
Abstract
Continuing education in nursing homes (NHs) is facing a transition to distance learning, such as web-based education, as demonstrated during the COVID-19 pandemic. Since behavioral and psychological symptoms of dementia (BPSD) are managed through integrative direct care by nursing staff, including nurses, nursing assistants, and care workers with diverse educational backgrounds and needs, an effective and efficient web-based education program with a concrete pedagogical and theoretical basis is essential. Therefore, this study aimed to develop an adaptive learning web-based BPSD education system for NH nursing staff. The adaptive learning web-based BPSD education program, with an embedded artificial intelligence chatbot, was developed based on the frameworks of BPSD education and adaptive learning models. The educational program was evaluated using a multisite, single-blinded, quasi-experimental design. Fifty-eight nursing staff were recruited from five different NHs. The experimental group received an adaptive learning system that tailored content to prior knowledge, while the control group received a non-adaptive web-based system. The results from the analysis indicated that all components of learning effectiveness, including BPSD competence, BPSD knowledge, and self-efficacy, were significantly improved in the experimental group compared with the control group. System satisfaction was significantly higher in the experimental group than in the control group, and 75% of the participants in the experimental group actively adapted their individual educational content. These findings indicate that the adaptive learning system had positive outcomes on learning and system effectiveness, suggesting an innovative strategy toward a “new normal” education for NH nursing staff in the post-COVID-19 era.
Keywords
Background
Continuing education in nursing homes (NHs) is an essential way for nursing staff to retain and enhance their provision of high-quality care for improving residents’ health status and quality of life (S. J. Lee et al., 2020; Moreno-Martin et al., 2022; Riesch et al., 2018). As demonstrated during the COVID-19 pandemic, the need to develop effective distance learning systems such as web-based education programs has been increasing in tandem with nursing staffs’ increased workloads and concerns on infection prevention and control (Edelman et al., 2020). Free from most time and space constraints, web-based education possesses the advantages of convenience and flexibility without compromising nursing staff working hours while also providing a versatile and cost-efficient approach (Choi et al., 2021; McDermid et al., 2024; X. Xie et al., 2020; Yoshioka-Maeda et al., 2019). Previous studies have reported that web-based education has positive impacts on nursing staff in increasing their knowledge and efforts at better practice in major NH problem domains, including infection control, management of pain, and emergency care (Choi et al., 2021; Hendricksen et al., 2022). Given these advantages, it is expected that constructing and applying effective web-based education will continue to receive attention after the COVID-19 pandemic has subsided (Choi et al., 2021; Edelman et al., 2020).
Behavioral and psychological symptoms of dementia (BPSD), common among residents of NHs, affect their quality of life by influencing factors such as pain, agitation, and engagement in activities, with varied assessment and care methods (Jeong et al., 2021; E. Y. Kim et al., 2020; Y. N. Lee et al., 2021; Lim et al., 2022). Improving BPSD care competence has been a major dementia education goal for nursing staff in NHs (Ho et al., 2015; Taneichi & Rokkaku, 2020). Choosing an appropriate pharmacological and/or non-pharmacological approach is a comprehensive process that simultaneously considers both a resident’s presenting symptoms and personal characteristics, while also taking into account the facility’s environment (Kales et al., 2015; D. Kim et al., 2022, 2024a). Therefore, BPSD care in NHs requires more intensive education. However, BPSD has typically been covered as part of broader dementia education rather than receiving a dedicated focus, resulting in limitations in the depth and specificity of content related to NH settings (Bauer et al., 2018; Wang et al., 2020; Y. Zhao et al., 2021). The lack of specialized BPSD education has been a global concern among healthcare professionals, as it may hinder the effective BPSD care in NHs (Kales et al., 2020; W. Zhao et al., 2022). Since 80% of the residents with dementia in NHs show more than one symptom of BPSD, developing an effective web-based education centered on BPSD would improve the quality of dementia care practice and residents’ quality of life (Lu et al., 2022; Song & Oh, 2015; Yasuda & Sakakibara, 2017).
