
Abstract
This article aims to critically analyse current literature that explores nurses’ perspectives concerning the use of chemical restraints amongst people with dementia—regarding behavioral and psychological symptoms of dementia (BPSD)—to consolidate existing knowledge on this phenomenon and generate a foundation for further research. This literature review followed the 12-step approach by Kable et al. A total of 17 articles published between 2012 and 2022 were included following critical appraisal. A total of 2,806 participants, primarily consisting of nurses of various levels (44%) were included amongst the 17 included articles. Five themes emerged from the analysis of the findings: (a) nurses’ perceptions of BPSD, (b) perceived effectiveness and safety of chemical restraints, (c) influence of the practice environment, (d) perceptions of non-pharmacological approaches (NPA)s, and (e) barriers to using NPAs. Explicit and implicit pressures to prescribe and utilize chemical restraints exerted by nurses and families promote the use of chemical restraints, amplified by barriers to using alternative approaches. A tentative conceptual model was proposed to explain these emergent concepts and relationships between the themes.
Plain language summary
Keywords
Background
Dementia is a condition hallmarked by a cognitive decline significant enough to impede independent daily functioning (Dementia Australia, 2017). The prevalence of dementia is increasing, especially in developed countries—due to longer life spans—and has been found globally in 7% of individuals above 65 years (8%–10% in developed countries) (Gale et al., 2018). There is an extensive list of causes for dementia, and the etiology in most cases is therefore difficult to pinpoint (Dementia Australia, 2017). The numerous types of dementia increase this difficulty and include Alzheimer’s disease, vascular dementia, Lewy body dementias, and frontotemporal dementia (Dementia Australia, 2017; Gale et al., 2018).
People with dementia commonly experience cognitive decline, find communication increasingly difficult, and exhibit behavioral changes. The term behavioral and psychological symptoms of dementia (BPSD) will be used in this literature review to describe these behaviors—as recommended by the Dementia Language Guidelines in a clinical context (Dementia Australia, 2018). These behaviors have been known colloquially as “challenging,”“difficult,” or “inappropriate behaviors,” although these terms are deemed inappropriate by the same guidelines (Dementia Australia, 2018). The significant contributors to these BPSD are changes in the person’s environment, health or medications, as well as the person’s reduced ability to understand explanations and express their needs, especially in people with frontotemporal dementia; creating behaviors that are often misinterpreted by healthcare professionals (Dementia Australia, 2015). These BPSD can be divided into four categories:
Physically aggressive behaviors, such as hitting and spitting;
Physically non-aggressive behaviors, such as wandering and inappropriate sexual behaviors;
Verbally aggressive behaviors, such as screaming and swearing;
Verbally non-aggressive behaviors, such as constant repetition of words or requests (Dementia Australia, 2015).
Healthcare providers and family members caring for a person with dementia who presents with these behaviors may find them challenging and turn to chemical restraints to manage a problematic situation (Peisah & Skladzien, 2014). Chemical restraints are a part of the broader term restrictive practices and refer to
a restraint that is, or that involves, the use of medication or a chemical substance for the purpose of influencing a person’s behavior, other than medication prescribed for the treatment of, or to enable treatment of, a diagnosed mental disorder, a physical illness or a physical condition. (Aged Care Act 1997 (Cth), s. 1)
Despite safety and ethical concerns, chemical restraints are commonly used as first-line management by healthcare professionals caring for people with dementia who exhibit BPSD. These medications remain highly prevalent in acute and long-term care facilities, with approximately half of people in residential care facilities and up to 80% of people with dementia being prescribed or administered these medications (Peisah & Skladzien, 2014).
Purpose of the Study
The purpose of this structured literature review was to explore nurses’ perspectives concerning the use of chemical restraints amongst people with dementia in acute or long-term care facilities. This literature review aimed to provide an understanding of existing knowledge on this phenomenon and critically appraise this knowledge to provide a foundation for future research.
Research Question
What are nurses’ perspectives concerning the use of chemical restraint amongst people with dementia in acute and long-term care facilities?
Method
The structured literature review followed the 12-step approach documented by Kable et al. (2012) and aimed to locate published studies. This approach involved (a) specifying the research question, (b) documenting the databases used, (c) specifying the limits applied to the search, (d) listing the inclusion and exclusion criteria, (e) listing the search terms used, (f) documenting the search process for each search engine, (g) accessing retrieved articles for relevance, (h) documenting a summary table of included articles, (i) providing a statement specifying the number of retrieved articles, (j) conducing quality appraisal of retrieved literature, (k) critically reviewing the literature, and (l) checking the reference list for accuracy (Kable et al., 2012). All steps are included in the following section, whilst not following the exact headings above.
