
Abstract
As dementia is becoming a great challenge worldwide, modifying its risk factors is a primary preventive approach. However, there is a scarcity of integrated efforts to determine dementia-specific factors that influence preventive behaviors, particularly when considering a theoretical framework. Therefore, this scoping review aimed to map the evidence on factors affecting dementia-preventive behaviors based on the PRECEDE framework. Five electronic databases—PubMed, PsycINFO, CINAHL, EMBASE, and Cochrane CENTRAL—were searched for articles published until May 2022, and only peer-reviewed studies were included to gather robust evidence. During the initial search, 37,331 articles were retrieved. Of these, 22 articles met the inclusion criteria and were included in the evidence synthesis. The scoping review identified 28 specific determinants within the six conceptual categories of the PRECEDE framework, thereby highlighting the multi-dimensional nature of factors influencing dementia-preventive behaviors. Future studies should consider multilevel and multi-dimensional personalized strategies to promote dementia-preventive behavior.
Plain Language Summary
Our study focused on understanding the factors that influence dementia-preventive behaviors. We aimed to identify these factors using a theoretical framework called PRECEDE, which could guide future preventive strategies. To gather reliable evidence, we conducted a scoping review by searching five electronic databases for peer-reviewed articles published until May 2022. After a thorough search, we analyzed 22 articles that met our inclusion criteria. Through our review, we identified twenty-eight specific factors within six conceptual categories of the PRECEDE framework that affect dementia-preventive behaviors. This finding emphasizes the complex and multi-dimensional nature of these factors and their impact on dementia preventive efforts. Our study’s findings have important implications for promoting dementia prevention. To be effective, future preventive strategies should consider personalized approaches that target multiple levels and dimensions, addressing the diverse factors influencing individuals’ behaviors. We acknowledge some limitations in our study. We focused on individual-level factors and did not explore administrative and policy aspects that could also influence dementia prevention. Additionally, the majority of the included studies were conducted in Asian countries, potentially limiting the generalizability of our findings to other cultural contexts. Further research should consider these aspects for a more comprehensive understanding of dementia prevention. In conclusion, our study contributes valuable insights to dementia prevention efforts. By addressing the identified factors, healthcare professionals and policymakers can design more effective interventions to protect cognitive health and enhance the overall well-being of individuals at risk of dementia.
Introduction
With an increase in the aging population and changes in the demographic structure worldwide, the prevalence of dementia is also increasing. In 2019, the number of people living with dementia worldwide was estimated at 57.4 million, and this figure is expected to reach 83.2 million and 152.8 million by 2030 and 2050, respectively (Nichols et al., 2022).
Dementia is one of the greatest challenges for the public health and social care system because it imposes a burden on both individuals and society. People living with dementia may experience not only difficulties in all activities of daily living (Mograbi et al., 2018; Prince et al., 2015), but also worsened perceived dignity and quality of life (Kisvetrová et al., 2021). With greater challenges in meeting basic personal needs as the illness progresses, caregivers’ and families’ physical, mental, and social health can deteriorate, thereby overwhelming their lives (World Health Organization, 2021). Additionally, the cost of direct and indirect medical and social care, including informal care costs, will inevitably increase for dementia (World Health Organization, 2021).
Regarding the impact of dementia, a growing body of evidence highlights the importance of delaying the onset of or preventing dementia by modifying its risk factors. The 2020 Lancet Commission has identified 12 risk factors that could be managed to prevent or delay the onset of dementia: low education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, low social contact, excessive alcohol consumption, traumatic brain injury, and air pollution (Livingston et al., 2020). In addition, there is a consensus that multifaceted behavioral modification may be key to reducing the incidence of dementia (Siette et al., 2022).
Currently, healthcare providers are responsible for developing strategies to put dementia-preventive behaviors into practice. However, to establish evidence-based strategies, the determinants of dementia-preventive behaviors must be systematically identified and integrated on the basis of a theoretical framework. The PRECEDE–PROCEED framework (Green & Kreuter, 2005) is a practical theoretical framework for conducting intervention studies on health behavior change. The PRECEDE framework consists of four evaluation phases—social assessment; epidemiological, behavioral, and environmental assessment; educational and ecological assessment; administrative and policy assessment—that precede the intervention planning stage to prioritize modifiable targets. As the PRECEDE framework encompasses diverse theoretical frameworks and multi-level determinants (community, interpersonal, and individual levels), it is useful for systematically synthesizing evidence from several studies (Gielen et al., 2008). Accordingly, this approach would allow us to clarify what we know and what the priorities are for subsequent research.