In NHs, BPSD are managed by integrative nursing staff care that includes nurses, nursing assistants, and care workers. They share the common duty of providing direct care to the residents with BPSD, but as their professions are different, their educational background and needs also differ (Taneichi & Rokkaku, 2020). However, web-based education has been mostly limited to assisting face-to-face lectures by providing digital materials such as video (Kutschar et al., 2020; Y. Zhao et al., 2021). Such limited web-based education, which delivers only uniform information, neither considers the learners’ various educational backgrounds and needs nor provides opportunities for communication between educators and learners (Y. Zhao et al., 2021). In addition, although a web-based education that has a specific pedagogical basis and educational framework could effectively improve nursing practice in NHs, most such programs had no theoretical basis (Choi et al., 2021, 2022; Y. Zhao et al., 2021). These limitations led to inconsistent results in educational outcomes related to practical practice such as competence and self-efficacy, even though nurses’ knowledge levels may have been increased (Y. Zhao et al., 2021). Therefore, a systematic and effective BPSD education must be constructed based on a specific theoretical basis.
In this context, adaptive learning could be considered an innovative educational strategy for an effective web-based BPSD education. Adaptive learning is a pedagogical strategy that enables individually tailored approaches according to the learner’s characteristics and needs (Andersen et al., 2021; Gligorea et al., 2023; Vincent et al., 2017). It is based on constructivist theory, which emphasizes that an education is an individual process of constructing according to each learner’s perception, an activity beyond simple knowledge transfer. By adapting time and content according to individual needs, focusing on only the necessary elements, adaptive learning enables individual approaches, which are reported to be more effective in improving learner’s knowledge, competence, and self-efficacy (Hinkle et al., 2020; Martin et al., 2020). Providing a differentiated educational experience has been reported to be more appropriate for attaining educational benefits than the traditional uniform approach that targets average learners (Demartini et al., 2024; Sarnato et al., 2024; Shamir et al., 2019). Adaptive learning’s efficiency and effectiveness are further increased when it is used in web-based education; hence, many efforts are currently being made for developing web-based adaptive learning systems in university education and for healthcare professionals (Andersen et al., 2021; Martin et al., 2020). In particular, efficiency and effectiveness have been verified in nursing students’ education (Andersen et al., 2021; Cardiel et al., 2022; Hinkle et al., 2020). Characterized with technological drive, difference of learners, and learner-focused education, adaptive learning in nursing education has positive consequences of increasing learners’ interest and engagement in education and achieving overall learning success (Cardiel et al., 2022). Considering the strength of adaptive learning in nursing education, it can be expected that applying adaptive learning to nursing practice will generate great positive outcomes, especially in terms of BPSD care in NHs, where integrative direct care is provided by nursing staff whose educational needs vary.
Individualized approaches and interactions facilitate the efficiency of web-based education (Moehead et al., 2020). An adaptive learning web-based education can overcome the limited function of providing simple information online by promoting communication between instructors and learners, which can create a powerful synergy. Therefore, we aimed to develop an adaptive learning web-based BPSD education system and investigate its effect on outcomes in learners and systemic aspects to illuminate a new direction in continuing education for NH nursing staff. We hypothesized that there would be a significant difference in mean scores for BPSD competence, BPSD knowledge, self-efficacy, and system user-friendliness and satisfaction between nursing staff who received adaptive learning web-based BPSD education and those who received non-adaptive web-based education.
Methods
Contents Design
The program’s educational contents were developed based on a preliminary educational framework that guides the core domains of BPSD care practice in NHs (D. Kim et al., 2022). This framework was constructed by focusing on NH nursing staff who provide direct care to residents with BPSD, rather than on a broad and general context. The educational content was designed through an extensive literature review, incorporating evidence-based guidelines for BPSD care (Table 1).
Contents of Education.

Note. BPSD = behavioral and psychological symptoms of dementia.
Adaptable content, which learners can skip.
Non-adaptable content, which learners cannot skip.
The course encompassed both basic and core elements. The basic section provided fundamental information, while the core section included advanced competencies essential for effective BPSD care as outlined in the framework. To enhance engagement and leverage the advantages of an online learning environment, a variety of media and resources—including news articles from the National Institute of Dementia—were integrated.
To promote active learning, participants engaged in interactive activities such as fill-in-the-blank exercises, concept-matching tasks, and short quizzes embedded within each session, culminating in a multiple-choice self-test at the end of each module. Additionally, case-based learning was incorporated to reinforce the practical application of knowledge. A structured case scenario featuring an 81-year-old resident diagnosed with Alzheimer’s disease who exhibited agitation, hallucinations, and aggression, was developed to mirror real-world challenges. Learners were required to apply their knowledge from each session to this case, ultimately integrating their understanding of BPSD care by the end of the program.
To ensure content validity and clinical relevance, all educational materials—including the case scenario and the differentiation between basic and core content—were reviewed and validated by one nursing professor and two NH directors, all of whom hold doctoral degrees in nursing. Their expertise helped ensure that the learning experiences accurately reflected the complexities of BPSD care and aligned with the practical needs of NH nursing staff.
