
Abstract
The review explored topical vaccination themes in literature to describe the barriers and drivers of effective COVID-19 vaccination in Ghana. We searched Scopus, Medline, Cinahl, and Google Scholar, covering papers published exclusively in Ghana between December 2019 and January 2023. Using predefined inclusion and exclusion criteria, 27 papers were included in the review. We adopted the 5As taxonomy to organize the papers into five dimensions, namely, Access, Affordability, Awareness, Acceptance, and Activation. Our analysis shows that Acceptance was the most frequently research theme (n = 23, 85.1%), followed by Awareness (n = 19, 70.4%), Activation (n = 14, 52%), Access (n = 7, 25.7%), and Affordability (n = 6, 22.2%). Further, we found awareness campaign messages to be largely concentrated in Accra, Kumasi and other hotspots. Further studies on vaccine financing, access and inclusion of individuals and families in information dissemination campaigns is highly recommended.
Plain language summary
According to the World Health Organization, vaccination is the safest way to curb the spread of COVID-19. Yet, weak governance and health system infrastructures in low and middle-income countries, coupled with burdening socioeconomic effects of the pandemic, had crippled vaccine programs in LMICs. Accordingly, this national-level scoping review sets to understand the topical COVID-19 vaccination themes explored in literature, to identify the barriers and drivers of vaccination in Ghana. We searched Scopus, Medline, Cinahl, and Google Scholar, covering papers published exclusively in Ghana between December 2019 and January 2023. Using predefined inclusion and exclusion criteria, 27 papers were included in the review. We adopted the 5As taxonomy to organize the papers into 5 dimensions: Access, Affordability, Awareness, Acceptance and Activation. Our analysis shows that Acceptance was the most frequently research theme (n = 23, 85.1%), followed by Awareness (n = 19, 70.4%), Activation (n = 14, 52%), Access (n = 7, 25.7%), and Affordability (n = 6, 22.2%). Aside from the limited publications identified on cost and access, we found that albeit awareness campaign was widespread, the campaign messages were largely concentrated in Accra, Kumasi and other hotspots. Additionally, approaches required to engender peer-to-peer education toward vaccine uptake among Ghanaians was absent. Consequently, further studies on vaccine financing, vaccine access, and awareness creation through community leadership is highly recommended. The high concentration of records on Acceptance, Awareness and Activation in this study indicates the need for government to pay attention to these areas to ensure effectiveness and efficiency in future vaccination exercises.
Introduction
By January 31, 2023, the world recorded 754,367,807 COVID-19 infections, with over 6,825,461 deaths and millions of businesses lost (World Health Organization [WHO], 2023). The high fatality and hospitalization rates prompted the rapid development of vaccines to contain the virus (Dinleyici et al., 2021; WHO, 2021a).
During the last quarter of 2020, various vaccines, such as Pfizer-BioNTech, Moderna, AstraZeneca, Sinovac, COVAX, and Johnson and Johnson, among others, were developed (WHO, 2021b). However, cost limited access to the vaccines, and countries’ vaccine procurement aligned with their financial capacity (Green and Loualiche, 2021). As of December 1, 2020, a jab of mRNA-1273 (Moderna) was selling for $37, Coronavac (Sinovac) for $30, BNT162b2 (Pfizer & BioNTech) for $20, Gam-COVID-Vac Sputnik V at $10, JNJ-78436735 (Johnson & Johnson) for $10, and ChAdOx1 nCoV-2019 (AstraZeneca) for $4, among others (Statista, 2020, December 1). Estimates from December 2020 indicate that while direct purchase agreements allowed high-income countries to order close to$4 billion worth COVID-19 vaccines, Low and Middle-Income Countries (LMICs) could buy confirmed doses worth only$2.7 billion (Burgess et al., 2021). For instance, before their development, the United States had already ordered Pfizer vaccines worth $1.95 billion totaling 500 million doses, and an additional 300 million doses of Moderna COVID-19 vaccines (Ofori et al., 2023; U.S. Department of Health and Human Services, Public Health Emergency, 2020).On the contrary, due to their limited financial capacity, LMICs relied heavily on the COVAX ACT Accelerator agreement which covered only 20% of their total vaccination needs (Burgess et al., 2021). Economic recessions during the pandemic and unprepared health systems in LMICs hindered the acquisition of vaccines resulting in low vaccination coverage in these countries (Afrifa-Anane et al., 2022). For instance, while the United Arab Emirates and Portugal achieved over 90% COVID-19 vaccination coverage in 2022, Yemen, Haiti, and the Democratic Republic of Congo recorded below 2% (Lupu and Tiganasu, 2023).
