
Abstract
Admiral Nurses (ANs), specialists in dementia, provide care management to families affected by dementia. A survey was designed to explore family carers’ views on the care received. A mixed-method survey questionnaire was distributed to all carers in receipt of AN services, or those recently discharged. This article presents the qualitative findings. Three overarching themes emerged from the data: “value of bio-medical, practical, psychosocial, and local expertise”; “transformative impact on carers”; and “availability/responsiveness.” Difficulties included navigating the system, unlocking resources and support, fragile service provision, understanding/coping with dementia, isolation, and guilt. Respondents highly rated the support provided by ANs, with outcomes affirmative for “positive experience of care and support” and “enhanced quality of life for carers” domains of National Health Service (NHS) Outcome Framework for England and Adult Social Care Outcomes Framework. While results suggest ANs successfully facilitated continuity of care, carers still felt exposed to potential cuts to services.
Introduction
Family carers of people with dementia in the United Kingdom play a pivotal role in the national provision of dementia care and support: their contribution has been estimated to absorb just under 50% of the overall cost to society (Prince et al., 2014) and to meet two thirds (£17.4 billion) of the direct cost of care provision through unpaid care (£11.6 billion) or self-funding of social care (Alzheimer’s Society, 2014). Carers are also likely to leave work or retire earlier to provide care, with costs to the economy in terms of loss of skills and experience which are predicted to rise from the current £628 million to £1.16 billion by 2030 (estimates made in the review for the House of Commons by Parkin & Baker, 2015).
Looking after someone can have negative consequences for family carers’ health and well-being (La Fontaine, Read, Brooker, Evans, & Jutlla, 2016), with increased risk of depression, anxiety, burnout (Parker, Arksey, & Harden, 2010; Schulz & Martire, 2004), premature mortality, coronary heart disease, and stroke (Haley, Roth, Howard, & Stafford, 2010; Lee, Colditz, Berkman, & Kawachi, 2003). Carers of people with dementia, moreover, can experience worse health outcomes compared with other caring groups, with increased risk of developing dementia themselves and increased risk of death following hospitalization (Tremont, 2011). Increasing evidence suggests that tailored psychosocial interventions are effective at reducing carer burden (Beinart, Weinman, Wade, & Brady, 2012) and points to the importance of the protective function of factors such as self-efficacy (Beinart et al., 2012; Gallagher et al., 2011a, 2011b). Timely and relevant support and services is therefore important to carers; however, the experience is often reported as difficult (Newbronner, Chamberlain, Borthwick, Baxter, & Glendinning, 2013).
This study was designed to explore how family carers found the support provided by Admiral Nurses. Admiral Nurses are specialist dementia nurses who provide holistic and person-centered support to families living with dementia, through a range of psychosocial interventions, practical support, and education (Bunn et al., 2012). The model was originally developed as a response to the lived caring experience of a London family who went on to found a national charity, Dementia UK. Dementia UK works in partnership with National Health Service (NHS), Social Care Services, third-sector organizations, and residential settings who act as hosts to Admiral Nurse posts. Dementia UK provides a structure for continuous professional and practice development of the nurses. Admiral Nurses tailor their interventions to individual clients’ circumstances. Diverging from a common patient-centric approach, family carers are also direct clients of Admiral Nurse services.
Direct support to families is provided in the form of one-to-one support; group-based interventions, such as Carers’ Support Groups (Brake, Graham, Marshallsay, & Springthorpe, 2007) or Carers’ Information Programmes (Sarna & Thompson, 2008), can also be delivered to respond to the varying needs of the localities in which the services are based.
Admiral Nurses also promote best practice in dementia care by providing education, training, advice, and guidance to other staff working with people with dementia and their families (Thompson & Devenny, 2007).
