
Abstract
Given the limited and scattered data on nursing students’ behavioral intentions regarding interprofessional collaboration and the factors influencing them, there is a need for comprehensive, theory-driven research on the topic from nursing students’ perspectives. Using a theoretical framework provided by the theory of planned behavior, this study aimed to evaluate the behavioral intentions of Polish nursing students regarding interprofessional collaboration, including their attitudes, subjective norms, and perceived behavioral control. Sixteen nursing students participated in semi-structured interviews. Data were collected on the MS Teams application between February and May 2022 using a thematic guide created following manuals dedicated to the theory. They were thematically analyzed by two researchers using Atlas.ti Software. The results showed that students’ attitudes were mostly positive. The benefits of interprofessional collaboration included positive patient outcomes, exchange of mutual knowledge and expertise, comfort, and improved work atmosphere. The risks originating from human-dependent factors were viewed as a negative aspect. The relevant groups of people influencing their subjective norms comprised nursing community representatives, other medical professionals, patients, and members of society. Perceived behavioral control aspects covered the work organization, lack of incentives for collaboration, atmosphere and habits prevailing in the workplace, and insufficient practical experience and knowledge regarding collaboration. To conclude, although positive attitudes expressed by nursing students seem to constitute a positive predictor of their involvement in interprofessional collaboration, relevant decision-makers should address negative feelings and aspects identified during this study.
Plain language summary
Given the limited and scattered data on nursing students’ behavioral intentions regarding interprofessional collaboration (between representatives of different professions) and the factors influencing them, there is a need for comprehensive, theory-driven research on the topic from nursing students’ perspectives. Using a theoretical framework provided by the theory of planned behavior, this study aimed to evaluate the behavioral intentions of Polish nursing students regarding interprofessional collaboration. Sixteen nursing students participated in semi-structured interviews. Data were collected on the MS Teams application between February and May 2022 using a thematic guide created following manuals dedicated to the theory. They were thematically analyzed by two researchers using Atlas.ti Software. The results showed that even though interprofessional collaboration in Poland is currently limited, positive attitudes expressed by nursing students seem to constitute a positive indication for improvement. Students also expressed some negative feelings, which should be addressed. Patients, society, and most of the healthcare community were indicated as sources of positive pressure toward the behavior. However, there was a mixed sense of pressure from some nurses and doctors. Moreover, the process may be impeded by barriers to collaboration listed by students.
Introduction
The increasing complexity of patients’ health issues and needs calls for teamwork and collaboration among the medical staff in order to avoid the fragmentation of care and provide the best care to the patients, especially in the case of most fragile groups (Robben et al., 2012). A team can be defined as a group of at least two individuals (assigned with specific roles or functions and having a limited membership lifespan) interacting in a dynamic, interdependent, and adaptive way toward a common and valued goal, objective, or mission (World Health Organization, 2011). However, it should be emphasized that patient care is not a task for only one professional group. On the contrary, in line with the complex and interprofessional needs of the patients, also the provision and enhancement of healthcare require interprofessional efforts (Herrmann et al., 2015). Such an interprofessional collaborative practice is believed to occur when “health workers from different professional backgrounds work together with patients, families, careers and communities to deliver the highest quality of care” (World Health Organization, 2010). The literature provides many examples of the positive effects of interprofessional collaboration between different healthcare professionals on the quality of care, hospitalization length, patients’ satisfaction, safety, outcomes, and recovery, as well as the incidence of errors, inter alia (Lee et al., 2020; Lestari et al., 2019; Piquette et al., 2009; Song & Nam, 2022; Szafran et al., 2021). Consequently, it is nowadays considered a vital element in ensuring the provision of safe, high-quality, and patient-centered care (Lee et al., 2020; Lestari et al., 2019; Seaman et al., 2018; Song & Nam, 2022; Szafran et al., 2021). The benefits arising from interprofessional collaboration can also positively affect medical staff members as well as the healthcare system in the form of greater job satisfaction, more optimal use of human and financial resources, or better access of society members to healthcare (Prentice et al., 2015; Song & Nam, 2022). Therefore, interprofessional collaboration should be promoted in healthcare, and medical staff members should be encouraged to collaborate.
However, in this aspect, it is also important to consider whether healthcare professionals are willing to collaborate with representatives of other professions and which instances could influence their intentions in this regard. The same is also true for students of healthcare faculties, who will enter their respective professions in the near future. In their case, obtaining a detailed understanding of the issue could uncover potential areas for improvement or solutions that could be introduced already at the level of their studies. Studies conducted so far show mostly positive attitudes toward interprofessional collaboration among nursing and other healthcare students (Avrech Bar et al., 2018). Moreover, many studies have demonstrated that attitudes toward collaborative behaviors tend to be more positive attitudes among nursing students (Delunas & Rouse, 2014; Friman et al., 2017; Wilhelmsson et al., 2011) and nurses (Alsallum et al., 2019; Elsous et al., 2017; Kaifi et al., 2021; Sollami et al., 2015) in comparison with medical students and physicians, for instance. Similarly, in a study conducted on other student groups, nursing students were shown to attribute higher value to interprofessional education and be more open to interprofessionalism than occupational therapy, physical therapy, biomedical laboratory science, and radiography students (Almås & Ødegård, 2010). However, in another study, nursing students’ actual cooperation perception was slightly lower than occupational therapy and physical therapy students (Avrech Bar et al., 2018). The correlation between nursing students’ gender or personality and their readiness for interprofessional learning was also observed, for instance (Axelsson et al., 2019). Apart from that, little is still known about individual factors that could influence nursing students’ intentions toward interprofessional collaboration.