Ghana’s COVID-19 vaccination experience mirrored that of other LMICs (Yawson et al., 2017). The country has historically relied on donations to fulfill its vaccination needs. Between 2014 and 2019, for instance, Ghana received a total of USD $18,059,296 from the GAVI Alliance (2019) in support of its immunization programs. Following a declining domestic health expenditure of 1.38% as a share of its Gross Domestic Product (GDP) in 2019, vaccine financing remained a significant drawback to Ghana’s COVID-19 immunization efforts (Statista, 2023). The National Budgetary Statement on March 12, 2021, revealed a government revenue deficit of GH¢13.6 billion (USD $2,361,111,111), with unplanned expenditures around GH¢11.7 billion (USD $2,031,250,000) (where US$1.00 = GH¢5.76) (Ministry of Finance [MoF], 2021). Furthermore, the Ministry of Finance’s March 2, 2021 budget statement indicated a 4.9% shrink in the country’s economy since 2020 when the first COVID-19 infection was recorded in the country (Bukari et al., 2021; MoF, 2021). Consequently, like many LMICs, Ghana pinned her hopes on donations for its COVID-19 vaccination needs, and in 2021 became the first African country to receive COVAX vaccines (The United Nations Children’s Fund [UNICEF], 2021; WHO, 2021c). On February 24th, 2021, the President received 600,000 COVAX vaccines, aiming to eventually vaccinate 20 million Ghanaians (GAVI Alliance, 2021; WHO, 2021c). However, facing insufficient supplies from GAVI due to the overwhelming impact of the Indian Delta Plus variant, the government of Ghana shifted attention to bilateral and multilateral donor support from Russia, China, European Union, African Union and the United States, among others, to meet its vaccination needs. By January 30, 2023, Ghana administered 23,226,767 vaccine doses to 40.8% of the country’s 31 million people, with around 3,580,565 individuals receiving at least one booster dose (Ghana Health Service, 2023).
Although many applauded the 40.8% vaccine coverage as an improvement over Africa’s continental average of 15% (World Health Organization, 2022), it remained considerably low compared to richer countries like Palau (115.29%), Malta (108.40%), and Brunei (108.04%), among others, which recorded vaccination rates above the global average (John Hopkins University, 2023). Critics of Ghana’s vaccination coverage attributed the country’ performance to many factors. According to Botwe et al. (2022), misconceptions of the adverse effects of vaccines on reproductive health, coupled with the unprepared emergency response system of Ghana’s health system, were responsible for the low vaccine coverage (Lamptey et al., 2021). In addition, Forkuo et al. (2022), attributed Ghana’s ineffective vaccination efforts to misinformation (54.8%) about the vaccine’s efficacy. Out of 382 respondents investigated, about 47.98% believed that vaccines are dangerous (Forkuo et al., 2022), and another 23.98% thought it could worsen allergic reactions. Similarly, Awuni et al. (2022) observed that mistrust for vaccines had negatively influenced intentions to receive COVID-19 vaccines in Ghana. Aside from misconception and mistrust, Afrifa-Anane et al. (2022) noted managerial lapses such as long queues at vaccination centers, misconception, and vaccines shortages undermining what could have been a smoother COVID-19 vaccination campaign in Ghana.
To strengthen Ghana’s public health response system to effectively address potential disease outbreaks in the future, a critical analysis of the barriers and drivers of her COVID-19 vaccination exercise using the 5A Taxonomy is timely.
Thomson’s 5A Taxonomy
The 5A model is a framework for diagnosing the determinants of vaccination coverage and implications for health policy in specific contexts (Thomson et al., 2016). The framework examines complex bio-psychosocial, organizational, and structural determinants of vaccine coverage under five dimensions: Access, Affordability, Awareness, Acceptability, and Activation. Access removes barriers to vaccination, enabling individuals to reach or be reached by vaccines. Affordability connotes the time and money expended by individuals to receive vaccines. Awareness measures people’s knowledge of vaccine benefits and risks. Acceptance assesses the willingness to receive vaccines. Finally, Activation explains the structural preparedness of health systems, and the regularity of reminders to individuals, families, and communities to vaccinate.
The 5A taxonomy is widely adopted in literature. In Crawshaw et al. (2022), the model was used to describe vaccine uptake and hesitancy among migrant populations in Europe. Reviewing 67 records from 16 countries, the paper highlighted access and acceptance as key determinants of COVID-19 vaccine coverage. Similarly, Newman et al. (2022) used the 5A and 5C models to evaluate COVID-19 vaccine hesitancy among marginalized populations in the USA and Canada and observed that 5A has advantages in explaining structural hinderances to vaccine access, including location, time, cost, trust, individual attitude, health beliefs and contact with health systems, among others (Newman et al., 2022).
