
Abstract
The purpose of this paper is to identify the intervention components, key actors and models of social innovation that can contribute to the improvement of health rehabilitation services from a biopsychosocial perspective, aimed at people with lower limb amputation in a situation of disability. Likewise, it aims to analyze the ways in which Community Based Rehabilitation (CBR) facilitates the elimination of barriers in rehabilitation services and promotes a better quality of life for people with disabilities. A systematic review of scientific literature for the period 2001 to 2019 was carried out, starting with a bibliometric analysis of publications found in the Web of Science and Scopus databases; followed by content analysis with NVivo 12 software. Among the findings, it was identified that the optimization of health services for the population with disabilities in emerging countries requires investment and training. In addition, the success and deficiencies in CBR programs were analyzed, since according to the systematic review, these are limited to the care of people with lower limb amputation in contexts of armed conflict.
Keywords
Introduction
Lower extremity amputation is common in contexts of armed conflict, specifically due to Anti-Personnel Landmines (APL), Unexploded Ordnance (UXO) or Improvised Explosive Devices (IED) (United Nations, 2015). People enduring this situation suffer significant sequelae in their quality of life, with functional, psychological and social side effects (Nizamli, 2020). They must also adapt to facing an altered physical reality and the initial loss of independence, while the rehabilitation process is activated (Deepak et al., 2023; Sureshkumar et al., 2024).
According to Nussbaum (2008), from a capabilities perspective, quality of life focuses on distinctive elements such as health and body integrity, in which the attainment of human dignity is a governmental task granted through public policies that define equitable living conditions, in addition to the freedom related to health care, which according to Sen (2000) promotes quality of life and development. In this framework, Saravanan and Menold (2023) found that factors such as the type of social security coverage, the care of health professionals, the financial situation of the amputee patient, the ability to cover the cost of the prosthesis and access to appropriate devices have an influence on the rehabilitation process.
As mentioned, it is important that health systems offer quality services in which the perception and participation of the patient are taken into consideration, with respect to their rehabilitation process (Matos et al., 2020; Sayeed et al., 2024). Likewise, Dhole et al. (2021) infer that the design of protocols to conduct individualized rehabilitation is fundamental, based on the functional capacity of the person, along with their motivations and socioeconomic conditions.
Since health services for people with disabilities due to lower extremity amputation are complex due to the aforementioned factors, Community-Based Rehabilitation (CBR) emerges as a globally proposed strategy to improve the quality of life of this group, mainly in emerging countries (Muñoz et al., 2020). CBR comprises five dimensions: health, education, livelihoods, social and empowerment (Raha et al., 2023). Some programs implement inclusive education, institutional networks and early intervention (Jose et al., 2023); however, there remain gaps that influence the continuity of the rehabilitation process and the reintegration by the person into the community (Sayeed et al., 2023b).
In Colombia, CBR has contributed to the promotion of guarantees for health provision in regions where infrastructure for primary care is limited; consequently, this strategy is cross-sectional at the community level, through actions focused on the person with disabilities, their families and the community (Ortiz et al., 2014). According to Bachfischer et al. (2023), the perceptions of people with disabilities in Colombia show a level of dissatisfaction regarding community participation in their rehabilitation process; that is, the community component is not a priority. Hence, limitations associated with geographical, economic and cultural barriers that prevent social inclusion arise (Agudelo-Hernández & Rojas-Andrade, 2023).
The Ministry of Health and Social Protection of Colombia (2014) defines CBR as:
A socio-economic development and social inclusion strategy to meet basic needs, create opportunities, develop capacities, support and work with Disabled People’s Organizations and Support Groups, involving intersectoral participation, promoting the leadership and participation of local governments and taking advantage of the country’s legislative, legal and social systems. (p. 17)
CBR arises within the framework of the biopsychosocial model, which integrates biological, individual and social perspectives (World Health Organization, 2010). On the other hand, the medical model has traditionally focused on the recovery of the patient’s physical health, failing to address traumatic events that affect a comprehensive rehabilitation process (Pérefdz & Chhabra, 2019); concurrently, the social model understands and addresses the systematic barriers that hinder a person with disabilities from equal access to human rights (McCusker et al., 2023). For this study, rehabilitation is considered a multilevel and multisectoral process in which professionals, families and communities collaborate to achieve a better quality of life. That is why the process must be holistic and include assistive technology, education, job training, sports, arts and recreation, with the joint participation of caregivers and families (Toro-Hernández et al., 2019).