Method
Study Design
To sample the views of family carers in receipt of Admiral Nursing support, a mixed-method survey questionnaire was designed. A survey approach was taken to capture a wide range of experiences allowing us to reach all carers currently in receipt of support from, or very recently discharged by, three different Admiral Nursing services (two urban and one urban/rural setting, in the north east, east, and south of England). The two urban services were well established, while the third one—covering an urban/rural area—had only operated for a year but had already been put on notice of closure (due to lack of funding) by the time that the survey reached the carers.
The Questionnaire Tool
The questionnaire was developed around the Admiral Nurse Standards, building upon a previous external evaluation (Clare et al., 2005). The tool adopted a mixed-method approach, eliciting feedback using both a 5-point Likert-type scale and free text comments for each section of the questionnaire (see the appendix). Basic demographic information was also invited at the end of the questionnaire, including relationship with the person cared for. The survey was run between 2012 and 2013. More information on the development of the tool can be found in the paper presenting the survey’s quantitative findings (Maio, Botsford, & Iliffe, 2016). This article will present the results of the analysis of the qualitative data only.
As the questionnaire’s aim was service evaluation, formal ethics committee approval was not required; however, the local research and development departments of each of the three sites were notified of the intention to conduct the survey prior to any contact with family carers.
Participation in the survey was voluntary. The information sheet given to prospective participants clearly stated that the care they were receiving would have not be affected by their decision to take part or not, and that all data would be anonymized.
Sample
The sample comprised all family carers currently in contact with the service, including those awaiting first assessment, as well as those who had been discharged in the 3 months prior to the sampling date. Non-availability of the address, or refusal to be contacted (a single case), was the only exclusion criteria (Maio et al., 2016).
Analysis
The qualitative data were transcribed from the free text boxes of the questionnaire tools into an Excel™ database, coded, and analyzed using thematic analysis (Strauss & Corbin, 1990). Themes were independently generated by three researchers and discussed until consensus was reached. To minimize confirmation bias, quotes were read and re-read and themes were grounded in the data, generating them bottom-up. Relevant literature on families’ experiences of specialist nursing was sought post-analysis, and results were compared.
Results
In total, 685 questionnaires were posted; 223 were returned (32.6% return rate), 207 of which contained sufficient data for the analysis (30.2% response rate) (Maio et al., 2016); this reflected the choice of a postal survey and was in line with the response rate attained by a large postal survey run around the same period of time at national level (34.3%; Ipsos MORI, 2014).
Family carers responding to the survey were predominantly female (n = 147, 75%), mostly wives (n = 76, 38.4%) or daughters (n = 52, 26.3%), and the majority living with the person they were caring for (n = 137, 68.8%) (Maio et al., 2016). The largest group was above the age of 65 (n = 129, 64.9%), and generally above the age of 35 (n = 197, 99%); they were mostly White British (n = 184, 92.9%; Census average = 93.8%, Office for National Statistics, 2013), consistent with the relevant regional data for the 65 and above age group from the Census 2011 (Maio et al., 2016). The modal period of caring was 2 to 3 years (n = 85, 44.4%; M = 4.3 years, range = 1-26 years). The data within the three individual settings showed a consistent trend, regardless of the regional location, rural or urban settings, and length of operation of the service (Maio et al., 2016).
Eighty-four percent of the respondents provided free text comments, the length of which varied from very brief notes to more expansive accounts of their experience of the Admiral Nursing Service and of caring.
We defined three overarching themes in relation to how carers described their experiences:
Value of bio-medical, practical, psychosocial, and local expertise
Transformative impact on carers
Availability/responsiveness
Quotations are used to illustrate thematic points; where available, relationship to the person with dementia is provided with each quote. Themes had broadly a similar level of support in the quotes, with carers commenting slightly more often on the impact on their own coping skills and resilience.
Value of Bio-Medical, Practical, Psychosocial, and Local Expertise
Family carers responding to the questionnaire described the Admiral Nurses as extremely competent and knowledgeable, placing a high value on their expertise. Carers described this as multi-faceted, covering at the same time the following:
Bio-medical knowledge of the condition
This was mainly discussed in terms of knowledge of dementia, helping carers understand symptoms and its impact on the behavior and capabilities of the person they cared for, alongside enabling them to consider potential future developments.