In Africa, however, the adoption of 5A taxonomy in literature is scarce. A preliminary literature search on Google Scholar database over the past 10 years generated a total of three (3) papers (Kalu et al., 2022; Nyasa et al., 2023; Thomson et al., 2016). Kalu et al. (2022) used 5A taxonomy to conduct a mapping review on COVID-19 vaccine uptake among adults in 33 countries in African countries. The finding of the review of 68 papers found Acceptance to be a principal determinant of vaccination coverage, with minimal influence from Activation. They recommended further studies on the impact of activation. A few limitations were noted in the paper. Most notable was that the review was completed using articles published between 2020 and 2021, and at a time when COVID-19 vaccines were newly developed and deployed. In other words, since the greater part of COVID-19 vaccination occurred between late 2021 and 2023, this constraint affected the number of empirical studies the review could generate on COVID-19 vaccination, and the comprehensiveness of the investigations. In Nyasa et al. (2023), the authors adopted the model to explain health workers’ reaction to hepatitis B vaccines in Zambia and found that although the vaccines were Affordable and Accessible to most of the research participants, Awareness of the vaccines was low. They saw the absence r late dissemination of regular notifications (Awareness) for vaccine update to be a major hinderance to Activation. Finally, in a narrative review on the determinants of vaccine uptake using the 5A taxonomy, Thomson et al. (2016) found all the five (5) dimensions to have a notable effect on vaccine uptake. However, they highlighted the significance of the location of vaccination centers, knowledge, perceived safety, past behavior, and the regularity of reminders as imperatives for vaccine uptake. Moreover, majority of African literature adopting the 5A taxonomy targeted multiple countries. This makes it difficult to estimate the actual immunization gaps in individual countries.
In view of these, the review of empirical records on COVID-19 vaccination in specific African countries to inform public health policies is vital.
Methods
Levac et al. (2010) six steps framework for scoping review was employed for this review. These include identifying research questions and linking them to the research purpose; generating literature by comparing the study’s feasibility against its breadth and comprehensiveness; using iterative team approaches to screen selections and extract data; chart data to show the numerical summary and themes generated; collate, summarize and report the result; and as an optional step, consult to confirm the findings.
Eligibility Criteria
We searched for empirical records on COVID-19 vaccination in Ghana. Only studies conducted originally in the English language and published in peer-reviewed journals were selected. Again, quantitative, qualitative, and mixed-method studies were considered. However, to meet the inclusion criteria, they must be empirical papers conducted between December 1st 2019 and 3rd January 2023.

Source. Authors’ conception.
Search Strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews (Tricco et al., 2018). As outlined in the standard Joanna Briggs Institute (JBI) systematic review method, we used the following step to search for papers. First, we performed a limited search in the Medline database. The articles we generated were analyzed in Microsoft Excel® (version 2016) to identify keywords and index terms in the titles and abstracts. We then had a discussion on what to include in the final search terms. The outcome of this discussion was further discussed with a public health expert to validate the decision and advise us. Forward, we conducted a full search on the selected databases and used Mendeley Reference Manager (Version 1.19.8) and Microsoft Excel® (2016) sheets to manage the articles generated. Consistent with Webster et al. (2017), we did not consider grey literature for this critical scoping review.
After the review of preliminary literature and consultation with the public health expert, Scopus, Medline, Google Scholar, and Cinahl, databases were searched for relevant articles.
PICO Framework
The study adopted Thomson et al. (2016) definition of the dimensions of 5A taxonomy. Accordingly, Access indicates the removal of barriers to vaccination to ensure that every individual could reach or be reached by COVID-19 vaccines. Affordability denotes the time and money required by households and individuals to take up vaccines. We defined Awareness as the level of knowledge individuals have on the benefits and risks of vaccination. Activation is the readiness of health systems, and strategies adopted to engage individuals, families, and communities to vaccinate. Finally, Acceptance examines the willingness to receive vaccines.