Due to the holistic and multisectoral nature of CBR aimed at people with disabilities due to lower extremity amputation, it is important to inquire about the elements of social innovation that integrate these intervention processes and provide tools that facilitate daily life. For example, a study conducted by Pritvorova et al. (2022) shows an innovative proposal related to subsidizing energy services for families with disabled children, thus integrating social assistance with the purchase of appliances and rehabilitation equipment with energy-saving characteristics. Mohamad Hashim et al. (2022) present a community initiative that adopts affordable 3D printing technologies for the prescription of adaptive and assistive devices required by people with disabilities.
Through a systematic literature review, we seek to collect evidence on the trajectory and transformations of the CBR process at the global level over two decades with a retrospective view, (LeCroy et al., 2023; Sumner et al., 2023), focusing on people with lower extremity amputation in a situation of disability. From the field of public health in Colombia, the scientific community has recognized the importance of establishing a Disability Research agenda (Cruz-Velandia et al., 2017) that integrates aspects of the armed conflict (Pinilla-Roncancio & Cedeño-Ocampo, 2023), employability opportunities (Pinilla-Roncancio & Gallardo, 2023) and access to social innovation alternatives that facilitate an adaptable life (Bazán et al., 2023).
As a result, two problem questions are raised:
Q1: What are the intervention components, key players and social innovation models that contribute to the improvement of CBR services from a biopsychosocial approach, aimed at people with lower extremity amputation in a situation of disability?
Q2: How are CBR models structured to facilitate the removal of barriers in rehabilitation services and promote a better quality of life among people with disabilities?
Method
The systematic review method was implemented to collect information related to the topic of interest, through databases with high impact on the scientific literature; in addition to providing an analytical categorization to reach the research objectives (Aguilera Eguía, 2014). Thus, Figure 1 shows the four methodological phases.

Methodological phases of the systematic review.
Database Tracing and Search Equation
The Web of Science (WoS) and Scopus databases were selected, as they are interdisciplinary and allow the search to be broadened in areas compatible with the health area. The first compiles the references of the main scientific publications in various disciplines of knowledge, covering approximately 22,000 journals (Delgado Vázquez et al., 2019); the second compiles scientific literature linked to a wide variety of specialties, in addition to access to metrics and analysis tools (Elsevier Company, 2023). The process began with the preliminary exploration of keywords in the Unesco and ERIC thesauri, to later determine the terms and thematic axes that guided the construction of the search equations.
After exploring the possible combinations of the equation, the research team decided to define two equations, since the first one makes it possible to address CBR, people with lower limb amputation in contexts of armed conflict and social innovation as a model for improvement. The second refers to Non-Governmental Organizations (NGO) and supranational bodies that analyze and intervene on the subject of interest.
Equations 1 and 2 are presented in Table 1. Table 2 shows the inclusion and exclusion criteria defined to select documents related to the objectives and subject matter of the study. Regarding the selection of the period 2001 to 2019, a 10-year exploratory survey was initially provided between 2009 and 2019; however, the search was extended 8 years to identify studies published at the beginning of the millenium and find a larger number of documents, especially due to the small number of studies found in the exploratory phase.
Search Equations.

Inclusion and Exclusion Criteria.

The PRISMA guide (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) was taken as a reference, which facilitates the meticulous structuring of the review process and provides rigor in the search and filtering of documents (PRISMA, 2015), according to the results obtained by transcribing the search equation and the selection of publications based on the inclusion and exclusion criteria. In Figures 2 and 3 the PRISMA flow diagrams of each equation are presented, divided into four stages: the identification of the total number of articles collected by each database, followed by screening for the review of the abstract and the title of each publication. Then the documents were selected, based on their suitability to the subject of study; including relevant publications when read completely. As a result, 52 articles were included in equation 1 and 40 documents were selected in equation 2. In total, 67 publications were collected.

PRISMA flow diagram (equation 1). Moher et al. (2009).

