave a Cronbach’s alpha = .840, a KMO = 0.819, and the Bartlett sphericity test a p-value < 0.001. In turn, it was possible to explain 57% of the variance of the data by obtaining two factors: one related to “mouth and throat movements” and the other to “body movements or exaggerated gesticulation.” According to the promax rotation, these had a correlation between factors of 0.58 and represented about 40% and 17% of the explained variance, respectively. The first factor presented a Cronbach’s alpha = .88 (Table 2). However, factor 2 gave a Cronbach’s alpha = .58, a total correlation = 0.31, and a communality of 0.32 for item Q27 (see people dancing), which gives the understanding that it is an item with minimal similarity to the rest of the questions.
Matrix of Rotated Factorial Components, Communality, Uniqueness, and Complexity Index of the Items in Block 2.
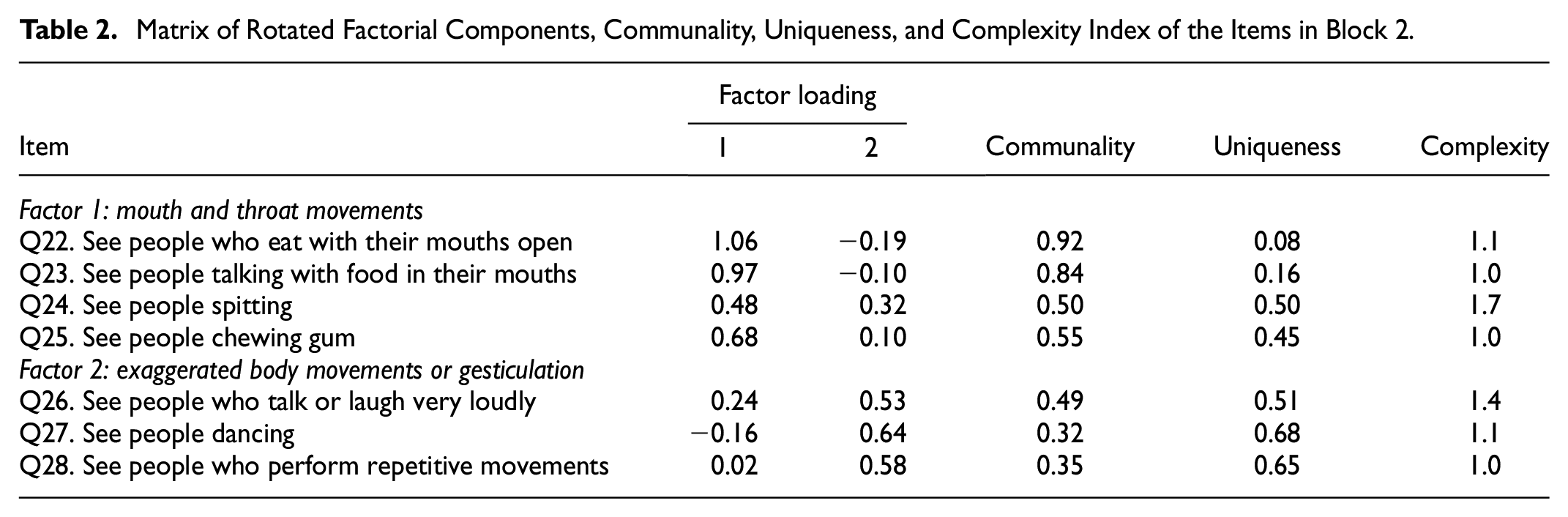
The first of these factors may be associated with misophonia by synesthesia, while the second seems to be related to misokinesia and hyperacusis.
Block 3: Origin of Sounds
When analyzing the group of questions that link the participants’ reactions to the origin of the sounds, a Cronbach’s alpha = .690, a KMO = 0.633, and the Bartlett sphericity test with a value p < .001 were determined (Table 3). On the other hand, the factorial analysis obtained two dimensions correlated at a level of 0.55, with which 54% of the variance is explained. In this sense, the latent variables were associated according to the emotional closeness that the respondent reports with the emitter of the sound, that is, “low emotional closeness” when the sound refers to peers, colleagues, or strangers, and “high emotional closeness” comes from a partner, father or siblings. These represented 33% and 21% of the data variance, respectively.