Search String
-
-
-
-
Study Selection and Data Extraction
We designed a standardized extraction form based on PRISMA guidelines for the review. Search and screening was carried out by LY and AHNK with guidance from GAA. The search results were imported into Mendeley Reference Manager (version 1.19.8) and screened at three levels. First, we screened the titles, language, and dates of publication. To be included in the review, the title must contain the terms “SARS-Cov-2 or COVID-19 or vaccination or vaccine.” Further, only articles originally published in English language between December 2019 and January 2023 were selected. Next, we screened the abstracts to establish their relevance by types of research papers, geolocation and the research methodology used. We selected only empirical studies conducted in Ghana. Finally, a full text review was conducted to determine completeness, and eligibility to be included in the final list. In addition to extracting records based on relevant themes, the extracted materials were also scrutinized against the quality of information presented. At any point where the two authors could not agree on the decisions to exclude or include a paper, the views of GAA, a Health Service Administrator and Public Health expert, were sought.
Data Summary
Our combined search from the selected databases generated 1,844 papers. Using authors’ names and titles of papers, 134 duplicates were detected and deleted. Together with the title screening, language screening and screening for completeness, an additional 1,060 irrelevant records were deleted. Abstract screening was conducted to determine: (i) the appropriateness of the research population, (ii) method used, and (iii) ensure that the studies were conducted empirically. This led to the deletion of an extra 511 papers. Finally, a full-text screening of 139 records was conducted. From this, we found 27 papers to be eligible for inclusion in the final analyses (Figure 1). The University of Ghana Library System granted access to the databases.

Summary of literature search.
Quality Appraisal and Ethical Considerations
Given that a scoping review is primarily focused on comprehensiveness rather than the quality of the individual papers, the included records were only assessed for their relevance (Brien et al., 2010; Pham et al., 2014).
To avoid publication bias, a well-defined eligibility criteria was used to identify the records, and justifications for the inclusion of records presented and approved before the records were included. In addition, to ensure research integrity, the authors engaged a public health expert to advise them during disagreements.
Collating Results
We adopted Thomson et al. (2016) 5A taxonomy to synthesize the articles under five themes. These include Access, Affordability, Awareness, Acceptance, and Activation (Thomson et al., 2016, p. 1019) (Table 3).
Analysis
LY and HNKA undertook analysis of records. Mendeley reference manager and Microsoft Excel (2016) were used to prepare a literature summary table under relevant themes, namely, authors, year of publication, scope of the study, sector, study objectives, method, research design, sample size (Table 1), title, results, drivers of vaccination and barriers of vaccination (Table 2). The papers were compared against their contents and thematized in line with the 5A model and the research objective. We used narrative review for this paper.
Authors, year of publication, scope, sector, type of study, method, and design.

Factors associated with Ghana’s COVID-19 vaccination exercise.

Results
Each of the 27 research papers included in this review was carried out exclusively in Ghana (Table 1). On the research methodology adopted, we found that majority of the records 23 (85.2%) used quantitative research methodology, 2 (7.4%) employed qualitative methodology, and 2 (7.4%) used mixed-research methodology (Figure 2). On the research designs used, majority (n = 22, 81.5%) employed cross-sectional design. The rest include 1 Sequential mixed method design, 1 Descriptive study, 1 QIMS study, 1 Age-stratified model, and 1 CVIC design (Figure 3). In addition, majority of the articles were published in 2022 (n = 15), followed by those published in 2021 (n = 10) and the publications in 2023 (n = 2) (Figure 4). We found most of the articles (n = 14) to be focused on Public Health issues (Figure 5). The remaining 15 were focused on Health communication (n = 3), Radiography (n = 1), Clinical Care (n = 2), Health Financing (n = 2), Health Human Resource (n = 2), and Health Systems Policy (n = 3) (Figure 4). On the scope of the studies, 4% were facility based, 15% were focused on the administrative regions of Ghana, and 81% on the entire country (Figure 6). When mapped against the 5A model, we found only one paper exclusively on Acceptance. Thus each of the remaining 26, (96.3%) articles was focused on multiple dimensions of the model. Specifically, seven articles (25.7%) were related to Access, 6 (22.2%) Affordability, 19 (70.4%) Awareness, 23 (85.1%) Acceptance, and 14 (52%) Activation (Table 3; Figure 7). We presented the summary report for records included in this review in Table 2.

Method.