As it was demonstrated above, much of the research conducted so far has been focused on students’ attitudes. However, according to the theory of planned behavior (TPB) (Ajzen, 1991), whether a person undertakes a given activity is influenced not only by their attitudes but also by subjective norms and perceived behavioral control. Attitudes denote the extent to which given behavior is perceived as favorable or unfavorable, as well as beliefs in its expected outcomes. Subjective norms depict personally identified social expectations related to the behavior. Finally, perceived behavioral control assumes two aspects, namely individual’s control over the behavior and confidence in the ability to undertake it, including the influence of both situational and internal factors (Ajzen, 1991). In order to predict whether an individual intends to perform a given behavior, knowledge of all three elements is required. This means that even though students may hold positive attitudes toward interprofessional collaboration, their intentions toward it may also be influenced by social expectations and perceived behavioral control aspects, both positive and negative. The above-mentioned reports on differences in attitudes between nurses and nursing students and representatives of different faculties, especially physicians and medical students, may indicate the existence of groups that could view interprofessional collaboration less favorably than the nursing community and thus exert negative social pressure. This observation also seems consistent with the principle of least interest, suggesting that those in a position of power and traditionally higher in the hierarchy tend to be less eager to collaborate (Van Winkle et al., 2011). Furthermore, previous studies have also suggested some barriers to interprofessional collaboration, which may decrease the perceived behavioral control of future nurses, including the persisting authoritarian and hierarchical attitudes at the wards, the culture of a given profession, limited trust and awareness of the mutual roles, contributions, and competencies between different team members, as well as lack of time and remuneration for additional tasks (Friman et al., 2017; Kangas et al., 2021; Lestari et al., 2019). However, to the best knowledge of authors, no study so far has comprehensively examined the intentions of nursing students toward interprofessional collaboration in regard to all three above-mentioned variables. Consequently, given the limited and scattered nature of the available data on it from nursing students’ perspective, the topic seems worthy of examining with the use of a strong theoretical foundation as the lack of a robust body of theory-driven research is considered an important problem in medical education research (Cleland & Durning, 2019).
We decided to implement TPB in this study for several reasons. Firstly, one of the most significant contributions of TPB is the possibility of using intentions as proximal measures of behavior. Therefore, its variables can be used even in light of the lack of available measures of the actual behavior (Francis et al., 2004). We viewed this as an important asset in this study, given its topic and the study group involved. Moreover, our decision was aided by the results of a meta-analysis showing its efficacy as a predictor of intentions and behavior in the healthcare setting (Armitage & Conner, 2001) as well as a recent study, demonstrating its applicability also in regard to the topic of interprofessional collaboration on the example of Polish physicians and pharmacists or medical students (Przymuszała et al., 2023; Zielińska-Tomczak et al., 2021).
Taking all of the above into consideration, with the help of the theoretical foundation provided by TPB, this study sets out to explore the behavioral intentions of Polish nursing students in their last year of study toward interprofessional collaboration. The detailed study aims are as follows:
- to evaluate the attitudes of nursing students toward interprofessional collaboration
- to evaluate subjective norms and the sources of external pressure regarding interprofessional collaboration indicated by nursing students
- to evaluate the perceived behavioral control of nursing students regarding interprofessional collaboration
- to determine the direction of impact of the above factors on nursing students’ behavioral intentions regarding interprofessional collaboration.
Following the results of previously mentioned studies showing rather positive attitudes toward collaborative behaviors among nursing students (Delunas & Rouse, 2014; Friman et al., 2017; Wilhelmsson et al., 2011) and nurses (Alsallum et al., 2019; Elsous et al., 2017; Kaifi et al., 2021) in comparison with medical students and physicians, the principle of least interest, suggesting that those in a position of power and traditionally higher in the hierarchy tend to be less eager to collaborate (Van Winkle et al., 2011), and the barriers suggested in previous research on nursing students, we set the following hypotheses:
1) The attitudes of Polish nursing students toward interprofessional collaboration are mostly positive.
2) In students’ opinions, social pressure and expectations regarding interprofessional collaboration are rather positive. However, the sense of subjective norms is weakened by negative pressure from some of the representatives of the physicians’ community.
3) Students notice several barriers to interprofessional collaboration that negatively affect their perceived behavioral control.
Methods
Ethics Review
Before starting the study, its plan was subjected to the opinion of the Bioethical Committee of the Poznan University of Medical Sciences, which determined that in accordance with Polish law, the study did not demand its approval (Decision No. KB—928/21). Additionally, efforts were made to meet the highest ethical standards as indicated in the BERA Guidelines (British Educational Research Association [BERA], 2018).
Study Setting and Sampling
Invitations to participate in the study were sent to potential participants via social media, informing them about the study’s aims and voluntary character. During the study, we used convenience sampling. The sole inclusion criteria included being a student in the final year of a master’s degree in nursing studies and the agreement to take part in the study. No other restrictions on potential respondents were introduced, and we did not exclude any students who expressed their willingness to participate. Final-year students were selected as they potentially gained more experience during their education, suggesting they could provide the most detailed and thorough analysis of the issue, which deemed them the most suitable given the study aims. In total, sixteen semi-structured interviews with nursing students were conducted from February to May 2022.
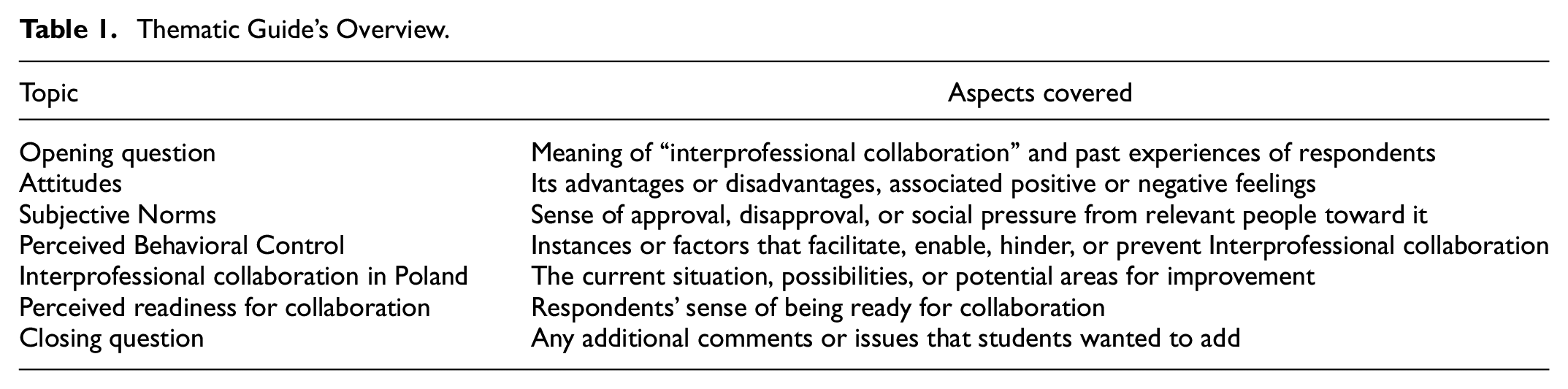
Due to safety concerns associated with the COVID-19 pandemic, all interviews were carried out with the help of the MS Teams application. For participants’ convenience, they were conducted at the most suitable time chosen by respondents. Furthermore, to increase respondents’ comfort during the interviews and avoid putting pressure on them with an intent to elicit their genuine thoughts and opinions, they were interviewed by the second author (also a nursing student). It also should be indicated that before the data collection process was started, she was prepared by the first and third authors for conducting the interviews by receiving information and explanation on TPB, principles of qualitative methods, asking questions, a detailed discussion of the thematic guide, and last but not least, a trial session, when she practiced posing questions. Before commencing the interviews, each respondent was once again informed about the aims of the study, the anonymity of collected data, and the voluntary character of their participation. They were also informed that the interviews were being audio recorded. Informed verbal consent was collected from all respondents participating in the study. The interviews were conducted using a thematic guide presented in Table 1. It was created with the help of designated manuals on TPB (Ajzen, n.d.; Francis et al., 2004).