System Design
The educational program was developed based on the conceptual framework of adaptive learning models (Martin et al., 2020). The adaptive source includes the personal characteristics of the learner, and the adaptive target refers to what will be adapted according to the adaptive source (Martin et al., 2020; Vandewaetere et al., 2011). Following this theoretical framework, we structured an adaptive learning-based BPSD education program (Figure 1).
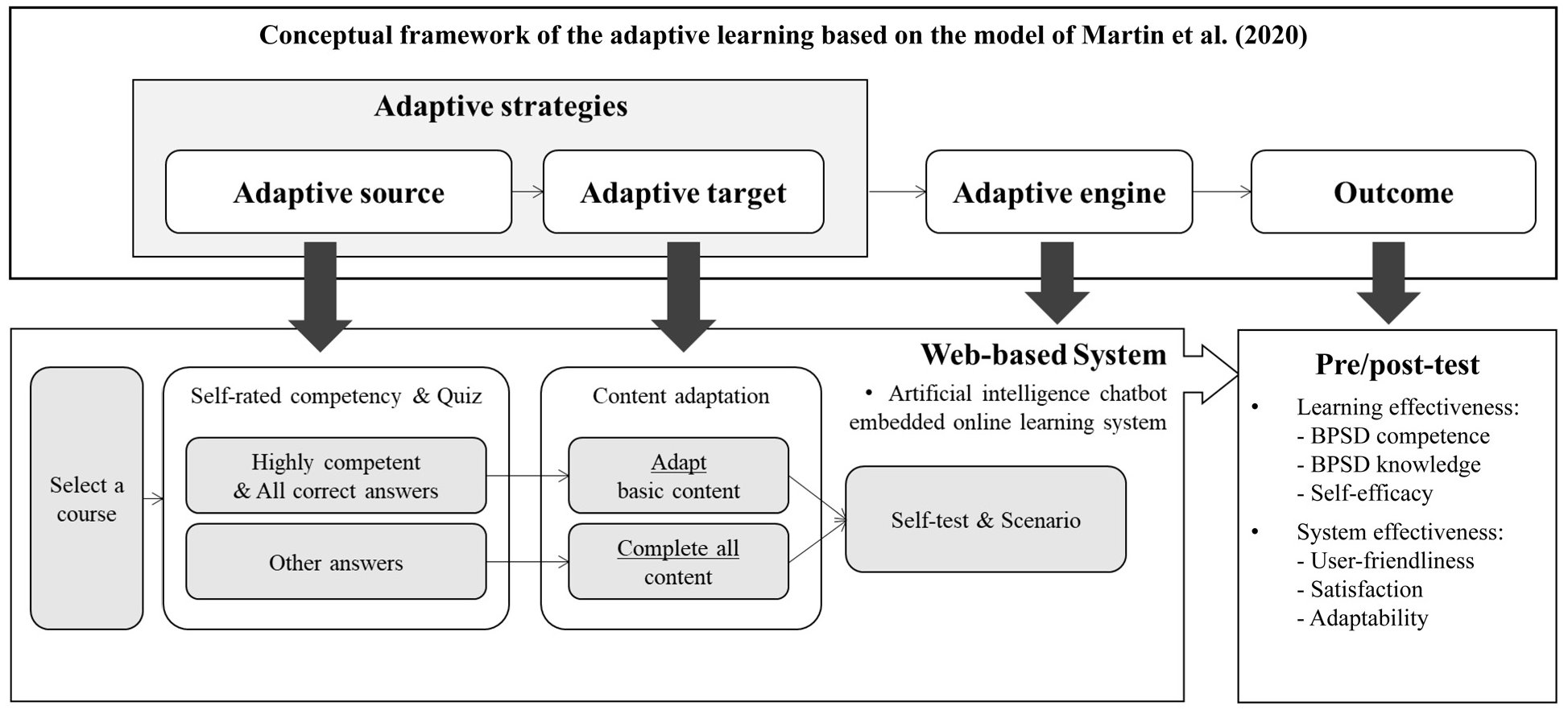
Overview of the structure of the adaptive learning web-based BPSD education program.
In our program, the adaptive source was the learner’s prior knowledge and competence in BPSD care, while the adaptive target was the educational content. If a learner correctly answered the objective quiz questions for a basic component and also rated themselves as competent in that area, the related educational content was adapted accordingly. For example, if a nursing staff member correctly answered all quiz questions and self-assessed as highly competent in a particular session, they could skip the basic content for that session. However, completion of the core content remained mandatory for all learners, regardless of their prior knowledge and competence in BPSD care.