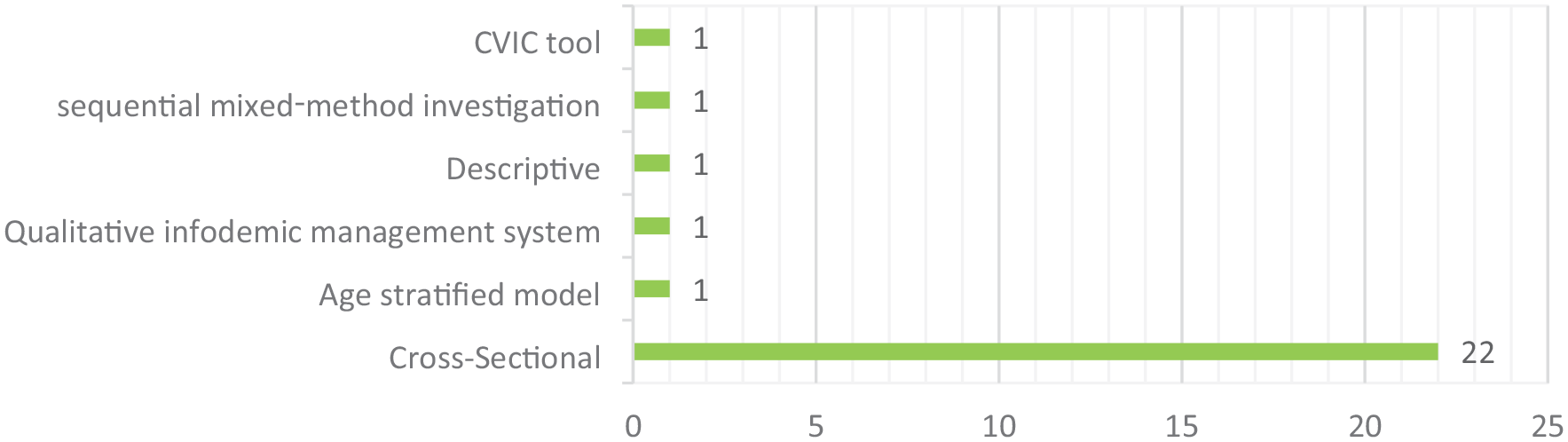
Research design.

Year of publication.

Sector.

Scope.
Thomson’s 5As Model.


5A dimensions.
Discussion
The 5A taxonomy is a widely accepted framework for analyzing vaccination coverage (Nyasa et al., 2023; Thomson et al., 2016). In this review, Thomson et al. (2016) 5A taxonomy was adopted to examine empirical literature on COVID-19 vaccination in Ghana. The articles were mapped against five dimensions of the framework to determine gaps in the country’s vaccination coverage. The dimensions include Access, Affordability, Awareness, Acceptance, and Activation. From the mapping, we observed that majority of the dimensions overlapped. For instance, articles mapped against Acceptance also assessed Awareness. Similarly, articles assessing Access also measured Affordability.
Acceptance
We found that Acceptance is significantly associated with vaccination coverage in Ghana. Aligned with the narrative review by Thomson et al. (2016), Acceptance emerged the most significant factor influencing vaccination coverage in Ghana. From the records, 23 (85.2%) articles were centered on COVID-19 vaccine Acceptance in Ghana. Aside from their areas of concentration, we analyzed the findings presented in each article and found that the majority reported high vaccine acceptance rates in Ghana. On Table 2, the records show that between 39.3% and 82.6% of study participants were willing to accept COVID-19 vaccines in Ghana. However, the degree of acceptance is influenced by several factors. Some of these include the present health conditions, prior exposure to COVID-19 virus, and societal influencers, among others (Acheampong et al., 2021; Addo et al., 2021; Agyekum et al., 2021; Amo-Adjei et al., 2022). Acceptance increased among persons with chronic illnesses (Acheampong et al., 2021), individuals infected with COVID-19 (Agyekum et al., 2021), and those influenced by prominent political personalities (Asumah et al., 2022; Lohiniva et al., 2022; Thomson et al., 2016). Additionally, willingness to accept COVID-19 vaccines was high when people are well-informed about their benefits, safety, and associated risks (Adjaottor et al., 2022; Adomako et al., 2021; Agyekum et al., 2021; Kyei-Arthur et al., 2022). As vaccine acceptance is the determinant of herd immunity (Malik et al., 2020) and potentially the most significant indicator for success (Kalu et al., 2022), its not surprising that our review found most of the records to be focused on vaccine acceptance. However, instead of exploring the experiences of research participants, from the research methodologies analyzed, we found majority of these papers to be merely interested in the rates of vaccine acceptance. From the records, 22 out of 23 articles employed quantitative research methodology, and many of them utilizing multiple-item Likert scales (Acheampong et al., 2021; Addo et al., 2021; Adjaottor et al., 2022).