Made me more understanding of the disease and a better carer to mum. (Site 1, Daughter) She helped myself and my brother to understand better why mum had become “difficult” and hard to reach. She made us approach situations with mum in different ways to minimise her distress. She has helped us make choices re medication and referred us to committed specialists in social work team who are trying to engage mum in more activities and make her life easier, e.g. Meals on Wheels. (Site 3, Daughter)
Medication discussions appeared to have been held only in some cases, perhaps because, as some reported, these conversations had already happened with other specialists (e.g., the psychiatrist). However, if needed, Admiral Nurses were reported as able to address the issue confidently, helping the carer to understand medications better.
[The Admiral Nurse] told me about contact groups, how to cope with mood swings for me as a carer and my mum (Alzheimer’s), what side effects medication caused and explained in a way without big words I could understand. (Site 3, Daughter)
Psychosocial expertise
Help in addressing their emotional needs was an element that was very widely discussed in the responses. Family carers talked of how they felt Admiral Nurses had a deep understanding of the caring role and of what it entails, and how the nurse had helped them to identify and address their own emotional needs.
Have found some situations that I have had to endure and overcome as a result of my wife’s dementia, frightening, depressing for me and although numerous people give advice and offer to help, few have knowledge or expertise that can be trusted and it finishes up by “try this or try that.” On my contact with an Admiral Nurse for the first time I felt a relief that I had found someone to give me back my confidence to care for my wife. (Site 2, Husband) [The Admiral Nurse] made us aware that it wasn’t only mum we had to worry about, it was also dad and us as well, and that if it came that mum was to go into respite, it would be OK for all of us to have a rest too, and we shouldn’t feel guilty, we also had our lives to lead as well. (Site 3, Daughter-in-law)
This second quote also highlights a common subtheme: a sense of guilt that carers reported feeling when taking time for attending to their own needs, or more generally for a sense of “not being good enough” at their caring role.
Respondents, who wrote about the sense of guilt, gave positive feedback to Admiral Nurses’ interventions, which they found helpful in overcoming it. Mostly, this was achieved by helping them to acknowledge their own needs as carers or by validating what they were doing well.
My Admiral Nurse has helped me realise how much I have put in place and have been doing—as I felt guilty I wasn’t doing enough. (Site 3, Daughter)
Carers also put often in relation the support received, particularly to come out of crisis, with the feeling of being better equipped to manage care.
[The Admiral Nurse] understands the illness in much better detail than myself so explanations to situations were answered and understood better and strategies put in place to overcome difficult situation. (Site 2, Daughter) Since moving down to live with [my father] my “Life” has become more isolated, not only due to being in a town I have no connection with but to be a full time Carer has placed all kinds of demands upon me both emotionally and physically as well as obviously financially. . . My mental health started to deteriorate as did my isolation and the commitment required to make his needs and health met have significantly compromised my own . . . It was my first meeting with [the Admiral Nurse] which enabled me to speak out loud about the problems I was having for the first time. (Site 3, Daughter)
Expertise in relation to practical skills and issues
Respondents also valued the advice given in relation to practical support with their caring role. This could range from suggestions on how to improve daily living tasks: I was given written information concerning speech and feeding problems, also advice on how to cope with incontinence. (Site 1, Wife)
Or on supporting the well-being of the person cared for drawing on their life story: When she realized he used to play table tennis suggested he should meet another patient who played at the [local carers] café—which we did. (Site 1, Wife 2)
To support around responding to behavioral issues: How to react to mood swings and understand them. When my husband gets frustrated and confused. (Site 3, Wife)
Local expertise
A common remark was that “the system” appeared very difficult to navigate: If help and support was available, carers found it hard to locate and/or to gain access to it.
Carers felt relieved that Admiral Nurses facilitated the navigation process; in some cases, this was limited to providing the right kind of information and directing to the appropriate service, while in others, Admiral Nurses appeared to act as advocates or even directly co-ordinate care.