The adaptive engine system was developed as a Google Chrome-based website with an embedded artificial intelligence (AI) chatbot that promoted an interactive learning experience. The contents display was on the left side of the website, and the AI chatbot was presented on the right side (Figure 2). The system provided a two-way interaction between the instructor and the learners via the AI chatbot. Learners were able to ask questions through the chatbot as soon as a question occurred to them. If the questions were simple ones such as about the use of the system, answers were provided automatically. However, if learners asked complex questions regarding educational content or technical problems with the system, the researchers responded in real time via the chatbot whenever available. Given the asynchronous nature of the program, researchers continuously monitored participants’ educational progress and ensured that questions were addressed as soon as possible, even if immediate responses were not feasible. This approach allowed for timely support while maintaining the flexibility for staff to complete the program at their convenience. Moreover, the AI chatbot provided learners with supplemental electronic content, such as an encyclopedia, videos, and photos, as well as hints for incorrect quiz answers and messages of encouragement to support their engagement with the program.

An example of educational program.
Experiment Design
Participant and Setting
The experiment was performed with a multisite single-blinded quasi-experimental design. Convenience sampling was conducted to sample the participants. We contacted five different NHs located in Seoul and Gyeonggi Province in the Republic of Korea whose capacities ranged from 49 to 320 residents and were certified by the National Health Insurance Service. The inclusion criteria were that the participants were nursing staff, including nurses, care workers, or nursing assistants, who were currently working in NHs. Those who had difficulties using computers, such as opening the Google Chrome browser and entering the program website, were excluded.
To estimate the sample size, a power of 0.80 and potential attrition rate of 15% were considered based on prior studies of web-based education for NH staff (Choi et al., 2021; Tompkins et al., 2020). Using the G*Power 3.1.9.4 (Heinrich-Heine-Universität, Düsseldorf, Germany) indicated that with a two-tailed test with a significance level of .05, 52 participants were required. Therefore, 60 nursing staff who voluntarily agreed to participate were recruited to the experiment, which was conducted from December 2021 to January 2022. To avoid any potential diffusion effects, participants were allocated so that there was no mixing of the experimental and control groups within the same facility. Participants in two NHs allocated as the experimental group, and those working in the three other NHs were the control group; each group comprised 30 participants. Those who did not complete the program or the survey were excluded from the analysis. Finally, 58 participants were included for analysis as two participants of the experimental group withdrew due to becoming infected with COVID-19 and resignation (Figure 3).
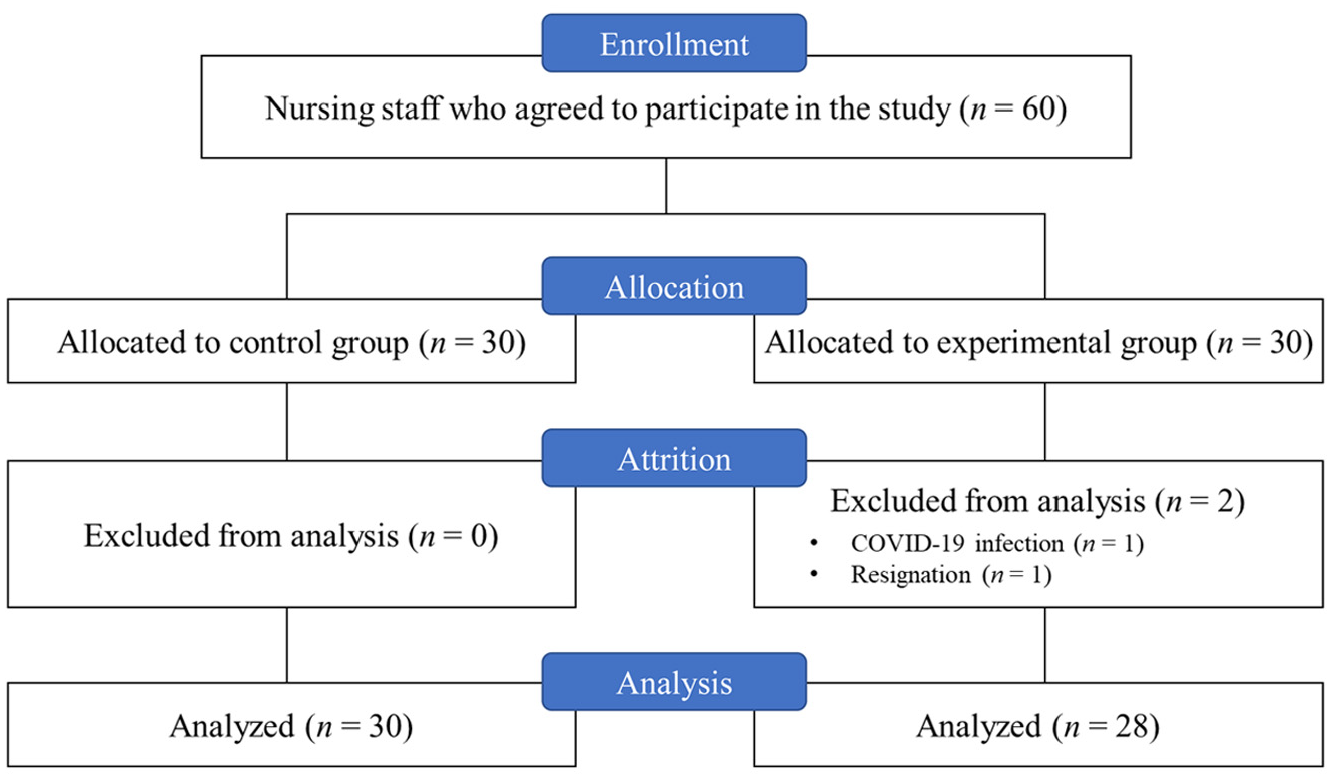
Flowchart of participant recruitment and retention.
Procedure
Before starting the education, we visited the five NHs and met with the participants to demonstrate the program and provide a basic instruction manual. Each participant was given an individual ID and leaflets with detailed explanations of the purpose of the education and how to use the program. All participants were blinded to the allocation of the experimental and control groups. The experimental group received an adaptive learning system equipped with an AI chatbot that allowed them to customize their educational experience based on prior knowledge. This system adapted content delivery by enabling learners to skip basic sections if they demonstrated proficiency through self-assessments. In contrast, the control group received a standard web-based learning system that was not adaptable. Participants in this group had to complete all content sequentially, regardless of prior knowledge, without the ability to tailor their learning experience.
