
Abstract
People with dementia (PWD) are fragile and need aid and care in their daily lives. This scoping review explores the extent to which PWD can be involved in society and their daily lives. Publications were selected according to PRISMA guidelines. We graded the level of participation/involvement in daily life and research using a five-level participation model developed by Shier. A higher grade means a greater ambition to involve PWD in decisions. Of the 11 included studies, three reached level three according to Shier’s model. The studies describe ways of and potentials for participation, capabilities of PWD, caregivers’ opportunities to foster involvement, and cooperation between PWD caregivers and relatives. Caregivers and managers must have the attitude that PWD can be involved in decisions and caregivers need opportunities to actively promote such involvement. Shier’s model can be a tool with which organizations strive to involve PWD.
Keywords
Living With Dementia Is a Growing Social Challenge
Fifty million people are living with dementia worldwide (World Health Organization [WHO], 2020), and social workers must be prepared for the increasing number of such people needing everyday support to live their lives as well as possible. According to the International Federation of Social Workers (IFSW, 2020), the profession can promote older adults’ dignity and inclusion in decision-making at all levels of society. Social workers focus on the social inclusion of people with dementia (PWD) as a crucial part of their roles (Hokenstad & Roberts, 2011). In some countries, social workers can be care managers, and social workers are responsible for the assessment and placement of people with dementia and follow-up of placements when conditions change. Social workers are sometimes managers of nursing homes. Thus they have an important role even if they are not always involved in the daily care of the PWD (Österholm, 2016; Vård och omsorgsanalys, 2021).
We use the acronym PWD in this study. However, we are aware that people with dementia should not be assumed to lack the capacity to participate in decision-making, even if they no longer live independently, as for example emphasized in the UK Mental Capacity Act (National Health Service, 2005). As dementia is among the most common reasons for living in a nursing home (NH) (Smith et al., 2000; Toot et al., 2017), caregivers must find ways to involve NH residents despite their cognitive disabilities (Jakobsen & Sörlie, 2010), and caregivers’ approaches to the involvement of residents in decisions range from independent decision-making to exclusion from decision-making (Erlandsson et al., 2022). However, the social worker can support caregivers to work toward greater involvement of residents (Hardy et al., 2020).
Civil Rights/Human Rights
According to the WHO (2020), people’s participation is defined in terms of their engagement in particular life situations, and civil rights are as essential for PWD as they are for other citizens. PWD must be seen as active agents in society (IFSW, 2020). Shakespeare et al. (2019) argued that PWD can be considered people with a disability, whose daily experience is affected by their environment. Dementia is often considered a disease, but here we define dementia as a disability according to the reasoning of Shakespeare et al. (2019). We will strengthen the rationale of PWD as people with disabilities. We therefore include the group of PWD in The United Nations (UN, 2006) Convention on the Rights of Persons with Disabilities (CRPD), which states that people with disabilities have rights to independent living (article 19), freedom of expression (article 21), and participation in culture, recreation, and leisure (article 30). Cieza and Kostansjek (2021, p. 1), referring to the International Classification of Functioning, Disability and Health (ICF), argued that “the individual, the experience of health and disability depending on the physical, human-built, attitudinal, and socio-political environment all play a role for an inclusive environment.”
Nedlund and Bartlett (2017) emphasized that PWD are active agents who exert power over their own lives as actors in society. Informal/formal caregivers must support PWD so that they can interact with those in their social context. Citizenship concerns autonomous persons and their ability to understand their situation; however, this may sometimes be impossible for PWD due to cognitive impairment. Citizenship must therefore be explored in a different way. The citizenship of PWD has been studied in terms of rights to, belonging to, access to, and participation in the community (Nedlund & Bartlett, 2017). According to Kelly and Innes (2011), PWD may be denied human and civil rights when caregivers prioritize protection from harm instead of considering human rights. Kelly and Innes (2011) suggested a practice based on dignity and respect, and how such a practice works depends both on caregivers’ understanding of human rights and on having the right conditions to promote participation. Caregivers and care managers must develop a culture in which participation in daily life is prioritized (Helgesen et al., 2014). There is a link between empowerment among caregivers and empowerment among care receivers. Laschinger et al. (2010) identified empowerment as a precondition for both care recipients and caregivers if care recipients are to be supported. According to Kontos (2011), PWD can be involved in care decisions even if they cannot communicate their wishes. Haugen et al. (2019) stated that PWD can be involved in care decisions if they are supported by relatives or caregivers.