PRISMA flow diagram (equation 2).
Table 3 records details of each of the selected papers, specifying the main objective, methodology, concept or main category of the research.
Records Details of Each of the Selected Papers.

Table 4 shows in detail the categories constructed for the systematic analysis of the selected documents. Each item was assigned one code per category (P1–P67), according to the eight categories assigned.
Categories Constructed for the Systematic Analysis of the Selected Documents.

Bibliometric Analysis
Once the results had been identified in the scientific databases, the information collected was analyzed with the Vantage Point software, a specialized program for mining text from platforms such as WoS and Scopus, to process large volumes of data structured information for the visualization of patterns and relationships between factors (Vantage Point, 2023). Thus, the scientific mapping shows the distribution of publications by year and country; in addition to the most influential authors and subject areas.
Categorization of Results
After the development of bibliometrics, the documents compiled from the two selected databases were analyzed with the Nvivo 12 software. The units of analysis were identified to proceed with the coding, which groups the information into categories that facilitate the comparison between elements (Maxwell, 2019). It should be noted that as the analysis of the documents progressed, emerging codes were defined for the appropriate categorization of determining information in the study; thus, biases were eliminated when coding the data obtained among the members of the research team (Gibbs, 2014).
Systematic Review
We proceeded to the structured compilation of the information collected and categorized, in order to analyze the conceptual and methodological trends of the study topic at a global level (Rocha et al., 2012), identifying future lines of work and the contributions to knowledge that determine the intervention components, key actors and models of social innovation that should be involved in rehabilitation, in order to improve the health care conditions of the population with disabilities.
Results
Bibliometric Analysis