Thematic Guide’s Overview.
Data Processing and Analysis
The interview recordings were then encoded and thematically analyzed by two independent researchers (researcher’s triangulation) for a broader research perspective and confirmation of its findings (Carter et al., 2014). Atlas.ti Software was used for data analysis. It followed the stages defined by Braun and Clarke (Braun & Clarke, 2006)— familiarizing with data, generating initial codes, themes searching and then reviewing, defining and naming themes, and at last, producing the report. The two above-mentioned researchers separately familiarized themselves with the data, generated initial codes, and created initial themes, and then in order to share their perspectives and increase their insight into data, they discussed them to create final themes and the final report. In case of their disagreement during the data analysis process, the disputed issue was to be discussed with the whole research theme. It should be emphasized that this process was mainly intended to increase insight into data. Data saturation was reached at the 14th interview when no new information was discovered. In order to ensure that, two additional interviews were conducted, aiding the decision to end data collection. The paper was written following the Standards for reporting qualitative research (O’Brien et al., 2014).
Results
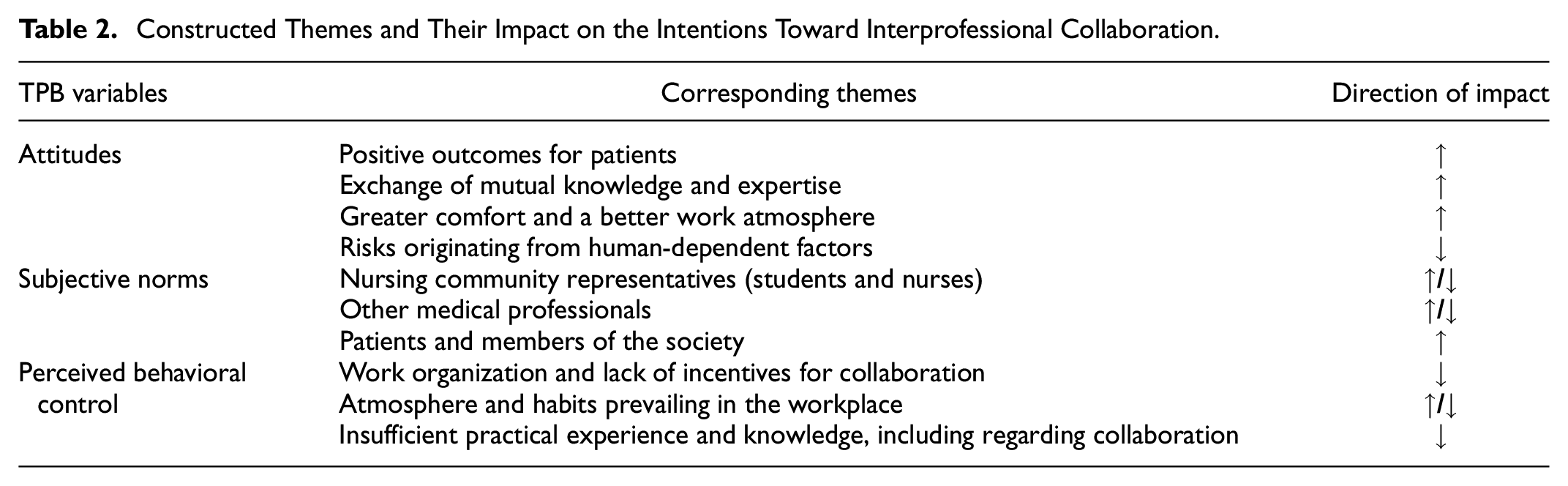
Sixteen semi-structured interviews with nursing students were conducted. Their average duration time was equal to 24 minute 55 seconds. All respondents were females. The themes created during this study were presented in Table 2 in relation to relevant TPB concepts to demonstrate their direction of impact on students’ intentions. They were also explored in the text below in more detail.
Constructed Themes and Their Impact on the Intentions Toward Interprofessional Collaboration.
The following themes pertaining to nursing students’
Positive Outcomes for Patients
Many benefits of interprofessional collaboration noticed by nursing students were connected with patients, who were seen as potentially benefiting the most from it. Respondents mentioned varying roles and contributions of different medical professions in regard to patient care. Among them, nurses were seen as spending the biggest amount of time with patients resulting in their better contact and more extensive knowledge of them, allowing them to detect early signs of deterioration of their condition, unusual symptoms for a given patient, changes in their mood, or their needs and communicate them further to other team members. The other way around, due to the amount of time spent with patients, nurses can also inform other professionals whether the patient understood or followed the recommendations. Therefore, a nurse was also perceived as a patient’s representative and a person binding the interprofessional team.