Previous Research About Daily Life in Nursing Homes for PWD
Symptoms of dementia may worsen if psychosocial needs such as attachment, comfort, identity, inclusion, and love go unmet. Kitwood (1997) advocated person-centered care to meet PWD needs. In person-centered care, caregivers treat all PWD as unique individuals. Scales et al. (2017) examined the interaction between people and their environment and noted that formal caregivers need empowerment to enhance person-centered care. According to Boumans et al. (2019), formal caregivers should have a flexible attitude toward residents’ needs, behaviors, and wishes, and should welcome informal caregivers and efforts to promote residents’ autonomy. The care environment and technology can improve autonomy for NH residents. In a systematic review, Davies et al. (2019) described how decision aids (i.e., videos, booklets, or web-based tools) can improve caregivers’ abilities to facilitate decisions regarding PWD. Moreover, caregivers need the knowledge to promote autonomy in NH residents. However, balancing PWD’s opportunities for autonomy against protection from harm is a difficult and ongoing effort (Holm, 2001; Sammet, 2007). Taghizadeh Larsson and Österholm (2014) found that most care decisions regarding PWD were made by relatives alone with no PWD involvement. These researchers noted that more research was needed regarding PWD and their right to make decisions about care services. Bolling et al. (2016) recommended further research on how to involve PWD in decision-making in NHs, given that most relevant research emphasizes the caregiver perspective, not that of PWD. This includes both PWD and the caregivers’ efforts to support PWD. A social worker can play an essential role in supporting caregivers in nursing homes, according to Hardy et al. (2020). Examples of what a social worker can contribute within a nursing home are holistic care, supporting the needs of staff, residents, and their relatives, advocacy, and supporting decision-making between PWD and staff.
Aim of Study
Since both PWD and how they are supported by staff play a role in the agency of PWD, we included both perspectives in this scoping review. The following research questions were accordingly formulated:
What is known from the literature about PWD living in NHs and their opportunities to be active agents in their daily lives?
How do caregivers facilitate participation (methods and level of influence) among PWD living in NHs?
Theoretical Framework for Participation
Shier’s (2001) model can be used as a tool by organizations when planning for and facilitating user participation. The model contains five levels of participation and was originally constructed to describe children’s opportunities to participate in decisions. In addition to levels of involvement, the model is also based on three stages of commitment—openings, opportunities, and obligations—in which the organization fosters participation in different ways. There is one question for each level in the model, so organizations can determine at which level they are positioned regarding participation among children (Shier, 2001). Although Shier was mainly describing children’s participation, the model is also used among adults with cognitive disabilities (Talman et al., 2019). Furthermore, Talman et al. (2019) noted that people with intellectual disabilities depend, in their daily lives, on others who also control their opportunities to participate. A similar situation faces PWD regarding their opportunities to participate (Figure 1).

Levels of participation of people with dementia.
Method
To answer the research questions, a scoping review was chosen as the appropriate research design (Arksey & O’Malley, 2003). We used the PRISMA extension for scoping reviews (Tricco, 2018).
Included Papers
Original peer-reviewed empirical papers written in English and published between 2010 and 2020.
The papers had to examine PWD living in NHs and explore how PWD can be active agents in their daily lives.
PWD’s own viewpoints had to be treated in the papers. PWD must have interacted with the researcher(s) in interviews, informal talks, and image support.
We identified the included papers using Shier’s (2001) theoretical framework of participation to capture whether (according to the papers) PWD were involved in their daily lives, how their perspectives were considered, and how caregivers facilitated PWD involvement.