The educational program that was developed required about 2 hr for the control group to complete. However, due to being able to adapt the program, the total training time for each participant of the experimental group was expected to vary. In consideration of their shift work, the participants were given about 7 days to finish the program to avoid their being pressed for time. The educational program was available 24 hr a day for the participants, allowing them to study the program at any time. During the study, the researchers were able to track the learners’ progress, answers to the quiz and self-test, and chatbot messages.
Outcome Measures
Both learning and system effectiveness were examined by online questionnaire to evaluate the outcomes of the adaptive learning program (Martin et al., 2020). The learning effectiveness, including improvements in competence, knowledge, and self-efficacy, was measured before and after the education. The system effectiveness was evaluated after the education by focusing on the system’s user-friendliness, satisfaction and adaptation features.
To evaluate the program’s learning effectiveness, tools to measure the self-rated competence in BPSD care, BPSD knowledge, and self-efficacy were used. The self-rated competence of BPSD care was constructed by researchers based on the frame of BPSD care competence (D. Kim et al., 2022). Learners were asked to rate how competent they felt (0 = not competent at all, 5 = very competent) on 10 items in four domains of BPSD care competence: “using knowledge for assessment and monitoring the status of residents (3 items),”“individualizing approaches on how to understand residents and address BPSD (3 items),”“building relationships for shared decision-making (2 items)” and “securing a safe environment for NH residents and staff (2 items).” All participants were asked to score each domain separately before the beginning of each course when they took the quiz on the preceding course content, and only the experimental group could determine the adaptability based on the scores. After the course was finished, participants were asked to score all domains again in the post-test. The analysis was calculated as the total sum of the items for a total score of 50, with higher scores indicating higher competence. Cronbach’s α was .86 in the pre-test and .92 in the post-test in this study.
The BPSD knowledge was measured by a tool consisting of 30 Items that estimated the participants’ understanding of dementia and BPSD, knowledge about the definitions and characteristics of BPSD types, and their management (Song et al., 2013). This tool is scored with 1 for correct answers and 0 for wrong ones, with higher scores indicating higher BPSD knowledge. In this study, the Cronbach’s α was .71 and .72 in the pre- and post-test, respectively.
Self-efficacy is the belief that an individual can successfully decide and perform the actions required to produce an outcome and achieve its purpose (Bandura, 1986). In the present study, it was estimated by a 17-item tool scored on a Likert 5-point scale (Sherer et al., 1982) and adapted for use in the Korean language (Jung, 2007). The total score ranged from a minimum of 17 to a maximum of 85, with higher scores indicating higher self-efficacy. Cronbach’s α was .92 in the pre-test and .93 in the post-test in this study.