Scoping reviews are useful for mapping emerging evidence from disciplines to bridge the gap between evidence and practice (Peters et al., 2015). Therefore, by adopting this approach, we aimed to determine the status of existing studies on dementia-preventive behaviors and provide a comprehensive understanding of the factors influencing dementia-preventive behaviors.
Methods
This review was guided by the five-stage methodological framework by Arksey and O’Malley (2005) and recommendations by Levac et al. (2010). The five stages comprise identifying the research question; identifying relevant studies; selecting studies; charting the data; and collating, summarizing, and reporting results (Arksey & O’Malley, 2005).
Stage 1: Identifying the Research Question and Determining the Inclusion and Exclusion Criteria
Although scoping reviews may include diverse sources, including gray literature or other sources that have not been formally published, the current study included only peer-reviewed studies to ensure the credibility of the evidence. To provide the most up-to-date and relevant evidence, we chose articles up until the point to search. Additionally, to ensure comprehensive coverage and to avoid language bias by selecting a single language, we considered articles in both English and Korean languages. The final inclusion and exclusion criteria were as follows:
The inclusion criteria:
(1) Articles published in peer-reviewed journals focused on dementia-preventive behaviors.
(2) Articles published until May 9, 2022.
(3) Articles published in English or Korean.
The exclusion criteria:
(1) Articles not related to the study aim.
(2) Articles not published in peer-reviewed journals.
(3) Review articles, conference papers, commentaries, and publications without full text.
Stage 2: Identifying Relevant Studies
A comprehensive and rigorous search strategy was employed to identify relevant studies. We combined the concept and target outcomes of interest (Levac et al., 2010). The search query was designed to explore the topic of “dementia preventive behavior” by crafting three distinct queries, each focusing on the individual terms “dementia,”“preventive,” and “behavior.” The initial search terms were selected from thesauruses (MeSH, Emtree, and Cumulative Index for Nursing and Allied Health Literature [CINAHL] headings); free-text terms with wildcards were used to improve sensitivity. The terms were combined and linked with Boolean operators: “OR” for combining all terms in each class and “AND” for linking the classes. Final search queries were guided by a university-based medical health science librarian, who possesses specialized expertise in systematic literature reviews. To ensure the search’s comprehensiveness and precision, the librarian conducted two face-to-face meetings and one email consultation with the research team, refining and finalizing the search strategy. The full query with search terms and Boolean operations for each database is provided in
Manual literature searches were conducted using PubMed, PsycINFO, CINAHL, Excerpta Medica Database (EMBASE), and Cochrane CENTRAL. The search was conducted on March 18, 2021, and updated on May 9, 2022, using the same strategy and databases.
Stage 3: Study Selection
The records were retrieved from databases and manual searching. Further, the identified studies’ bibliographies were screened in three steps by two reviewers. First, one researcher (SI) screened the titles and abstracts of the primary records to determine whether they met the minimum inclusion criteria. In the second step, two researchers (SI and MH) independently assessed the eligibility of the searched studies by screening titles and abstracts and then discussed inconsistencies until consensus was reached. Finally, two researchers independently screened full-text articles based on the inclusion and exclusion criteria, and any disagreements were resolved through discussion.
Stage 4: Charting the Data
An Excel-based data extraction tool was developed and used for data charting. The initial form was designed by one of the researchers (SI) and refined by another (MH). During the data extraction process, the data charting form was updated interactively. Information pertaining to the study characteristics (e.g., country, published year, study design, population, and sample size for analysis), factors influencing dementia-preventive behavior, and the direction of association was charted.
Stage 5: Collating, Summarizing, and Reporting Results
Three systematic steps were adopted to synthesize the findings based on the recommendations of Levac et al. (2010). First, a descriptive numerical synthesis was performed to obtain an overall and comprehensive perspective. Second, the findings are reported according to the purpose of the study. Finally, the integrated findings are presented with practical implications and key priorities for subsequent studies.
Results
Characteristics of the Included Studies
Figure 1 presents the flow of the study selection process (Page et al., 2021). In the initial search, 37,331 articles were retrieved through database searches, and 15 articles were identified through manual and citation-based searching. Twenty-two articles that met the inclusion criteria were included in the review. Table 1 presents the characteristics of the included studies. The first study included in this review was published in 2001, and more than half of the studies (59.1%) were published after 2019. Most studies were conducted in Asia, especially in South Korea. In most of the reviewed studies, the participants did not consist of specific disease patients or adult children of patients with dementia.