Excluded Papers
Studies about moving into NHs
Studies of PWD, including those in palliative care, if they did not describe PWD involvement in daily life in NHs
Studies of PWD living in their own homes, with or without homecare, or visiting daycare
Observational studies in which PWD were not involved as agents
Reviews and books
Information sources
To identify potentially relevant abstracts, we searched the following bibliographic databases from January 2010 to June 2020: PubMed, Psych Info, SocIndex, Cinahl, WoS, Scopus, Academic Search Elite, Science Direct, Social Services Abstracts, and Sociological Abstracts. The following search terms (and similar terms) were used: TITLE-ABS-KEY: dementia, nursing homes, autonomy.
Data
We extracted data on how the NHs involved PWD in decisions regarding their daily lives and how the researchers and caregivers interacted with PWD to facilitate such involvement. We synthesized the included papers and analyzed them regarding the involvement of PWD in decisions and the NH organizations’ preparedness to facilitate such involvement.
Selection of Sources of Evidence
Two of the authors independently screened the sampled titles and abstracts using Rayyan, a web application for screening abstracts (Ouzzani et al., 2016). In total, 3100 abstracts were identified, and a library technician removed duplicates. To promote transparency, we used a PRISMA flow chart (Moher et al., 2009). After reviewing the abstracts, we discussed the 42 remaining full-text publications. A third author was consulted if disagreements occurred regarding abstracts or regarding the evaluation of articles related to Shier’s (2001) model. The selection process ended with the identification of ten publications. In addition, we searched the reference lists of the included publications for relevant papers and found five, one of which was included in the review. In total, 11 publications were selected for the scoping review (Figure 2 and Table 1).
Results

Flow chart according to PRISMA.
Included Publications.

How we used Shier’s model
We interpreted and rated the papers in accordance with Shier’s five-level model. To illustrate this rating approach, we use Serarano Cardona et al. (2013) as an example. In the first column of Table 2, we consider the level of involvement in daily life: in Serarano Cardona et al. (2013), PWD expressed their viewpoints, but could not affect decisions and were not helped to express their views. The caregivers were ready to listen to PWD, achieving level one in Shier’s model; for a higher level, they must take responsibility for helping PWD to express their views.
Interpretation of Shier’s Key Concepts.
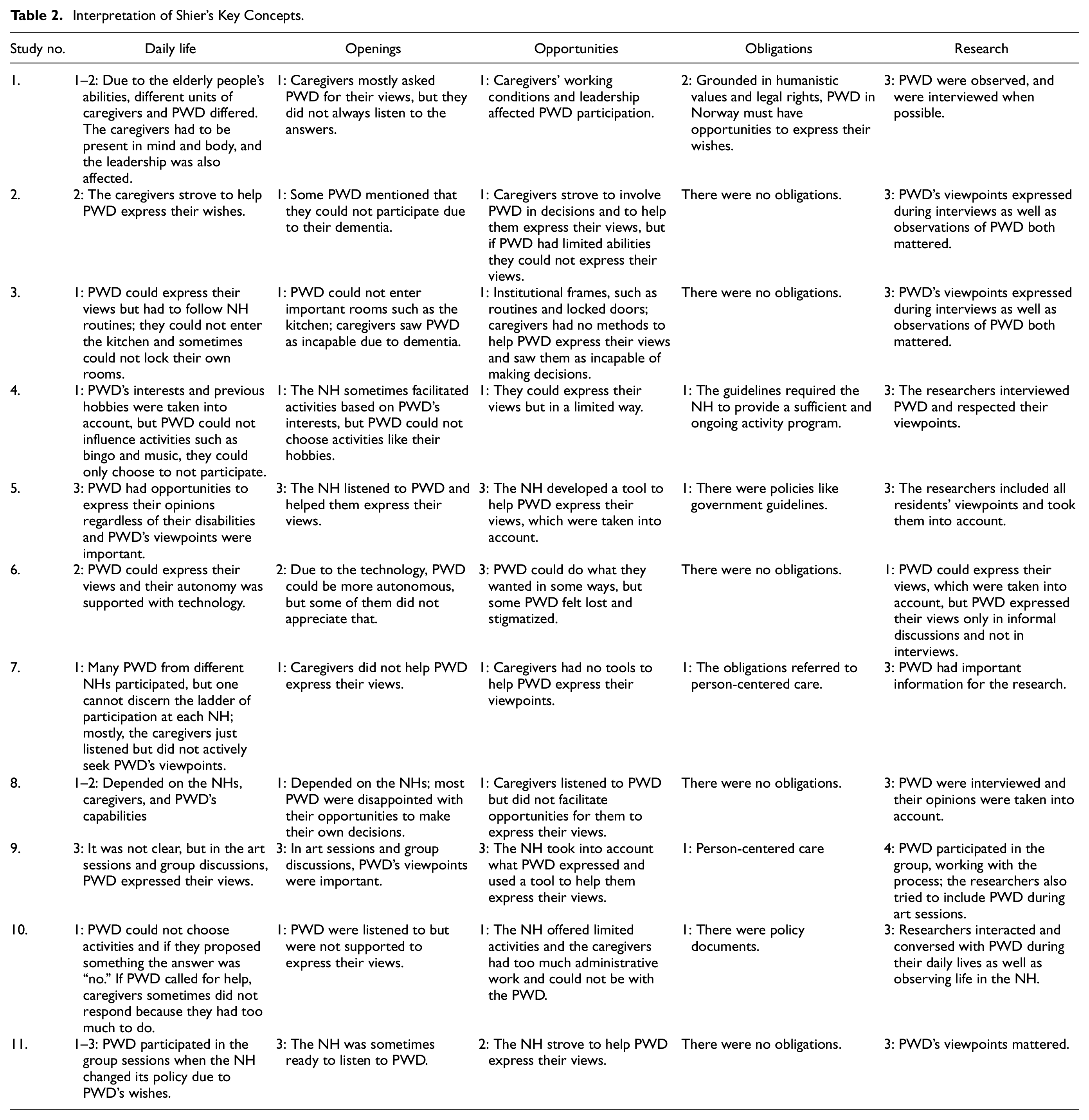