To measure system effectiveness, questionnaires regarding user-friendliness, system satisfaction, and adaptability were constructed. System user-friendliness was measured with six items that asked whether the educational contents, learning activities, and system use were easy to navigate and understand. System satisfaction was measured with six items regarding the appropriateness of the courses and progress structure, satisfaction with the learning activities and scenarios, use of chatbots, and the user interface. Both the system user-friendliness and satisfaction score totals had a maximum of 30 points each, with higher scores indicating more positive evaluations. Cronbach’s α of system user-friendliness was .89 and of system satisfaction was .83. System adaptability was measured with the system records of the experimental group’s learning progress and was calculated as a proportion of participants who skipped the basic contents. Lastly, an open question for leaving any comments regarding the educational program was provided to participants at the end of the post-test questionnaire.
Data Analysis
To analyze the data, SPSS 27.0 (SPSS Inc., Chicago, Ill., USA) was used. Shapiro-Wilk tests were performed on the data to determine normal distribution, finding that the data were not normally distributed, as the significance values were less than .05 (Yap & Sim, 2011). Therefore, non-parametric statistics were performed to compare variables between and within the control and experimental groups. Descriptive statistics were used to identify the characteristics of the participants by chi-squared or Fisher’s exact tests and the Mann-Whitney U test. The Mann-Whitney U test was also utilized to identify the homogeneity of the pre-test between the groups, and Wilcoxon’s signed-rank test was performed to identify the differences of before and after the experiment within the groups. As the online education experience and the level of BPSD knowledge were not homogeneous, a ranked analysis of covariance (ANCOVA) was performed by treating those scores as covariates. All analyses were validated at a significance level of .05.
Ethical Considerations
This study was approved by the Institutional Review Board of the university (KUIRB-2021-0142-01). All participants were informed that they could withdraw at any time without any disadvantage. Written informed consent was obtained from participants involved in the study.
Results
Participants’ Characteristics
A total of 58 NH nursing staff completed the educational program and were included in the analysis. The control and experimental groups had no significant differences in their demographic characteristics. The average age was 56.29 years old, and the participants were all female except for one male in the control group (The demographic details are presented in Table 2). The participants’ professions were nurse (43.1%), nurse assistant (22.4%), and care worker (34.5%). About half of the participants were college graduates (55.8%), and the others were high school graduates (44.8%). On average, they have worked in NHs for 6.21 years. The majority of the participants had experience with online education (88%); however, the control group had significantly more participants who had experience with online education than did the experimental group (96.7% vs. 78.6%, p = .48).
General Characteristics of Participants.

Note. SD = standard deviation.
Fisher’s exact test.
p < .05.
The Baseline Homogeneity Test for the Outcome Variables of the Program’s Learning Effectiveness
Before the experiment, the baseline BPSD knowledge was significantly different between the control and experimental groups; the average score was higher in the control group (p = .043). Concerning the other pre-test variables, the experimental group participants scored lower in BPSD competence, and self-efficacy than did the control group, but the differences were not statistically significant (Table 3).
Homogeneity Test for Variables Between the Control Group (N = 30) and the Experimental Group (N = 28).

Note. BPSD = behavioral and psychological symptoms of dementia; SD = standard deviation.
p < .05.
The Outcomes of the Adaptive Learning-Based BPSD Education Program
The between-group comparisons were analyzed by the ranked ANCOVA with online education experience and baseline BPSD knowledge scores controlled as covariates (Table 4). All three components of learning effectiveness—BPSD competence, BPSD knowledge and self-efficacy—were significantly improved in the experimental group compared with the control group (F = 4.636, p = .036; F = 10.021, p = .003; and F = 10.805, p = .002; respectively). After the education without the adaptive learning system, the control group’s BPSD competence scores were significantly higher compared to their baseline scores (z = 3.141, p = .002).
Effects of the Educational Program and Differences Between the Control Group (N = 30) and the Experimental Group (N = 28).

Note. BPSD = behavioral and psychological symptoms of dementia; SD = standard deviation; CI = confidence interval; Cont. = control group; Exp. = experimental group.
Mann-Whitney U test.
Adjusted online education experience.
Adjusted online education experience and the level of pre-test of BPSD knowledge.
p < .05.