Search Strategy
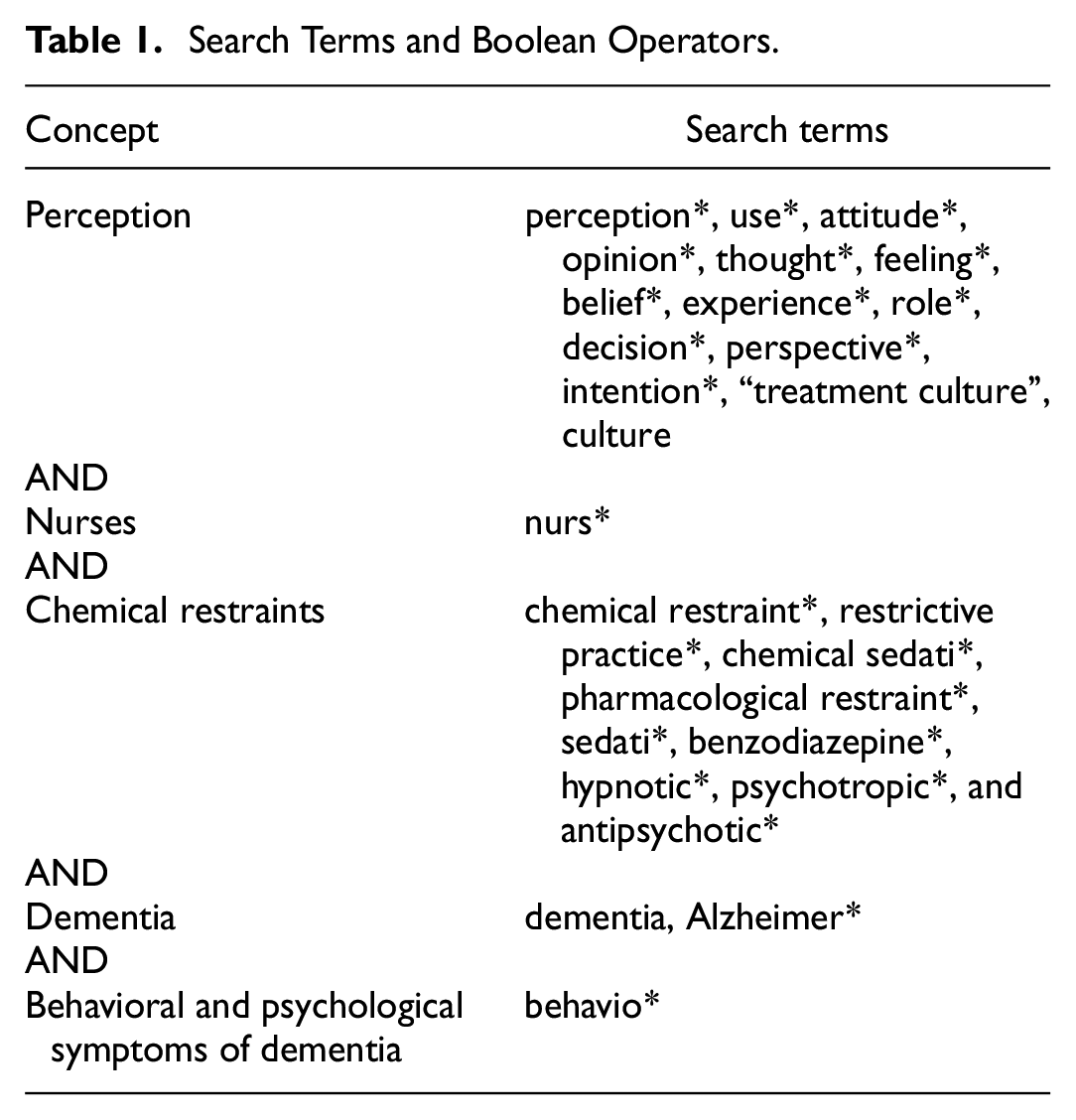
The search included all articles published in English and peer-reviewed studies from 01 January 2010 to 04 February 2023 to reflect the most contemporary literature in this area. The databases were searched sequentially using the search terms and Boolean operators (Table 1). The reference lists of all full-text articles retained for eligibility assessment were manually screened for additional relevant articles. All identified studies were collated and uploaded into Endnote (Clarivate Analytics, 2013), and duplicates were removed.