Matrix of Rotated Factorial Components, Communality, Uniqueness, and Complexity Index of the Items in Block 3.
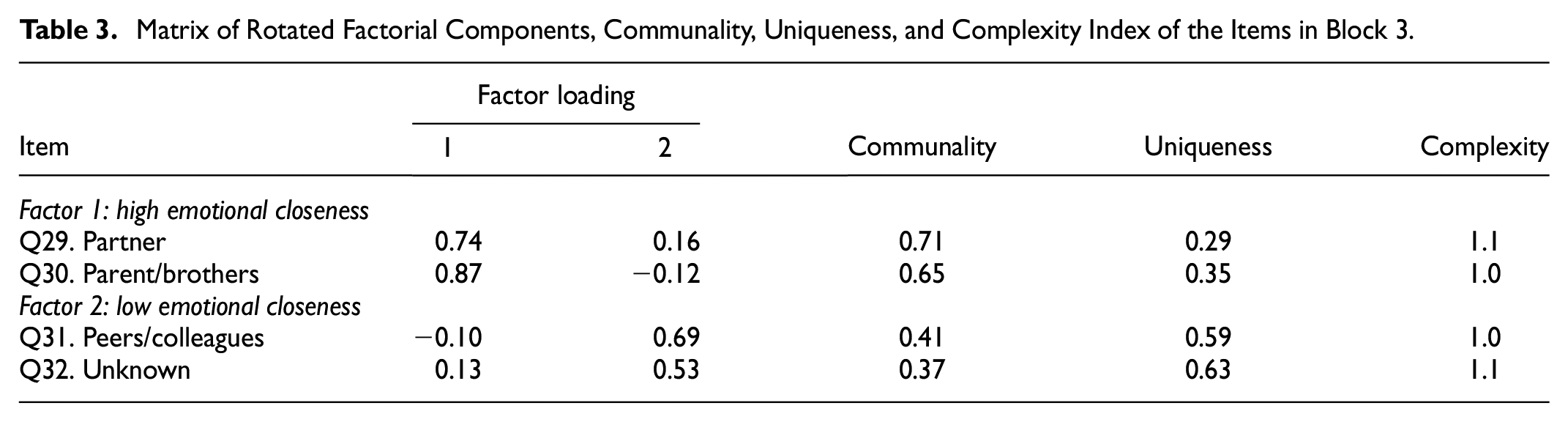
Even though this block of questions is the most difficult to measure psychometrically, the KMO statistic is low but acceptable (Field, 2013; Li et al., 2011; Kaiser, 1974; Norusis, 2007). In addition, Matsunaga (2010) states that for low KMO values (between 0.5 and 0.6), the relevance of the items can be tested through the interpretability of the factors, allowing the variables to be kept when they clearly belong to a single factor and have loads factorials greater than 0.5. In this work, the KMO was greater than 0.6, the unique belonging of each variable to a single factor is clear (with complexity coefficients close to or equal to 1), and the factor loadings are greater than 0.5.
Block 4: Impact of Misophonia. Psychometric Properties
The following block of questions tries to identify the impact of misophonia on the quality of life of the person who experiences it. To do this, participants have been consulted on six essential instances which most of them experience. These are labor relations, studies, free time or recreation, love relationships, parents and siblings, and relationships with their children.
When performing the factorial analysis, a Cronbach’s alpha = .861, a KMO = 0.820, and the Bartlett sphericity test had a p < .001. On the other hand, about 63% of the explained variance was obtained in the selection of four dimensions. In this sense, the instrument detected the latent variables: nasal, mouth, and throat sounds; ambient sounds; material rubbing sounds; and pronunciation sounds. The first factor predominated in this group of variables, explaining 33% of the rotated variance.