Distribution of publications by year: Figure 4 shows the trends in the publication of documents on the subject of study. There is a growing trend in the number of publications during the last 3 years (2017–2019), reaching a maximum of 19 publications in 2017 and 2018; 18 documents in 2019 and one paper in January 2020. Likewise, there is a wide variability in the number of publications during the period 2011 to 2016.
Distribution of publications by country: regarding the geographical distribution of the publications obtained (Figure 5), the countries with the highest number of documents are identified in red: Japan, 34; Great Britain, 33; and the United States, 14. It follows that with respect to the subject of interest tracked in the two high-impact databases, the three countries mentioned are characterized by having prevalence in the analysis of studies on armed conflict and supranational entities involved in it. They are characterized by having a broad influence in the scientific literature, as well as participation in public health, disability, and humanitarian contexts.
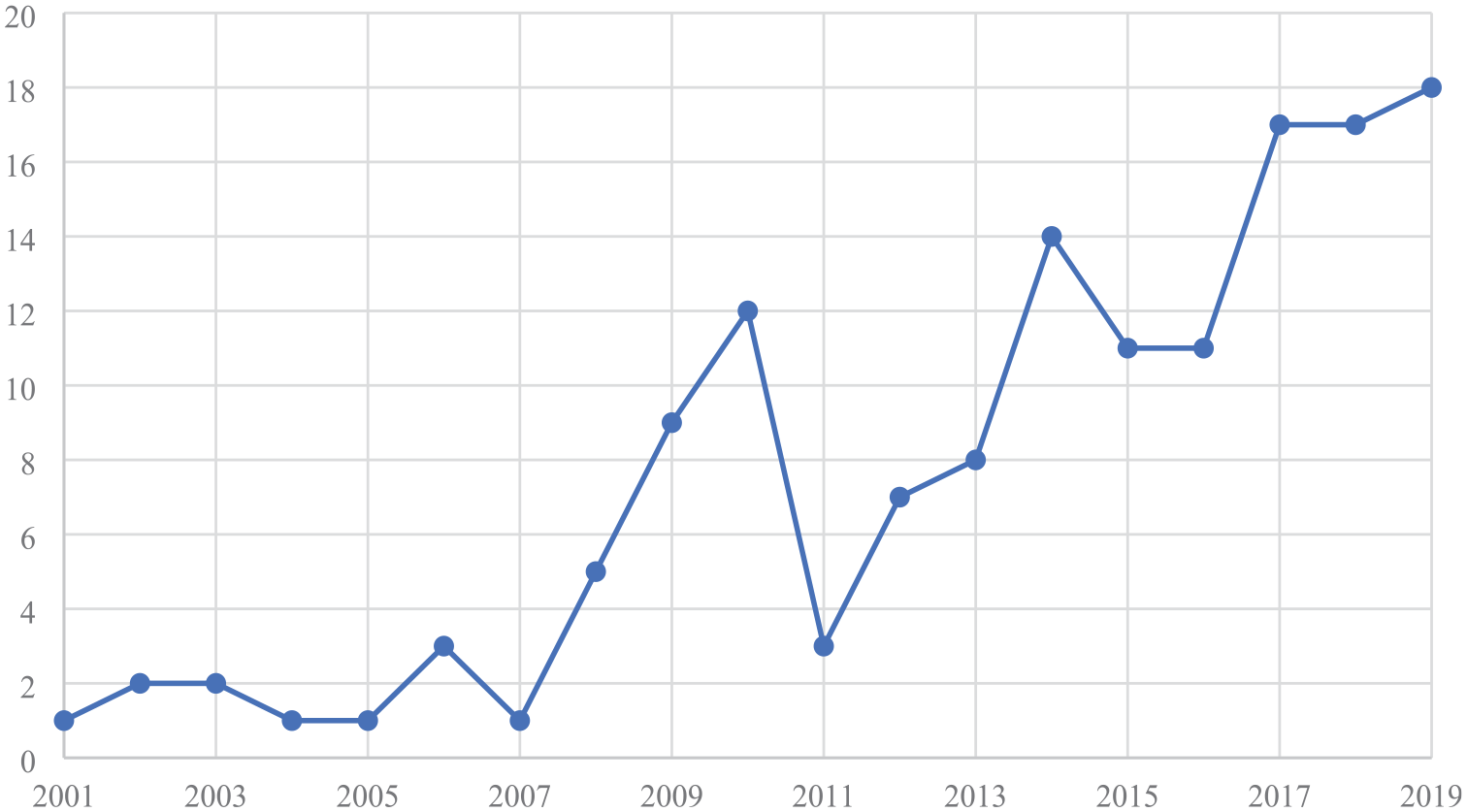
Distribution of publications per year.

Heat map—Distribution of publications by country.
On the other hand, Mexico, Colombia, Brazil and Chile are highlighted in light yellow, since they are in a range of 1 to 3 publications in the last 3 years.
3. Relationship of publications between authors: Figure 6 identifies intellectual production and its importance in terms of absolute frequency, highlighting the three main authors: Tolstrup has the highest absolute frequency of documents with a total of 17, followed by Granbeck with 6 and Becker with 4. In this way, the relationship between authors and their incidence in the scientific literature on the subject of interest is evidenced.
4. Cloud of most relevant words and their close relationship: Figure 7 shows the cloud of keywords contained in the selected documents. Knowledge transfer is highlighted as a cross-sectional term in the research topic, followed by social innovation, knowledge management, model, information, complex networks, management, evolution and dynamics. However, as it is a topic linked to the health area, some medical terms related to disability, its classification and rehabilitation function emerged.