Provided information that was otherwise not provided –made me realise that there is some help available. (Site 1, Daughter) The nurse soon got us help from the Social Services, worked hard for us. (Site 3, Wife) Show all the support that is available and then coordinated that so that we had calls from various agencies. (Site 1, Relation to the person with dementia not declared)
These facets of Admiral Nursing expertise were not deployed in isolation: Carers placed high value on their use in combination with each other as this responded flexibly to a number of their needs.
Our Admiral nurse is an adviser, teacher and counsellor all rolled into one. As a family looking after a dementia sufferer, we have good days and bad, and our admiral nurse just gives us the confidence and reassurance to cope and carry on doing what we do. (Site 3, Daughter)
It also contributed to develop a deep sense of trust in the advice received.
Feeling safe to accept the advice of a trained person I could trust. (Site 2, Husband)
Transformative Impact on Carers
There were many comments relating to the differences that respondents perceived the Admiral Nurses had made to them. These could be broadly grouped in three categories.
Carer resilience and coping
A large proportion of the respondents described difficult experiences of caring: anxiety, feeling at loss and isolated, not knowing how to deal with changes in the person they cared for, or not knowing how to deal with the complexities of the system. By accessing the support of the Admiral Nurse, family carers responding to the survey reported being enabled to address a number of the issues, reducing their stress and anxiety and increasing their resilience.
I feel that without the open dialogue and support from [the Admiral Nurse] I would have had a break down as I was feeling isolated, and was overloading my brain with information on dementia/Alzheimer’s. Thank you for your help. (Site 3, Daughter) I don’t know how I would have managed without my Admiral Nurse. I was at the end of my tether, physically and emotionally exhausted and increasingly concerned about my husband’s confusion, aggressive behaviour, and social isolation. My Admiral Nurse also had a wealth of useful information e.g. local support groups and services, and knowledge of social security benefits and legal procedures. (Site 2, Wife)
Empowerment
Through their interactions with the Admiral Nurse, respondents reported feeling empowered with a better understanding of dementia, its effects on the person being cared for, and its potential future developments. This made them feel better able to care and cope.
The Admiral Nurse helped me increase my skills as a Carer, by explaining what can happen (not necessary to my husband) to a person with dementia, what can be done. Making sure I got help, I needed. This was so important as I felt I was letting my husband down, because I was beginning not to cope with his dementia. (Site 2, Wife)
This was partly due to feeling better able to deal with caring at present, and also to be able to start planning for the future.
Making sure I am aware of the expectations the future will hold and how to deal with them to my best ability as they arise. (Site 1, Husband)
Carers also reported feeling better able to put their requests forward to other professionals and services.
. . . often helped me to express myself to others in the family and doctors, social services etc. (Site 3, Daughter)
Feeling valued
As discussed under the “Psychosocial Expertise” section, several respondents reported that their caring role brought them to feel isolated, guilty when attending to their own needs, or generally experience a loss of agency.
Their interaction with the Admiral Nurse was described as counteracting these feelings, bringing a sense of value to the carer.
Honestly, without judgement. She made me feel human. (Site 2, Daughter)
This was partly a consequence of feeling listened to, understood, and validated: I could talk about my problems at ease like my stress levels and what I do as a carer and my life style in general, it was nice to be listened too, my Admiral Nurse respected all of this and understood. (Site 3, Niece)
And partly the result of a new appreciation of the value of their role, and the need to support their own needs, whether personal health and well-being or social and emotional.
Made me feel I was entitled to a life too and did not have to feel guilty when I felt I wasn’t coping. (Site 2, Wife) Made me feel I should look after my own health as well. (Site 3, Daughter)
Availability and Responsiveness
Knowing that they would be able to access the Admiral Nurses’ support, in case of need, was an element frequently mentioned in the responses, and seemed to foster a sense of reassurance.