The impact of misophonia is expressed in two contexts or dimensions: daily work and emotional closeness, which can be seen factorially in Table 4. Although labor relations belong to the daily work factor, they have a complexity index close to 1.4 because emotional relationships can be generated in the work context (Guetta et al., 2022). The relationship with their children item has a communality value and a total item correlation (Appendix 2) lower than the rest of the questions. This may be because 168 participants declared they did not have children.
Matrix of Rotated Factorial Components, Communality, Uniqueness, and Complexity Index of the Items in Block 4.

In each of the blocks and dimensions, no statistically significant differences (p = .05) were observed in the results by sex or age. However, given the difference in the number of responses by gender, it is proposed that future research should consider a greater focus on this variable.
Discussion
When validating in Spanish one of the first questionnaires on the self-perception of the type of sound, visual identification, and origin of the sounds of people with suspected misophonia, various factors or dimensions were discovered that contributed to modeling and understanding misophonia and its impact on the mental health of Spanish-speaking people. The psychometric properties were satisfactory, although these are not comparable with the MQ (M. S. Wu et al., 2014), MAQ (Rosenthal et al., 2021), MER (Dozier, 2015), and MCR (Rosenthal et al., 2021) questionnaires since the orientation of our instrument has another Likert measurement scale (modified in the level of disgust), along with a complete view of misophonia, such as synesthesia and hyperacusis.
Misophonia can appear in a variety of contexts and depends on the patient’s environment (Swedo et al., 2022). In the study, some of the participants stated that they avoid public recreational spaces such as cinemas, restaurants, or similar places because of the sounds that others make when eating, generating problems in adapting to everyday social environments.
According to M. Jastreboff and Jastreboff (2014), individuals with misophonia seldom seek the assistance of specialists. Taking into account the aforementioned information as well as the exploratory findings presented in this study, it becomes apparent that misophonia is a public health concern that significantly affects the quality of life of both the individuals experiencing it and those around them (Kokowska, 2018). Furthermore, there is a limited availability of epidemiological tools that enable researchers to develop long-term prognostic models for misophonia.
Question block 1 managed to group the types of sounds previously consolidated by the MQ instrument (M. S. Wu et al., 2014) plus the questions included in this questionnaire about other sounds such as breathing, whispers, car brakes, and cracking bones, among others, grouped into mouth sounds and throat, environmental, materials, and grammar. Secondly, the questions in block 2 explore the visualization of scenes associated with factor 1 in block 1, which is why CUDEMM is the first questionnaire to consider this type of relationship as part of misophonia. Thirdly, the questions in block 3 confer the reaction to the triggering sounds, given an emotional closeness with the issuer. This is how the trust between the couple, parents, and siblings triggers them to pay more attention to the triggering sounds, obtaining reactions of greater displeasure with relatives than with friends and pets. Finally, the fourth block of questions revealed that one of the effects in which misophonia has generated the greatest impact is in affective relationships; therefore, greater attention and repair should be paid to this point.
The main difference between the CUDEMM questionnaire and the MQ (M. S. Wu et al., 2014), MAQ (Rosenthal et al., 2021), MER (Dozier, 2015), and MCR (Rosenthal et al., 2021) questionnaires is that the CUDEMM questionnaire describes the sounds that trigger misophonia in terms of disgust and the effects that have on the social and personal lives of the person with misophonia, paying special attention to synesthesia, and gives the information needed to make a structural model of this condition. In the same way, sound disgust scales like the MPRS (Bauman, 2015), MTS (Dozier, 2015), and MAS-1 are compactly unified for four levels in each factor of each block of questions. This makes it possible to get a set of misophonia-related scores with different meanings. On the other hand, the questionnaire seeks the psychometric quality that gives it value in a public health study (Lloret-Segura et al., 2014; Terwee et al., 2007).
Numerous studies (Ferrer-Torres & Giménez-Llort, 2022a; Quek et al., 2018; Schwartz et al., 2011; Siepsiak & Dragan, 2019) have highlighted the recognition of misophonia as a public health issue. The CUDEMM questionnaire introduced in this research captures the significant impact of misophonia on both personal and social aspects of an individual’s life, aligning with the consensus on new findings about this disorder (Swedo et al., 2022). It considers the inclusion of misokinesis, hyperacusis, and synesthesia as integral components of the study of misophonia.