Search Terms and Boolean Operators.
Databases Searched
A comprehensive search of CINAHL, PubMed and Scopus databases was conducted in February 2023 to locate published peer-reviewed literature using the keywords identified.
Search Terms
Twenty-seven search terms were used to search the databases (Table 1), and the Boolean operators “AND” and “OR” were used to combine search terms. In addition, quotations were used to consider a phrase containing multiple words, and parentheses to control the order in which the string was read. Notably, the term “Alzheimer” was specially selected as a search term for the interchangeable nature between Alzheimer and dementia.
Inclusion Criteria and Exclusion Criteria
Table 2 should be located here
Inclusion and Exclusion Criteria for Literature Review.
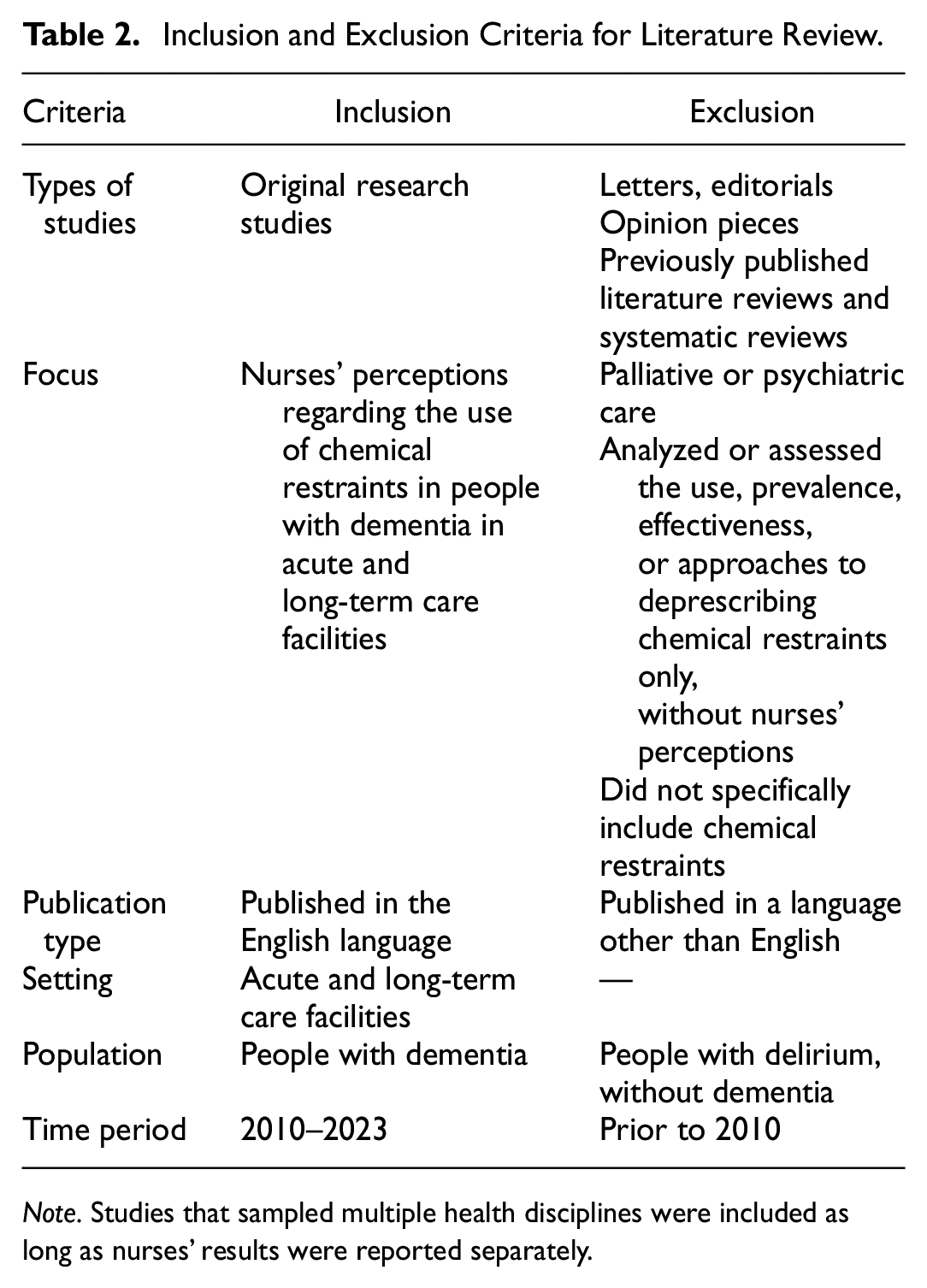
Note. Studies that sampled multiple health disciplines were included as long as nurses’ results were reported separately.