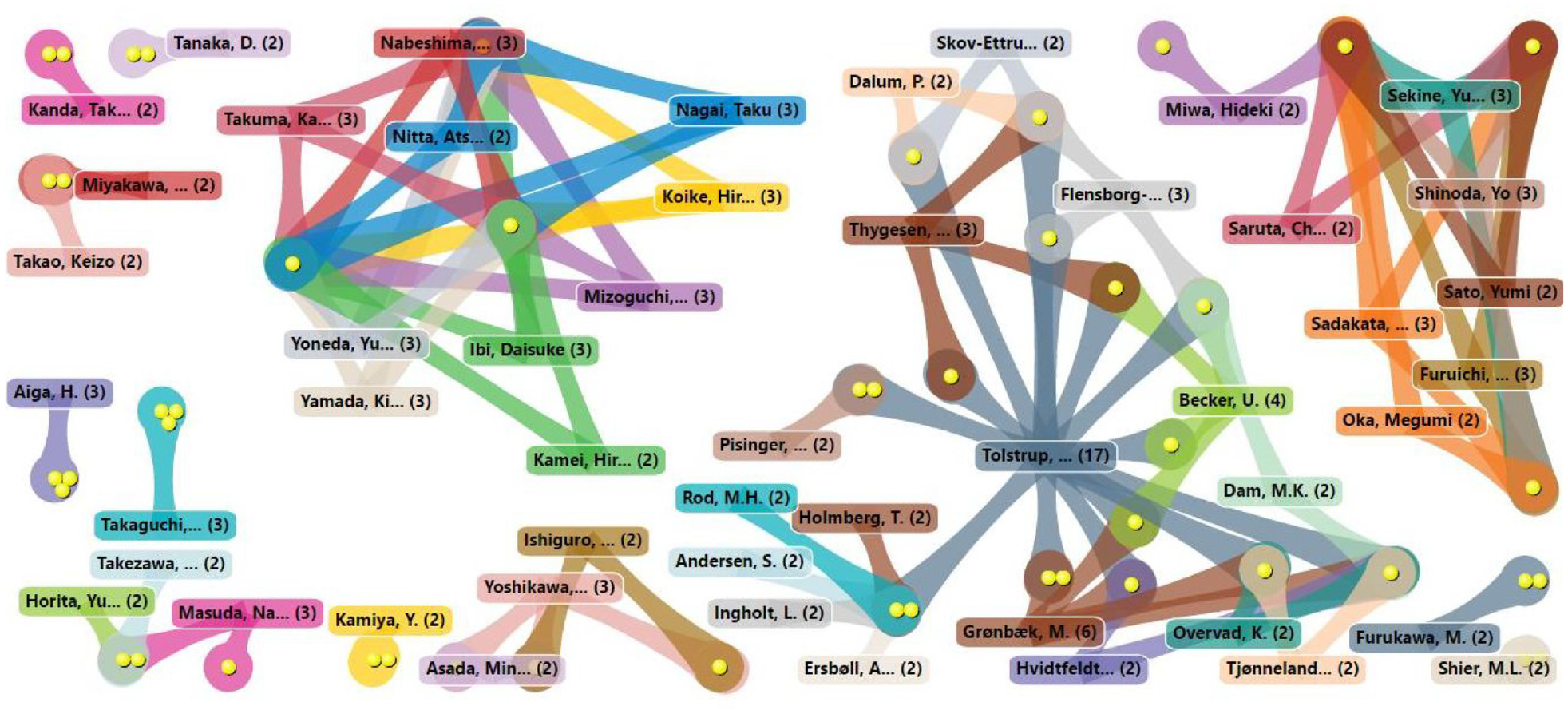
List of publications between authors.

Keyword cloud.
Content Analysis
Through the coding system developed with the NVivo software, the content of publications that refer to components of community health intervention for populations at risk or with a differential approach was adapted as a conceptual and methodological basis to analyze the topic of interest. This is the case for studies referring to maternity and early childhood, in which CBR is implemented and it works as a point of reference to ask questions in the scientific community, referring to the construction of improvement strategies for care with a biopsychosocial approach, aimed at people with disabilities due to lower extremity amputation in contexts of armed conflict. Thus, the contents found in the selected literature are divided into three aspects: intervention components, key actors and the influence of social innovation on community health.
Regarding the first element, it was found that the basis for optimizing community health intervention corresponds to the improvement of medical services, based on the creation of scientific knowledge distribution networks, with open operation for common access to procedural tools (Boyer, 2013). People with lower extremity amputations require that their rehabilitation process be guided by health guarantees, based on a principle of equity in service coverage (e.g., the Lives Saved Tool in Ghana) (Nakamura et al., 2011).
This also implies that the system provides the medical expenses of the population residing in the peripheries of countries with emerging economies (Sakisaka et al., 2010), providing health personnel with different incentives for moving to rural areas that require community intervention (Kawakatsu et al., 2014, 2015) and financing care centers in which services are provided following the CBR methodology (Matsuoka et al., 2014). The factors mentioned correspond to the challenges that the health system must face at the global level, especially in regions where basic needs still lack coverage (Kuhlmann et al., 2018).