The second column is about openings, that is, how to facilitate caregivers and the involvement of PWD. In Serarano Cardona et al. (2013), the caregivers only attained level one, as they did not help PWD overcome barriers to expressing their views (e.g., the PWD had limited opportunities to affect the schedule when they chose activities). Column three is about opportunities for PWD to express their views, and whether staff have time to listen to them. The organization studied in Serarano Cardona et al. (2013) lacked a range of methods to facilitate PWD involvement (e.g., if the organization had tools such as visual methods to facilitate PWD opportunities to express views, it would have achieved a higher level according to Shier’s model).
Column four is about obligations, and in Serarano Cardona et al. (2013), these referred to guidelines the NH should follow regarding participation. The fifth column is about how the authors of the included publications interacted with PWD; according to the inclusion criteria, the researchers had to determine the PWD’s viewpoints. In Serarano Cardona et al. (2013), the researcher interviewed PWD and reported their viewpoints in the results, resulting in a higher level (i.e., level three) according to Shier’s model. Table 2 presents the publications categorized according to Shier’s model: column one, participation in care; column two, the organization’s openings for participation; column three, the organization’s opportunities for participation; column four, the organization’s obligations regarding participation; and column five, the ladder of participation in the research.
Synthesis of the results
PWD could be involved in decisions related to their cognitive and physical abilities (Helgesen et al., 2010), express opinions on NH architecture (Godwin, 2014), and express viewpoints on how to live their daily lives (Godman et al., 2013). The NH organizations could set rules that PWD had to follow; for example, PWD could not enter all the rooms in the NHs (Heggestad et al., 2013). According to Serarano Cardona et al. (2013), care workers tried to determine what PWD were interested in, but the activities were not adapted to PWD’s wishes. The PWD–caregiver relationship was the precondition for participation (Bolling et al., 2016; Helgesen et al., 2010; Mondaca et al., 2018). Studies described by Godwin (2014), McKeown et al. (2016), and Shura et al. (2011) reached the highest level of participation in all dimensions of Shier’s model. The caregivers created groups working with managers, PWD, and relatives in the studies by McKeown et al. (2016) and Shura et al. (2011). When ideas were raised in these working groups, they were tried out in a practical context. Moreover, these two studies involved PWD participation in decisions regarding the NH organization, whereas PWD participation in the other studies was mostly relevant to individual decisions. Godwin (2014) used tools to facilitate participation so that even persons with severe disabilities could be involved in decisions. In the studies by Godwin (2014), McKeown et al. (2016), and Shura et al. (2011), the organization tried to help PWD express their viewpoints, resulting in a higher Shier’s model score regarding openings and opportunities.