Search Results
One thousand thirty-seven articles were initially identified through the database search, and 650 remained after duplicates were removed. The title and abstracts were screened against the inclusion and exclusion criteria, and 625 did not meet the inclusion criteria or met the exclusion criteria. The remaining 25 articles were read in full, and 16 articles meeting the inclusion criteria were retained. One additional relevant article was retrieved from a manual search of the reference lists of included articles, totaling 17 articles selected for quality appraisal. All 17 articles critically appraised achieved a high standard and were included in the review. The quality appraisal process is detailed below.
The results of the search are presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart (Figure 1) (Moher et al., 2009).
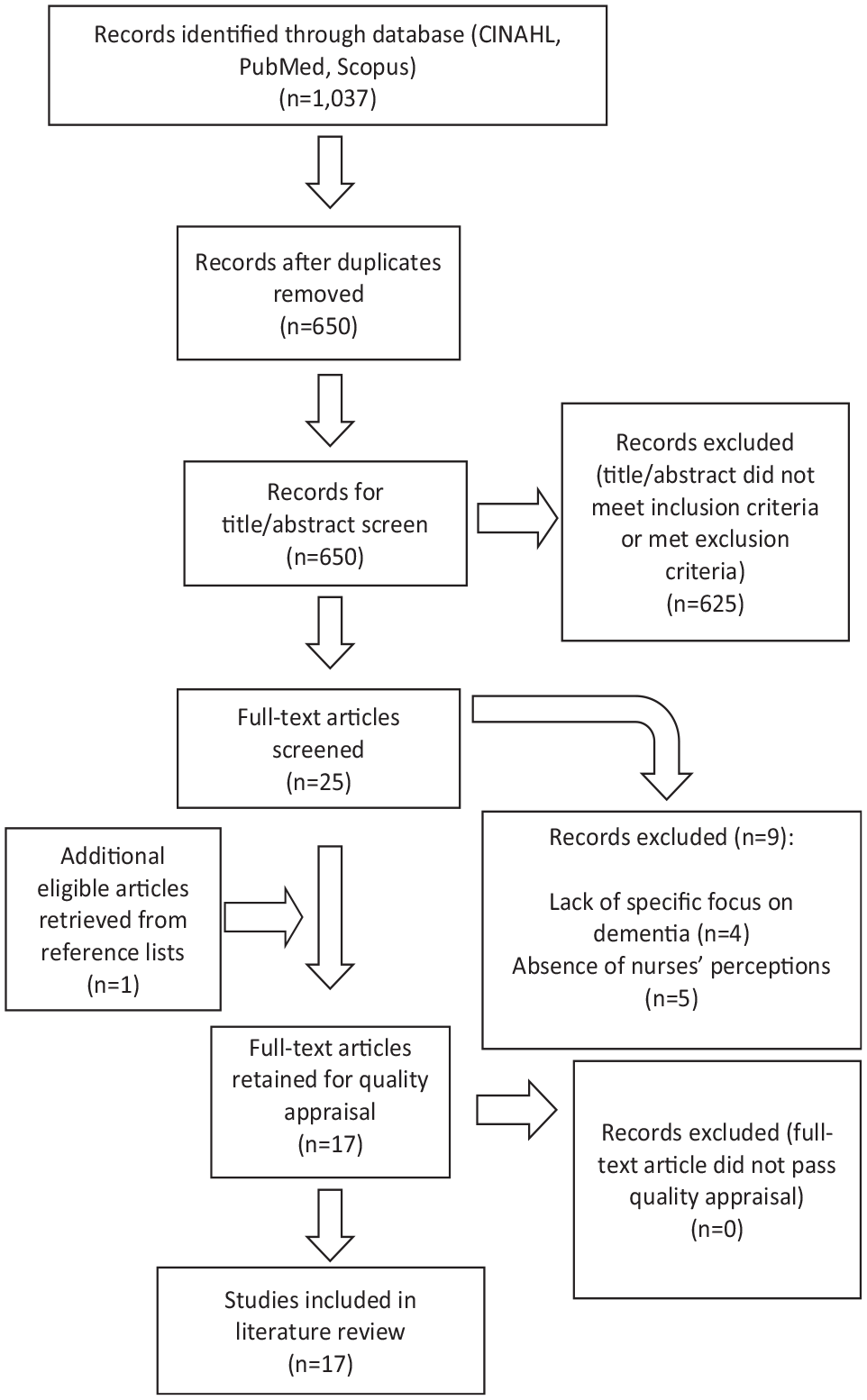
PRISMA flowchart of search process.