“Surely the greatest benefit is for the patient because the patient then receives, so to speak, a full package of services from people who are most experienced with them [the services].”
“A nurse is a person who actually knows the patient best […]. We know when their mood changes, what they need, when they are more sensitive, and when they feel worse, so I think that in the whole team, a nurse should be a party that binds the situation together and acts on behalf of the patient.”
Consequently, interprofessional collaboration and nurses’ participation in it was recognized as allowing for a broader picture and better understanding of the patient’s condition, translating into better and more comprehensive care. The improved patient outcomes mentioned by students included, among others, patients’ satisfaction, better quality of provided services, faster recovery, and fewer complications, adverse events, or medical errors.
“I think that the effects are visible later in such a ward that you can simply see it, I do not know, that there are fewer complications, certainly less of some adverse events.”
Exchange of Mutual Knowledge and Expertise
Collaboration between representatives of different professions was also perceived as an occasion for mutual exchange of knowledge, skills, and experience, resulting in professional growth, nurses’ development, and greater engagement in patient care. Development occasions were also noticed regarding interpersonal and communication skills.
“Even though all medical fields of study are similar, in the sense that there are similar subjects, inevitably, each of us knows something different and specializes in something different. I think such cooperation would be quite important because everyone is a bit of a specialist in their field, and by exchanging experiences, knowledge, or anything, without judging, one can learn a lot.”
“A positive thing would be that I could learn more and help these patients. […] also just getting along with people, developing interpersonal relationships, deepening my knowledge.”
Additionally, the knowledge and expertise of other team members were also seen as a possibility to seek advice and help in case of uncertainty or lack of knowledge on a given topic or procedure.
“It is nice to work when you know that you can rely on someone, and someone has knowledge that can complement your knowledge and experience.”
Greater Comfort and a Better Work Atmosphere
Consequently, collaboration in an interprofessional team was also seen to contribute to better conditions, comfort, and atmosphere at work, increased effectiveness, and a lowered burden on individual team members. Students’ arguments for increased comfort and conditions of work as a result of interprofessional collaboration involved, among others, the possibility to rely on other team members’ knowledge and expertise as well as help each other, optimize and relieve the work of members of different professions.
“I see a lot of advantages in this collaboration, and it would be nice to create such collaboration between other professions because it brings benefits, not only for the patient but also for us because our work is better, much more pleasant, and much more effective.”
“Certainly, not only one professional group is burdened with a given, I do not know, disease entity or patients, but many people can get involved in it.”
“Above all, I think [the feeling of] peace because I have certainty that when I do not know something, another person will be able to advise me on a given topic. This is probably my best feeling - such inner peace.”
Risks Originating From Human-Dependent Factors
Despite its advantages and the benefits that interprofessional collaboration may bring to their future work and patients, nursing students also noticed associated disadvantages or difficulties. However, they seemed not so much to be a result of interprofessional collaboration as such, but rather a mix of various human-dependent factors, including stereotypical views of different professions, mutual animosities, sense of losing one’s competencies, fear of coming off as uneducated or unprepared in front of other professions or being taken advantage of and conflicts or communication problems within the team.
“There is such a big risk because everyone is, let’s say, a specialist in their field, and when we want to ask something, we also show that we have some shortcomings. […] Asking others and cooperation with others uncovers one’s shortcomings, and I think that it is difficult […]. It is also known that you can encounter people who, in such a situation of dividing duties between several people, will take advantage of them, who will not do their part but will somehow prey on you and your diligence, whatever, and then for me, it is not really a collaboration, there is always a risk that someone will not do their piece of work.”
“I think that the idea of an interprofessional team does not have disadvantages as such, although I know that in practice there are certain stereotypes, maybe you can call it that. A lot of people are also prejudiced due to some typical stereotypes that a doctor and a nurse do not get along, that a doctor looks down on a nurse or physiotherapist - well, these are some flaws, first of all, that somewhere in people’s minds they cannot go beyond that and focus only on the patient, they just replicate these stereotypes all the time […]. Sometimes there are situations where maybe it is not that communication fails, but sometimes just some people do not listen to each other, and then situations arise that someone is angry that someone did not tell them something about the patient, and then there are problems […].”
“Disadvantages? In theory, I could say that someone could complain that some of their competencies are taken away or something like that - I do not know. There are more advantages than disadvantages - I have such an impression. […] Negative would be that I would be afraid that someone could see that I have some gaps in knowledge.”
Relevant groups of people listed by the respondents as part of
Nursing Community Representatives (Students and Nurses)
Other nurses and nursing students were viewed as having rather positive beliefs about interprofessional collaboration. As representatives of the respondents’ profession, they seemed to constitute an important source of potential pressure. However, students’ perceptions of this group and the attributed beliefs about the behavior differed depending on its members’ age, educational background, and professional experiences. The most positive opinions about interprofessional collaboration were assigned by the respondents to nursing students and young nurses. As respondents noticed, members of this group may be, in general, more ambitious and willing to learn, broaden their horizons, try something new, or introduce some changes and innovations to patient care. They were also viewed as less likely to be burnout or already accustomed to their duties or professional roles. Also, the curricula of contemporary nursing study programs emphasize the significance of interprofessional collaboration more than in the past.
“From my perspective, where during studies we were taught all the time somewhere that it is better, so to speak, to cooperate for the benefit of the patient […], for sure nursing studies and future nurses are prepared for this that you cannot look down on each other, that each of us should work together. I think they would be very supportive.”
“Yes, the young ones because we have such young blood in us that we probably want it, that is one thing. Secondly, we are not burnt out yet professionally, and I think it speaks very much through us.”
Older generations of nurses were seen as potentially more reluctant to establish interprofessional collaboration due to conflicts in the environment or because it would entail changing their habits or the necessity to learn something new, like competencies of other professions. Longer work experience of older nurses was also perceived as contributing to a higher risk of professional burnout, which also was seen as limiting their willingness to engage in something new.
“Due to how it used to be, there are still consequences of the old system. And I also think that some nurses… most nurses do not want to—they rest on their laurels and do not want to learn [something new]. And it is like they are closing up a bit because of it.”