In the study by Niemeijer et al. (2015), technology helped PWD to be more autonomous, but not all of them appreciated the technology: some felt stigmatized, and that the technology did not help them express their viewpoints and wishes. Heggestad et al. (2013) found that caregivers asked PWD for input but did not listen to the responses, so caregivers did not help PWD express their views. Feeling at home was complicated, because PWD did not recognize the other residents in NHs (Heggestad et al., 2013). Most PWD were dependent on caregivers to involve them in decisions regarding their daily lives (Bangerter et al., 2016; Bolling et al., 2016; Godman et al., 2013; Heggestad et al., 2013; Helgesen et al., 2010). Moreover, PWD described a lack of autonomy (Bangerter et al., 2016; Bolling et al., 2016; Heggestad et al., 2013), and PWD could make decisions regarding their lives if given the opportunity (Godman et al., 2013). Lack of caregiver time and short staffing reduced interactions with PWD and their opportunities to be involved (Mondaca et al., 2018).
Involvement in research generated a higher level of PWD participation, according to our interpretation of Shier’s model, due to our inclusion criterion that PWD should be involved. Most publications reported factors affecting PWD’s opportunities to be involved in decisions, for example: caregiver attitudes, caregiver working conditions, architecture, relatives, PWD capabilities, technology, leadership, and cooperation between PWD’s caregivers and relatives.
Regarding obligations for PWD to be involved in decisions affecting their daily lives, we found five studies that did not refer to policy documents (Bolling et al., 2016; Godman et al., 2013; Heggestad et al., 2013; Niemeijer et al., 2015; Shura et al., 2011). Two studies referred to person-centered care (Bangerter et al., 2016; McKeown et al., 2016), and four referred to documents concerning civil rights or local policies (Godwin, 2014; Helgesen et al., 2010; Mondaca et al., 2018; Serarano Cardona et al., 2013).
Discussion
The included publications were about how PWD could be involved in decisions regarding their daily lives as well as any required interactions with researchers. The first question was: What is known from the literature about PWD living in NHs and their opportunities to be active agents in their daily lives?
PWD could be involved in decisions regarding their daily lives and the NH organization, but most reviewed publications described such participation as at a low level in terms of Shier’s model and the individual level (Table 2, column one). Some of the included studies referred to policy documents concerning civil rights and person-centered care that addressed PWD involvement in decisions. Moreover, this review shows that there are civil rights demands related to PWD involvement in NHs, and that NHs can themselves strive to foster PWD involvement. Furthermore, person-centered care and a holistic approach to PWD are essential.
The second question was: How do caregivers facilitate participation? Each interaction between PWD and their caregivers is unique, depending on various factors such as PWD capability, caregiver experience and attitudes, the working environment, resources, support, and leadership that facilitates the caregiver role. Using the categorization of Shier’s ladder of participation, we found that nursing homes should be prepared to value and facilitate participation. If the caregivers obtained support from their organizations and managers, they had better preconditions for addressing PWD participation.
According to Haugen et al. (2019), caregivers or relatives must help PWD take part in decision-making. If caregivers are to help empower PWD to become involved in decisions regarding their daily lives, they must first experience their own empowerment. If caregivers are to empower PWD, they need access to information, support, resources, opportunities to learn/grow, and formal/informal power, all of which affect their behavior and work attitude in the workplace (Laschinger et al., 2010). According to Mondaca et al. (2018), caregivers need time and sufficient staffing to support PWD participation. PWD participation was not prioritized in hectic daily life in NHs, and unskilled caregivers could not strive to involve PWD. Caregivers were more interested in satisfying colleagues’ expectations than in involving PWD in decisions. The results of this scoping review confirm that some PWD need support from caregivers, and that, if they get this support, they can participate in decisions regarding both the organization level and their own lives, according to the CRPD (UN, 2006).