The comfort that there is someone available with great insight and experience of our situation on which we can rely and seek advice. (Site 1, Relationship to the person with dementia not declared) Knowing there is someone there for me—excellent safety net!! (Site 2, Daughter)
Carers highly valued the responsiveness and availability of the Admiral Nurses that helped them manage the arising needs; indeed, the sense of reassurance was so profound that when access was limited, for example, in case of a prolonged sickness leave, respondents reported a feeling of loss.
Somebody to stand in as sickness cover so we do not feel everything has stopped. There is a lot of questions to be answered, support to be offered, advice to be given in how to and what help there is to assist carer. (Site 3, Husband)
This was more acute for one group of respondents. As mentioned in the “Method” section, the service covering the rural/urban area was a 1-year pilot. At the time of receiving the questionnaire, the family carers had just been notified of its imminent withdrawal for lack of funding. The reactions to the news in the comments were mostly of distress, acute pain, and frustration that a service they had valued was going to disappear; carers felt let down and they described a fear in their ability to cope with future changes in the people they cared for.
. . . Now that the service has been withdrawn, and with no gradual preparation owning the withdrawal of funding, I had no time to get used to the idea and am now coping with bereavement on these two levels, my mother’s death and the loss of my Admiral Nurse. (Site 2, Daughter) . . . I feel the rug has been pulled from underneath my feet. (Site 2, Daughter 2)
Some did not see the remaining services as sufficient support.
. . . I can obtain medical advice from our doctor and medical centre and they are wonderful—but finding someone who deals with dementia and all its “nightmarish” conditions was impossible until I was contacted by an Admiral Nurse. (Site 2, Husband)
Indeed, carers generally felt so exposed to the risk of losing the service that the fear this might happen was expressed even in comments made by carers from another area, where there were no indications of a potential service closure.
Very pleased with the help and support from Admiral Nurses; just make sure it is not taken away. (Site 3, Son) Do not withdraw this service—Admiral Nurses are vital to carers. (Site 3, Daughter)
Discussion
This questionnaire was the first multi-site survey of family carers of people with dementia supported by Admiral Nurses since the one undertaken by Clare, Willis, Jones, Townsend and Ventris in 2005, when the service provision in the community was 54% lower (35 nurses in 2005; 77 nurses in July 2013). Clare et al. reported a highly positive evaluation of the service and the support accessed: Carers praised the Admiral Nurses and described them as a knowledgeable and invaluable source of support, advice, and information, putting this in context with otherwise difficult experiences of caring, a sense of guilt, and difficulties in accessing support from the system. There is a marked consistency in the qualitative findings between the two surveys, in particular in the value carers placed on having access to knowledgeable and skilful clinicians, on the Admiral Nurses’ ability to create a therapeutic rapport and on their availability and responsiveness in times of need. In both surveys, carers also self-reported an increase in their ability to care as a result of the Admiral Nurse intervention. This suggests continuity and consistency in the quality of the service as it is experienced by family carers.
The consistency in the comments is also evident with regard to some of the general difficulties the carers describe. Some of the challenges mentioned related to their role (e.g., understanding and coping with the condition, a sense of isolation and guilt, etc.) and are in line with the findings in literature: feelings of guilt, for example, have been frequently observed in the caregiving literature (Gonyea, Paris, & de Saxe Zerden, 2008; Yaffe, 1988). They are associated with negative outcomes for carers’ mental health, and scales such as the Zarit Burden Interview (Zarit, Reever, & Bach-Peterson, 1980) analyze guilt as a factor influencing carers’ burden (Losada, Marquez-Gonzalez, Penacoba, & Romero-Moreno, 2010). Other challenges related to more structural barriers that seem to persist: a system perceived as difficult to navigate and challenges in unlocking resources and support. Evidence in the carer literature concurs with our findings, both in regard to delays in accessing information (Newbronner et al., 2013) and the perception of the system as lacking transparency, responsiveness, and ability to meet the needs of carers (Rand & Malley, 2014). Respondents also fed back a persisting issue with a care structure that appears not particularly able to absorb sudden staff loss (e.g., due to prolonged sickness leave) without causing a temporary loss of service.