“I think that the oldest generation of nurses is rather not willing to undertake such cooperation, and I think that the oldest generation of doctors is also not willing to undertake such cooperation […] I think it is because this oldest generation is most conflicted with each other, and besides, I think that they do not find each other in their mutual competencies - that these older doctors have no idea what a nurse is really supposed to do, and older nurses also have different education, and I think that they often hesitate about what belongs to their competences.”
Other Medical Professionals
Similar observations in terms of age differences were also made about other medical professions. Students believed that the medical community would rather have positive views toward collaboration with nurses due to its many aforementioned benefits. Younger representatives of medical professions were viewed as more open to the idea of interprofessional collaborations, while older members of the medical community as potentially more reluctant. Among different professions, respondents paid much attention to physicians who may sometimes either not see the need for the collaboration or associate negative feelings with it due to their pride, overconfidence, lack of interest in other professions’ opinions, or fear of losing competencies and authority.
“I think that generally looking at it, the young generation would be more willing to undertake it, regardless of their profession. However, it seems to me that doctors, until they come across the negative consequences of the lack of such cooperation, do not see this need. […] These are my feelings—that they turn their noses up and think they know everything best. But then it turns out that not necessarily, and at this point, they change their attitude a bit.”
“From observation, I believe that older people, 50+ type, as well as nurses, doctors, and other professions, seem to have a tough time adapting to it because when they were learning, everything was completely different. There was a different pattern to these competitions, and I think it is hard to adapt to what we are learning now that such a thing should exist.”
“I think the nurses would definitely approve. It seems to me that so would doctors, at least most of them, and rather the younger ones […]. I do not know about other professional groups because I do not deal with them much. But I think, I do not know, dietitians for sure because if they have good contact with nurses who see these patients on the ward, there will be better information and feedback, and they will be able to find better solutions, so I think that all groups should want it.”
Patients and Members of the Society
On the other hand, broadly understood members of the society were believed to hold predominantly positive views about the nurses’ involvement in interprofessional collaboration due to its many advantages. The society in this context included the general public, including patients, respondents’ family members, superiors, or hospital management.
“Well, I think everyone would be happy, including the patient. Because for the patient, it would only mean benefits. […] Besides, the whole society would be happy, we would be better off, and the health care system would not look the way it looks. […] I think that even the management [of the hospital] would be pleased.”
“It seems to me that the patients, if it were explained to them what such an interprofessional team is all about, would be most in favor because each of us would like to be provided with professional care in every aspect of medicine. If I had to talk, for example, with my grandparents, I think they would like a nurse, a doctor, a physiotherapist, and a nutritionist to take care of them. I think such people would feel more taken care of, and maybe they would also have greater trust in the medical staff.”
“In fact, even when it comes to my family members, if it appeared somewhere in the conversation, then their approach to such matters was like—that is great!”
The instances influencing participants’
Work Organization and Lack of Incentives for Collaboration
Among factors potentially influencing their perceived behavioral control, nursing students mentioned organizational aspects like physical barriers between employees from different professions (e.g., separate rooms and offices), lack of time due to insufficient numbers of medical staff, or perceived lack of incentives or motivational factors for interprofessional collaboration. An example of such an incentive was additional remuneration or salary increase, which seemed to suggest that collaboration may not be viewed as an inherent part of their work. Time savings as a result of more efficient work organization were also mentioned.
“It also makes it difficult that our offices are often far away, and one is always closed, and there is no way to get inside. It also gives such a strange perspective. If I need something, there cannot be a situation that I will come in, and we will sort of talk as equals—here I mean these kinds of non-verbal factors that affect communication—only I am standing, he [the physician] is sitting. That is already showing that it is not a collaboration. Collaboration is with people who are on the same level.”
“Time—unfortunately, the hospital is also poorly staffed when it comes to the personnel, whether it is nurses or doctors. Everyone is busy, and this also certainly contributes to the fact that this cooperation is limited.”
“Certainly earnings […] If someone wants to be a volunteer and work in such a team, there will certainly be such people, but there are also people for whom the main category is simply earnings, and this is what people are guided by.”
Atmosphere and Habits Prevailing in the Workplace
The atmosphere and relations existing on the ward were also seen as factors influencing respondents’ perceived behavioral control toward interprofessional collaboration. Nursing students acknowledged that it would be easier for them to establish interprofessional relations if the members of the team they entered were open, polite, empathetic, and positive toward them and if such interprofessional relations were already a norm in their new workplace. In this context, observations were made that it may come more naturally in some working environments due to the character of work (e.g., emergency medicine).
“Most of all, the kindness of my co-workers - the fact that I am not afraid to approach them and ask, for example, something I do not know because I know that I will not be reprimanded […] the atmosphere is the basis of every good relationship and every cooperation.”
“Certainly, if I knew that I was to be employed in a ward and that something like this existed there, it would encourage me to go deeper into it. If they would ask me for my opinion—these other employees and other professions. Because this is, you can say, such a mini-appreciation if someone asks you for your opinion: what do you think, is it a good solution or not?”
On the other hand, conflicts and a tense atmosphere in the ward were seen as impeding factors. Similarly, students noticed it would be harder to collaborate if they knew or saw that other healthcare team members were unwilling or negative about it. One student (S12) compared this situation and the frustration associated with it to “hitting the wall.”
“Probably some customs in this ward, or the age of these people who may have some other habits, or that it was simply always like that in this place that someone was the boss, someone carried out orders, and it will be very hard to change that.”
“I am discouraged by the reluctance of others—if someone would not be in favor of it or would hinder any activities or try to discourage me.”
The potential risk of the unwillingness of other team members was also associated with the issue of who should initiate such collaboration attempts and nursing students’ uncertainties and worries in this regard, especially when it comes to contact with physicians. The need for greater integration between different healthcare team members was noted in the form of joint integration meetings outside of the work scenario. Expectations of greater involvement of the managing bodies were also raised as the entities who should set the example and control the implementation of collaboration.
“The management should also pay more attention to it in the [employees’] evaluation, send us to some training also in the field of communication and collaboration. […] Additionally, what I miss is that the head of the nurses at the ward, as a person directly superior to their nurses, but also the head of the ward, as the superior of doctors, and so on, would monitor how people work. Or, I do not know, the professor at the ward could create some kind of team that monitors it regularly and catches that someone has a problem, and I do not know, someone argues with someone, and so on so that some mediations were done here in this direction and not that there is some conflict and nothing is done about it.”