According to Kitwood (1997), person-centered care means that caregivers should involve PWD in decisions. However, Kitwood also noted that all PWD differ, and that caregivers should consider PWD’s lived experiences. Our results highlight the complex interactions between PWD and caregivers, who all are unique. Using Shier’s model, we identified the enablers of and barriers to achieving participation, including dimensions affecting participation: capabilities, caregivers’ conditions for addressing participation, and cooperation between PWD, caregivers, and relatives.
The studies reporting the highest level of involvement according to Shier’s model (i.e., Godwin, 2014; McKeown et al., 2016; Shura et al., 2011) used some form of aid (ballot card) or model (PAR) to facilitate PWD involvement. Decision aids could facilitate the involvement of PWD in decisions (Davies et al., 2019). Most publications reviewed here found that NHs lacked such aids. Attitudes toward involving PWD and seeing them as autonomous affected how the studied NHs managed such involvement (Bangerter et al., 2016; Bolling et al., 2016; Heggestad et al., 2013).
Shier’s model has been criticized, mainly because its different steps or levels could be interpreted as a hierarchy of participation illustrating how adults in organizations could help children express their views (Cahill & Dadvan, 2018). Our review found that PWD could not reach the highest level of participation due to their cognitive capabilities and reliance on decision aids in their daily lives (Haugen et al., 2019). However, Shier’s (2001) model could be a first step toward developing an action plan addressing PWD participation, and the model could help NH staff identify where they are on the ladder regarding work on participation.
The Role of Social Workers
The reviewed articles did not specifically discuss social workers’ role in NHs and how they could help promote PWD participation. Perhaps both social workers and NHs have some work to do regarding this, particularly to improve the preconditions for participation. Social work is sometimes viewed as a human rights profession (Mapp et al., 2019; Reynaert et al., 2022); and, according to the IFSW (2020), social workers must promote civil rights for PWD. However, Erlandsson et al. (2022) argues that caregivers in NHs need policy documents that clarify involvement for PWD and organizational support to implement that. Furthermore, some caregivers in NHs exclude PWD from decisions and act based on their observations without asking for the PWD’s opinion. This scoping review confirmed that nursing homes could improve the work with participation from PWDs’ point of view. Social workers can support caregivers’ readiness to involve PWD in decisions (Hardy et al. 2020).
Moreover, if we define dementia as a disability in line with Shakespeare et al. (2019), then social workers have grounds to strengthen the work in NHs according to the civil rights of PWD and support formal caregivers to work in line with CRPD (UN, 2006). Furthermore, social workers in some countries work as care managers and are responsible for assessing needs and the placing of PWD in nursing homes (Österholm, 2016). As care managers, social workers can promote Shier’s model as a tool in the effort to increase participation. Hardy et al. (2020) argued that social workers can use an interdisciplinary approach to finding ways to help stakeholders improve PWDs’ psychosocial life, dignity, well-being, worth, and quality of life. Examples of roles for social workers in NHs are supporting PWD’s and formal/informal caregivers’ needs, facilitating PWD decision-making, and striving for a holistic approach to care in NHs. Bangerter et al. (2016) illustrated the importance of interpersonal interactions that promote person-centered care. Heggestad et al. (2013) emphasized the importance of caregivers seeing the whole person and their abilities. Moreover, social workers could have a crucial role in person-centered care in NHs and in supporting decision-making by PWD, who are unheard due to their disabilities (Hardy et al., 2020).
Limitations
We only included studies that reached at least participation level one according to Shier’s model, due to our inclusion criterion requiring the active involvement of PWD in decisions about daily life, as shown in the reviewed research. Many studies only observed PWD but did not actively interact with them in the research process, and those studies were excluded. The reviewed articles came from different countries, and we have no information about who the studied caregivers and managers were, what kind of education they had, or whether the NHs were for-profit or nonprofit institutions.
Conclusion
Despite the complexity of PWD participation, we propose that PWD can be involved in decisions at different levels in NH organizations, but that they need support in this.
The Shier (2001) model can help organizations identify how to manage PWD involvement in decisions.
Managers should strive to involve PWD in decisions and give caregivers time and tools to work with PWD, mainly because of demands for civil rights for PWD.
More professionals applying a holistic/person-centered approach would help promote PWD participation in NHs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.