Quality Appraisal of the Studies
The 17 studies were appraised for quality using the Critical Appraisal Skills Programme (CASP) tool for qualitative research and the Mixed Methods Appraisal Tool (MMAT) for quantitative and mixed-method research design.
The CASP tool includes ten indicators, nine of which were scorable evaluated and scored as “yes” (1 point), “no” (0 points), or “can’t tell” (0 points). The studies were categorized into high quality (8 or more points), moderate quality (5–7 points), and low quality (4 or fewer points) based on the total score. Only studies of moderate or high quality were retained.
The MMAT included two screening questions/criteria for all study types, followed by five questions specific to the study type. These questions were scored as “yes” (1 point), “no” (0 points), or “can’t tell” (0 points). The studies were categorized into high quality (6 or more points), moderate quality (4–5 points), and low quality (3 or fewer points) based on the total score. Only studies of high or moderate quality were included in the review.
A total of 17 articles were included in the review following quality appraisal, and the following data were extracted for analysis: (a) characteristics of the paper; (b) research aim, study design and data collection; (c) sample size and sites; and (d) key findings. The data extraction and quality appraisal classification table is provided (Table 3).
Data Extracted from Included Articles and Quality Appraisal Classification.

Results
The final sample of 17 included articles were all published between 2012 and 2022. The geographical settings were: the United Kingdom (n = 1), England (n = 1), the United States of America (n = 6), Canada (n = 1), the Netherlands (n = 3), Australia (n = 4), and Ireland and New Zealand (n = 1). Study designs included mixed methods (n = 2), qualitative approaches (n = 10), and quantitative methodologies (n = 5). Data collection procedures comprised of; semi-structured and structured interviews (n = 7), surveys (n = 4), and questionnaires (n = 6). The 17 studies included 2,806 participants, which primarily consisted of nurses of various levels (44%). Members of the multidisciplinary team; including pharmacists, social workers, and medical doctors, accounted for 31%; and both nursing and medical managers/directors constituted 14%. The remaining 9% of participants comprised family members and caregivers, students, proxies, non-clinical administration, and an undefined “others” category.
Analysis of the findings reported in the 17 included studies generated five themes describing nurses’ perceptions of, and rationale for, using chemical restraints to manage BPSD in people with dementia: (a) perceptions of BPSD; (b) perceived effectiveness and safety of chemical restraints; (c) influence of the practice environment; (d) perceptions of non-pharmacological approaches (NPA)s; and (e) barriers to using NPAs.
Perceptions of BPSD
Nurses working in acute care and residential care settings indicated that BPSD made up the primary rationale for the use of chemical restraints. The cited behaviors were aggression, anger, agitation, sadness, crying, wandering, perseveration, inappropriate sexual behavior, fecal smearing, and spitting—encompassing the four categories of BPSD as aforementioned (Almutairi et al., 2018; Bonner et al., 2015; Cornegé-Blokland et al., 2012; Mallon et al., 2019; Simmons et al., 2018; Walsh et al., 2022; Watson & Hatcher, 2021). These behaviors were considered as risks to the welfare and safety of the people exhibiting them, as well as others and participants described chemical restraints as necessary to prevent perceived harm (Walsh et al., 2022; Watson & Hatcher, 2021). Nurses found these behaviors challenging to manage with only NPAs and tended to utilize chemical restraints—Lemay et al. (2013) stated that only 37% of care staff believed they could manage BPSD with NPAs alone. These behaviors led to a tendency for staff to resort to pharmacological approaches to aid in “settling” or “calming down” patients—as described by Walsh et al. (2022). Walsh et al. (2022) extend the indication for chemical restraint use beyond BPSD, and stated that nurses used PRNs to prevent these behaviors before they manifested; predicting that BPSD would be exhibited if chemical restraints were not used.