“It would be nice to have some integration meetings to get to know each other at a slightly shorter distance. It would also be nice to have some training on talking or solving problems together […]. [There is a lack of] someone who would lead it all because I might want to cooperate, but I do not feel like someone who will suddenly go to doctors or other team members and preach a theory about the greatness of cooperation. It would be nice if there were a person responsible for this communication and cooperation who knows how to do it and how to lead employees.”
Insufficient Practical Experience and Knowledge, Including Regarding Collaboration
Nursing students’ insufficient knowledge and experience were also seen as a barrier. On the one hand, it involved potential gaps in their medical knowledge. On the other hand, it also involved a low level of knowledge about interprofessional collaboration, opportunities, and mutual roles and responsibilities.
“I think that a difficulty in establishing such cooperation is that very often members of the team do not know each other’s competencies, and this is where many misunderstandings arise, and it is precisely this miscommunication that often causes this cooperation to fail and that there are negative attitudes towards it. […] I know how much knowledge I lack. I think that this is it, that I am at the beginning of my professional career, and despite such theoretical knowledge, sometimes it is still difficult for me to translate it into practice, and that is why I sometimes feel that I do not know something and that I will make a fool out of myself […]. I also often do not know what belongs to other people’s competencies, and as far as it is easy for me to find myself in what belongs to my competencies because even if I hesitate, I know where to check it. If I had to, for example, find the competencies of a physiotherapist or a laboratory diagnostician, I would have a problem with it. And then, if I do not know what the other person’s competencies are, the other person either does not know or does not want to tell me what competencies they have, it is really difficult to establish such cooperation, and I regret that we do not have such knowledge.”
“Definitely, [I lack] such understanding and showing me how the work of a doctor, a midwife, a physiotherapist, or a dietician looks like, for example, these basic professions that are part of the team. What their work looks like? What is it about? What is the scope of their duties? And what overlaps in our fields and what does not? Because we may think we know, but then various things come up, and it turns out that what we thought was so obvious is not.”
To amend this situation, nursing students provided various solutions, including additional courses on communication and collaboration and the broader implementation of interprofessional and communication skills learning at the undergraduate level, like common classes or the use of simulated conditions in medical simulation centers.
“I think that such courses should be provided in hospitals on what an interprofessional team is and how to best shape it, modernize it, and how people should communicate with each other. […] As we know, the average age of doctors and nurses in Poland is very high, and some people may know the definition, for example, but may not know how it works, that this is how it should be done. There is nothing wrong with not knowing, and it is only important that they want to learn it and keep developing because if we stick to the past, we will not achieve anything. We have to move on with the times, we have to develop. As medicine develops, so should our communication.”
“I think that it would have to be resolved at the level of studies—that these different faculties should have some classes together and learn what the tasks of these other professions look like to simply know, respect, and already at this level learn how to work together […]. Because later, when you enter the hospital environment and such a ward, where the same people have been for 40 years, it is hard to do it because every new person who enters there, well, willy-nilly, they will pick up their habits because they will not have the clout.”
“A lot could be done during studies. I would really like such communication classes. One thing is that I would like to have such classes, and two, I would really like other professional groups also to have such classes, and I think it would also be a nice idea if we could have some of these classes together when possible. […] If we could all meet in such real conditions, for example, within the simulation center, and have the opportunity to observe each other’s work. And then we would learn from the beginning that everyone does a slightly different thing, but together we can do something best, and I think that then we would also acquire such respect for each other’s work.”
One participant shared her experiences after an interprofessional class with physical therapy students.
“The first thing that comes to my mind are classes together already at the level of studies. We had one such example, I remember not all groups, but we had classes with physiotherapists, and we had a task to do, but it was amazing because then I first noticed that it was one problem but two solutions. So, it seems that the longer we would not separate ourselves as professional bubbles, the better it would be because the younger you are, you are more flexible, the faster you learn, the easier it will be later.”
Discussion
This study aimed to examine Polish nursing students’ intentions for interprofessional collaboration using TPB as a theoretical framework. For this purpose, following TPB principles, we needed to explore three elements influencing their intentions, namely attitudes, subjective norms, and perceived behavioral control.
Our first aim was to evaluate the attitudes of nursing students toward interprofessional collaboration, which according to the theory, denote their positive and negative beliefs about the behavior and its presumed outcomes (Ajzen, 1991). We hypothesized that the attitudes of Polish nursing students toward interprofessional collaboration would be mostly positive, and as our results show, this hypothesis was confirmed. The prevailing positive attitudes of students are consistent with previous research on nursing and other healthcare students (Avrech Bar et al., 2018).
When it comes to the nursing students’ positive beliefs regarding interprofessional collaboration, its benefits include positive outcomes for patients, the possibility for the exchange of mutual knowledge and expertise, greater comfort, and a better work atmosphere. The only negative aspects of interprofessional collaboration noticed by nursing students in our study were connected with human factors, with provided examples focusing on existing stereotypes about different professions, conflicts or communication problems, fears of losing one’s competencies, coming off as uneducated or unprepared in front of other professions or being taken advantage of. The positive effects of interprofessional collaboration on, inter alia, patient health outcomes, recovery, satisfaction, and quality of care mentioned by nursing students in our research were also previously listed by other authors (Kaifi et al., 2021; Lee et al., 2020; Lestari et al., 2019; Seaman et al., 2018; Song & Nam, 2022; Szafran et al., 2021). For our respondents, they were a result of differing roles and contributions of team members and how they can complement each other. The time spent by nurses with patients was also raised in this aspect as contributing to the ease of contact and their knowledge about patients allowing them to catch any new symptoms or deterioration of their condition, react to their specific needs, or verify their compliance with doctors’ orders, for instance. As a result, nursing students saw their profession as facilitators of the two-way information flow between patients and other team members and an integral part of the team. Similar perceptions of nursing students were also documented in previous research, in which they described nurses’ roles as holistic and oriented toward close and better contact with patients, while doctors’ roles as more disease-oriented and focused on diagnosis (Friman et al., 2017). Another study also demonstrated similar differences between nursing and medical students’ perceptions of both professions. While nursing professionals were believed to have better knowledge of patients and be more caring, doctors were portrayed as having a more formal approach (Salberg et al., 2022).