Again, although high acceptance rates were observed among particular populations, including healthcare workers and teachers, the national data shows a low coverage rates in comparison with advanced countries. COVID-19 vaccination uptake in high-income countries generally showcased higher rates of vaccine acceptance, often exceeding the global average in some regions (John Hopkins University, 2023). This is largely because advanced nations implemented robust and extensive vaccination programs, leading to increased awareness and confidence in the vaccines offered (Awuni et al., 2022). Countries such as the USA and UK had invested substantially into education and awareness creation, expanded access to healthcare, and built trust in government policies and healthcare institutions (Deb et al., 2023). In contrast, our review revealed the lack of structural and policy preparedness in Ghana to respond to the pandemic (Kyei-Arthur et al., 2022; Ofori et al., 2023).
In summary, while the factors influencing acceptance are well documented in literature, there remains a need for more comprehensive studies elucidating strategies to enhance vaccine acceptance in Ghana. Additionally, the reliance on quantitative methods warrants exploration into qualitative approaches to provide deeper insights into the nuances of vaccine acceptance among Ghana’s populace. Further research could adopt qualitative research designs to explore interventions targeting these factors to bolster acceptance rates and inform robust vaccination strategies.
Awareness
Out of 23 articles concerned with Acceptance, 17 were connected with Awareness. Authors, including Zhou et al. (2022), Okai and Abekah-Nkrumah (2022), Boi-Dsane et al. (2023), Kyei-Arthur et al., 2022, and Lohiniva et al. (2022) argued that adequate knowledge of the benefits and risks of vaccination is an indispensable requirement for enhanced vaccination coverage in Ghana. Analyses of these records show high prevalence of misinformation, misconception, and ignorance with associated high vaccine hesitancy in Ghana (Twum et al., 2021; Kyei-Arthur et al., 2022; Yeboah et al., 2021; Zhou et al., 2022). For instance, Okai and Abekah-Nkrumah (2022) noted Ghanaians’ concerns about potential risks of vaccine uptake to their reproductive health. Similarly, some Ghanaians expressed fear of vaccines from Western countries, suspecting them of being designed to harm the black race and older persons (Boi-Dsane et al., 2023). Lohiniva et al. (2022) recounted an incident where a local Premier League football coach attributed his team’s loss to players’ weakened physical condition post COVID-19 vaccination; illustrating the limited understanding many Ghanaians had regarding vaccine benefits and risks. Similarly, Zhou et al. (2022) highlighted that exposure to misleading public communications via media platforms heightened vaccine hesitancy among Ghanaians. It is important to mention, however, that although records from our review supported this finding, contrasting these findings with COVID-19 vaccination statistics from high-income countries reveals a stark divergence in the factors influencing hesitancy. While misinformation and misconceptions play a role globally, the specific concerns regarding the origin and intent of vaccines seem more prevalent in the Ghanaian context compared to high-income countries (Agyekum et al., 2021; Alhassan et al., 2021). Additionally, the impact of influential figures attributing sports outcomes to vaccination effects is not a commonly reported issue in high-income countries.
On the other hand, Yeboah et al. (2021) challenged the notion that greater vaccine knowledge directly translates to increased vaccine uptake. Analyzing 1,560 respondents, they discovered that although over 69.9% were well-informed about vaccine benefits and risks, only 31% were willing to be vaccinated. They argue that extensive knowledge doesn’t necessarily result in compliance with preventive measures. Yeboah et al. (2021) admitted, however, that social media and informal relationships are major influencers of vaccination choices, with 93.6% of willing respondents being influenced by recommendations from friends and family. Thus, the paper observed that instead of focusing resources on the types of information communicated, policy makers should rather pay attention to the medium or channel of communication. However, the dominance of social networks in influencing vaccination decisions appears to be more pronounced in Ghana than in high-income countries, where factors like trust in institutions and access to healthcare might play a more significant role. In addition, the recommendation to center attention on communication mediums rather than specific information types warrants further investigation (Yeboah et al., 2021). While this approach might be relevant in Ghana, it might not fully align with the dynamics in high-income countries where a blend of targeted information and credible sources might play a more critical role in vaccination promotion strategies.
In summary, we are of the view that tailoring communication strategies to suit specific cultural contexts remains crucial, but further research on a blended approach to increase Awareness is necessary to inform vaccination policies in Ghana and other contexts.
Access
Although health systems in LMICs are largely constrained by infrastructure and institutional structures, our review identified only seven papers related to Access dimension with divergent opinions on the phenomenon.