Health services have different types of barriers in global peripheries, among which we find: (i) financial barriers due to poor investment, (ii) physical barriers in the geographical limits for access to health centers, (iii) cognitive barriers regarding the negative concept and misinformation of patients about the service, (iv) organizational barriers due to the way in which medical personnel addresses needs, (v) psychological and socio-cultural barriers due to the traditions of the community and the lack of credibility regarding professionals (Matsuoka et al., 2010).
In this sense, one of the most solid proposals relates to the planning and application of public policies in community health, by implementing rigorous management protocols (Nababan et al., 2017). The starting point for achieving this consists of a consolidation initiative, supporting the dissemination of scientific production in open access public health (De Castro et al., 2012). This requires articulating with research projects that include stakeholders (policymakers, professionals and affected communities) in the development of the design, analysis and dissemination of the process (McAneney et al., 2010). Likewise, one of the proposals of Meagher-Stewart et al. (2012) is to improve the competencies of health professionals to practice evidence-based decision-making in public health (EIDM), which could strengthen the capacity of the health system and improve outcomes.
In Kenya, the Third Strategic Plan of the Health Sector (2012–2017) was proposed, which aimed to improve the health system at the following levels: (i) community, (ii) primary care, (iii) departmental level and (iv) national level (Miseda et al., 2017). On the other hand, Duarte et al., 2011) proposed a binational health model for the Wayúu population on the Colombia-Venezuela border, which suggests eight components in health: intersectorality, integrality, interculturality, participation, information and research, sustainability, surveillance and control and health services. The two models are a benchmark for the implementation of CBR among people with disabilities due to lower extremity amputation, assessing the particularity of their needs and the socio-political and socio-cultural context that defines their life history.
According to Table 5, related to the key actors involved in the process, the three networks stand out for the participation of people and institutions that together can shape the expected changes in a community health system in which CBR is applied to people with disabilities. As mentioned, publications related to disability and armed conflict are limited (Lamichhane, 2015), especially those referring to people with disabilities due to victimizing events occurring in war contexts. Only nine papers refer to disability due to lower extremity amputation with different medical backgrounds and four papers refer to the armed conflict in Colombia, specifically in terms of psychosocial care for victims.
Key Actors According to the Network to Which They Belong.

One of the key players is the International Committee of the Red Cross (ICRC). The publications that mention it refer to the humanitarian personnel linked to this body, who are present in contexts of armed conflict in different scenarios. Dahlgren et al. (2009) analyze the perceived health consequences after a year of mission, along with the difficulty of the process and the stress it caused. Ballon (2016) describes his experience as a humanitarian worker, visiting people deprived of freedom in different prisons around the world; he described how a micro-society is configured in the context of the prison and how each individual positions himself in front of his community. du Mortier and Arpagaus (2005) exposed the ways in which medical personnel provide protection and assistance to victims of armed conflicts, through uninterrupted local health centers.
In addition to the primary network of a person with a disability due to lower extremity amputation, together with national and international entities involved in community health services, the global scientific community was found to be a key and indispensable actor. This is one of the most important findings, due to the scope of the systematic review methodology that was developed throughout the study and the results related to knowledge management.
Knowledge management is the mechanism for the transfer of information in the form of knowledge, in order to transform knowledge into the experience of organizations and individuals (Lora L & Rocha J, 2016). It focuses on analyzing and improving the bidirectional links between the production of scientific evidence and the construction of policies or practices (e.g., CBR; Contandriopoulos et al., 2017). This methodology maintains a close connection with social innovation, as it allows for the development of innovative knowledge for problem solving (Rentsch et al., 2010), with effective adaptability (Cummings et al., 2011), while applying creativity (Khirfan & Jaffer, 2014). Likewise, different knowledge is shared and valued through solutions and experiences by incorporating them as community practices (Hurtubise et al., 2016; Lora & Rocha, 2016; Nidhra et al., 2013). In addition, skills are acquired through collective learning and network integration (Nilsson, 2019).