Moreover, in line with our respondents’ perceptions, other studies also show that interprofessional collaboration not only positively impacts patient outcomes but also the conditions of healthcare professionals’ work. Several studies demonstrated that non-successful collaboration or disruptive behaviors negatively influence staff members’ concentration, stress levels, fatigue, turnover intentions, and interpersonal relations (Kvarnström, 2008; Rosen et al., 2018; Rosenstein & O’Daniel, 2005). Finally, as evidenced by accounts of medical and nursing students participating in an interprofessional patient assessment program, such experiences can also help notice their shortcomings and serve as a platform for exchanging points of view on patient care (Kara et al., 2018). Another study also revealed students’ perceptions of interprofessional collaboration as mutually beneficial for healthcare team members and providing them the opportunity to learn from each other (Kangas et al., 2021).
Our second aim was to evaluate subjective norms regarding interprofessional collaboration indicated by nursing students, signifying their sense of social expectations or pressure from others regarding a given behavior (Ajzen, 1991). We hypothesized that students would feel mostly positive social pressure and expectations regarding interprofessional collaboration, which was confirmed during the study. However, we also assumed that this positive pressure could be weakened by negative pressure from some of the representatives of the physicians’ community, and as we described below, this also finds support in the findings.
Our participants’ subjective norms included the following relevant groups of people: nursing students and nurses, other medical professionals, patients, and broadly understood members of society. Among them, current or future representatives of their profession were regarded as rather positively oriented toward interprofessional collaboration. However, the potential influence of age, educational background, and professional experiences in this regard were also noticed. Previous research also covered potential differences among them depending on certain features. For example, nursing students’ personality was found to correlate with their readiness for interprofessional learning, with more outgoing, open-minded, and agreeable students being more ready for it (Axelsson et al., 2019). Also, female nursing students seem more positive regarding collaboration than their male colleagues (Axelsson et al., 2019; Wilhelmsson et al., 2011). Given the advantages of interprofessional collaboration, members of other medical professions were also viewed as mostly positively inclined toward it. However, potential differences were described by students, especially regarding age and the represented profession. While younger healthcare staff members were seen as rather open toward collaboration with nurses, older were perceived as more hesitant. Physicians were also given as an example of a professional group, in which some of its members may look unfavorably upon the idea of interprofessional collaboration with nurses for reasons like being overly confident in their abilities, not being interested in the opinions of other team members or fearing the loss of authority and competences. This view seems to be supported by the results of another study, in which nursing students also viewed older doctors, particularly males, as more authoritarian and order-giving, while younger doctors were expected to be more open to listening to them (Friman et al., 2017). In this context, previous studies also show that nursing students tend to have more positive attitudes toward interprofessional collaboration than medical students (Delunas & Rouse, 2014; Friman et al., 2017; Wilhelmsson et al., 2011). A similar trend is also observable among nurses and physicians (Alsallum et al., 2019; Elsous et al., 2017; Kaifi et al., 2021). On the other hand, there are reports of nursing students’ slightly lower actual cooperation perception than occupational therapy and physical therapy students (Avrech Bar et al., 2018). Finally, the advantages of interprofessional collaboration in terms of the quality of patient care and outcomes described in detail above also seem consistent with nursing students’ anticipation of its positive reception by patients and society.
Our third aim was to evaluate the perceived behavioral control of nursing students regarding interprofessional collaboration, which represents their confidence in the ability to carry out the behavior in question and their control over the process (Ajzen, 1991). We hypothesized that students would report several barriers negatively affecting their perceived behavioral control in this aspect, and it was confirmed. In the case of our respondents, the instances mentioned by them included organizational aspects, the separation between different professions, an insufficient amount of time and members of the medical staff, lack of incentives or motivational factors, the role of existing atmosphere and relations in the workplace, willingness and attitudes of co-workers, perceived support and expectations of managing bodies, or students’ insufficient experience and knowledge, both medical and related to collaboration and roles and responsibilities of other professions.
Existing literature also attests to similar factors preventing effective interprofessional collaboration like low knowledge and trust in the expertise of other team members, limited understanding of their contributions and problems with contacting them, the culture within a given profession, limited time, and lack of remuneration (Lestari et al., 2019). Other important factors mentioned by nursing and medical students in a recent study included the need for a clear and effective care pathway and policies, functional environment (observation similar to the separation between different professionals described in our study), and resources, as well as the awareness of mutual roles and competencies, among others (Kangas et al., 2021).
Working with other professions may still be troublesome for healthcare professionals due to gaps in their collaboration and communication competencies (Digregorio et al., 2019). The situation seems to be additionally hindered by the persistence of authoritarian and hierarchical attitudes, noticeable already to students (Friman et al., 2017). In fact, the ability to collaborate with members of other professions does not seem intuitive or easy to acquire later in professional life. Instead, it should be developed as an integral part of undergraduate education programs, as noticed by our respondents and previous research (Axelsson et al., 2019; Barnsteiner et al., 2007; Song & Nam, 2022). Such an educational approach in the form of interprofessional education is supposed to provide students of different healthcare faculties with opportunities to “learn about, from and with each other to enable effective collaboration and improve health outcomes” (World Health Organization, 2010). As previous studies show, it can have a positive effect on healthcare students’ awareness and knowledge of other professions’ roles and competencies, as well as their attitudes and self-efficacy in this regard (Kent & Keating, 2015; MacLeod et al., 2022; Thistlethwaite & Moran, 2010). Importantly, even a simple interprofessional course, organized without creating substantial costs, can bring positive effects, which means that similar initiatives can be implemented even in a limited resource setting (Cerbin-Koczorowska et al., 2022). Moreover, interprofessional education can also act against the formation of prejudices or negative attitudes among healthcare professionals (Ferri et al., 2018). Also, informal communication between students can have positive effects (Herrmann et al., 2015). However, as also expressed by our respondents, it seems that such occasions for student socialization or integrated interprofessional learning are still limited both in Poland and in other countries because of the organization of the learning process in medical universities and profession-specific curricula of individual faculties (Cerbin-Koczorowska et al., 2020; Chua et al., 2019; Herrmann et al., 2015). Therefore, to ensure that graduating nurses are ready for interprofessional collaboration, interprofessional learning experiences should be integrated into nursing curricula (Murdoch et al., 2017).