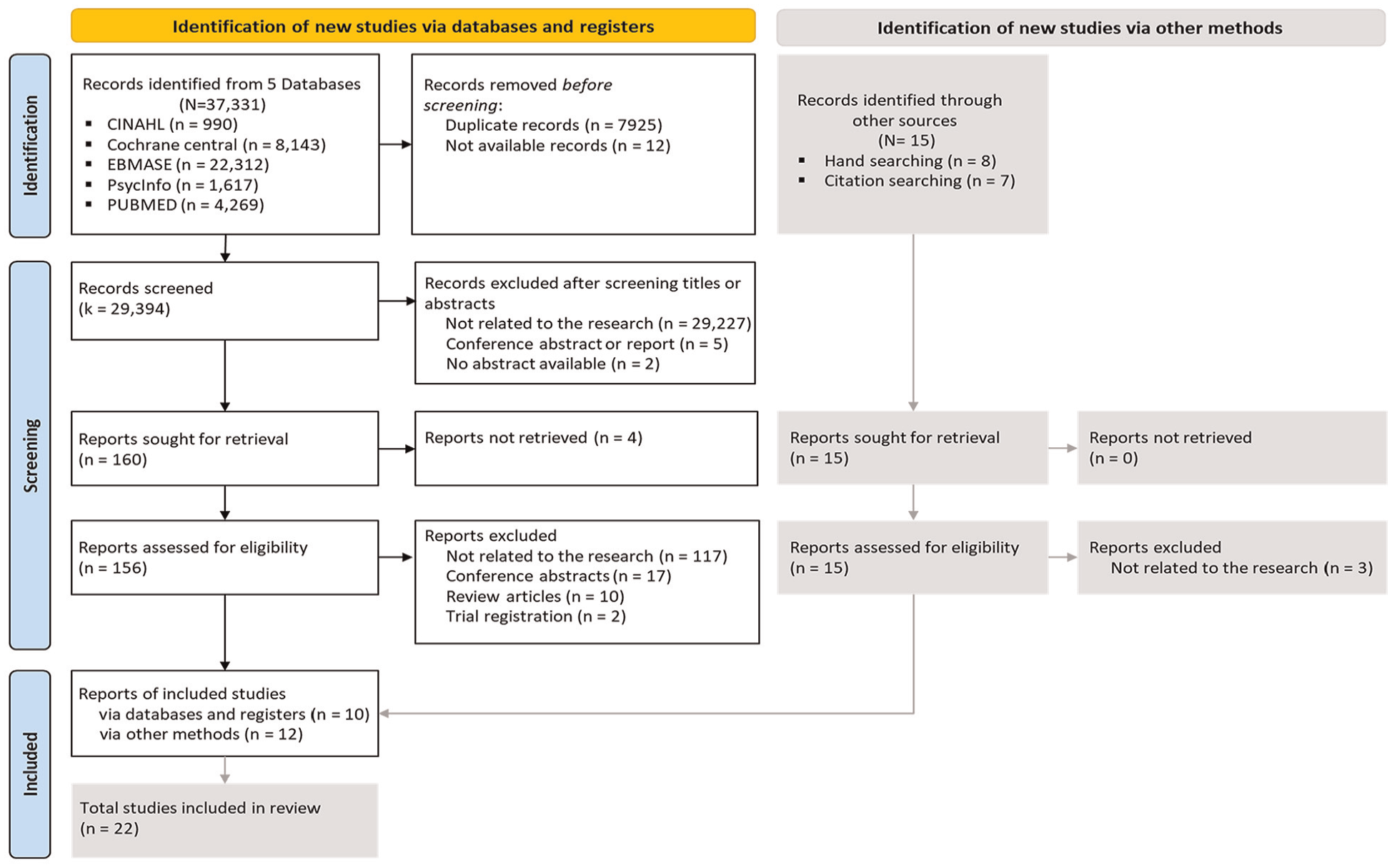
Flowchart of the study selection process.
Characteristics of the Included Studies (N = 22).

Determinants of Dementia-Preventive Behaviors
The identified factors were grouped into 28 specific determinants according to the conceptual categories of the PRECEDE framework (Green & Kreuter, 2005), as shown in Table 2 and Supplementary Information 2. Among the conceptual categories, six categories were identified: epidemiology, behavioral, environmental, predisposing, enabling, and reinforcing.