System satisfaction was significantly higher in the experimental group than in the control group (F = 10.953, p = .002, Table 4). However, there was no statistically significant difference between the groups in regard to the system’s user-friendliness, which was rated lower in the experimental group than in the control group (mean score 20.25 vs. 20.30, z = −0.117, p = .907).
Regarding adaptability, 75% of the participants in the experimental group used the system’s ability to adapt individual educational contents, while 25% did not and instead completed all the given courses, just as the control group did. Among those who adapted educational contents, 66.7% changed more than one course. On average, two courses were adapted. In detail, the most adaptation was made on the first course “using knowledge for assessment and monitoring the status of residents” (66.7% of total adaptation), followed by the third (52.4%), fourth (47.6%) and second courses (42.9%).
The comments of the participants at the end of the experiment were mostly about the system usage. Positive comments were made in regard to the appropriate and helpful contents and the interactive communication through the chatbot, for example, “It was convenient to solve the difficulties of using the program systems by asking a chatbot (participant 55, care worker).” On the other hand, there were some negative comments about the system manipulation, for example, “It was cumbersome to click a lot when editing the quiz answer (participant 16, nursing assistant),” and “The manual was helpful, but it was difficult to get used to the system at first (participant 32, nurse).”
Discussion
This study developed and evaluated an adaptive learning BPSD education system for NH nursing staff. Grounded in pedagogical theory and a robust educational framework, the program demonstrated positive outcomes for both learning effectiveness and system efficiency. Based on the principles of adaptive learning, which emphasize personalized instruction and active learner engagement, we hypothesized that nursing staff who received adaptive learning web-based BPSD education would demonstrate significantly higher mean scores in BPSD competence, BPSD knowledge, self-efficacy, and system satisfaction compared to those who received non-adaptive web-based education. This hypothesis was supported by the results. However, the hypothesis regarding system user-friendliness was not supported.
Among the significantly improved variables in the between-group comparisons, self-efficacy showed the greatest increase. This implies that the self-directed attribute of the adaptative learning was engaged, as learners took an active role in constructing their education contents (Zhou et al., 2018). High efficacy has been reported to be essential for effective BPSD care in NHs because it reduces the nursing staff’s burden and stress (Nogales-González et al., 2015; van der Lee et al., 2014). Improvements in the mental health of nursing staff who provide direct care for residents with dementia can lead to a decrease in BPSD incidence due to the staff’s more positive perception and attitude in BPSD care (Hu et al., 2022; Nogales-González et al., 2015)
The adaptive learning system in this present study significantly improved the BPSD knowledge of the nursing staff. Although there was a significant difference in the baseline BPSD knowledge level between the control and experimental groups, the post-test scores were significantly higher in the experimental group, which had experienced adaptive learning. Since part of the idea behind adaptive learning is that the learner directs it, it was implied that its active nature promotes effective increments on the knowledge. That the first course, which dealt mainly with BPSD knowledge, had the highest adaptation rate, could indicate that the knowledge level of the learners in the experimental group was improved more effectively by their ability to selectively focus on the areas in which they lacked knowledge. Many previous studies have emphasized the importance of nursing staff staying up-to-date on knowledge that affects their practice, especially those who apply that practice at the very close side of residents with dementia, reporting that it leads to a positive attitude, reduced burden, and better care ability (Hu et al., 2022; Khalil et al., 2020; D. Kim et al., 2022). Considering the direct moderate effect of self-efficacy to the knowledge improvement (Hu et al., 2022), it could be suggested that an adaptive learning-based BPSD education, which this study showed significantly increased both knowledge, and self-efficacy, is an appropriate direction for future NH education.
The significant improvement in BPSD competence after adaptive learning could support the previous finding that individually adaptive education that suits each nursing professional’s level leads to more competent practice and thus to more effective care (Taneichi & Rokkaku, 2020). Although the experimental group was significantly improved more than the control group, the web-based education without adaptive learning also had a significant positive effect on BPSD care competence. This could be explained by both programs provided to the experimental and control groups having been developed based on an identical educational framework that targets the improvement of BPSD care competence in NHs (D. Kim et al., 2022). This result supports the appropriateness and effectiveness of the framework, suggesting the importance of the specific educational framework for effective web-based educational outcomes.