The final aim of the study was to determine the direction of impact of the identified factors on the behavioral intentions of nursing students regarding interprofessional collaboration. As presented in Table 2 and discussed above, Polish nursing students hold mostly positive attitudes toward interprofessional collaboration, which increase their behavioral intentions. However, some negative attitudes and feelings are also present, reducing these intentions. Depending on the referenced groups of people, social expectations identified by the respondent were mostly positive, having a positive impact on behavioral intentions. However, a reported mixed sense of pressure from some nurses and physicians may have a discouraging effect on students. Finally, students referenced multiple barriers to collaboration, which seemed to decrease their perceived behavioral control, and, thus, can reduce their behavioral intentions.
The results of this study lead to the following implications and suggestions for policy-makers, managers, and other authors:
1) The positive effect that the awareness of the benefits of interprofessional collaboration has on nursing students’ intention to collaborate should urge the stakeholders and educators to emphasize them to the students on different occasions. These may include various forms, both formal and informal, including official documents and reports, textbooks, conferences, nursing curricula, or classes with students.
2) The negative aspects and difficulties associated with interprofessional collaboration should also be taken into account, and appropriate steps should be taken to address them appropriately, for example, in the form of conflict-solving or communication skills learning or actions aimed at increasing students’ confidence in their abilities.
3) The effect of social pressure on students’ intentions should be considered. Positive sources of subjective norms should be strengthened, and the awareness of their existence should be increased among the students. On the other hand, efforts should be taken to reach those groups or individuals who may constitute sources of negative pressure and attempt to address their negative feelings or prejudices to show them the benefits of collaboration.
4) Barriers identified in the study, including the work organization, lack of incentives for collaboration, atmosphere and habits prevailing in the workplace, and insufficient practical experience and knowledge regarding collaboration, should be approached, and attempts should be made to eliminate them.
5) As an interprofessional collaboration, per definition, requires the participation of representatives of different healthcare professions, further research should focus on identifying factors influencing the perceptions and intentions of students and healthcare professionals with different educational backgrounds. It would also seem beneficial to verify whether aspects identified during this study would also be prevalent in other countries and settings. A quantitative investigation of a representative population of nursing students could be considered to confirm and broaden the results of this study.
The strengths of this research comprise its robust theoretical framework in the form of using the theory of planned behavior as well as an important but so far not enough studied topic of nursing students’ behavioral intentions for interprofessional collaboration.
Limitations
The results presented in the study should be interpreted within its weaknesses and limitations. Firstly, the risk of author bias should be mentioned, although countermeasures were introduced to reduce it, and we took several steps to validate obtained data. Authors with diverse backgrounds were invited to participate in the study to account for the risk of potential author bias – they involved both representatives of the nursing community (a nurse and a nursing student) and other professionals (two physicians and two pharmacists). All interviews were recorded to ensure the high quality of the data obtained. We followed a recognized data analysis method and used researcher triangulation to broaden the research perspective and gain confirmation of its findings. What is more, we collected data until saturation was reached, and when preparing the paper, we followed Standards for reporting qualitative research guidelines. The next limitation we noticed is that convenience sampling could indicate that the individuals interviewed may have had firmer beliefs on the topic than their peers. Moreover, adopting a remote method for conducting interviews can also be a source of interview errors. To prevent that, at different stages of the study, potential participants were reassured of the significance and validity of all their views and opinions and invited to express them freely. Also, apart from their consent to participate and last-year nursing student status, no other inclusion criteria were introduced. Moreover, to minimize the chance that students may want to conceal their real beliefs, as indicated above, the interviews were conducted by another nursing student after her thorough preparation by the research team members. Also, the interviewer attempted to hide her personal views on the topic and not to suggest the responses to the participant. We also put great emphasis on making the respondent feel comfortable during the interviews, for instance, by letting them choose the most suitable time for them to conduct it and giving them a chance to warm up to the subject with the use of an opening question, which also helped us to verify that the respondent would know what we mean by interprofessional collaboration. In the case of online interviews, a potential problem that could have occurred is interruptions due to connection problems. Therefore, before starting to talk, the interviewer ensured the respondent was done talking. Another issue that could be considered a limitation of the study is the fact that all our respondents were females, as gender differences could also have an impact on the results. While we are aware that the situation may look different in some countries, in Poland, the nursing profession is still feminized, and a vast majority of nurses and nursing students are female. For example, when we conducted our study, there were approximately 70 final-year nursing students that year. Among them, there was only one male student, and the rest were female. Unfortunately, this one male student did not want to participate in the study—students’ participation was voluntary. However, given that proportion, we believe that our study sufficiently represents the examined population.
Conclusion
Given the importance of interprofessional collaboration in the healthcare system, it seems vital to carefully explore students’ behavioral intentions to obtain detailed insight into the topic and uncover areas for potential improvements or interventions if required. In this study, the intentions of nursing students were examined. Although, as students noticed, the current state of interprofessional collaboration in Poland is limited, their rather positive attitudes indicate a potential for improvement. However, their reservations and fears expressed throughout the study should also be addressed. Also, their subjective norms, especially involving patients, society, and most healthcare community members, indicate rather positive pressure toward the behavior. However, this effect can be diminished due to a mixed sense of social pressure from some nurses and doctors. Moreover, barriers to collaboration listed by students seem negatively affect their perceived behavioral control, which may impede the process. It seems necessary to confirm the results of this study on a representative population of Polish nursing students, which is why we intend to develop a dedicated tool on the matter and use it in a survey study on Polish students.
Footnotes
Acknowledgements
We would like to thank all the students who agreed to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The Bioethical Committee of the Poznan University of Medical Sciences determined that, in accordance with Polish law, the study did not demand its approval (Decision No. KB—928/21).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.