Determinants Identified by Synthesizing Evidence on Outcomes Reported in the Included Studies.

Epidemiological determinants
Family history or genetics, priority health problems, and objective and subjective health status were identified as the epidemiological determinants of dementia-preventive behaviors. Three studies reported that family history or genetics serve as motivators for dementia-preventive behaviors. Notably, one study reported that the association, whether positive or negative, between family history/genetics and dementia-preventive behavior depends on individual’s knowledge, feelings, and attitudes toward dementia (Rosenberg et al., 2020). Two studies identified priority health problems as a barrier to practicing dementia-preventive behavior.
Five reported studies highlighted the role of objective health status in dementia-preventive behaviors. Three out of five studies reported a negative association between objective health status and dementia-preventive behaviors. Specifically, having a certain disease or additional diseases was linked to reduced engagement in dementia-preventive behaviors (Kim & Kwon, 2019; Ko & Shin, 2013; Lim et al., 2021). Further, two studies reported a positive association between objective health status and dementia-preventive behaviors (Coulson et al., 2001; Pipatpiboon et al., 2022).
Three studies consistently showed a positive association between subjective health status and dementia-preventive behaviors (Coulson et al., 2001; Kang et al., 2015; J. Park & Shin, 2021). However, the association in one study was unclear due to insufficient reporting.
Behavioral determinants
Health behaviors and habits were identified as the behavioral determinants of dementia-preventive behaviors. Four studies reported that practicing healthy behaviors is positively associated with dementia-preventive behaviors (Coulson et al., 2001; Kim & Kwon, 2019; M.-R. Lee, 2019; Y. R. Lee, 2020); however, in one study, the direction of the relationship was unclear due to insufficient information. One study identified fixed habits as a barrier to practicing dementia-preventive behaviors.
Environmental determinants
The availability of time and healthy food are challenging environmental determinants. Three studies employing different study designs found that lack of time and readily available food interfered with dementia-preventive behaviors.
Predisposing determinants
Various factors were identified as key determinants in dementia-preventive behaviors, including socioeconomic characteristics, knowledge, perceptions, attitudes, interest, motivation, belief in one’s own ability, indirect experience of dementia, and emotional and cognitive responses to dementia. Specifically, among the socioeconomic characteristics, being over 40 years of age, female, having a relatively high educational level (more than high school or university), and having a high income were identified as positive factors influencing dementia-preventive behaviors.
Knowledge was the most examined determinant of dementia-preventive behaviors in two streams: dementia knowledge or literacy and medical and health knowledge (n = 11). Consistently, the majority of studies reported that more knowledge or literacy is positively associated with dementia-preventive behaviors. However, two studies reported no evidence for this association (Lim et al., 2021; Yamane et al., 2021).
Eight studies focused on the perceptions of benefits, barriers, achievability, and control. Based on the results of a previous study, self-efficacy and locus of control were grouped as perceptions of control (Au, 2015) . Perceiving dementia-preventive behaviors as beneficial, achievable, and controllable may facilitate dementia-preventive behaviors. Meanwhile, two studies reported opposing conclusions about the influence of perceived barriers, with one reporting it as a motivator and one reporting it as a barrier (Bird et al., 2021; Pipatpiboon et al., 2022).
Five study outcomes that directly or indirectly pertained to the degree of interest were grouped as determinants of “interest” (e.g., acquisition of dementia-related information, the number of participating programs on cognitive health). In four studies, a higher interest score on dementia or dementia prevention positively affected dementia-preventive behaviors (Kang et al., 2015; Kim & Kwon, 2019; Y. R. Lee, 2020; Lim et al., 2021). However, in one study, the direction of the relationship was unclear owing to insufficient information.
Five studies pointed out that positive attitudes toward dementia are positively associated with dementia-preventive behaviors, and vice versa. In one study, attitudes toward dementia were a mediating variable in the relationship between dementia knowledge and self-efficacy for practicing dementia-preventive behaviors (J.-H. Lee & Lee, 2016). However, two studies showed no evidence of an association between attitudes toward dementia and dementia-preventive behaviors (M.-R. Lee, 2019; Y. R. Lee, 2020).