Indeed, despite the unknown etiology of misophonia (Ferrer-Torres & Giménez-Llort, 2022a; Kumar et al., 2017), the study’s respondents reported that misophonia not only affects themselves but also has a significant impact on others, particularly their relatives. They expressed that specific sounds made by their relatives bothered them, leading to rejection or aversion towards those who did not experience the same problem (Lloret-Segura et al., 2014; Swedo et al., 2022). This finding highlights the profound effect of misophonia on interpersonal relationships and underscores the importance of increasing understanding and awareness of the condition. By raising awareness, we can foster empathy and support for individuals with misophonia, thereby promoting healthier and more inclusive relationships.
An interesting aspect to consider is that the presence of misophonia symptoms in individuals can lead those without the condition to become more attentive to these sounds and others in their daily lives. This phenomenon aligns with the findings reported by Rouw and Erfanian (2017), Erfanian and Rouw (2018), and Sanchez and Silva (2018), who observed a higher incidence of individuals having relatives with misophonia. The awareness and impact of misophonia within close familial relationships may result in heightened sensitivity and attention towards triggering sounds, affecting the behavior and perception of those without the condition. This highlights the potential influence of misophonia on both individuals with the condition and their family members. Further research in this area can provide valuable insights into the dynamics and implications of misophonia within family units.
A strength of this work is that it validates in a single questionnaire the perception of the level and characteristics of the dislike for certain sounds, along with the visual identification of certain movements, the emotional proximity to the emitter of unpleasant sounds, and some effects on the patient’s quality of life. This instrument could be useful for public health studies in the Spanish-speaking community, as existing instruments have been developed primarily in English.
The main limitations of the study include the lack of clinical validity. Additionally, a notable gender imbalance was observed in the responses, suggesting that future research should examine whether this difference is due to the bias of the online instrument, the predominance of misophonia in women, or both factors. There is also a need to investigate children, adolescents, and sociocultural differences, even within the Spanish-speaking community.
On the other hand, this study used convenience sampling, which limits its generalizability. Nevertheless, it has an exploratory nature and encourages future research to conduct a confirmatory analysis with random sampling, evaluating the sensitivity, specificity, and predictive value of the instrument. This instrument was factor-validated in Spanish, so for it to be translated and analyzed in another language, it is necessary to validate it again to confirm its consistency and reliability in another linguistic community.
However, this study also opens up new avenues for research. It highlights the need to explore the simultaneous association between different types of triggering sounds, synesthesia, emotional closeness with the sound emitter, and their impact on the daily lives of individuals with misophonia and their close emotional circle. Such investigations can contribute to guiding the diagnosis and treatment of misophonia, estimating the quality of life of affected individuals, implementing preventive strategies, and providing support for family members. Also, using statistical and mathematical techniques or tools can make it easier to design and model prevalence in the population, figure out how well a treatment might work, and help us learn more about misophonia and related conditions like phonophobia and hyperacusis.
Conclusions
In summary, the CUDEMM questionnaire is the first psychometric instrument validated in Spanish to evaluate the presence of misophonia, mysokinesia, emotional proximity, and visualization. This questionnaire may benefit both the public and private healthcare sectors. As the prevalence of misophonia has increased in recent years, it is conceivable that in the future it will be recognized as a mental health issue.
The modified Likert scale utilized in the questionnaire provided detailed information regarding the degree to which each sound triggered misophonia in individuals. The dimensions obtained through factor analysis helped to characterize trigger sounds based on their effect on the participants. The associations between these variables and queries pertaining to social and daily activities shed light on the extent to which individuals experience misophonia and its impact on society.
Using question blocks, the questionnaire accurately described both the sounds that induce misophonia and their effects on misophonia sufferers. In addition, the study investigated responses based on the degree of emotional proximity and the impact of visualizing actions associated with trigger noises. The presence of synesthesia in individuals with misophonia has a significant impact on the condition’s etiology. Despite the fact that misophonia is defined as a phobia of sound, visualization also emerges as an aversion trigger.