Some of the records reported a positive correlation between selected workplaces and professionals and enhanced vaccine Access (Agyekum et al., 2021; Amo-Adjei et al., 2022; Serwaa, et al., 2021). According to Amo-Adjei et al. (2022) and Agyekum et al. (2021), Ghana’s initial vaccine distribution targeted critical patients, the elderly, and frontline workers such as healthcare professionals, security forces, and policymakers (Alhassan et al., 2021, 2022; Aram et al., 2021; Serwaa, et al., 2021). This prioritization minimized travel distances for these groups, provided firsthand vaccine information, and reduced inconveniences during vaccination, potentially fostering higher acceptance. Affordability thus emerged as a significant factor intertwined with access.
In a contrary view, other findings revealed critical structural factors which barred Ghanaians from reaching or being reached by COVID-19 vaccines. Some of these include distance from immunization centers, place of residence, place of work, inequities on vaccine distribution, and vaccine shortages, among others. For instance, in their examination of facilitators and barriers to COVID-19 vaccine uptake among women in two regions of Ghana, Afrifa-Anane et al. (2022) observed that participants could not vaccinate because of long queues at vaccination centers and shortage of vaccines. Queueing and vaccine shortages was particularly frequent when the initial 600,000 jabs were received from the COVAX facility (Afrifa-Anane et al., 2022; Alhassan et al., 2022) and the fear of contracting the disease or dying resulted in a rush for the vaccines. Due to the waiting time required to receive the jabs, many full-time employees were not vaccinated during the initial phase of the rollout.
In comparison with data in high-income countries, we observed stack disparities in resource allocation, distribution strategies, and prioritization. In the US and other high-income countries, equitable distribution was attained due to robust infrastructure, proactive dissemination strategies, and adequate vaccine supply policies (Amponsa-Achiano et al., 2022; Deb et al., 2023; Dubik, 2022). Again, contrary to LMICs where shortages and distance hindered access, high-income countries achieved a broader vaccine accessibility (Dubik, 2022).
The contrast between LMICs and high-income countries underscores the impact of structural inequalities on vaccine accessibility (Ofori, et al., 2023). While high-income nations demonstrated a more systematic approach, LMICs grappled with multifaceted challenges. Addressing these disparities demands a comprehensive approach, considering not only vaccine availability but also equitable distribution strategies, infrastructure improvements, and targeted interventions to mitigate accessibility barriers in LMICs.
Affordability
Affordability describes the monetary and non-monetary expenses related to obtaining COVID-19 vaccines (Thomson et al., 2016). Our findings indicate a close link between affordability and vaccine accessibility with significant effects at the national and household levels (Kalu et al., 2022).
On a national scale, findings from our records show that despite Ghana receiving multiple doses of COVID-19 vaccines from initiatives like COVAX and through bilateral relations with the United States and the European Union, supply was insufficient to cover the entire population. This shortage stemmed from the nation’s economic downturn when the pandemic struck, hindering the government’s ability to procure the remaining doses. As a result, there was a scarcity of vaccines, limited vaccination centers, and subsequently, reduced access to vaccination (Kalu et al., 2022).
At the individual level, our data reveals a strong association between coverage and vaccine affordability. Household cost elements included service fees, transportation expenses to vaccination sites, and the time invested in waiting for vaccines (Thomson et al., 2016). Alhassan et al. (2021) conducted a study involving 1,556 individuals and found that those residing outside Accra, the capital city, were unwilling to bear the cost of transportation to vaccination centers. This reluctance was likely because populations living outside Accra and other major cities in Ghana fall within the extremely poor category and unlikely to afford the transportation costs associated with receiving the jabs (Alhassan et al., 2021; Amo-Adjei et al., 2022). Furthermore, the long waiting time at vaccination centers acting as a deterrent for workers, especially casual workers and full-time employees (Afrifa-Anane et al., 2022; Thomson et al., 2016). Coupled with limited awareness of the benefits and risks of COVID-19 vaccines outside major cities, it is expected that many households would lack the motivation spend their time and savings on vaccination.
Comparatively, in advanced countries, accessibility to COVID-19 vaccines tends to be more widespread due to robust healthcare infrastructure and greater financial resources. Affordability barriers are less pronounced, often mitigated through government-funded vaccination programs that prioritize free or low-cost inoculations for the entire population (Amponsa-Achiano et al., 2021; Dubik, 2022; Nonvignon et al., 2022). Moreover, higher awareness levels and better dissemination of information contribute to increased vaccine uptake, minimizing reluctance among individuals and reducing the impact of long waiting times at vaccination sites (Alhassan et al., 2022).
Critically assessing the disparities between high-income countries and regions like Ghana highlights the significant impact of economic constraints on vaccine accessibility. While affluent nations can navigate affordability barriers and ensure comprehensive coverage, lower-income settings face substantial hurdles due to limited resources, ultimately affecting vaccine distribution and uptake. Addressing these disparities demands tailored strategies that account for the economic realities and informational needs of diverse populations.