The third element refers to social innovation, as a fundamental component in the construction and application of CBR in the population with disabilities. Salom-Carrasco et al. (2017) and Ludvig et al. (2018) report that in 2009, the United States created the Office of Social Innovation and Citizen Participation, to support innovative ideas with social objectives. Hence, it became a “service that meets certain needs of citizens or an original initiative that improves the effectiveness of public action” (Morales Gutiérrez, 2009, p. 152). In these cases, social innovation was implemented to introduce new solutions that provide alternatives for transforming social problems (Huq, 2019), based on the possible intervention of for-profit or non-profit organizations that mediate in the process (Le Ber & Branzei, 2010; Pandey et al., 2018).
Concurrently with social innovation, it is necessary to resort to Information and Communication Technologies (ICT) in the construction of social inclusion policies and the application of creativity as a basis for action (De Filippi et al., 2017; Rivera et al., 2010). Reyes et al. (2011) designed a device to improve the quality of daily activities of children with osteoporosis. Bernasconi et al. (2018) developed an Algorithm for the Management of Acute Childhood Diseases (ALMANACH) with a variety of tools, including a rapid diagnostic test and real-time data synchronization. From these examples, it is highlighted that health engineering makes it possible to resort to best practices, facilitating the interaction between agents, the process and the formulation of innovations (Chung et al., 2018).
According to the publications found, academics propose that innovation is a new way of solving local and global social problems, through the provision of services that contribute to equality and balanced development (Jelinčić et al., 2016; Széman & Tróbert, 2017). Hence the importance of building intersectoral partnerships between for-profit and non-profit organizations (Le Ber & Branzei, 2010), which allow the consolidation of initiatives such as CBR in health services for people with disabilities. Social innovation improves the effectiveness and adequacy of social policies (Kucsera & Misuraca, 2016) through a direct social impact for the expansion of services. It facilitates the integration of stakeholders and civil society (Széman & Tróbert, 2017), in addition to the possibility of being a transferable and reproducible model in the local and global environment (Morales Gutiérrez, 2009).
Discussion and Conclusions
Community health care is essential in settings permeated by the armed conflict. Therefore, it is necessary for the Colombian government to recognize the importance of building social welfare programs for people who became disabled as a result of the conflict, based on the application of CBR with training for independent living and the development of vocational skills (Lamichhane, 2015). Health care is a right that requires immediate application to alleviate the physical and psychosocial consequences of war (Coupland, 2013).
Therefore, it is essential to provide accompaniment in emotional recovery and in overcoming the damages caused by the conflict. This includes rehabilitation, physical reconstruction, compensation, emotional and psychosocial well-being (Rebolledo & Rondón, 2010). Within the framework of the Colombian armed conflict, reparation places victims in care routes for psychosocial accompaniment that enable the transformation of individual subjectivation (Estrada Mesa et al., 2010). CBR allows the person with a lower extremity amputation disability to have the support of their social network and companions in the process (Arévalo Naranjo, 2010); in addition to the biopsychosocial and legal mechanisms required to overcome the damages caused by the war (Quintero & Carvajal, 2009).
The social model allows us to understand that there are various barriers that lead to the exclusion and isolation of people with disabilities, preventing their full participation in society (Len, 2009). This model is an alternative to consider new ways of intervening in community health (Dhillon et al., 2010), taking as a guide the different debates that have been generated regarding disability policies (Burke & Barnes, 2018) and the importance of leading actions around a paradigm shift of society (Do, 2017). In this way, the medical rehabilitation of people with lower extremity amputation must be complemented with the biopsychosocial model, with the aim of successfully reintegrating into a daily life that resembles the style and quality of life prior to amputation (Kovač et al., 2015). In this regard, CBR may be the only strategy for providing health services to people with disabilities, little resources and difficulties in accessing health care.
Community participation in relation to public health policies is highlighted, since communities are usually involved only in the implementation process (Bachfischer et al., 2023), leaving aside their considerations in the design and planning phases. Likewise, national governments must facilitate the establishment of social networks based on trust; that is, they must provide innovation alternatives that are accepted and established (Kolleck & Bormann, 2014). Hence the importance of knowledge management and its role in the construction of models of social innovation in community health with communication components that involve all stakeholders (Lewin et al., 2011); for example, in the interaction between rehabilitation professionals, patients and specialist physicians (León-delgado & Flórez-rojas, 2010).