Challenges were discussed in the responses as a way to illustrate the positive effects of the interactions with Admiral Nurses and articulate how the Nurses had helped them to address most of them. The examples provided, presented in the section above under the three overarching themes of “value of bio-medical, practical, psychosocial, and local expertise,” “transformative impact on carers,” and “availability/responsiveness,” show that Admiral Nurses brought about positive outcomes against two broad domains of the NHS Outcome Framework (NHSOF) for England and the Adult Social Care Outcomes Framework (ASCOF), 1 namely, the ones around “positive experience of care and support” 2 and “enhanced quality of life for carers.” 3
The attributes that respondents appear to appreciate the most in Admiral Nurses are consistent with findings of the systematic review of Bunn et al. (2012) around what people living with dementia and their family carers perceive as helpful support services (i.e., continuity of care/flexibility, information about aids and entitlements, ongoing opportunities to talk to supportive professionals, specialist support, signposting to appropriate statutory and voluntary services, individually tailored information, and peer support; Bunn et al., 2012, as elaborated on in the later report Bunn, Pinkney, Drennan, & Goodman, 2013), and also resonate with findings of external evaluations of other nursing specialties, like the British Heart Foundation palliative care nurses (Rogers, 2011) and the multiple sclerosis specialist nurses (Mynors, Suppiah, & Bowen, 2015). Both organizations interviewed or surveyed clients of their nurses and, as here, respondents highly valued the specialist knowledge and experience of the nurses (which they perceived could not be offered by other health care professionals), their availability and responsiveness to arising needs, alongside their ability to create rapport. In both these reports, as well as in these findings, respondents linked these qualities to a self-reported increase in quality of life. In psychoanalytical terms, the specialist nurses in these three studies appear, therefore, to put in place the therapeutic function of containing, which allows clients to address difficult emotions and situations. 4
Our data also suggest that Admiral Nurses implement or facilitate continuity of care in the three aspects defined by Freeman’s conceptual framework and refined by the linked study commissioned by the Canadian Health Services Research Foundation (see Freeman et al., 2007, for both studies). 5 Positive associations were found in the Freeman study between continuity of care and satisfaction for users, carers, and professionals (Freeman et al., 2007); the Canadian study also found that continuity of care was associated, within the management of mental health, to an improvement in health outcomes after 1 year (Adair et al., 2004) and a decrease in hospital costs, with an increase of community costs (Adair et al., 2005). This function, however, is exposed to the fragility of the current commissioning climate where health care services are constantly facing financial challenges. In spite of the positive outcomes reported, which are compliant with the national guidelines, the Admiral Nursing provision still remains vulnerable to the uncertainties of the commissioning of services for families affected by dementia. Recent National Institute for Health and Care Excellence (NICE; 2018) guidance recommends for further research on the effectiveness and cost effectiveness of what they describe as “high-intensity case management” for the person living with dementia and their carers, which describes Admiral Nurses’ family-centered, holistic approach may potentially influence this in the future.
Our data show that family carers experience pain and distress when a service is suddenly lost, with some describing it in terms of a bereavement, breach of trust, and neglect; the sense of instability, as we have seen, is such that experienced even in areas where no service closure is actually planned. The Sustainability and Transformation Plans (STP) 6 launched in 2016 in the United Kingdom have already elicited anxieties over potential new cuts to services (Edwards, 2016). One encouraging signal is family carers being explicitly mentioned in the six principles for engaging local communities and their knowledge in the drawing of STPs released by the People and Communities Board, with support from National Voices (People and Communities Board National Voices, 2016). However, tensions around the approach are still quite visible. In fact, a very recent report for The Health Foundation has highlighted how 2016/2017 has seen a de facto fall in per person spending in health care in England, with funds from the STP containing the deficit but being over-proportionally allocated to emergency services, and an increase in the number of commissioners in deficit, in spite of an overall improvement in the financial position of the NHS (Kraindler, Firth, & Charlesworth, 2018).