Activation
Activation is the structural preparedness of health systems, and the effectiveness of reminders for vaccination. We identified fourteen papers showing a push toward both preventive measures and COVID-19 vaccination. For instance, Kalu et al. (2022) and Yeboah et al. (2021) reported that early in the pandemic, emergency strategies and media campaigns, including contact tracing, community address systems for hand hygiene education, hand sanitizers, masking, lockdowns, and social distancing protocols, were implemented to curb community infections and deaths. However, as vaccines became available in greater numbers, emphasis was centered on vaccination awareness campaigns. Media campaigns during the pandemic’s early stages played a crucial role in correcting misconceptions and promoting adherence to preventive protocols (Adomako et al., 2021). The media facilitated a strong connection and trust in government-provided information, and compliance with preventive measures. Adomako et al. (2021) documented that these preventive measures were largely successful, especially given the initial ineffectiveness of traditional treatment approaches. Agyekum et al. (2021) reported that 42.3% of respondents trusting government information, for instance, expressed willingness to take the vaccines. Similarly, Addo et al. (2021) found that health personnel engagement increased vaccine acceptance, emphasizing the role of close interactions in reducing hesitancy among health workers. Despite its significance, our records indicate inadequacy in the media awareness campaign (Acheampong et al., 2021). In their study on vaccine hesitancy in Sub-Saharan Africa, Acheampong et al. (2021) revealed that 53% of 2,345 Ghanaian adults surveyed were not well-informed about the vaccines. This lack of information led to 61% expressing doubts about the clinical safety of the vaccines and 35% having doubts about their effectiveness. Addressing this gap in information is vital to overcoming vaccine hesitancy and ensuring widespread acceptance of COVID-19 vaccines in diverse regions.
This contrasts with developed countries where comprehensive communication strategies contribute to higher public awareness and understanding of vaccination efforts. Media campaigns, contact tracing, and community education played a pivotal role in shaping public perception and adherence to safety protocols in countries that recorded high vaccination coverage (Lohiniva et al., 2022; Zhou et al., 2022).
In summary, Activation underscored the importance of early and effective communication strategies, especially in regions with limited information access. However, comparing data on Activation in Ghana with developed countries emphasize the need for tailored approaches to promote public trust. Future efforts should prioritize targeted media campaigns and health personnel engagement to ensure widespread understanding and acceptance of COVID-19 vaccines, contributing to global public health initiatives.
Limitations
The review has some limitations. While our review had successfully assessed operational strategies used to roll out the Ghana’s COVID-19 vaccine program, the 5A taxonomy was inadequate in accessing the role of enablers within family units. Some of these enablers include age, gender, rural-urban divides, and other interpersonal relationships which could affect vaccination decisions. While this omission does not take away the relevance of our findings to public health policies in Ghana, we recommend that further research is done in this area to inform the message that media organizations can communicate to the public during a pandemic. Additionally, since our review was focused exclusively on peer-reviewed empirical papers published in English, we are likely to miss out on other information published in editorials, commentaries, and newspaper publications, among others. In the same vein, since many national journals in Africa are not indexed in the databases we used for this research, we could miss useful information contained in papers published in such journals. Finally, we did not consult with stakeholders to validate our research findings. However, since this process can greatly enhance the quality of the review, we recommend users of our findings to, as much as possible seek additional interpretations from the relevant experts.
Conclusion
There is a plethora of publications on COVID-19 vaccination using different models which are sometimes overlapping. Our work harmonizes all these articles using the 5A taxonomy to scientifically regroup and classify these articles to advise policy makers to enact evidence-informed policies and programs to address the gaps identified. Regarding research gaps, our findings recommend further empirical investigations on vaccine financing (Affordability) and access constrains in Ghana. With many disease outbreaks in Africa, including Ebola, Measles, Hepatitis B and other childhood diseases, vaccination would remain a health policy choice for African nations for many years. The best way to enhance the effectiveness (Acceptance) of vaccination on the continent is to engage in continuous scientific assessment of the strategies (Activation) governments and health entrepreneurs adopt to make the jabs available to those who need it, and the results they produce.
Footnotes
Acknowledgements
I sincerely appreciate the support of the team at the Catholic Health Service Trust-Ghana (CHST) and the Health Policy and Management class of the University of Ghana Business School (UGBS).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This is not applicable.
Data Availability Statement
The data underlying this study, including the literature search records, study selection process, and all data supporting the findings of this review are included in the article.