While motivation is a consistent determinant that is positively correlated with dementia-preventive behaviors (Bird et al., 2021; Reynolds et al., 2022), patients’ indirect experiences of dementia remain controversial. Regarding indirect experiences, two studies demonstrated the positive effects of dementia-preventive behaviors (Bird et al., 2021; Smith et al., 2015). However, one qualitative study suggested that indirect experiences of dementia may act as a barrier to having a deterministic attitude toward dementia prevention (Rosenberg et al., 2020).
Based on a previous scoping review, studies on the concepts of concern, anxiety, fear, and worry about dementia were grouped into emotional and cognitive responses to dementia (Werner et al., 2021). Three studies examining concern, worry, and fear regarding dementia reported a positive correlation with dementia-preventive behaviors (Bosco et al., 2020; Rosenberg et al., 2020; Smith et al., 2015), whereas two studies examining anxiety about dementia concluded a negative association (K.-W. Lee & Kim, 2018; Vrijsen et al., 2021).
Enabling determinants
Credible programs and evidence-based information were identified as the determinants of dementia-preventive behavior. Studies also suggest that these could facilitate behavioral change for dementia prevention or vice versa.
Reinforcing determinants
Bird et al. (2021) reported that peer support is a reinforcing determinant of dementia-preventive behaviors. They found that lack of peer support can negatively affect dementia-preventive behaviors.
Discussion
In this study, evidence for the determinants of dementia-preventive behaviors was mapped using the PRECEDE model. Through a comprehensive scoping review, 28 specific determinants of dementia-preventive behaviors were established and organized into six conceptual categories. Our findings shed light on crucial factors influencing the adoption of preventive behaviors against dementia. In the following discussion, we will delve into these results, analyzing their implications and potential applications. Furthermore, we will leverage this knowledge to propose effective evidence-based strategies aimed at preventing dementia and promoting cognitive health.
The first step is to have innovative and practical perspectives to understand the specific determinants of dementia-preventive behaviors. Consistent with the current results, common factors affecting behavioral changes at the individual and ecological levels have been shared in several previous studies on chronic illness, cancer, cardiovascular disease, and type 2 diabetes mellitus (T2DM) (i.e., availability, socioeconomic characteristics, health status, knowledge, beliefs, attitudes, perceptions, peer support, motivation, evidence-based information, and available programs) (Moshki et al., 2017; Oliveri et al., 2018; Rainey et al., 2018; Saei Ghare Naz et al., 2018). Since previous studies were based on pre-existing theoretical models, the current study and previous studies inevitably report on common facilitating or hindering factors that affect behavior. Indeed, dementia is non-communicable and hereditary-related and is severe enough to impact an individual’s integrity of all aspects of one’s life, which can cause fear and worry (Chao et al., 2008; Ebert et al., 2020; Grande et al., 2020). In the same context, this study identified “emotional and cognitive response to dementia” and “indirect experience of dementia” as predisposing factors and “family history or genetics” as an epidemiological factor of dementia-preventive behavior. Therefore, as an emerging field of behavioral science for dementia prevention, an innovative and empirical approach is needed to identify dementia-specific determinants.
The second step is to identify the population-based determinants of dementia-preventive behaviors. Based on the findings of this review, two directions are suggested. First, future studies should consider various cultural contexts. In this review, most studies were conducted in Asia, especially in South Korea. Asia has the highest annual dementia incidence in the world (Prince et al., 2015), and South Korea is reporting as demonstrating the fastest incidence among the OECD countries (Organization for Economic Co-operation and Development, 2021). Against demographic and epidemiologic challenges, healthcare professionals in South Korea have engaged in proactive approaches to improve dementia-preventive behaviors. The increase in the number of people with dementia due to aging is a global megatrend. The Public Health National Center for Innovations has noted the importance of cultural sensitivity and population-appropriate approaches in public healthcare strategies (Centers for Disease Control and Prevention, 2020). Therefore, researchers must pay attention to cultural backgrounds and identify specific determinants of dementia, which can help guide an effective population-based intervention. Second, it is necessary to identify the determinants of dementia-preventive behaviors considering underlying diseases or conditions. A reviewed study on participants with T2DM reported that a longer disease duration is positively associated with dementia-preventive behaviors (Pipatpiboon et al., 2022). Consistent with the study, another study of an overactive bladder patient who was taking non-central nervous system (CNS)-sparing medication recommended changing the therapy plan to CNS-sparing medication to preserve cognitive function (Millimet et al., 2022). While the duration of T2DM and CNS-sparing medication may not apply to the general population, these may be essential to individuals with specific diseases. Therefore, population-based studies targeting specific diseases could enhance population-tailored strategies.