Implications for Dementia Service Provision
This study has highlighted the value placed by families living with dementia on having access to a consistent, knowledgeable, and skilled source of advice and support. It has also highlighted the additional stress experienced by carers, over and above their caring role, where they perceive that support to be in danger of being withdrawn.
In a climate of reducing resources and frequent closures, the feedback in this study reinforces the need for commissioners of services to pay attention to sustainability, as well as efficiency, when reviewing existing services or developing new ones.
Strengths and Limitations of This Study
This study is the first cross-teams survey of experiences of family carers in receipt of support of Admiral Nurses since Clare et al. (2005), which was an externally commissioned evaluation. Building on the previous survey, it shows continuity in the reporting from the family carers with regard to both the perceived benefits of Admiral Nursing support and difficulties experienced. Three of the four researchers were internally employed by Dementia UK, and although steps were taken to minimize confirmation bias by rooting the analysis in the quotes and in external literature accessed post-analysis, we cannot fully exclude that there may be an influence on our work.
This was run as a postal survey, the sample of respondents is open to self-selection bias, as participation in the survey was voluntary. Carers who could not read and write in English, or were visually impaired, were also limited in their access to the survey as it was solely provided in English and in non-tactile print. Although we know from the demographics that the profile of the respondents is consistent with the national profile of carers of people with dementia (Alzheimer’s Research UK, n.d.), we are not able to state whether they were representative of the population on caseload of each team at the time of the survey. The findings presented in this article are from the qualitative arm of the study, and although they may be transferable to other settings, we do not claim that they are generalizable.
Footnotes
Appendix
Questions for the Nine Sections With Free Text Box Available.
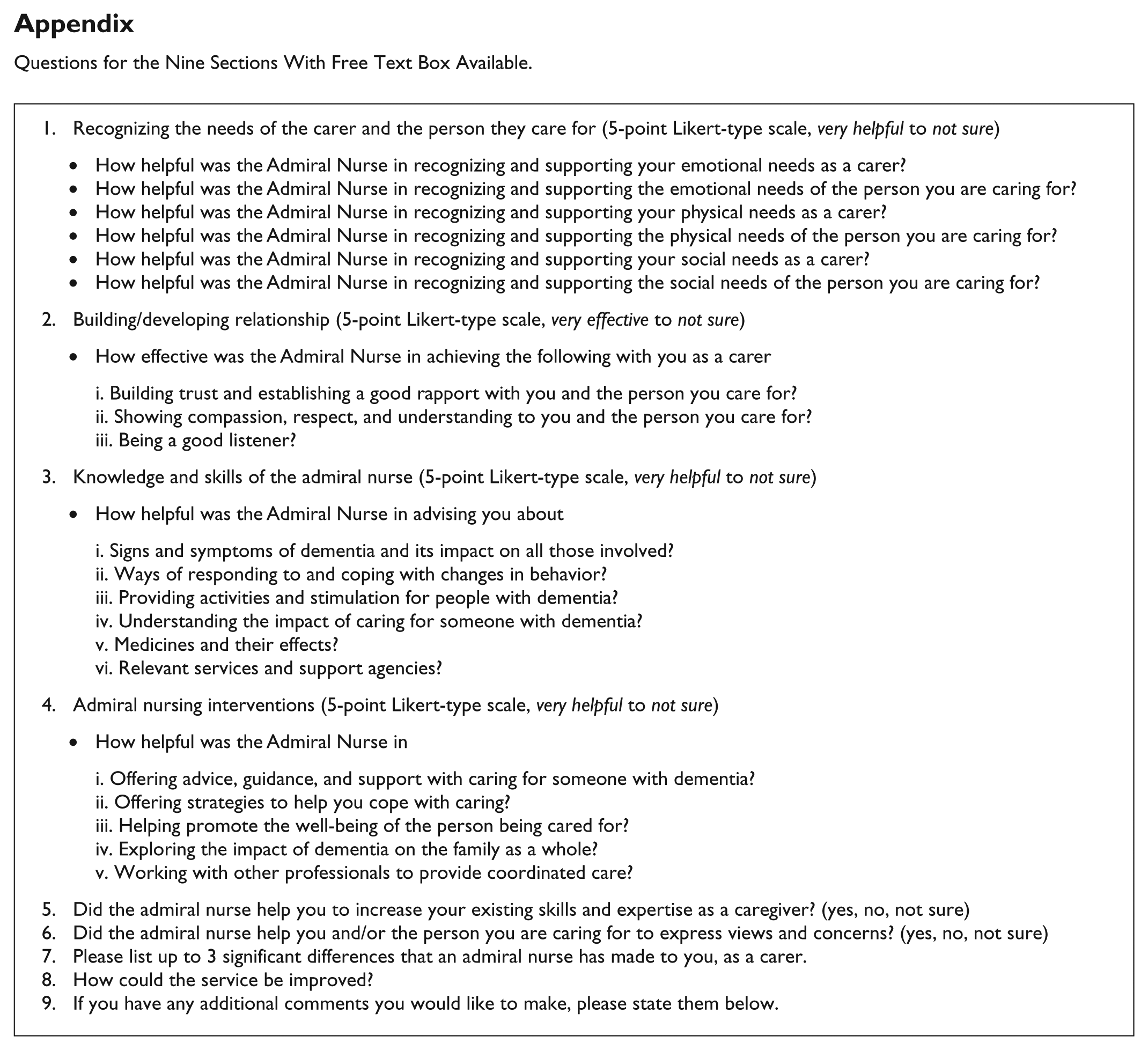