Alternatively, one article stated that participants viewed BPSD as resulting from an unmet need or a response to an unsuitable environment, yet, whilst RNs disagreed with the frequency of chemical restraint use for BPSD, ENs and personal care workers believed they should be used more frequently (Roe et al., 2020).
Perceived Effectiveness and Safety of Chemical Restraints
Seven of the 17 articles explicitly stated that the participants perceived chemical restraints as an effective intervention for BPSD (Almutairi et al., 2018; Cornegé-Blokland et al., 2012; Dys & Carder, 2022; Janus, van Manen, Ijzerman, et al., 2017; Janus, van Manen, van Til, et al., 2017; Kerns et al., 2018; Lemay et al., 2013).This perception of effectiveness was consolidated by perceptions that chemical sedation enabled nurses to manage high workloads and time constraints in the short term by reducing the need to attend to the person with dementia, along with the ease of requesting and administering medication (Almutairi et al., 2018; Lemay et al., 2013; Ludwin & Meeks, 2018; Simmons et al., 2018). Lemay et al. (2013) reported that 56% of nurse participants felt the medications used for BPSD were effective, with Cornegé-Blokland et al. (2012) reporting the nurse perceived probability of antipsychotic effectiveness for BPSD to be 53%. Nurses in other studies, however, while aware that medication had side-effects such as an increased risk of falls, reduced mobility and decreased quality of life, did not consider these to be severe (Kerns et al., 2018; Simmons et al., 2018; Watson & Hatcher, 2021). Several studies reported that nurses perceived medication effectiveness to be more evident than the side effects and, therefore, worth the risk (Almutairi et al., 2018; Janus, van Manen, van Til, et al., 2017; Kerns et al., 2018). Furthermore, two studies reported that nurses’ belief in the safety of chemical restraints related to the perception that small doses are safe and useful based on their subjective experiences of using these medications in practice (Almutairi et al., 2018; Kerns et al., 2018).
Influence of Practice Environment
Most nurses reported taking the initiative to consider medication prescription and request that the treating doctor prescribes a chemical restraint (Cornegé-Blokland et al., 2012; Ervin et al., 2012). For example, Janus, van Manen, Ijzerman, et al. (2017) found that 74% of nurses had requested the prescription of antipsychotic medication at least once over 3 months. In turn, in three studies that reported doctors’ perspectives alongside nurses,’ the medical staff described feeling pressured to prescribe antipsychotic medications (Almutairi et al., 2018; Cornegé-Blokland et al., 2012; Janus, van Manen, van Til, et al., 2017). Cornegé-Blokland et al. (2012) reported that this pressure existed in 17% of cases where BPSD occurred, illustrating nurses’ influence on prescribing. Furthermore, 43% of nurses surveyed by Janus, van Manen, Ijzerman, et al. (2017) believed their colleagues would request antipsychotic medication to manage BPSD. Lemay et al. (2013) described these pressures as the prescribing culture and identified the issue this creates as the normative use of chemical restraints. This is referred to by Lemay et al. (2013) as “local practices, attitudes, and beliefs among facility staff regarding antipsychotic medications and behavior management can exert a strong influence on clinical practice”Lemay et al. (2013, p. 896). Walsh et al. (2022) further described this culture; finding that nurses used language that reflected a nursing culture, where PRN decision-making was considered a collective decision rather than an individuals.
Perceptions of NPAs
Nurses’ attitudes to and expectations of outcomes from NPAs were favorable, most often due to the perceived absence of side effects, an overarching moral position regarding the “right” or “wrong” of medication versus NPAs and the role in maintaining the health and well-being of the person with dementia (Dys & Carder, 2022; Janus, van Manen, van Til, et al., 2017; Roe et al., 2020). Janus, van Manen, Ijzerman et al. (2017) pointed out that nurses utilized interventions, not for the intervention’s effectiveness but for the reduced risk to patients and residents. These reported NPAs included aromatherapy, multisensory stimulation, massage, music and dancing, distraction, and cognitive therapies (Almutairi et al., 2018; Cornegé-Blokland et al., 2012; Ervin et al., 2012; Janus, van Manen, van Til, et al., 2017; Kerns et al., 2018; Ludwin & Meeks, 2018; Mallon et al., 2019; Peisah & Skladzien, 2014; Watson & Hatcher, 2021).