Additionally, to implement CBR in contexts of armed conflict and interaction with victims, it is essential to include the biopsychosocial model with interdisciplinary and ICT components which promote an independent life for people with disabilities (Roush & Sharby, 2011). It is also important to apply Universal Design in rehabilitation processes, with physical settings available to all individuals (Erkiliç, 2011) and educational programs in which the patient and their primary network receive training in their home and community setting, focused on the care and new lifestyle of the person with lower extremity amputation (Islam et al., 2015).
It has been shown that specialized rehabilitation programs are, for the most part, used by people of low socioeconomic levels and dependent on the public health system (García P & San Martín P, 2015). Within the framework of the socio-political and sociocultural context of this study, CBR is a basic tool for victims with disabilities due to lower extremity amputation in the context of the Colombian armed conflict to access a better quality of life and achieve independence.
On the other hand, decision-making coming from the international organizations involved in the fate of people with disabilities as a basis for global consensus (McCusker et al., 2023) must be permeated by the implementation of decisions related to formal employment for this population group (Haafkens et al., 2011; Mizunoya et al., 2016), as a basis to curve the aftermath of the war. Other aspects to be considered are the construction of memory as a collective process to know history and not repeat it (Kunt, 2017), along with the investment in Geographic Information Systems (GIS; Branch, 2014), as part of the interaction with the scientific community that builds the foundations for knowledge management. These aspects have been strengthened among the countries of the global south (known as south-south collaboration), whereby innovative, context-adjusted, and cost-effective solutions are shared to advance their economic, social, cultural, and environmental action plans (Were et al., 2019).
According to the results obtained, the action components, key actors and social innovation models that contribute to the improvement of CBR services are complementary elements in the intervention aimed at people with disabilities due to lower extremity amputation in contexts of armed conflict. This is because specific components of immediate application were found to improve the living conditions of this population group, in which different actors and basic solution alternatives focused on social innovation are involved in a cross-sectional manner.
In this sense, the scientific literature found global references with different experiences from countries that have applied CBR models, in addition to the opinions of academics regarding the scope of implementing CBR in community health services to promote a better quality of life among people with disabilities. Therefore, the finding of the scientific community as a key player in knowledge management is one of the components that best suited the analysis of the problem of interest.
The lack of studies that directly relate people with disabilities due to lower extremity amputation in contexts of armed conflict and health intervention implementing CBR shows the validity of the debate related to the urgent need to inform about the intervention methods used in the phases of research and application of social innovations with successful results, in order to open up more effective, replicable and applicable interventions in everyday life (Nielsen et al., 2018). This interpretative basis of the problem opens the way to the construction of new questions and ways of considering effective alternative solutions.
At the same time, the increasing number of publications on the subject indicates that academics worldwide are interested in analyzing the problems that are demarcated in that socio-political and socio-cultural context, with elements of community health in rehabilitation processes. Likewise, the small number of publications in Latin American countries stands out, which is directly related to the absence of studies related to the armed conflict and disability.
Limitations and Future Research
Regarding the limitations, it should be noted that the construction of two search equations could limit the number of records integrating the two components we intend to relate. However, searches of gray literature and the contents of some of the publications continue to demonstrate the lack of papers that directly link the categories: people with disabilities due to lower extremity amputation in contexts of armed conflict; and health intervention implementing CBR. Additionally, we expected to find a larger number of publications and analysis content referring to the key players in the secondary and tertiary networks, in order to strengthen their intervention in community health.
For future research, it is suggested to investigate in depth the role that the scientific community plays or could play in knowledge management, by integrating the following elements of analysis: people who acquired a disability due to the victimizing events in a context of armed conflict, health intervention implementing CBR, social innovation models and community health system in countries with emerging economies. In this way, the interpretative and proactive dimension of the problem analyzed is expanded, giving rise to a broader framework of replicable solution alternatives aimed at the population that has become disabled as a result of the armed conflict.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funded by Vicerrectoría de Investigación y Extensión, Universidad Industrial de Santander. Project: “A social innovation model for victims of anti-personnel landmines with lower limb amputations, integrating the Community Based Rehabilitation (CBR) strategy and the virtual technology-based service model for the development of prosthetic sockets.” Code number 8583. The APC was funded by the authors.
Informed Consent Statement
No applicable.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.