In the third step, efforts should be made to apply the current findings to improve the robustness of the strategies. In this review, 6 out of 28 determinants are still controversial: family history or genetics, objective health status, dementia knowledge or literacy, attitude, the indirect experience of dementia, and emotional and cognitive response to dementia. To disentangle the mixed findings on the factors of dementia-preventive behaviors, we suggest identifying the mediating and moderating variables to better understand this relationship. Among the studies included in this review, two implied the need to infer complex correlational or causal relationships (Coulson et al., 2001; Y. W. Lee et al., 2009). Consistent with previous studies, two cross-sectional studies have attempted to elucidate possible mechanisms, focusing on dementia knowledge, self-efficacy, and attitudes (Ko & Shin, 2013; J.-H. Lee & Lee, 2016). Notably, a quantitative study that revealed family history or genetics as a motivating factor of dementia-preventive behaviors asserted that it could be both a motivating factor and barrier depending on attitudes (Rosenberg et al., 2020). Furthermore, pathway analysis and structural equation modeling are required to gain comprehensive insight into a single network of linking factors so as to infer causality.
Finally, it is necessary to consider the content and structure of existing strategies to develop more effective interventions that promote dementia-preventive behaviors. For this, health practitioners must be astute to up-to-date evidence and develop evidence-based interventions. According to the current review, credible and evidence-based recommendations are one of the key motivators for promoting dementia-preventive behaviors (Bird et al., 2021; Bosco et al., 2020). Conversely, unreliable information may result in skepticism about recommendations for dementia-preventive behaviors. Therefore, interventions are more effective if they are based on empirical evidence. Moreover, personalized multi-level strategies can foster behavioral changes for dementia prevention. The current review found that dementia-preventive behaviors are also based on a complex interplay of an individual’s environmental, personal, and social factors. Consistent with the current results, the Body Brain Life Project—a randomized controlled trial—has verified that multi-component interventions are effective in enhancing dementia-preventive behaviors and reducing dementia risk (Anstey et al., 2015; McMaster et al., 2020). Moreover, one study highlighted that personalized recommendations may apply to their lifestyle (Vrijsen et al., 2021). Therefore, interventions tailored to an individual’s environmental, personal, and social factors will be a practical and effective approach to promoting dementia-preventive behaviors.
This study contributes to the body of evidence on dementia by synthesizing findings from only peer-reviewed studies and integrating scattered pieces of evidence based on a theoretical model. However, this study has some limitations. First, since this study was based on an individual-level approach, administrative and policy assessments were not considered. Therefore, it is necessary to investigate the political and administrative factors of each society to identify what hinders or promote dementia-preventive behaviors. Second, more than half of the included studies were conducted in Asian countries. Although the determinants identified in this review encompass diversity, further studies in various cultural contexts are required.
Conclusion
This scoping review notably synthesized current research evidence by identifying 28 determinants across 6 conceptual categories of dementia-preventive behaviors based on the PRECEDE framework. The results provide an in-depth perspective for healthcare providers and researchers, guiding effective, evidence-based interventions to promote behavioral changes for dementia prevention. The comprehensive findings from this review hold significant potential to inform policymakers, empowering them to develop targeted strategies that mitigate the global burden of dementia and enhance cognitive well-being across diverse populations.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241263690 – Supplemental material for Determinants of Dementia-Preventive Behaviors: A Scoping Review Based on the PRECEDE Model
Supplemental material, sj-docx-1-sgo-10.1177_21582440241263690 for Determinants of Dementia-Preventive Behaviors: A Scoping Review Based on the PRECEDE Model by So Im Ryu, Min Hye Lee and Yeon-Hwan Park in SAGE Open
Supplemental Material
sj-docx-2-sgo-10.1177_21582440241263690 – Supplemental material for Determinants of Dementia-Preventive Behaviors: A Scoping Review Based on the PRECEDE Model
Supplemental material, sj-docx-2-sgo-10.1177_21582440241263690 for Determinants of Dementia-Preventive Behaviors: A Scoping Review Based on the PRECEDE Model by So Im Ryu, Min Hye Lee and Yeon-Hwan Park in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (Grant number: RS-2024-00345763). The funder had no role in the design and conduct of the study; collection, analysis, and interpretation of data; the preparation of the manuscript; or the review or approval of the manuscript.
Ethical Approval
Not applicable.
Consent to Participate
Not applicable.
Data Availability
All relevant data are within the article and its supporting information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.