Eight articles identified nurses’ preference for using NPAs to remove sources of BPSD before chemical restraints were utilized, which Janus, van Manen, Ijzerman, et al. (2017) determined was up to 71% of nurse participants (Cornegé-Blokland et al., 2012; Ervin et al., 2012; Hughes et al., 2012; Kerns et al., 2018; Ludwin & Meeks, 2018; Mallon et al., 2019; Watson & Hatcher, 2021). Similarly, four articles found that using NPAs was considered a primary initiative to manage BPSD, followed by medications when they failed (Cornegé-Blokland et al., 2012; Ervin et al., 2012; Hughes et al., 2012; Mallon et al., 2019). At the same time, Kerns et al. (2018) found that respondents preferred to implement pharmacological approaches and NPAs simultaneously. Furthermore, it was evident that such behaviors generated a high demand for personal care from nurses, making them feel overwhelmed and unable to cope when using NPAs alone, especially when caring for multiple people with dementia who present with BPSD simultaneously (Kerns et al., 2018).
Barriers to Using NPAs
A perceived lack of resources concerned both the skills, knowledge and equipment nurses required to implement NPAs; and the resources available for people with dementia and those living alongside them (Cornegé-Blokland et al., 2012; Dys & Carder, 2022; Janus, van Manen, van Til, et al., 2017; Kerns et al., 2018; Simmons et al., 2018). Kerns et al. (2018) found that dementia information resources given to people with dementia and their families and carers were overly general and impersonal and were provided predominantly in pamphlet form or a location of support groups—which were difficult to access due to the BPSD.
Nurses felt constrained in their use of NPAs by a lack of education. Lemay et al. (2013) found that only 37% of direct care staff believed they had appropriate training suited for managing BPSD. Also, three articles reported that nurses recognized this training gap and desired further, ongoing training, which was not being accommodated (Ervin et al., 2014; Mallon et al., 2019; Simmons et al., 2018). Two of the studies specified that future training should target both knowledge and beliefs concerning chemical restraints to provide a more realistic view of the benefits and risks (Janus, van Manen, Ijzerman, et al., 2017; Lemay et al., 2013).
The time required to implement NPAs was cited as the most significant limitation, and studies found the time burden to be on the planning, implementation and maintenance stages of these approaches (Cornegé-Blokland et al., 2012; Ervin et al., 2014; Ervin et al., 2012; Janus, van Manen, Ijzerman, et al., 2017; Janus, van Manen, van Til, et al., 2017; Mallon et al., 2019; Simmons et al., 2018; Walsh et al., 2022). Moreover, nurses identified the need for NPAs to be tailored to the individual by learning about their past experiences during conversing, expanding the need for vast amounts of time and education (Ervin et al., 2014). Nevertheless, nurses reported perceptions that even with optimal resources and time, NPAs did not always work, leading them to resort to medication administration (Dys & Carder, 2022; Kerns et al., 2018). Furthermore, Kerns et al. (2018) found that BPSD generated high demand from nurses, leading them to feel overwhelmed and unable to cope when using NPAs alone, especially when caring for multiple people with dementia who present with BPSD simultaneously.
Additionally, nursing staff did not perceive NPAs to be within their scope of practice or role and believed other professions should implement these (Ervin et al., 2012; Ervin et al., 2014). Ervin et al. (2014) expanded this statement, finding that nurses perceived their role as medically orientated, suggesting that alleviating other barriers would not be effective in increasing NPA use as they do not see it as within their scope.
Discussion
Focusing on nurses’ perceptions concerning the use of chemical restraints amongst people with dementia and the perceived barriers to NPAs, this discussion unveils the key insights from the reviewed literature and leads toward a tentative conceptual model to illustrate the prevalent decision-making tendencies. The included literature revealed that, despite the majority of nurses preferring to utilize NPAs as a first-line method, many turned to chemical restraints to manage BPSD (Cornegé-Blokland et al., 2012; Ervin et al., 2014; Hughes et al., 2012; Janus, van Manen, Ijzerman, et al., 2017; Janus, van Manen, van Til, et al., 2017; Ludwin & Meeks, 2018; Mallon et al., 2019; Roe et al., 2020; Watson & Hatcher, 2021). It was evident that this inclination toward chemical restraints was, in part, due to numerous barriers encountered to using NPAs, such as (a) insufficient resources; (b) lack of knowledge and education, (c) perceptions that NPAs lacked effectiveness; (d) time constraints; and (e) perceptions that these approaches are outside the nursing role (Cornegé-Blokland et al., 2012; Dys & Carder, 2022; Ervin et al., 2012; Janus, van Manen, van Til, et al., 2017; Kerns et al., 2018; Simmons et al., 2018; Walsh et al., 2022). Considering these barriers to using NPAs, nurses used the more expedient strategy of administering chemical restraints to manage current and predicted BPSD in a person with dementia and to prevent potential harm to them and others (Walsh et al., 2022; Watson & Hatcher, 2021).