| 1. Recognizing the needs of the carer and the person they care for (5-point Likert-type scale, very helpful to not sure) • How helpful was the Admiral Nurse in recognizing and supporting your emotional needs as a carer? • How helpful was the Admiral Nurse in recognizing and supporting the emotional needs of the person you are caring for? • How helpful was the Admiral Nurse in recognizing and supporting your physical needs as a carer? • How helpful was the Admiral Nurse in recognizing and supporting the physical needs of the person you are caring for? • How helpful was the Admiral Nurse in recognizing and supporting your social needs as a carer? • How helpful was the Admiral Nurse in recognizing and supporting the social needs of the person you are caring for? 2. Building/developing relationship (5-point Likert-type scale, very effective to not sure) • How effective was the Admiral Nurse in achieving the following with you as a carer i. Building trust and establishing a good rapport with you and the person you care for? ii. Showing compassion, respect, and understanding to you and the person you care for? iii. Being a good listener? 3. Knowledge and skills of the admiral nurse (5-point Likert-type scale, very helpful to not sure) • How helpful was the Admiral Nurse in advising you about i. Signs and symptoms of dementia and its impact on all those involved? ii. Ways of responding to and coping with changes in behavior? iii. Providing activities and stimulation for people with dementia? iv. Understanding the impact of caring for someone with dementia? v. Medicines and their effects? vi. Relevant services and support agencies? 4. Admiral nursing interventions (5-point Likert-type scale, very helpful to not sure) • How helpful was the Admiral Nurse in i. Offering advice, guidance, and support with caring for someone with dementia? ii. Offering strategies to help you cope with caring? iii. Helping promote the well-being of the person being cared for? iv. Exploring the impact of dementia on the family as a whole? v. Working with other professionals to provide coordinated care? 5. Did the admiral nurse help you to increase your existing skills and expertise as a caregiver? (yes, no, not sure) 6. Did the admiral nurse help you and/or the person you are caring for to express views and concerns? (yes, no, not sure) 7. Please list up to 3 significant differences that an admiral nurse has made to you, as a carer. 8. How could the service be improved? 9. If you have any additional comments you would like to make, please state them below. |
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Laura Maio is employed by Dementia UK; Dr Julia Botsford and Dr Karen Harrison Dening are Admiral Nurses and employed by Dementia UK.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.