From a system aspect, it was found that learners were significantly satisfied with the adaptive learning system. This is consistent with previous studies that reported learners’ high levels of satisfaction with adaptive learning (Martin et al., 2020; Rosita et al., 2016). The study participants’ comments indicate that the interactive communication via the chatbot accounted for most of the system satisfaction. As opposed to one-way web-based education without communication, interaction between the instructor and learners improves the effectiveness of web-based education (Moehead et al., 2020). Many attempts have been made to maximize the effectiveness of adaptive learning system by applying information technologies such as AI, virtual reality, and cloud computing (Rosita et al., 2016; H. Xie et al., 2019). Those technologies assist the adaptation process and facilitate learners’ concentration and engagement through improved visualization and interactive communication. Using these technologies can potentially introduce innovation in in NH education to increase its effectiveness, for example, by expanding the functions of AI chatbots that mediate interactions. Therefore, we recommend that research that follows up on this study applies additional technologies to adaptive learning BPSD education programs as a means to improve learners’ satisfaction and those programs’ effectiveness.
It should be noted that learners experienced some difficulties in using the system. Their comments indicate that the problems they experienced could be explained by the unfamiliarity of the adaptive system and limitations of the system interface. This low user-friendliness could also account for the 25% of the experiment group participants who chose not to adapt. Our system’s adaptation occurred when learners made the decision to skip educational contents based on their previous knowledge and BPSD competence. Since new techniques and algorithms are being developed, it should be possible to develop better adaptive learning systems, such as path recommendation learning methods systems (Raj & Renumol, 2024; Zhou et al., 2018). However, the results of this study are meaningful in that 75% of the participants effectively used the adaptive learning system, even though it might have been unfamiliar and difficult on their first attempts. However, to feasibly apply such a program to NHs, an easy and simple education system is needed in consideration of the advanced age of many practitioners in NHs. Accordingly, the significant cost of time and effort to develop these systems and introduce them to learners who might not be familiar with web-based learning should be considered (Cardiel et al., 2022).
This study has limitations. Due to convenience sampling and non-randomized group assignments, potential biases cannot be entirely excluded. Although baseline differences were identified and statistically controlled for, complete homogeneity between the groups might not be achievable. In addition, while the AI chatbots presented additional educational data and functioned to mediate two-way communication, there was a limit to their automatic recommendations of advanced data and answers to complex questions. If a high-performance AI chatbot were applied after repeated research and sufficient natural language learning, the effectiveness of web-based education could be further improved. Finally, the rigor of measurement may have been limited by the reliance on self-report questionnaires to evaluate BPSD care competence and system effectiveness. Self-reported data are subject to potential biases, such as social desirability bias and recall bias, which may affect response accuracy. To improve the evaluation of educational effects, developing and validating culturally and linguistically appropriate assessment tools would enhance the accuracy and reliability of educational measurements.
The necessity and importance of appropriate NH education development are being strengthened by the expected increase in the dementia population due to global aging (Riesch et al., 2018). While BPSD care is still considered the most complex task in dementia care, requiring consideration of diverse subjective frames to ensure an appropriate approach (D. Kim et al., 2024b), we have developed an innovative educational program with a new pedagogical approach that aims to maximize effectiveness and efficiency for nursing staff in NHs. By verifying the effectiveness of the framework-based educational program, this study presented a new direction for subsequent nursing education research and emphasized the need to apply updated information and communication technology to education, such as AI chatbots. In addition, we provided nursing staff with opportunities to experience learning via a non-traditional method and presented pedagogical strategies to strengthen and retain practical expertise in the context of the post-COVID-19 era and the developing science and technology society.
Conclusion
To sum up, the adaptive learning web-based BPSD educational program developed for this study improved the BPSD knowledge, competence, and self-efficacy of NH nursing staff with high satisfaction. It is suggested that more effective web-based education is possible by drawing upon a specific, concrete theoretical basis and utilizing a more advanced application of the technology. However, given the non-randomized sample, caution should be exercised when generalizing these findings beyond the study population. The positive outcomes of this study suggest that the adaptive learning is an effective strategy toward a “new normal” education for nursing staff of NHs in the post-COIVD-19 era. Future studies are suggested for extending adaptive learning in continuing education for various nursing practice contexts in ways that reflect individual characteristics and educational needs.
Footnotes
Acknowledgements
None.
Ethical Considerations
This study was approved by the Ethics Committee of Korea University (Ethics Code: KUIRB-2021-0142-01) on May 11, 2021. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
Not applicable.
Author Contributions
Study design: DK and SOC. Data collection and analysis: DK, Y-RC, Y-NL, WHP, D-YK, and SOC. Drafting the manuscript: DK and SOC. All authors read and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology [NRF-2019R1A2C1086122, NRF-2022R1A2C1004542].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are not publicly available due to individual privacy could be compromised, but are available from the corresponding author on reasonable request.