Chemical restraints were additionally viewed as effective and safe by the majority of nurses, owing to the limited observable side-effects, furthering their appeal (Almutairi et al., 2018; Cornegé-Blokland et al., 2012; Dys & Carder, 2022; Janus, van Manen, Ijzerman, et al., 2017; Kerns et al., 2018; Lemay et al., 2013; Ludwin & Meeks, 2018). This literature suggests that these aspects, coupled with the abovementioned perceived barriers to using NPAs, tend to drive a chemical restraint focused practice environment.
Analysis and discussion of the included literature generated a tentative model that might explain nurses’ decision-making when managing BPSD (Figure 2). This model describes a process involving several steps and decision points that ensue when a nurse encounters BPSD in a person with dementia for whom they are caring.

Tentative conceptual model of chemical restraint predilection.
The initial step in the model is the nurse’s use of an NPA—evidenced to be the first-line choice—when a person with dementia first exhibits BPSD. If the person with dementia positively responds and the BPSD becomes less evident, the nurse considers the NPA effective, and the process is complete. However, if the nurse judges that the NPA is ineffective, they will move to the next step of employing medication. The sedative effect of such medication is likely to be successful in quelling the person’s activity, contributing to nurses’ perceptions of the effectiveness of pharmacological approaches and contributing to an overriding positive feedback loop that drives subsequent steps of the model. Ballard et al. (2009) and Peisah and Skladzien (2014) evidence that chemical restraint use in people with dementia leads to cognitive decline and increased BPSD. This evidence perpetuates the proposed loop, as it illustrates the need for additional chemical restraints–which were deemed effective due to the initial reduction in BPSD–due to increased BPSD because of a decline in cognition following initial chemical restraint use. The driving factors include (a) the influence of a chemical restraint driven treatment culture informed by staff members’ observation that chemical restraints are effective in the short term; (b) nurses’ experiences of barriers to using NPAs; and (c) nurses’ perceptions of the effectiveness and safety of medication used to manage BPSD (predilecting factors for the use of chemical restraints). It is proposed that these factors tend to consolidate nurses’ preferential shift toward choosing chemical restraints as a first-line intervention over NPAs to manage BPSD in people with dementia. This tentative conceptual model suggests that once the positive feedback loop of chemical restraint reliance initiates, difficulties in breaking the cycle and nurses’ reluctance to retry NPAs reinforces the use of chemical restraints.
Limitations
The search limits of English only articles may have introduced bias into the study, albeit this allows for primarily Western medicine to be analyzed, increasing generalizability in this culture. It is also notable that there may be response bias in the results from the respondents conveying perceptions that are espoused rather than actual, as raised by Hughes et al. (2012).
Conclusion
This literature review reveals that nurses working in acute care and residential care settings believed that BPSD made up the primary rationale for the use of chemical restraints, and, although pharmacological restraints were considered an effective intervention for BPSD, NPAs were still favorable in nurses due to the absence of side effects and an overarching moral position. However, the implementation of NPAs was limited mainly by the lack of training and resources available. Also, the prescription of and request for chemical restraints were influenced by the work practice environment. Based on the findings of this literature review, a tentative conceptual model explaining nurses’ decision making about the use of medication the manage BPSD has been developed. This model illustrates the explicit and implicit pressures to utilize chemical restraints exerted on nurses, which promotes their use and further shows how this is amplified by: (a) the barriers to using NPAs as an alternative; (b) a chemical restraint driven treatment culture; and (c) incorrect perceptions of the effectiveness and safety of chemical restraint use. Further research is recommended to validate the components of this tentative conceptual model prior to its integration into practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as not an animal nor human study.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.