The CUDEMM questionnaire provides valuable insights into the complexity of misophonia, its effects on individuals, and the need for additional research and understanding in this field.
Footnotes
Appendix
The Measures of Item Relevance in Each of Their Respective Block.
| Block | KMO | Item Chonbach’s alpha | Factor Chonbach’s alpha | Reliability if an item is dropped | Item total correlation |
|---|---|---|---|---|---|
| Block 1 | |||||
| Repetitive noises (pencil playing, foot tapping/keyboard) | 0.96 | .93 | .91 | .93 | 0.54 |
| People eating with their mouths open | 0.91 | .93 | .93 | 0.63 | |
| Crunchy noises when eating | 0.90 | .93 | .93 | 0.54 | |
| People who inhale hard | 0.94 | .93 | .92 | 0.67 | |
| People who sip liquids | 0.94 | .93 | .92 | 0.64 | |
| People who sniff | 0.93 | .92 | .92 | 0.70 | |
| People who swallow hard | 0.95 | .93 | .92 | 0.67 | |
| People, who cough, clear their throat. and/or sneeze | 0.93 | .93 | .92 | 0.67 | |
| Music of others or that is not to my complete liking | 0.90 | .93 | .86 | .93 | 0.41 |
| Vehicle noises (engine, horn) | 0.91 | .93 | .93 | 0.52 | |
| Animal noises (barking or similar) | 0.85 | .93 | .93 | 0.55 | |
| Crying or screeching of animals | 0.83 | .93 | .93 | 0.57 | |
| Screaming or crying of children/infants | 0.94 | .93 | .93 | 0.62 | |
| Whispers | 0.80 | .93 | .96 | .93 | 0.60 |
| Murmurs | 0.81 | .93 | .93 | 0.60 | |
| Marker on cardboard | 0.85 | .93 | .83 | .93 | 0.58 |
| Marker on whiteboard | 0.84 | .93 | .93 | 0.60 | |
| Fork scratching a plate | 0.95 | .93 | .93 | 0.58 | |
| Hearing mispronounced words | 0.91 | .93 | .85 | .93 | 0.61 |
| Listen to fillers | 0.90 | .93 | .93 | 0.64 | |
| Hear excessive use of letters such as s, r, ch, among others | 0.94 | .93 | .93 | 0.63 | |
| Block 2 | |||||
| See people who eat with their mouths open | 0.74 | .79 | .88 | .79 | 0.75 |
| See people talking with food in their mouths | 0.76 | .79 | .79 | 0.75 | |
| See people spitting | 0.90 | .81 | .81 | 0.66 | |
| See people chewing gum | 0.92 | .80 | .80 | 0.68 | |
| See people who talk or laugh very loudly | 0.87 | .82 | .58 | .82 | 0.59 |
| See people dancing | 0.75 | .85 | .85 | 0.31 | |
| See people who perform repetitive movements | 0.84 | .85 | .84 | 0.41 | |
| Block 3 | |||||
| Peers/colleagues | 0.60 | .54 | .54 | .54 | 0.63 |
| Unknown | 0.59 | .63 | .63 | 0.46 | |
| Partner | 0.69 | .70 | .78 | .70 | 0.36 |
| Parent/brothers | 0.74 | .63 | .63 | 0.47 | |
| Block 4 | |||||
| Labor relations | 0.86 | .79 | .83 | .82 | 0.73 |
| Studies | 0.76 | .81 | .83 | 0.70 | |
| Free time or recreation | 0.81 | .77 | .84 | 0.64 | |
| Love relationship | 0.81 | .70 | .72 | .84 | 0.63 |
| Relationship with parents and siblings | 0.81 | .70 | .84 | 0.63 | |
| Relationship with your children | 0.90 | .71 | .85 | 0.58 | |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Vice-Rector for Research and Graduate Studies of the Universidad Católica del Maule and does not include financial funds.
Ethical Approval
The Scientific Ethics Committee approved the study protocol and informed consent of the Universidad Católica del Maule, Act No. 25/2021.
Data Availability Statement
The datasets presented in this article are not available.